
Abstract
In this, study, the authors examined the moderating effects of partnership on the relationship between services and supports adequacy and family quality of life (FQOL) for families of children with deaf-blindness ages birth to 21. A social-ecological approach enabled examining the impact of disability on the family system. A survey, consisting of four measures, was completed by 227 parents of children with deaf-blindness. Results suggest that FQOL for families of children with deaf-blindness is explained, in part, by satisfaction with the adequacy of friend and family supports and child-care services. Satisfaction with partnership also significantly predicted FQOL for these families. Significant interaction effects indicated that the relationships (a) between education services adequacy and FQOL and (b) between related services adequacy and FQOL are dependent on satisfaction with partnership. Implications for research and practice are discussed.
Family quality of life (FQOL) is “a dynamic sense of well-being of the family, collectively and subjectively defined and informed by its members, in which individual and family-level needs interact” (Zuna, Summers, Turnbull, Hu, & Xu, 2010, p. 262). Research on families affected by disability is shifting away from examining the negative impact of disability on family life. Focusing on FQOL is an integral part of the movement from a deficit to a positive perspective (Chiu, Kyzar, et al., 2013). The presence of disability in the family system affects multiple aspects of family life, including family interaction, functioning, and life span (Turnbull, Turnbull, Erwin, Soodak, & Shogren, 2015). FQOL is sensitive to this multifaceted impact (Kober & Eggleton, 2009) and has been identified by families and service providers as an important outcome for services (Dunst & Bruder, 2002).
Zuna et al. (2010) defined services as “a range of educational, social, and health-related activities expected to improve outcomes for the individual or family as a whole” and supports as “less tangible resources provided to the individual or to the whole family which are expected to improve outcomes for the individual or family” (p. 15). Thus, services tend to be formally delivered by professionals, and supports tend to be informally delivered by family and friends. Although family research in the disability field has documented families’ unmet needs (Almasri et al., 2011; Chiu, Turnbull, & Summers, 2013) and perceptions of services and supports adequacy (Bitterman, Daley, Misra, Carlson, & Markowitz, 2008; Vohra, Madhaven, Sambamoorthi, & St Peter, 2014), very little research has linked perceptions of services and supports adequacy to holistic family outcomes, such as FQOL. Further, of the research that has linked families’ perceptions of services and supports to outcomes, the focus has been on supports rather than formal services (Kyzar, Turnbull, Summers, & Gómez, 2012).
The presence of disability in the family system affects multiple aspects of family life, including family interaction, functioning, and life span.
The scant research that does examine the relationship of services adequacy to holistic family outcomes indicates that services adequacy predicts outcomes such as FQOL and that satisfaction with family–professional partnership, hereafter referred to as partnership, is also a key variable influencing that relationship. Epley, Summers, and Turnbull (2011) examined the relationship between families’ perceptions of needs, adequacy of received services, and outcomes for families in early intervention (Part C) services. They found a path relationship in which immediate outcomes of service provision (as measured by the Office of Special Education Programs family outcomes) predicted FQOL when controlling for degree of unmet needs and parent ratings of Part C early intervention services adequacy. These findings suggest that parents’ ratings of early intervention services adequacy may be related to both immediate and broader family outcomes. Similarly, Summers et al. (2007) examined the association between early intervention and early childhood special education services adequacy and FQOL and found a positive correlation between ratings of services adequacy and FQOL. Summers and colleagues also found that families’ satisfaction with partnership was a partial mediator of the effects of services adequacy on FQOL, suggesting that “the quality of relationships with professionals is also a critical component of effective service models” (Summers et al., 2007, p. 334).
Other research examining the link between family-centered services and family outcomes has identified (a) a correlation between family-centered service delivery and FQOL (Davis & Gavidia-Payne, 2009) and (b) partnership as a key variable, particularly, partnerships that are characterized as including participatory practices in addition to relationship practices (Dempsey & Keen, 2008; Dunst, Trivette, & Hamby, 2007). This research, however, is limited by samples that, for the large part, include families of young children with mild disabilities.
The present study reports the relationship of service provision to family outcomes for one specific subset of families experiencing disability: families of children with deaf-blindness. The Individuals With Disabilities Education Act (IDEA; 2013) defines deaf-blindness as “concomitant hearing and visual impairments, the combination of which causes such severe communication and other developmental and educational needs that they cannot be accommodated in special education programs solely for children with deafness or children with blindness” (34 C.F.R. § 300.8[c][2]). According to the National Consortium on Deaf-Blindness (NCDB; 2014), there were 9,454 children and youth with deaf-blindness in the United States in 2013, 43% of whom had four or more additional disabilities. Malloy and Killoran (2007) documented that over 90% of children and youth with deaf-blindness have one or more additional disabilities. On the whole, families of children with deaf-blindness access a wide variety of services and supports to address both child and family outcomes.
Our study utilized data from a larger research project examining service provision and FQOL for families of children with deaf-blindness. In Kyzar and Summers’ (2014) study of services and supports utilization and satisfaction for families of children with deaf-blindness, participants reported high levels of use of friend and family support, education services, and related services. They reported lowest levels of use of mental health services and intervener services (i.e., related service providers who provide consistent one-on-one support to aid the student in communicating with and accessing his or her environment; NCDB, 2013). Kyzar and Summers found that although families of children with deaf-blindness were accessing a large number of services, on the whole they were only moderately satisfied with them.
