
Abstract
Approximately, 2.4 billion people, globally, lack access to safe toilets. The burden of this deficiency falls disproportionately on women living in informal settlements in developing countries. While there is a growing body of literature looking at the factors influencing women’s sanitation behavior, little is known about the role of the neighborhood environment. This study sought to explore this issue using data from a 2016 mixed-methods study focused on women in Mathare Valley informal settlement in Nairobi, Kenya. Qualitative and quantitative data were used to analyze the role of neighborhood disorganization in the relationship between women’s sanitation-related stressors and their sanitation behaviors (utilization). Findings suggest that neighborhood disorganization is inextricably linked to women’s daily sanitation behaviors and the stressors that are associated with those behaviors. These results suggest that the health and safety of neighborhood environments may be critical factors in the future success of sanitation-related interventions and policies.
Introduction
Safe sanitation is a prerequisite for the health and well-being of individuals and is essential to the development of communities and nations (Mara, Lane, Scott, & Trouba, 2010; Munamati, Nhapi, & Misi, 2016; Phukan, 2014). Despite substantial gains globally in sanitation access between 1990 and 2015 under the Millennium Development Goals, 2.4 billion people still lack access to basic sanitation (World Health Organization [WHO], 2016). Although access to sanitation is a global issue, there are vast disparities in coverage across regions and populations (WHO & United Nations Children’s Emergency Fund [UNICEF], 2017). While most high-income countries have achieved nearly universal access to sanitation, the same is yet to be seen in low- and lower-middle-income countries (LMICs). The majority of people without access to sanitation are in sub-Saharan Africa (Munamati et al., 2016; WHO & UNICEF, 2015).
In Nairobi, Kenya, where more than half of the population live in informal settlements, data suggest that 68% of settlement dwellers rely on public toilet facilities and an additional 6% have no access to toilets at all—resorting instead to such means as open defecation (OD) or plastic bags/buckets (Ruhiu et al., 2009). The problem of poor sanitary conditions is especially critical for the residents in these settlements because high population densities combined with poor or absent sanitation and sewerage systems increase residents’ risk of direct exposure to human feces. Neighborhood disorganization in these settlements—often marked by higher rates of crime and violence, lack of formal services to help maintain the environment (e.g., garbage collection, water, and sanitation), and high unemployment—can further limit residents’ ability to easily and safely navigate their environments, manage their daily tasks, and access the services that do exist (Parks, 2014; Winter & Barchi, 2015).
Women living in informal settlements are disproportionately burdened by lack of access to sanitation (Corburn & Hildebrand, 2015; Khosla, 2000). They face a number of gender-specific social stressors such as lack of privacy and dignity (Corburn & Hildebrand, 2015; Sahoo et al., 2015; Sommer, Ferron, Cavill, & House, 2014), sexual violence, and harassment associated with use of community toilets or sites for OD at night or during menstruation (Amnesty International, 2010; Khanna & Das, 2016; Khosla, 2000; Sahoo et al., 2015; Sommer et al., 2014)—stressors that are likely to be exacerbated by social and/or physical conditions of the neighborhood environment such as the presence of crime and violence (Winter & Barchi, 2015). To date, however, there has been limited research focused on the potential role of the neighborhood environment in women’s sanitation behaviors.
Neighborhood Disorganization in Sanitation Utilization
Social disorganization theory focuses predominantly on the relationship between neighborhood structure, social control, and crime. In their benchmark study, Sampson and Groves (1989) proposed that community organization is directly related to a community’s ability to come together to address shared problems. By extension, the absence of these social structures leads to highly disorganized communities (Markowitz, Bellair, Liska, & Liu, 2001; Villarreal & Silva, 2006). According to this theory, the physical conditions of a neighborhood play an important role in influencing residents’ attitudes regarding neighborhood safety (Austin & Sanders, 2007). Some places are labeled as “good” while others are labeled as “bad” depending on the conditions and standards that characterize them. In disorganized communities, for example, crime is not only likely to occur, but is uncontrollable and often very serious (Jackson & Bradford, 2009). To cope with the stress of living in these disorganized communities, people often adopt avoidance behaviors, such as limiting activity or avoiding unsafe areas at night, or defensive behaviors, such as hiring/bringing an escort, carrying a weapon, or adopting the buddy system (Rader, May, & Goodrum, 2007; Rollwagen, 2014).
Informal settlements are often considered highly disorganized communities with high rates of delinquency and violent crimes (Parks, 2014; Phukan, 2014). Most women living there do not have access to toilet facilities within their homes—relying largely on public or community toilets outside their homes and buildings (Corburn & Hildebrand, 2015; Corburn & Karanja, 2014; Srinivasan, 2015). In light of social disorganization and fear of crime theories, one might postulate that people who live in highly disorganized communities, for example, informal settlements, and lack adequate sanitation facilities may decide to avoid using shared or community toilets that could expose them to harassment, violence, or discomfort, especially at night or during menstruation (Amnesty International, 2010; Corburn & Hildebrand, 2015). Instead, women may opt to use bags/buckets at home and empty the raw sewage into nearby drainages in the morning to avoid exposure to the discomfort or risks of traveling to or using public/community facilities in these settlements at night (Corburn & Hildebrand, 2015; Greed, 2015)—a practice that increases women’s and other informal settlement residents’ risk of direct contact with untreated waste and is linked to serious environmental and public health consequences (Baum, Luh, & Bartram, 2013; Kulabako, Nalubega, Wozei, & Thunvik, 2010).
Although there is limited research linking neighborhood disorganization to women’s sanitation behaviors and choices, a number of studies have recognized the influence of neighborhood disorganization on certain types of behavior in informal settlements, for example, perpetration of violent crimes (Parks, 2014). The purpose of this study was to contribute a more in-depth understanding of the extent to which neighborhood disorganization may moderate the relationship between specific sanitation-related stressors and women’s sanitation behaviors in informal settlements in Kenya.
Method
Research Setting
Mathare Valley (Mathare) informal settlement (shown in Figure 1) is one of the oldest and largest informal settlements in East Africa. The first settlers in Mathare arrived in the 1920s. Today, Mathare has expanded to become home to approximately 230,000 residents living in an area smaller than 3 km2 (Lundine, Kovacic, & Poggiali, 2012). According to residents, Mathare consists of 11 villages but, to the “outsider,” the boundaries between these villages are often difficult to identify.

Views of Nairobi informal settlement.
Like all informal settlements in Kenya, service provision, living conditions, and health in today’s Mathare are inextricably linked to the country’s colonial history (Corburn & Karanja, 2014). In Kenya, colonial entities wanted to deter rural nationals from moving into urban centers; so, they deliberately stopped providing housing and basic services to the growing informal settlement areas (Nilsson & Nyanchaga, 2008). When their efforts to deter African migrants were unsuccessful, British colonials tried to demolish Mathare in 1952 and detain its residents (Corburn, Ngau, Karanja, & Makau, 2012). Despite worsening conditions, migrants poured into the Mathare settlement. Like all informal settlements, Mathare has continued to be excluded from the state’s formal planning framework and, consequently, formal services and utilities (water, sewerage, garbage disposal, power, etc.) are not available (Ruhiu et al., 2009).