Other studies of families of children with deaf-blindness have examined sibling relationships (Heller, Gallagher, & Frederick, 1999), grandparent involvement in communication development (Shaw, 2005), and the effect of coaching on mothers’ interactions with their child with deaf-blindness (Janssen, Riksen-Walraven, van Dijk, & Ruijssensars, 2010). Štěrbová and Kudláček (2014) examined mothers’ perspectives about leisure-time physical activities for their children with deaf-blindness—needs, barriers, and beliefs—and found that access to specialized programming, adaptive equipment, and family supports facilitated participation in these activities. Dammeyer (2010) found that families’ access to a network of professionals and other parents of children with deaf-blindness influenced child outcomes. Overall, current knowledge from the research literature on families of children with deaf-blindness includes a wide range of purposes and findings that lack both depth and breadth in informing future research and practice. Moreover, no study to date has quantitatively examined the relationship of services and supports to family outcomes for families of children with deaf-blindness.
Current knowledge from the research literature on families of children with deaf-blindness includes a wide range of purposes and findings that lack both depth and breadth in informing future research and practice.
The current study extends Kyzar and Summers’ (2014) findings by linking parents’ ratings of services and supports adequacy to their FQOL. In addition, given the literature suggesting that satisfaction with partnership is a key variable in understanding how services and supports adequacy are related to FQOL, we also examined the potential moderating effects of partnership. Our study fills a gap in the current literature on services and supports adequacy, FQOL, and partnership by focusing on (a) families of children with disabilities across a broader age span (birth to age 21) and (b) families of children with severe and multiple disabilities. The research question guiding this study was, What are the effects of perceived services and supports adequacy and satisfaction with partnership on FQOL?
Method
We utilized a survey research design for this study. Participants were primary caregivers of children who were identified as deaf-blind based on federal or state deaf-blind certification guidelines (34 C.F.R. § 396.4 [1]–[3]). Deaf-blind censuses are maintained at the state level by federally funded state deaf-blind technical assistance projects. To recruit participants, we contacted the project directors and family specialists associated with each of the 53 state projects, provided a description of the study, and requested that project personnel distribute the survey to families. In all, 16 state projects distributed 2,028 surveys (188 electronic, distributed link via e-mail; 1,840 paper, distributed via U.S. mail or at scheduled events). We received in return 227 surveys, a response rate of 11.2%.
Participants (N = 227) were caregivers of children and youth with deaf-blindness. The majority of the participants were female (90.3%), were White (78.9%), and described themselves as the parent (93.8%). Approximately 9% identified themselves as Hispanic or Latino, and 8.4% identified themselves as Black or African American. The remaining 3.4% identified themselves as either American Indian, Alaskan Native, or Asian or Pacific Islander (1.8%). Seventy-four percent of the participants were married or living with a partner, and about half (53.8%) held a degree post-high school. Approximately 20% of the sample reported earning less than $19,999 in the prior 12 months, 33.9% of the participants’ incomes fell within the range of $20,000 and $59,999, and the remaining 41% reported an income greater than $60,000. We dummy-coded income into two groups by collapsing those who reported an income of $49,999 or less (37.0%) and those who reported an income of $50,000 or greater (58.1%) based on U.S. Census Bureau (2010) data on median family income during the year of data collection (i.e., 2009). Thirty percent reported living in an urban area, 39.2% lived in a suburban area, and 28.2% lived in a rural area.
Participants identified their primary professional partner—that is, the professional who worked with their child the most over the past 6 months. The frequencies of primary professional partners identified by participants were: education service provider (e.g., special education teacher, teacher of the deaf or hard of hearing or visually impaired; 40.5%), related service provider (including interveners; 22.5%), health care provider (14.5%), child-care provider (5.7%), and service coordinator (4.8%). Participants reported any disabilities the child with deaf-blindness had in addition to dual sensory impairment. Only five participants (2.2%) noted that their children had no additional disability. The most frequently cited co-occurring disabilities were speech or language impairment (81.5%), developmental delay (79.9%), and physical disability (67.8%). Eight percent of the children were between the ages of birth and 2, 32.2% were between the ages of 3 and 8 years, 28.6% were between the ages of 9 and 14 years, 19.4% were between the ages of 15 and 18 years, and 9.7% were between the ages of 19 and 22 years.
Data Collection
After obtaining institutional review board approval, we sent the survey packets to participating state project directors to distribute to all families of children certified as deaf-blind in their state. Families completing the paper version returned a signed and dated consent form along with their completed survey directly to the first author using a provided business-reply envelope. We entered completed surveys into a SNAP Surveys software (Version 9) database and subsequently exported them to SPSS (Version 17.0) for analysis along with the electronic surveys.
Measures
Services and Supports Adequacy Survey–Deaf-Blind (SSAS-DB)
The SSAS-DB is a 52-item self-administered questionnaire that assesses families’ perceptions of how well services and supports adequately met their child and family needs during the 12 months prior to completion of the survey. Table 1 reports the seven domains included on the SSAS-DB and the items associated with each domain. A did not use option is available as well as an option to rate an other service or support that respondents define in an open-text box field.
Services and Supports Adequacy Survey–Deaf-Blind (SSAS-DB) Domain and Items.