Access to sanitation in Mathare has remained limited. Estimates from a recent study suggest that about 83% of residents rely on shared toilets (see Figures 2 and 3 for examples of these types of toilets; Corburn & Hildebrand, 2015). Maps show that there are approximately 144 of these shared toilets scattered throughout the settlement (Corburn & Hildebrand, 2015). On average, the toilets serve approximately 85 households and are located at least 50 m from people’s homes (Corburn & Hildebrand, 2015). A related study in Mathare found that over two thirds of the residents reported sometimes using plastic bags or buckets to dispose of urine and feces (Corburn & Karanja, 2014; see Figure 4). Only about 15% of residents in Mathare have access to a private toilet facility (Corburn & Hildebrand, 2015; see Figure 5).

Public/Community toilets are the most commonly used toilets by women in Mathare.

Toilets that are not open to the public, but are shared by many households, such as plot or building toilets, are also prevalent.

Use of open defecation, bags, and/or bucket is common among women in Mathare.

Private toilets—used by only a single household—are uncommon, but present in Mathare.
Data
This analysis uses cross-sectional data drawn from a 2016 study in Mathare that included information about women’s sanitation practices as well as a number of other measures focused on women’s health, experiences of violence, perceptions of their neighborhood, and basic sociodemographic information. Data for the Mathare study were collected in two phases. In Phase 1, in-depth, qualitative interviews were carried out with 55 women. Subsequently, in Phase 2, household surveys were carried out with 550 women.
Study Sample
In Phase 1, the chief of Mathare, chairmen from each of the 11 villages, and a local women’s health organization helped recruit women for introductory meetings about the study in each village. Women interested in participating signed up and provided basic demographic, sanitation, and contact information. Based on variations in women’s sanitation practices and demographics, five women from each of the 11 villages were invited to participate. Stratified random sampling was used to select women for Phase 2 of the study. Mapping software was used to generate a random sample of 50 households in each of Mathare’s 11 villages—a technique commonly applied to sample households in informal settlements (Corburn & Karanja, 2014; Kovacic, 2014; Tumwebaze & Lüthi, 2013). Individual women were then selected from each household using Kish (1965) methodology.
This analysis included qualitative data from the transcripts generated from interviews with the 55 women and quantitative data generated from women’s responses to questions on the 550 household surveys. Women across both phases of the study were between the ages of 18 and 72 years, spoke English and/or Swahili, and had lived in Mathare for at least 6 months prior to the study.
Measures
The purpose of this study was to test the moderating effect of neighborhood disorganization on the relationship between women’s sanitation-related stressors and their sanitation utilization practices (see model in Figure 1). Thus, the outcome variable is women’s sanitation utilization practices. Based on women’s responses to qualitative and quantitative questions about their daily sanitation utilization practices, we clustered women into three sanitation utilization categories: (a) unsafe day/unsafe night—uses unsafe methods of disposal for urination/defecation at least once during the day and at all times during the night; (b) toilet day/unsafe night—uses toilet for all urination/defecation during the day, but uses unsafe methods of disposal, for example, buckets, bags, OD, at night; and (c) toilet day/toilet night—uses toilet for all urination/defecation at all times.
Qualitative measures
Qualitative questions about sanitation-related stressors and their relationship to sanitation utilization behaviors and choices were open-ended and general to allow women’s own views about the stressors they encounter around sanitation to emerge. Questions such as “During the day/night, where do you usually urinate/defecate and/or how do you usually dispose of your urine/feces?” “What reasons influence your decision to use this/these particular facility/ies or method(s) of disposal over any other?” “What are the things you like best/least about using this/these facility/ies or method(s) of disposal?” “Will you describe any positive/negative experiences you have had while trying to access or while using this/these facility/ies or method(s) of disposal?” were used to elicit women’s reasons for using particular sanitation strategies rather than to provoke reactions to researcher-hypothesized factors shaping their behavior. Similarly, prompts such as “Would you describe what it is like to live in Mathare as a woman?” “Using your senses, would you describe what it is like to walk through your village during the day/at night?” “What does the environment/landscape look/smell/sound like?” “Would you describe a typical day for you in Mathare?” “Are there particular places or pathways in your village or Mathare, as a whole, that you intentionally choose to use/avoid?” “Are there certain people or groups in your village or Mathare, as a whole, whom you intentionally choose to see/avoid?” were used to elicit discussion from women about aspects of their social and physical environments that influence their perceptions of security, hygiene, and neighborhood disorganization.
Quantitative measures
Items for the Neighborhood Disorganization Scale were modified from Gau and Pratt’s (2008) 16-item Social Disorganization Scale. The scale has been validated in urban and rural contexts in the United States and shown to be a reliable measure of disorganization (αcronbach = .857-.868; Gau & Pratt, 2008, 2010). Respondents were asked to rate the seriousness (1 = not a problem, 2 = a problem, 3 = a serious problem) of 16 problems (e.g., violent crimes, rape/sex crimes, stray animals, garbage/litter) in their neighborhood (see Appendix A in supplementary material for the full list of items). Each of these 16 variables was then collapsed into a binary variable for which a woman was given a score of “1 = a problem or serious problem” on the item if she had a response of either 2 = a problem or 3 = a serious problem and a score of “0 = not a problem” if she responded that it was 1 = not a problem. Subsequently a score variable was created by taking the sum of these binary values for all 16 items. Thus each woman received a score that ranged between 0 = min and 16 = max (Kuder–Richardson [KR]-20 = .841).
A framework developed by Sahoo et al. (2015) that grouped sanitation-related stressors into environmental, social, and contextual categories (see Figure 6) was used as a guide to organize the quantitative sanitation-related stressors for this study as follows:
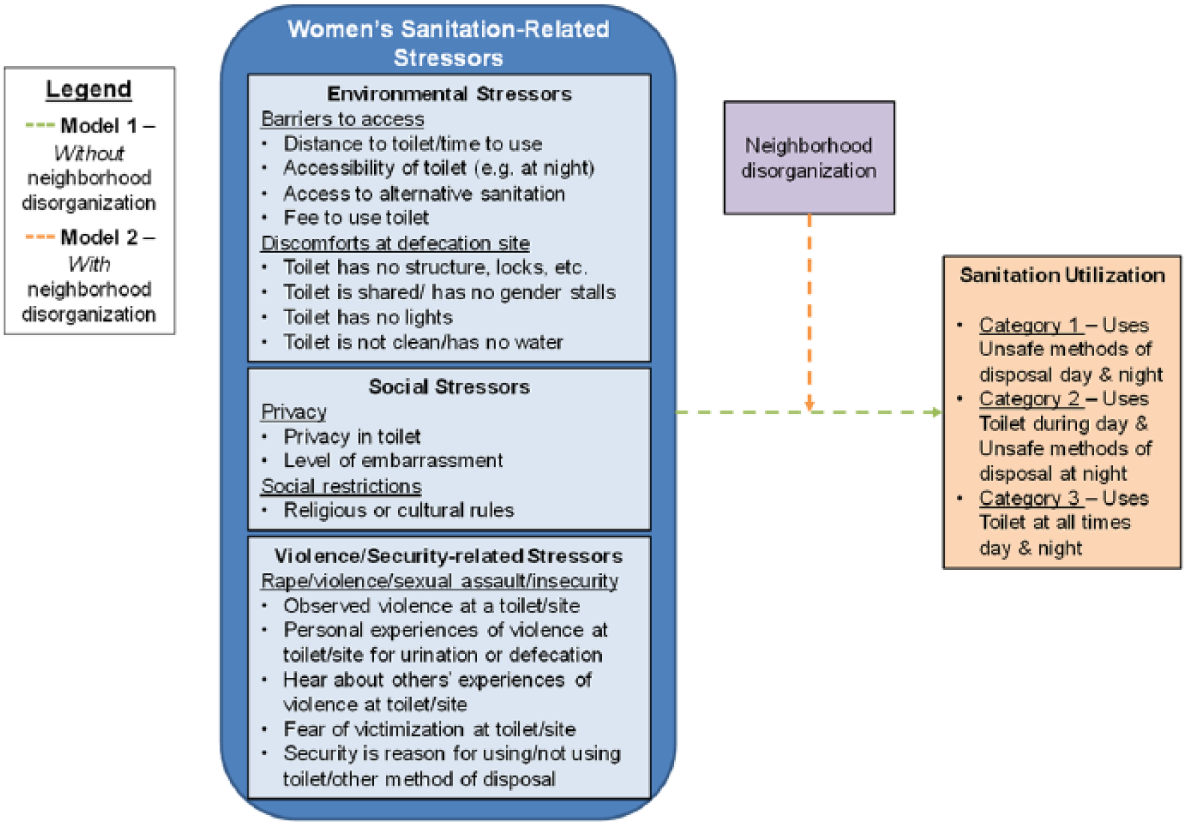
Neighborhood disorganization as a moderator of sanitation-related stressors and women’s sanitation utilization.
Environmental stressors
In this study, environmental stressors included a categorical variable for walk-time to site for urination/defecation (0 = doesn’t leave home, 1 = less than a minute, 2 = 1-2 min, 3 = 3-4 min, 4 = 5+ min) and several binary variables (0 = no, 1 = yes), measuring (a) whether or not a woman’s daytime toilet is generally open at night; (b) whether a woman has to queue to use her toilet at least sometimes; (c) whether a woman pays a fee to use her toilet; (d) whether a woman has access to alternative toilets other than her primary toilet or method of disposal; (e) whether her toilet has a superstructure, a roof, a tight-fitting door, and a lock; (f) whether her toilet has separate stalls for men and women; (g) whether her toilet has lights; (h) whether her toilet has running water; (i) whether her toilet is clean; and (j) whether her toilet is shared by more than 10 people.
Social stressors
One of the most prominent social stressors in the literature is women’s inability to manage menstruation when they lack access to private, safe, and hygienic toilets (Sommer, Kjellén, & Pensulo, 2013). In particular, studies have suggested that lack of access to private and hygienic toilets with functioning doors and locks, separate gender stalls, and running water risk feelings of embarrassment as well as poor health outcomes associated with neglectful menstruation practices (Lahme & Stern, 2017; Pillitteri, 2011; Sumpter & Torondel, 2013). We included several binary measures to capture these and other social stressors, that is, (a) whether or not a woman feels she has privacy when using her primary toilet/method of disposal, (b) whether a woman feels embarrassed using her primary toilet/method of disposal, (c) whether a participant’s religion has any rules about the disposal of human excreta and/or urine, and (d) whether her culture has any rules about the disposal of human excreta and/or urine.
Contextual stressors
Finally, a number of measures were used to capture contextual violence/security stressors. Women in the sample were asked many questions about whether they had experienced, observed, or heard about sexual, physical, or verbal harassment associated with walking to/from or using their toilet/site for urination/defecation. Three violence variables were created from responses to these questions: (a) an “observed recent violence against women (VAW) at toilet” variable, for which a woman was given a score of 1 = yes if she reported having observed physical, sexual, or verbal VAW while walking to/from or using her site of urination/defecation in the last 12 months; (b) a “heard about recent VAW at toilet” variable, for which a woman was given a score of 1 = yes if she reported having heard about any physical, sexual, or verbal VAW associated with women accessing or using her site for urination/defecation in the last 12 months; and (c) an “experienced recent VAW at toilet” variable, for which a woman was given a score of 1 = yes if she reported having experienced any physical, sexual, or verbal VAW while walking to/from or using her site of urination/defecation in the last 12 months.
Three variables were created to reflect security-related stressors. A dichotomous “fear of victimization” variable was created from a woman’s responses to two questions about (a) whether she feels it is generally safe for women to visit a toilet alone and (b) what she would fear might happen if a woman were to visit a toilet alone. Women who identified fear of violence, rape, robbery, or other personal attacks were given a score of 1 = fears victimization. A dichotomous variable, “security is reason for using method,” captured whether a woman identified security as a reason she regularly uses her current toilet/method of disposal. In addition, respondents in Phase 2 were asked to explain why they chose not to use available alternative toilets in their neighborhoods. Responses from this question were used to develop a third dichotomous variable, “Insecurity is reason for not using alternatives,” to reflect whether or not a woman identified insecurity as a reason she regularly chose not to use the alternative toilets.
Analysis Strategy
Interview transcripts were coded in Atlas.ti software (Scientific Software Development, 1999). Three researchers independently coded each of the transcripts. Cross-case and thematic analyses were used to develop a qualitative representation of women’s perception of neighborhood disorganization in their communities and in Mathare as a whole. Codes and concepts were compared among the three researchers. In instances where researchers’ codes did not agree, the full research team discussed discrepancies and decided upon final codes and resulting findings. In the presentation of qualitative results, pseudonyms were used in place of village and participant names to preserve participant confidentiality.
Quantitative data were analyzed in Stata Version 14 (StataCorp, 2015). There were minimal missing data for the variables used in this analysis (0%-3%, with most variables missing less than 1%); however, list-wise deletion would have led to the loss of 10% of the data. Thus, missing data were imputed using single hot deck imputation (Schonlau, 2012). Descriptive statistics and chi-square analyses were run for all potential sanitation-related stressors (see Table 2). A single-level, fixed effects, multinomial logistic regression (Model 1) was also run using the user-written program gllamm with 12 integration points to test associations between women’s stressors and their sanitation utilization practices without any neighborhood-level effects (Rabe-Hesketh, Skrondal, & Pickles, 2005). Finally, gllamm was used to run a two-level, random-intercept, multinomial logistic regression (Model 2) with the same set of variables used in Model 1. In this model, however, neighborhood disorganization was included as the Level-2 clustering variable to test the moderating role of neighborhood disorganization on the relationship between women’s sanitation-related stressors and their sanitation utilization.
Ethics Statement
The study protocol underwent ethics review by Kenya’s National Commission for Science, Technology, and Innovation and the institutional review board at Rutgers University.
Results
Qualitative Results
Sociodemographic characteristics
Characteristics of the qualitative sample are summarized in Table 1. The information is organized according to the three categories of sanitation utilization. Over three quarters of the women in the qualitative sample were between the ages of 25 and 44 years and just under half were married. Over a quarter of the women reported household incomes under 5,000 KES/month (about US$50) and an additional 31% reported household incomes between 5,000 and 9,999 KES/month. All but 24% of the women had at least completed primary school.
Sample Sociodemographic Characteristics.