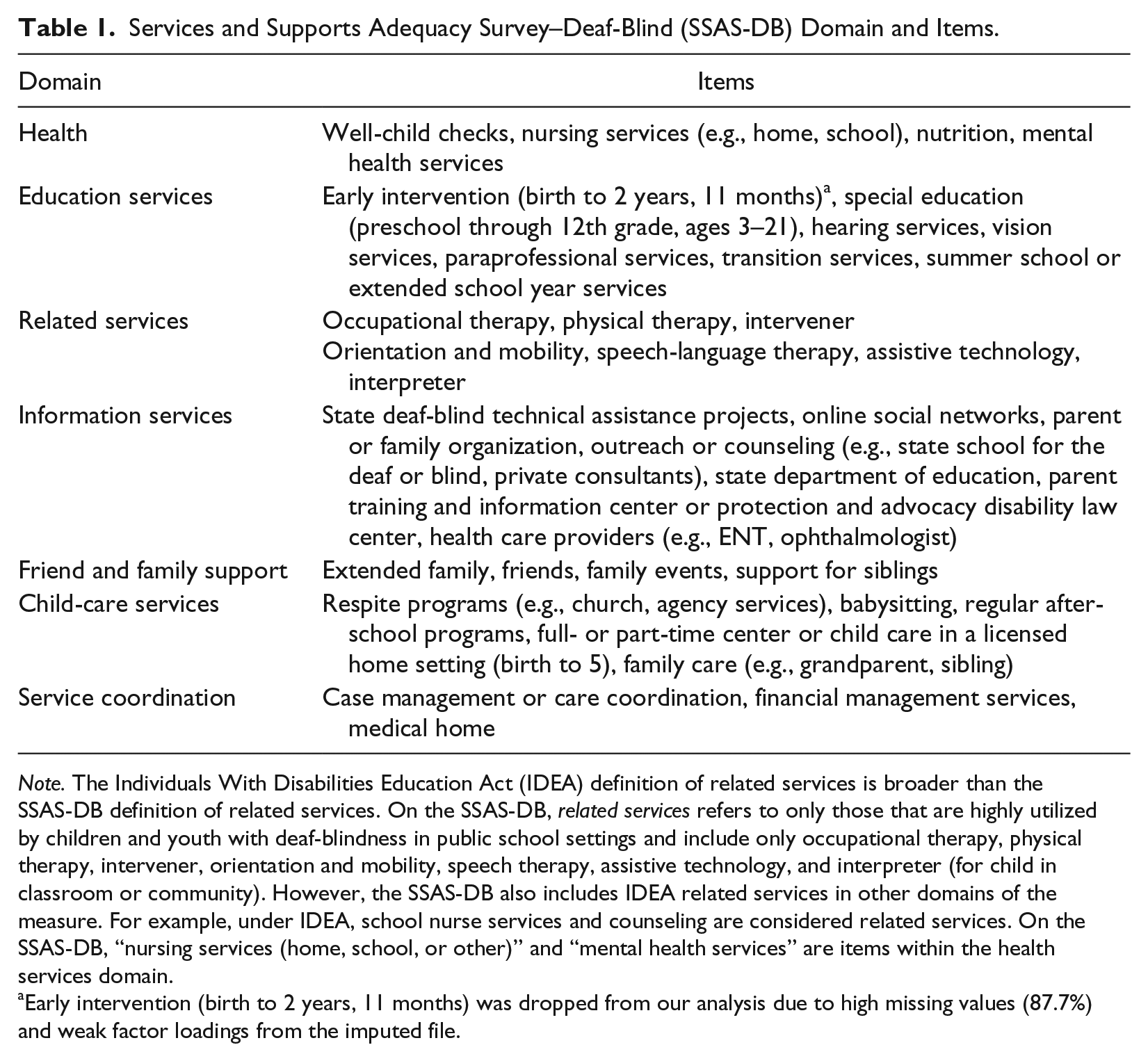
Note. The Individuals With Disabilities Education Act (IDEA) definition of related services is broader than the SSAS-DB definition of related services. On the SSAS-DB, related services refers to only those that are highly utilized by children and youth with deaf-blindness in public school settings and include only occupational therapy, physical therapy, intervener, orientation and mobility, speech therapy, assistive technology, and interpreter (for child in classroom or community). However, the SSAS-DB also includes IDEA related services in other domains of the measure. For example, under IDEA, school nurse services and counseling are considered related services. On the SSAS-DB, “nursing services (home, school, or other)” and “mental health services” are items within the health services domain.
Early intervention (birth to 2 years, 11 months) was dropped from our analysis due to high missing values (87.7%) and weak factor loadings from the imputed file.
We carried out expert review and pilot testing of the SSAS-DB utilizing cognitive interviewing techniques (Gray, Blake, & Campanelli, 2014). For a full description of the development of the SSAS-DB, see Kyzar and Summers (2014).
We conducted a factor analysis with varimax rotation on each of the seven categories to examine reliability of the SSAS-DB items. Factors with eigenvalues greater than 1.00 were retained. Items with factor loadings less than .300 and items that loaded on multiple factors were considered for removal. We dropped two items from the analysis due to weak factor loadings: early intervention (birth to 2 years, 11 months) and regular after-school programs. The analyses revealed that each subscale loaded onto one factor. The mean total variance of each factor analysis accounted for 59.11% to 75.80% of each SSAS-DB category. Because the internal consistencies of each SSAS-DB category were strong (αs ranged from .754 to .920), mean scores were calculated based upon the retained items from each of the seven SSAS-DB categories (rs ranged from .348–.713; ps < .001).