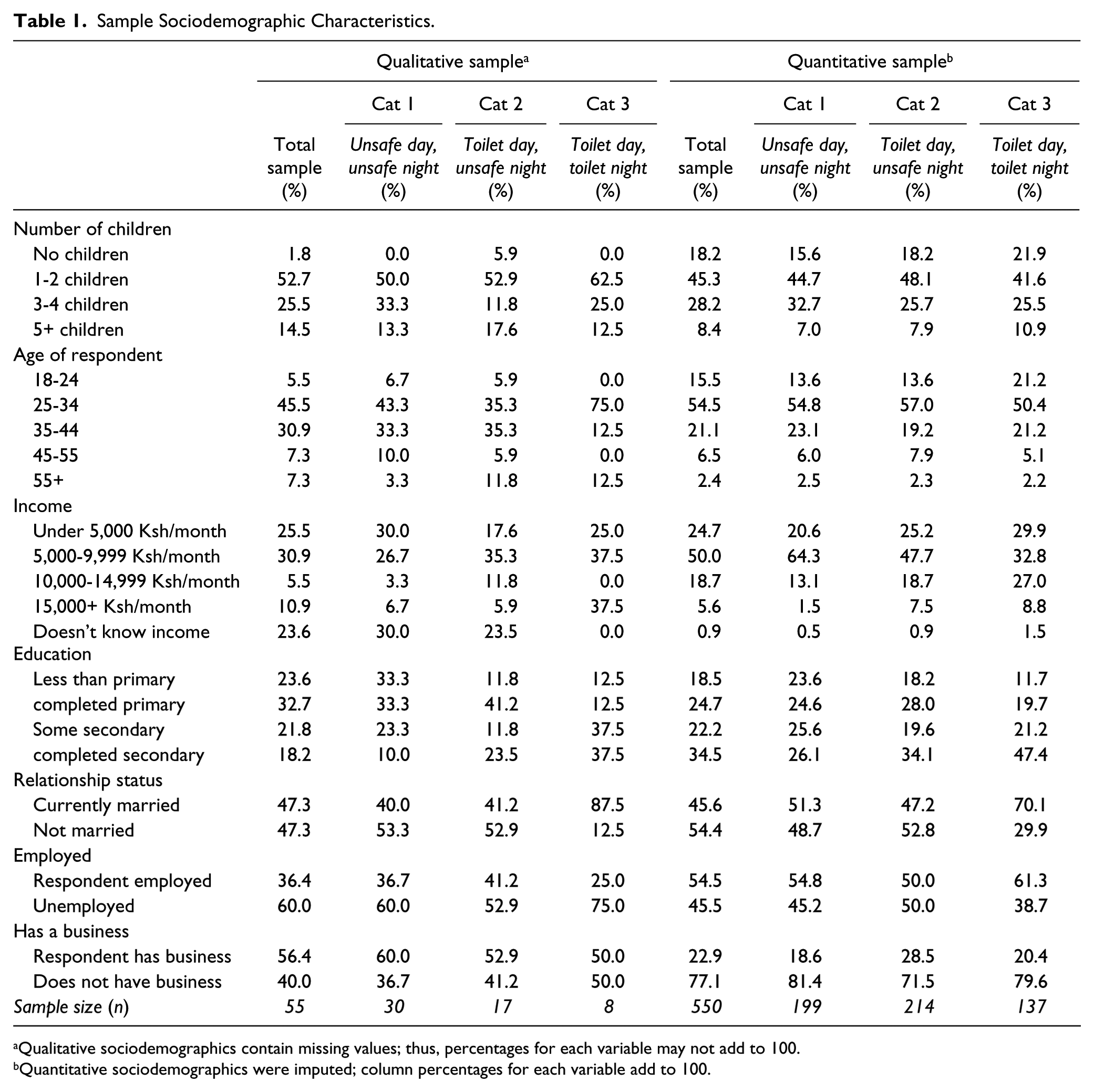
Qualitative sociodemographics contain missing values; thus, percentages for each variable may not add to 100.
Quantitative sociodemographics were imputed; column percentages for each variable add to 100.
Role of neighborhood disorganization
All but one of the 55 women in the qualitative sample talked about some aspect of their community that is representative of common manifestations of neighborhood disorganization. Characteristics indicative of neighborhood disorganization, such as child abuse, domestic violence, theft, stray animals, and idle youth, arose often when women were discussing (a) their reasons for using/not using different sanitation options during the day and night; (b) their daily experiences and feelings about security in their village and/or Mathare, in general; (c) their fears around going outside at night; and (d) their perceptions of “hygiene” or “cleanliness” of their environment. About 80% of women (n = 44) talked specifically about rape and/or sexual assault as an issue in Mathare, representing the majority of women in each sanitation utilization category.
Some women talked about their fears of rape or sexual assault in the context of trying to access sanitation in Mathare, for example, [T]here is one toilet that was closed down there in Village 8 due to rape cases. When ladies entered the toilet men were allowed to mingle around there pretending they were cleaning or mopping, and that’s not the true story. They just target. When a lady . . . a smart lady, has entered the toilet they grab her, they rape her . . . These cases have been reported several times. At long last it was closed down. (Cla, Village 1)
A few women also mentioned fear of rape as a stressor specifically associated with having to manage menstrual hygiene, for example, It is difficult for women. You know, men, they don’t have to worry. They can just stand anywhere and urinate, but a woman, for example, if she wants to change her pad, you see, it is a must she enters the toilet. So that is why women are often having a lot of problems . . . You can even be raped. You know, with men, they can do it anywhere, but for women they have to do it in a secure place. So I think women have to look for a private place. (Her, Village 3)
Several women provided examples of the ways in which the fear and/or incidences of rape actually influenced their adoption of alternative methods of dealing with urine and feces in an unsafe environment. For example, Toilets close between 9:30 and 10:00 p.m. So after that, they won’t open. So in case of anything [urination/defecation], it is a must now you use a bucket or you use a polythene [bag]. For security matters you cannot go outside . . . You can meet with a thief. We say, if you are a girl, you cannot expect a girl like this to go out . . . She can go out and even she can be raped; therefore, she cannot go out. (Kav, Village 1)
In addition to fears of rape or sexual crimes, many women in the qualitative sample also spoke about theft, for example, pickpocketing or “ngeta” (grabbing) of phones and/or house robbery as other serious issues in Mathare. Approximately, three quarters mentioned theft and/or robbery as a concern. Some women talked about experiences or personal fears associated with theft or robbery as a motive for choosing to use or to avoid certain sanitation options. For example, If you enter the toilet, the toilet has no electricity. There is pure darkness . . . you find that toilet is a completely dark place . . . there is no light. So you don’t know who you will find there inside, who you will find outside. Maybe you go and when you leave you find someone waiting for you outside . . . If you go to the toilet at night something can happen to you . . . like I am a woman; so I can be raped or if you have something with you, like a phone, it will go and others will even use a knife. (Gra, Village 7)
Some women provided specific stories about being robbed or about other women being robbed while trying to access sanitation at night.
There was [a woman]. She went to that toilet at night. Then she met with some youth. They grabbed her and they struck a bargain with some thieves . . . They stole her phone and they raped her . . . (Cat, Village 6)
Other women simply talked about robbery/theft in the context of poor security in Mathare, in general. For example, Security here is bad. Thieves are many. They stab people with knives. You cannot go outside at night. You don’t know who is outside that night . . . The thieves have expanded to steal people’s things. (Flo, Village 4)
Other factors characteristic of neighborhood organization that arose during women’s conversations about sanitation and their daily experiences in Mathare included idle youth (n = 32, 59%), violent crimes and/or weapons (n = 17, 31%), garbage everywhere (n = 17, 31%), drug and/or alcohol use (n = 12, 22%), a lack of security/street lights and/or darkness (n = 12, 22%), child abuse and/or harassment (n = 8, 15%), gangs (n = 5, 9%), and stray animals (n = 4, 7%). Many women in Mathare identified idle youth as one of the biggest contributors to the crime and general insecurity in Mathare. Most of these women expressed a belief that idle youth were frequently the perpetrators of rapes, robbery, and violent crimes. For example, Every person has his own needs . . . So if you have a good job and he doesn’t have a job, you see, like he can rob you . . . when Kenya National Youth Service (NYS) was here, you see, there was no crime, there were no youth stealing because they had work. They were just waiting some place for their salary. But like these days, now that there is no NYS here, the robbery has gone up. We were so grateful when those youth were working because it is those same youth that are the ones stealing. But now that there is no work, we have many problems. First, there are assaults at night, there are robberies every day. Even the day before last I was beaten and I went to hospital. (Sha, Village 7)
Finally, violent crimes showed up as a common disorganization factor among women’s testimonies. Some women talked more generally about the sorts of crimes that frequently occurred in their villages or Mathare. Others provided specific stories about incidences that had recently occurred. Some of these stories were related to women’s fear of using certain sanitation methods at night, for example, toilets outside their homes. For example, This one day a woman went to the toilet and it was 1:00 in the night. A man had gone and hidden himself in the women’s toilet. She didn’t know; so she went to open the toilet and found a man hiding himself there. He grabbed her and strangled and raped her. Now because of that rape that mama died. That is what scares people. That is why there is no one visiting there at night. (Dor, Village 6)
Interview responses seem to indicate that women more readily identify serious crime as the biggest neighborhood disorganization-related issue in Mathare. Far fewer women talked about general disorganization (e.g., litter, stray animals, vandalism) as a critical problem. However, some women did identify garbage, lack of street/security lights, drug and alcohol use, and stray animals as issues, but, usually, with far less frequency and detail than crimes. For example, We don’t have a dumping site [for garbage], but we use that place there at the road or else that sewer line—most people are used to using it as a dumping site. (Mil, Village 1) We don’t have lights. The criminals know that there are no lights. . . . you don’t know who has hidden himself there . . . we don’t even have those big lights. (Gra, Village 7) Me, myself, I will not agree to go outside . . . there are many things like cats out there, those black ones. If you go out, you can get scared. (Mar, Village 6) The other day here there was a man. He opened a door, he entered a house, he raped a woman during the night. Even the other day there was another mama. A robber entered and her husband works nights—he’s a soldier. [The robber] entered, he carried her to the river, and he raped her there . . . often those youth are drunk. They have smoked marijuana. Now, you know, they are not in their right mind. (Jan, Village 8)
Quantitative Results
Sociodemographic characteristics and bivariate statistics
Sociodemographic characteristics of the quantitative sample are summarized in Table 1. As in the qualitative sample, the majority of women in the quantitative sample were between the ages of 25 and 44 years, just under half were married, and most reported monthly household incomes less than KES 10,000 (about US$100). Descriptive and bivariate statistics of the sanitation-related stressors included in this study are summarized in Table 2.
Descriptive and Bivariate Statistics.
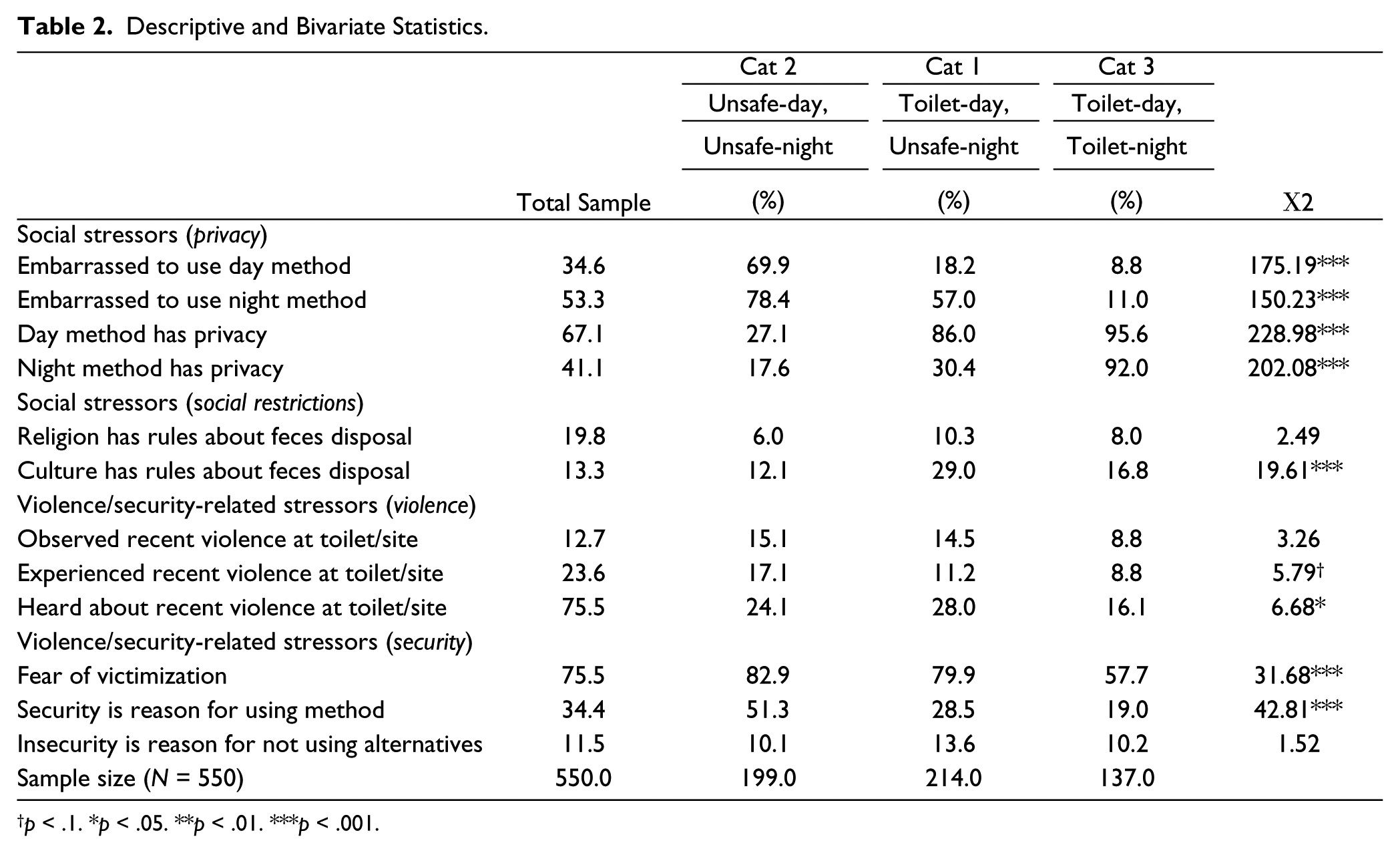
p < .1. *p < .05. **p < .01. ***p < .001.
Frequencies for the environmental and social stressors for women in Category 1 (those relying mostly on bags, buckets, and OD) often varied from those of women in the other sanitation utilization categories. Women in Category 1 generally had less access to clean facilities with lights, separate gender stalls, structural privacy features (e.g., doors, locks on doors, roof, and super structures), and running water. A small proportion of women in Category 1 reported having privacy while using their toilets/methods of disposal and a higher proportion reported feeling embarrassed when using their primary methods of disposal compared with women in the other two categories (significant chi-square, p < .001).