Beach Center on Disability Family Quality of Life Scale (FQOL Scale)
The FQOL Scale assesses families’ perceived satisfaction with their quality of life in 21 items across four domains: (a) family interaction, (b) parenting, (c) emotional well-being, and (d) physical or material well-being. Participants report their satisfaction with their quality of life on a 5-point scale, which ranges from 1 = very dissatisfied to 5 = very satisfied.
Studies establishing the reliability and validity of the FQOL Scale (e.g., Hoffman, Marquis, Poston, Summers, & Turnbull, 2006; Zuna, Selig, Summers, & Turnbull, 2009) have included samples of families whose children primarily have mild or moderate disabilities. To evaluate the psychometric properties of the FQOL Scale with families of children with deaf-blindness, we conducted an exploratory factor analysis utilizing the principal axis factoring method with promax rotation. Results suggested three factors—parenting (12 items; Cronbach’s α = .931), emotional well-being (four items; Cronbach’s α = .855), and physical or material well-being (five items; Cronbach’s α = .788)—that together accounted for 58.6% of the variance in FQOL. The overall scale, with 21 items, had excellent internal consistency (Cronbach’s α = .940).
Beach Center on Disability Family–Professional Partnership Scale (Partnership Scale)
The Partnership Scale is an 18-item measure that assesses families’ satisfaction with their relationship with the primary professional serving their child and family on a 5-point scale (1 = very dissatisfied to 5 = very satisfied). Participants identify one service provider—the service provider who has worked with the child the most over the past 6 months—and rate all items on the Partnership Scale according to their experiences with this specific service provider. Participants can choose from the various service provider options (i.e., health care provider; education service provider; related services provider, including intervener; child-care provider; service coordinator) or specify an other service provider category in an open-ended text field. Summers and colleagues (2005) reported that the overall measure, which includes two subscales (Child-Focused Relationships and Family-Focused Relationships), have excellent unidimensional and internal consistency (overall measure, Cronbach’s α = .96; Child-Focused Relationships, Cronbach’s α = .94; Family-Focused Relationships, Cronbach’s α = .92). We conducted a factor analysis on the Partnership Scale with this sample utilizing the principal axis factoring extraction method with promax rotation. Results were similar to previously reported factor structures (Summers et al., 2005). The resulting two factors strongly correlated with each other (r = .789), and the overall measure, totaling 18 items, had excellent internal consistency (Cronbach’s α = .973).
Data Analysis
Of the 227 returned surveys, 129 were incomplete (56.83%), amounting to a total of 3.60% missing data from the SSAS-DB in the data set. Given that the data were missing completely at random (MCAR test, p = .813) and that total missing data were less than 5%, we used single imputation using the expectation-maximization (EM) algorithm to treat missing values on all SSAS-DB items (Little, 1988; Rubin, 1987). We ran all analyses on the original data set with missing values and found consistency with analyses run on the imputed data set. Therefore, we report the results using the imputed values for SSAS-DB items. For the primary analysis, we conducted a multiple linear regression on FQOL scores by entering predictors into the model sequentially to determine whether each block of predictors significantly increased the total variance explained by the model. Because marital status and income have been shown to have separate effects on FQOL (Wang et al., 2004; Wheeler, Skinner, & Bailey, 2008), we entered these variables into the first step of the analysis as dummy-coded covariates (married vs. not married; income equal to or less than vs. more than $50,000 per year).
To examine the potential effects of differing primary professional partners on the study findings, we recoded the original five primary partner categories into two levels. The first level, instructional service provider (46.3%), included the primary partner categories that deliver instructional services, which were education service provider and child-care provider. The second level included all other services (48.5%): health care provider, related service provider (including interveners), and service coordinator. Primary professional partner (instructional service provider or other) was also entered into the first step of the analysis as a dummy-coded covariate to control for potential effects of the different types of professionals with whom parents in this study reported working most with their child over the past 6 months. We entered partnership (centered) into the second step and the seven SSAS-DB scores into the third step (centered). To examine whether FQOL varied as a function of services and supports adequacy and partnership, we entered the two-way interactions of partnership by each of the seven SSAS-DB scores in the fourth step (see Aiken & West, 1991). We examined significant interactions further with simple slope tests to assess the nature of moderating relationships (Rosenthal & Rosnow, 1985).
Results
Upon initial examination of the results, the inclusion of the seven separate interaction terms did not significantly increase the percentage of variance accounted for by the model, △R2 = .035, F(7, 180) = 1.47, p = .180. To improve parsimony, we dropped nonsignificant interactions from the fourth step of the model, which improved the percentage of variance accounted for by the model in the fourth step, △R2 = .025, F(2, 185) = 3.78, p = .025. Overall, the predictors accounted for 38.6% of the total variance in the final model (see Table 2).
Summary of Multiple Regression Analysis for Variables Predicting FQOL (N = 198).