Fewer women in Category 3 (those who use a toilet at all times) had heard about violence against another woman (sexual, physical, or verbal) associated with her walking to or using a toilet facility/method of disposal (16%) compared with women in the other categories (24%-28%). Results from the chi-square test suggest that fear of sanitation-related victimization varied significantly between the three sanitation categories, χ2(2, N = 550) = 31.7, p < .001, with fewer women in Category 3 reporting fear of sanitation-related victimization. Finally, over 51% of the women in Category 1 cited security as one of the primary reasons they use their current method of disposal compared with 29% in Category 2 and 19% in Category 3, χ2(2, N = 550) = 42.8, p < .001.
Moderated associations between stressors and sanitation behavior
Results from the multinomial logistic regressions examining the relationship between women’s sanitation-related stressors and their sanitation utilization with (Model 2) and without (Model 1) neighborhood disorganization as a moderator are summarized in Figures 7 and 8. Relative risk ratios (RRRs), 95% confidence intervals (CIs), and p values for Models 1 and 2 and Level-2 variances, and ICCs for Model 2 are provided in Appendix B in supplementary material. In these multinomial analyses, findings for women in Categories 1 (uses unsafe methods of disposal during the day and night) and 2 (uses toilet during the day and unsafe methods of disposal, for example, bags, buckets or OD, at night) are compared with those for women in Category 3 (uses a toilet at all times).
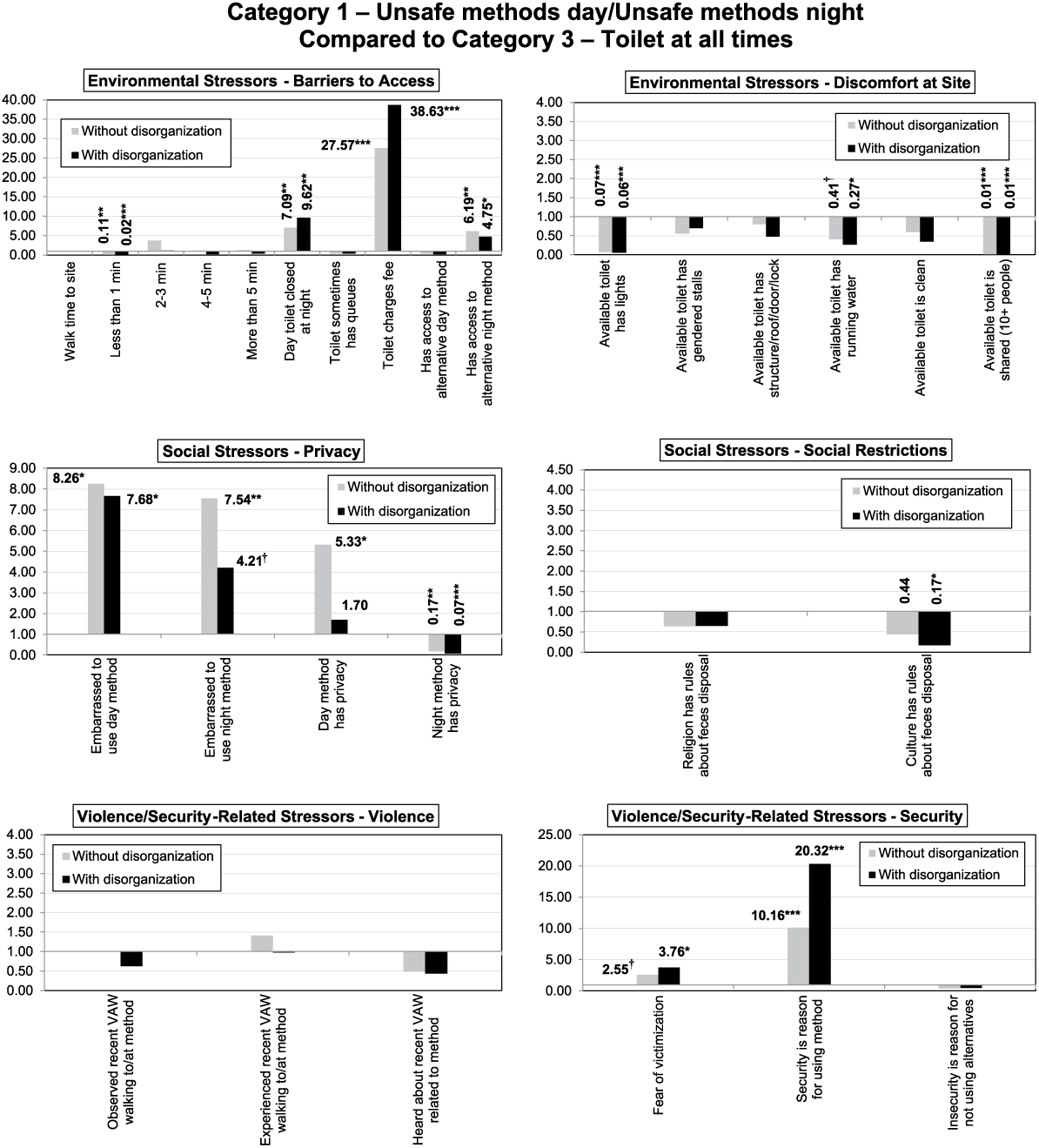
Associations (relative risk ratios) between sanitation-related stressors and Sanitation Utilization Category 1 (compared with Category 3) with and without neighborhood disorganization as a moderator.