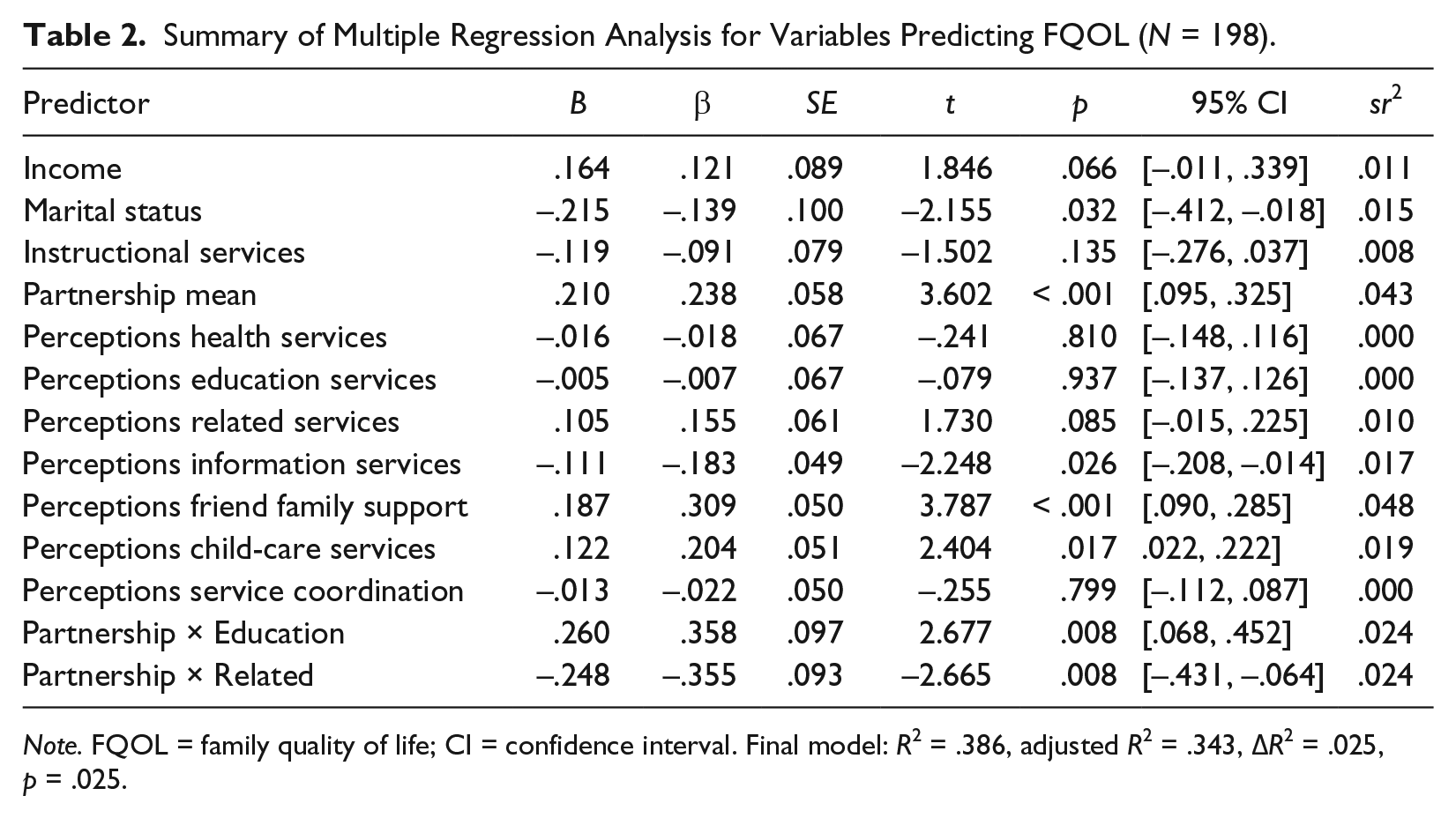
Note. FQOL = family quality of life; CI = confidence interval. Final model: R2 = .386, adjusted R2 = .343, △R2 = .025, p = .025.
Marital status significantly predicted FQOL, such that not being married predicted a decrease in FQOL, β = −.129, t(185) = −2.16, p = .032. There was also a significant effect found for partnership, β = .238, t(185) = 3.60, p < .001, suggesting that as families’ satisfaction with partnership increased, FQOL also increased (see Table 2). We also found main effects for friend and family supports adequacy, β = .309, t(185) = 3.79, p < .001, and child-care services adequacy, β = .214, t(185) = 2.40, p = .017, indicating that as friend and family supports adequacy and child-care services adequacy increased, FQOL also increased. Further, we found a significant main effect for information services, β = −.183, t(185) = −2.25, p = .026, suggesting that as information services adequacy increased, FQOL decreased. Finally, we found significant interactions for Partnership × Education Services Adequacy, β = .358, t(185) = 2.68, p = .008, as well as Partnership × Related Services Adequacy, β = −.355, t(194) = −2.67, p = .008 (see Figure 1). We conducted simple slope tests to examine the relationships with FQOL at one standard deviation above and below the mean for partnership, education services adequacy, and related services adequacy (Rosenthal & Rosnow, 1985). The results revealed that at high levels of partnership satisfaction, higher levels of perceptions of educational services adequacy predicted higher levels of FQOL, β = .247, t(185) = 2.13, p = .034. This linear relationship was not present at low levels of partnership satisfaction, p = .068. In addition, at low levels of partnership satisfaction, higher levels of perceptions of related services adequacy predicted higher levels of FQOL, β =.424, t(185) = 2.92, p = .004. This relationship was not present at high levels of partnership, p = .363. These results suggest that satisfaction with partnership moderates the relationship between perceptions of services and supports adequacy and FQOL.