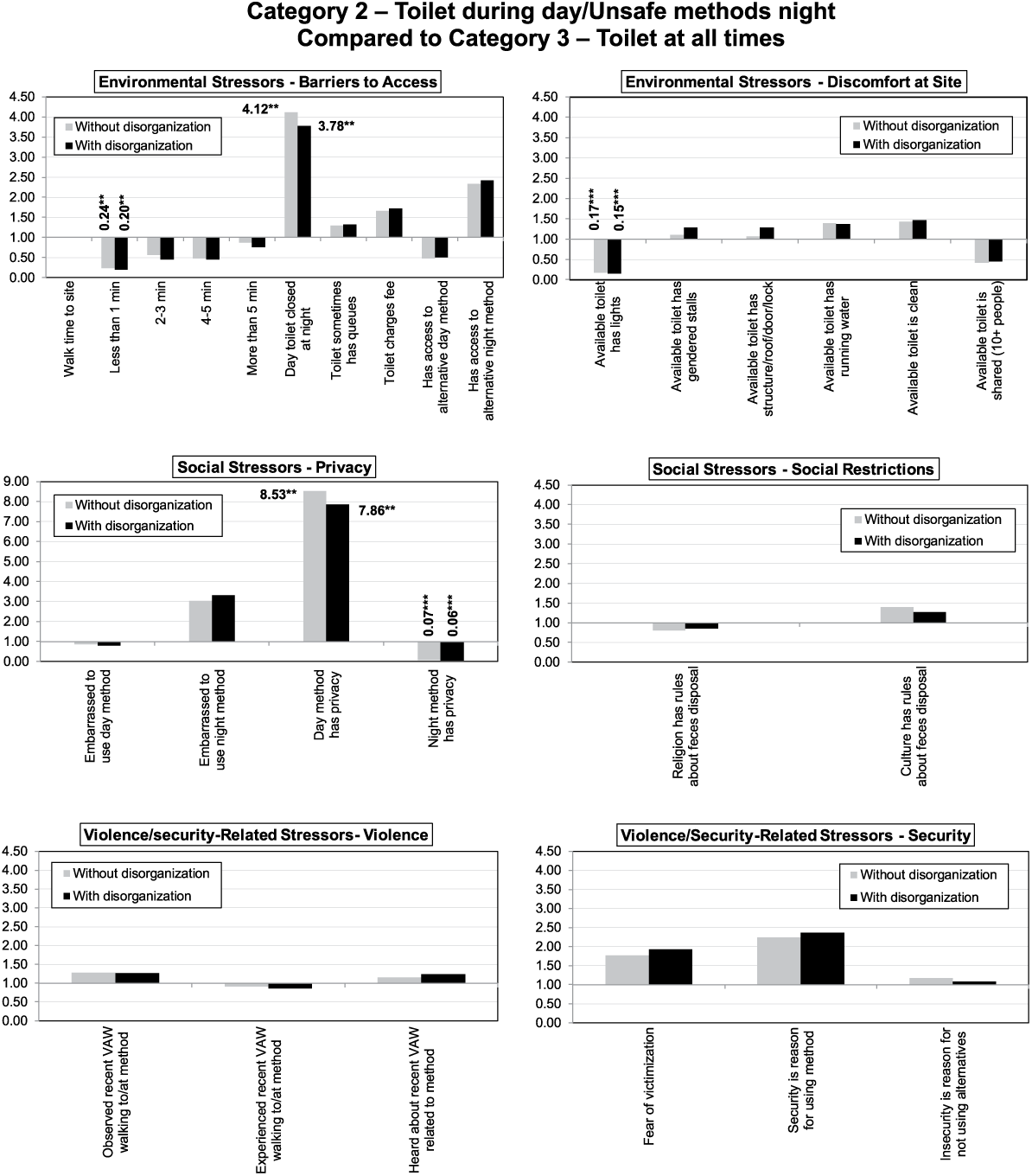
Associations (relative risk ratios) between sanitation-related stressors and Sanitation Utilization Category 2 (compared to Category 3) with and without neighborhood disorganization as a moderator.
The first thing to notice in Model 2 (includes Level-2 variable for neighborhood disorganization) is that the ICC (Ene, Leighton, Blue, & Bell, 2015) for women in Category 1 (those utilizing bags/buckets/OD in or near the home at all times), compared with those in Category 3 (those using toilets for all sanitation needs), was 87.6%—suggesting that most of the variance in the women’s sanitation utilization was accounted for by differences in women’s perceptions of neighborhood disorganization within their community. For women in Category 2 (women who utilize toilets during the day and buckets/bags/OD in or near the home for urination and/or defecation during the night), compared with those in Category 3, the ICC was only 4.1%, that is, for women in Category 2, compared with women in Category 3, only 4.1% of the variance in women’s sanitation utilization could be accounted for by differences in women’s perceptions of neighborhood disorganization. These findings suggest that the role of women’s perceptions of neighborhood disorganization was particularly important for women who use bags/buckets/OD for all or most of their sanitation needs (Category 1) compared with women who use a toilet for all of their sanitation needs (Category 3), but is probably less important for women who have access to a toilet during the day and, for some of them, during the night for urination as well (Category 2).
Figure 7 (Category 1 compared with Category 3) and Figure 8 (Category 2 compared with Category 3) provide visual summaries of the associations (RRRs) between women’s sanitation-related stressors and their sanitation utilization with (gray bars) and without (black bars) neighborhood disorganization as a moderator. As the role of women’s perceived level of neighborhood disorganization seems particularly important for women in Category 1 (Figure 7), only comparisons of the Category 1 stressors across Models 1 and 2 will be described here in the results. One of the key findings is that women’s fear of sanitation-related victimization, which is nonsignificant at the p < .05 level in the fixed effects model (Model 1), is not only significant (p < .05) in the random effects model (Model 2) but also has a higher RRR (2.6 in Model 1 and 3.8 in Model 2). Namely, when we account for differences in women’s perceptions of neighborhood disorganization, women who fear sanitation-related victimization have over 3.5 times the risk of using bags/buckets/OD in or near the home for all urination and defecation during the night and for urination and/or defecation during the day compared with utilizing a toilet for all urination/defecation needs.
In addition, the relative risk of women identifying security as the primary reason for using their current methods for urination/defecation is higher in Model 2 (RRRrandom = 20.3, p < .001) than in Model 1 (RRRfixed = 10.2, p < .001). This may suggest that, for women who have higher perceptions of neighborhood disorganization, security may be associated with women utilizing bags/buckets/OD in or near the home for all or most of their daily and nightly sanitation needs compared with utilizing a toilet, especially if that toilet is outside the home. On the contrary, results from Figure 7 suggest an opposite effect for stressors such as access to an alternative nighttime facility (RRRrandom = 4.8, p < .05 compared with RRRfixed = 6.2, p < .01), feeling embarrassed using the daytime method/facility (RRRrandom = 7.7, p < .05 compared with RRRfixed = 8.6, p < .01) or nighttime (RRRrandom = 4.2, p = .096 compared with RRRfixed = 7.5, p < .01), and privacy during the daytime (RRRrandom = 1.7, p = .536 compared with RRRfixed = 5.3, p < .05). For women who have higher perceptions of neighborhood disorganization, stressors like having an alternative nighttime facility, embarrassment about using a certain facility/method of disposal, and privacy using that facility/method of disposal during the day are associated with lower relative risk for women in Category 1 (those who use mostly unsafe methods for all or most urine/feces disposal during the day and for all calls during the night) compared with women in Category 3 (those who utilize toilets for all calls).
Discussion
A number of studies have recently expressed the importance of looking at factors that influence people’s ability to access and utilize sanitation beyond the individual level (Dreibelbis et al., 2013). Researchers like McFarlane, Desai, and Graham (2014), O’Reilly (2010, 2012, 2016), Khanna and Das (2016), Jewitt (2011), and D. Joshi, Fawcett, and Mannan (2011), in particular, recognize the important role of context, ecology, geography, and environment—political, social, and economic—in understanding people’s ability to access, adopt, utilize, or build sanitation, especially for vulnerable populations. Many have acknowledged the link between women’s lack of access to adequate sanitation and their risk of exposure to violence (Amnesty International, 2010; Gosling, Irvine, Schechtman, & Velleman, 2015; Khosla, 2000; O’Reilly, 2016; Sahoo et al., 2015; Sommer et al., 2014). Yet, for the most part, sanitation and water provision have been largely divorced from issues of community-level disorganization and security in empirical studies. Findings from this study suggest that neighborhood disorganization is, in fact, inextricably linked to women’s daily sanitation behaviors and the stressors that are associated with those behaviors. In this study, higher levels of perceived neighborhood disorganization explained a large amount of the variance (almost 88%) in women’s sanitation behaviors, particularly for women using bags, buckets, or OD in or near their homes for the majority of their daily and nightly sanitation needs (Category 1).