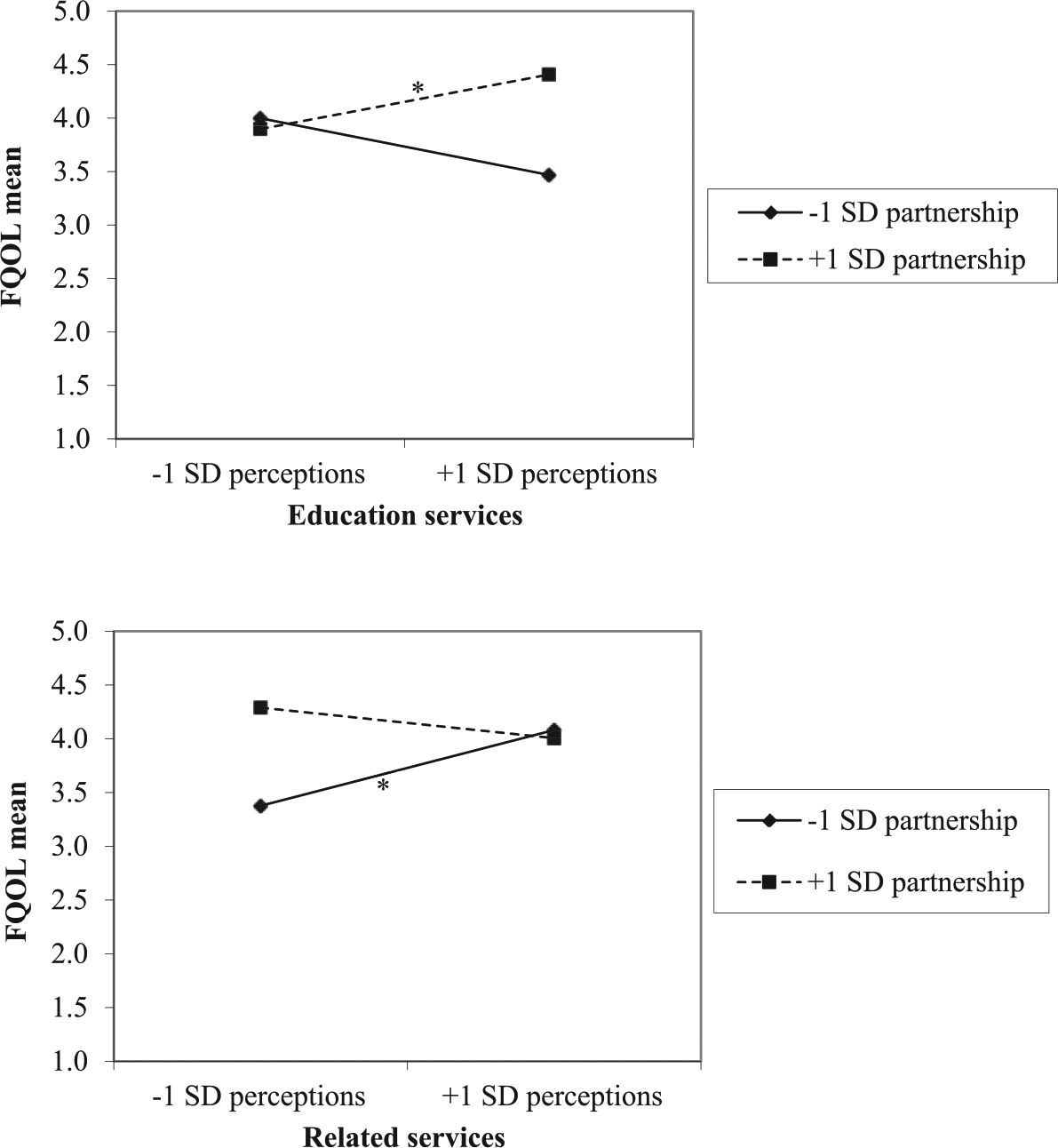
Relationship between Family Quality of Life (FQOL) scores and perceptions of education and related services as moderated by satisfaction with partnership. Partnership, education, and service adequacy scores are displayed at one standard deviation above and below the mean. *Slope differs significantly from zero, p < .05.
Discussion
In this study, we examined the relationship of services and supports adequacy, partnership, and FQOL for families of children with deaf-blindness. This study is unique in its examination of families of children with deaf-blindness, joining only a few others that have reported outcomes related to services and supports for this population (e.g., Dammeyer, 2010; Heller et al., 1999). Additionally, although previous research has documented that services and supports adequacy and partnership are each separately correlated with family outcomes, such as FQOL, few studies have examined how these independent variables interact to explain FQOL. No study has undertaken this examination specifically for families of children with deaf-blindness.
The results of this study indicate that satisfaction with partnership predicts FQOL for families of children who are deaf-blind. Although partnership is considered to be a crucial element of family-centered practice (Reschly & Christenson, 2012), scant research exists that links partnership to outcomes for families of children with disabilities. Burke and Hodapp (2014) are among the few. Their findings indicated that mothers of children with developmental disabilities who reported excellent partnerships with professionals experienced significantly less stress. Mothers who rated schools as often or very often engaging in practices aligned with items in the Partnership Scale used in this study (e.g., treating their child respectfully, having the skills to help their child succeed) experienced less stress than mothers of children who reported that the school did these things sometimes or occasionally.
In addition to documenting the main effects of services and supports adequacy and partnership on FQOL in isolation, we were also interested in understanding how these two variables interacted to predict FQOL. In our study, when satisfaction with partnership decreased, there was a positive relationship between related services adequacy and FQOL, suggesting that high levels of related services adequacy buffered the effects of low perceptions of partnership on FQOL. The interaction between education services adequacy and partnership, however, had a different pattern of effect. When partnership satisfaction increased, there was a positive relationship between education services adequacy and FQOL, suggesting that partnership and education service adequacy were both related to higher FQOL. These interaction effects occurred while controlling for the effects of marital status, income, and different primary professional partners on FQOL. Neither education services adequacy nor related services adequacy was correlated with FQOL. Therefore, it appears that partnership satisfaction was the key variable driving the effects. The finding that high perceptions of both education service adequacy and partnership are needed for families’ FQOL points to the integral role partnership has within the context of education services for students with deaf-blindness.
The finding that high perceptions of both education service adequacy and partnership are needed for families’ FQOL points to the integral role partnership has.
Although it may be reasonable to assume that high-quality schools yield high-quality outcomes overall, there are a number of issues facing any school—high or low quality—in educating students with deaf-blindness. There are documented shortages of teachers who have any level of pre- or in-service professional development specific to deaf-blindness (Office of Postsecondary Education, 2013; U.S. Department of Education, 2014). Bruce (2007) reported that only 10 out of 1,200 teacher preparation programs nationwide offered courses specific to deaf-blindness; these programs graduated only 32 teachers in the 2003–2004 year. Additionally, due to the methodological limitations inherent in studying a low-incidence population, “promising” research-based instructional practices specific to deaf-blindness (e.g., Brady & Bashinski, 2009) are not the same as evidence-based practices. Therefore, educators within school settings are also limited in the knowledge they are able to access from research about teaching students with deaf-blindness. These workforce challenges are magnified by the documented increases of students with deaf-blindness being educated in inclusive settings (NCDB, 2014). In all, it is not clear that the “information, resources, and access to expertise in deaf-blindness” (NCDB, 2014, p. 6) necessary to address the specific needs of students with dual sensory impairments are available to teachers in local schools (Szymanski, Lutz, Shahan, & Gala, 2013).
The use of interveners as a related service shows promise in bridging the knowledge gap related to deaf-blindness expertise within schools (Chen, Alsop, & Minor, 2000), and intervener training opportunities are becoming more prevalent (NCDB, 2013; Parker et al., 2015). However, Kyzar and Summers (2014) documented that 46.3% of participants in the larger study reported that they did not use intervener services within home, school, or community settings. Data indicating that only one state has a process for credentialing interveners and that a large majority of public school administrators are unaware of or unfamiliar with national credentialing for interveners (NCDB, 2012) suggest that lack of access to intervener services is an issue for these children and their families.
We hypothesize that our finding suggesting that families need high-quality instructional partnership and high-quality educational services for significantly higher FQOL is associated with these systemic limitations affecting the educational workforce and service quality. The lack of knowledge and training school personnel have about deaf-blindness may be a stark contrast to the level of knowledge and training parents have attained about their child’s deaf-blindness. Previous research has indicated that parents of children with low-incidence disabilities perceive that their children’s teachers lack necessary disability-specific training (Hodapp, Freeman, & Kasari, 1998). With such a wide array of challenges facing educators of students with deaf-blindness, the bar is raised; having sufficient educational programming does not make up for low-quality partnership satisfaction, and conversely, being satisfied with partnership does not make up for low-quality services. Turnbull et al. (2007) evaluated policy, research, and professional development within early intervention (i.e., Part C) related to family supports and services. They concluded that the field has focused primarily on the importance of partnership in addressing family outcomes and that insufficient attention has been given to services and supports adequacy. The results of our study support the need to focus on both partnership and services and supports adequacy in pursuit of optimal outcomes for families of children with deaf-blindness.
Families of children with deaf-blindness may have other unique circumstances that also lead to this high bar for educational services. Because many children with deaf-blindness have disabilities in addition to their dual sensory impairment, these families likely have more complexity in their day-to-day experiences than parents of children with milder or singular disabilities. Research has indicated that families of children with low-incidence disabilities (e.g., intellectual and developmental disabilities) experience higher levels of stress and depression than families of children without low-incidence disabilities (Emerson, 2003; Singer, 2006). Perhaps all possible resources at the school—high-quality partnership and high-quality educational services—are required for these families’ FQOL, given the potential of additional stressors outside of the school setting to also have an effect on their FQOL.
The interaction between related services and partnership had a different pattern of effect on FQOL: High perceptions of related services buffered the negative effects of low partnership perceptions on FQOL. This finding may be due to the nature of specialized work that related service providers carry out in comparison to education providers. Whereas teachers address a wide variety of academic and behavioral outcomes, related service providers (e.g., occupational therapists, speech-language pathologists) address outcomes within one developmental area. This defined area of expertise may elevate parents’ perceptions of related service providers’ qualifications, buffering the negative effects of low perceptions of partnership on FQOL.
Findings of our study indicate that friend and family supports adequacy significantly predicts FQOL for families of children with deaf-blindness. Kyzar and Summers (2014) reported that among all SSAS-DB domains, friend and family support had the highest satisfaction ratings. Our results support the findings of other studies that have documented that social support from family members is associated with higher family outcomes (e.g., Davis & Gavidia-Payne, 2009; Sipal & Sayin, 2013).
The results of this study indicate that child-care services adequacy is significantly related to FQOL for families of children with deaf-blindness. Young children with disabilities have been reported to experience lower-quality care than their peers without disabilities, and their parents have reported lower levels of satisfaction (Wall, Kisker, Peterson, Carta, & Jeon, 2006). Jinnah and Stoneman (2008) found that families of school-age children with intellectual or developmental disabilities experienced “numerous problems” (p. 970) in finding child care. One participant mentioned, “The childcare options that I currently have for my child is zero. How’s that for an answer? Zero. There is absolutely none anywhere” (Jinnah & Stoneman, 2008, p. 970). Families in Jinnah and Stoneman’s study reported challenges with finding out-of-school care settings within their geographical area, which has also been reported elsewhere (Niergarth & Winterman, 2010).