Urban planners, criminologists, and even sociologists who study sexual assault have, for a long time, understood the link between neighborhood variables such as social and environmental disorder and social efficacy and rates of crime, violence, and, relatedly, police and political intervention. Social disorganization and “broken windows” theorists, for example, have adamantly contended that there is a relationship between the physical (e.g., litter, vandalism, stray animals) and social order (e.g., idle youth, drugs/alcohol abuse, violence) of a community and the rates of crime in that community (Markowitz et al., 2001; Sampson & Groves, 1989; Sampson, Morenoff, & Gannon-Rowley, 2002; Sampson, Raudenbush, & Earls, 1997; Uthman, 2010). Studies have even drawn specific links between neighborhood disorganization and rates of violent offending and victimization in Nairobi informal settlements (Parks, 2014). The goal of this study was not to look at direct associations between neighborhood disorganization and women’s sanitation behaviors, but, rather, to explore how women’s perceptions of neighborhood disorganization may moderate associations between previously identified sanitation-related stressors and their sanitation practices. For example, would certain stressors, such as fear of sanitation-related victimization and hours of operation of a toilet or toilet security, be more important for women who perceive their communities to be highly disorganized? Or, by contrast, would certain stressors, such as the embarrassment a woman feels when using her primary means of urination/defecation, be less important for women who perceive their communities to be highly disorganized?
Findings from this analysis suggest that women’s perceptions of neighborhood disorganization do modify the relationship between a number of stressors and their sanitation utilization behaviors. For women who perceived their neighborhoods to be highly disorganized, fear of sanitation-related victimization, having to pay a fee to utilize the toilet, limited hours of operation of the toilet, and security, for example, were particularly important stressors. In addition, the issue of lack of privacy at night is seemingly exacerbated when women perceive their neighborhoods to be highly disorganized. These results seem plausible in light of sanitation literature that suggests that these stressors are especially challenging for women in informal settlements when trying to access sanitation at night (Amnesty International, 2010; D. Joshi et al., 2011; Khanna & Das, 2016; O’Reilly, 2016; Prabhakaran, Kar, Mehta, & Chowdhury, 2016) or during times of menstruation (Lahme & Stern, 2017; Sumpter & Torondel, 2013; van Eijk et al., 2016). This analysis provides more context for these findings—highlighting the magnitude of these daily sanitation-related stressors in settings where women perceive crime, violence, and disarray to be predominant characteristics of their communities. In some respects, it links to Nussbaum’s (2005) notion of women’s diminished capabilities, for example, the inability to access sanitation in an “atmosphere of threat” (p. 167). It raises the question, even if a woman has access to a toilet facility, such as a public facility, “Will she use it if she perceives her environment to be disorganized or violent?” A number of studies have highlighted a flaw in early assumptions that the accessibility of toilets, for example, the availability of any toilet, no matter the design or distance from a person’s home, is the key to the persistently high populations without access to sanitation (O’Reilly, 2016; Sommer et al., 2014). Findings from this study complement these contentions—suggesting that interventions and policies focused on availability of toilets alone will hardly be adequate or effective, particularly for women living in informal settlements.
This study also highlights a need for more interdisciplinary approaches and a broadening of perspective on exploring issues related to sanitation access and utilization, particularly for vulnerable populations living in highly disorganized communities. With the exception of a few researchers (Parks, 2014; Uthman, 2010; Uthman & Kongnyuy, 2008), for example, neighborhood disorganization studies have been carried out on data collected from mostly poor, inner-city communities in the United States or the United Kingdom. Consequently, these too have seemingly failed to recognize the link between the more traditional definitions of neighborhood disorganization and service provision, for example, the presence or absence of basic services such as toilets, piped water and sewerage, and water and sewage treatment. In LMICs, poverty and community disorganization go hand-in-hand with lack of access to basic services. More than issues of vandalism, litter, stray animals, and/or traffic problems (factors commonly used in neighborhood disorganization measures; Gau & Pratt, 2008, 2010), areas of extreme poverty and disorganization in informal settlements are often characterized by their lack of formal services and structures, particularly sanitation (Greed, 2015; A. Joshi, Prasad, Kasav, Segan, & Singh, 2013; D. Joshi et al., 2011; McFarlane et al., 2014; Prabhakaran et al., 2016). This lack of recognition of the link between neighborhood disorganization, violence, women’s sanitation-related stressors, and sanitation practices and behaviors in LMIC settings needs to be rectified. Perhaps, for example, neighborhood disorganization scales should be redesigned to include lack of basic services and, subsequently, be taken into account when looking at issues and interventions related to sanitation in informal settlements of developing countries.
While the results of this study provided an interesting and, perhaps broader, more interdisciplinary perspective on women’s ability to access and utilize sanitation, particularly in informal settlements, it was not without limitations. Perhaps the biggest limitation of the study is that it was carried out using cross-sectional data, which makes it impossible to make causal or temporal claims about the relationships between sanitation-related stressors and women’s sanitation practices and the role of women’s perceptions of neighborhood disorganization in that relationship. Is it neighborhood disorganization that leads to women’s perceptions of violence, disarray, and/or crime, which, in turn, change the magnitude or relevance of certain sanitation-related stressors and lead to a change in sanitation behavior, or are the arrows that link these various factors changing direction? Another limitation of the study is the lack of community-level measures in the model. In addition to temporal variables, it would be ideal to incorporate not only women’s perceptions of neighborhood disorganization but also community- and neighborhood-level measures of disorganization into future studies. Finally, at the time of this study, there were no validated measures of women’s sanitation-related stress and this study only captures information from one point in time; thus, mono-operation bias is a potential threat to the construct validity of our measures of sanitation-related stress, that is, the items used to measure sanitation-related stress in this study may not capture the full breadth of women’s sanitation-related stress in this environment or others.
Conclusion
Findings from this study could have meaningful implications for sanitation researchers as well as policy makers and developers. This study marked the first attempt to qualitatively and quantitatively explore the role of neighborhood disorganization in the constellation of stressors commonly associated with women’s sanitation behaviors in informal settlements. The theory and methodology used in this study highlight the need for more conversations, studies, and interventions that apply a truly interdisciplinary lens to developing strategies to explore, regulate, and solve the world’s persistent sanitation crisis. This is not the first study to recognize the importance of social, spatial, and environmental context. In fact, many qualitative studies coming out of anthropology and geography have drawn attention to the important role of context. However, this is the first study to try to combine sanitation and non-sanitation-related theories to study the role of neighborhood context, for example, neighborhood disorganization, in the relationship between women’s sanitation-related stressors and their behaviors. The results from the study suggest that neighborhood disorganization may, in fact, play a very important role in introducing new stressors or changing the overall direction or importance of the more familiar stressors on women’s sanitation behaviors in informal settlements. These findings, for example, should push policy makers and developers to broaden their approach to sanitation—looking perhaps at the overall context of each settlement neighborhood and developing strategies to encourage social cohesion and organization among residents in informal settlements. In addition, findings from this study emphasize the need for women-centered approaches to sanitation policy and development. Finally, this study highlights the inextricable link between neighborhood disorganization, women’s fear of violence, and sanitation behaviors in Mathare. This finding may suggest that sanitation-oriented interventions and policies should be integrated with those relating to policing, security, organization, and cohesion rather than treated as distinct areas of concern in creating healthy environments for women.
Supplemental Material
Appendix_A_and_B – Supplemental material for Neighborhood Disorganization and Women’s Sanitation Utilization Practices in Mathare Valley, Kenya
Supplemental material, Appendix_A_and_B for Neighborhood Disorganization and Women’s Sanitation Utilization Practices in Mathare Valley, Kenya by Samantha Winter, Francis Barchi and Millicent Ningoma Dzombo in Environment and Behavior
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.