Implications for Research
Further research is essential in interpreting the findings of this study. We recommend that future research on FOQL for families of children with deaf-blindness consider partnership as well as the quality of the services themselves. Future research should seek to understand specific indicators families consider important in defining high-quality education services for their children with deaf-blindness. This research should consider the effect of workforce variables, such as teacher certification and training related to deaf-blindness, on partnership, educational service adequacy, and FQOL. Given our findings that related services have the potential to buffer the negative effects of low partnership, this line of research could be further informed by examining differences between related services and educational services, and the partnership that the professionals within each of these disciplines form with families of children with deaf-blindness.
For the participants in this study, informational services adequacy was negatively related to FQOL; that is, the more satisfied parents were with the information they received about their child’s deaf-blindness, the less satisfied they were with their FQOL. The information services included on the SSAS-DB are services provided largely outside of school settings and are aimed at informing families about their child’s deaf-blindness as well as their rights within school settings. Research has indicated that dissatisfied mothers seek information, in part, to ensure that the information they receive from professionals aligns with current research (Starke & Möller, 2002). Trainor (2010) examined parental advocacy and found that one approach to advocacy involved parents becoming a “disability expert” (p. 40). Further research is needed to better understand the relationships among information provided to parents, perceived inadequate preparation of professionals, the perceived need to engage in advocacy, and FQOL.
To better understand the nature of partnership’s impact on FQOL, research should examine the effect of specific partnership indicators (including child- and family-focused relationships) on each FQOL domain (e.g., emotional well-being, parenting or family interaction) for families of children with deaf-blindness. A recent study by Eskow, Chasson, Mitchell, and Summers (2015) found that for families of children with autism spectrum disorder, higher satisfaction with child-focused partnership was associated with higher perceptions of child improvement and FQOL. Unpacking the relationship between partnership and FQOL for families of children with deaf-blindness is a logical next step in this line of research.
The strong associations between (a) friend and family supports adequacy and FQOL and (b) child-care services adequacy and FQOL found in our study provide other directions for future research. For example, future research could examine how services might support family members and friends in developing the ability to provide emotional and logistical support to children with deaf-blindness and their families.
Implications for Professional Development
We have suggested that there may be a gap between the specialization parents start developing shortly after their child’s birth and the training provided to special and general education teachers who infrequently teach students with this complex disability. Research that further explores this issue is needed to inform both preservice and in-service professional development. One of our author team is a coauthor of a leading textbook that provides an introduction to special education for undergraduate and graduate general and special education students (Turnbull, Turnbull, Wehmeyer, & Shogren, 2016). Although this book of 410 pages has a separate chapter on low vision and blindness and on hard of hearing and deaf, it includes only two paragraphs on deaf-blindness. In our combined approximately 90 years of teacher education experience, this textbook coverage is the rule rather than the exception. Much more attention needs to address (a) the creation of professional development resources, (b) the preparation of teachers specializing in deaf-blindness, and (c) the preparation of general educators to provide inclusive services to this population of students.
Limitations
This study was limited in that the majority of participants were mothers, and approximately 80% of participants reported being White. Although there are limited national demographics on students with deaf-blindness, we were unable to locate comparative national family-level data. Therefore, we are unable to document the representativeness of our sample of families of children with deaf-blindness to the population at large. We did not follow up with participants who did not respond to the initial survey request; therefore, the results of this study are at risk of bias due to nonresponse (Dillman, Smyth, & Christian, 2014). In general, there are challenges associated with garnering sufficiently large sample sizes from low-incidence populations. It is important to note that of the quantitative studies examining families of children with deaf-blindness, our study has the largest sample.
Finally, this study is limited by the lack of participant data regarding the educational settings (e.g., general education, school for the deaf or blind) of the children and youth with deaf-blindness within the participating families and the type of services (direct vs. consult) these students received from teachers trained in dual sensory impairment, such as teachers of the deaf or hard of hearing and teachers of the visually impaired. Due to these limitations, interpretation of the interaction effect of partnership and education services adequacy should not be associated with any specific educational setting or educational professional.
Conclusion
To date, this study represents the most comprehensive empirical examination of the predictors of FQOL for families of children with deaf-blindness. Findings suggest that future research on services and supports adequacy and family outcomes, such as FQOL, should consider partnership as a key variable. To extend the findings of this study, this research should more closely examine the specific partnership indicators (e.g., child focused vs. family focused) that predict FQOL, differences in perceptions depending on educational setting and service delivery model, and factors that influence families’ FQOL when they perceive their child’s school to be of high versus low quality.
Footnotes
Authors’ Notes
This manuscript is based on data also used in a previously published report of the first author’s dissertation. Another report of data from the database utilized for this study is cited in the article as Kyzar and Summers (2014).
The authors would like to acknowledge Dan Krutka, Mary Amanda Stewart, and Mary Dell Donelson, Department of Teacher Education, Texas Woman’s University, for their critique of this manuscript.
This research was supported by grants H325D060063 and H325D80047 from the U.S. Department of Education Office of Special Education Research to the University of Kansas. The opinions expressed are those of the authors and do not represent views of the Office of Special Education Programs or the U.S. Department of Education.