
Abstract
With the growing interest in the expertise approach to high performance, its application in surgery remains underexplored. This study uses a constructivist grounded theory design and intensive interviews to examine the development of professional excellence and cognitive productivity among six renowned surgeons. It traces their trajectories from early life to global recognition. The analysis generated the “Description of the Dynamics of Professional Excellence Formation in Surgical Medicine,” highlighting the crucial role of personal and physical abilities, psychological adaptability, and resilience in overcoming challenges. These elements, shaped by evolving contexts and complex interactions, foster continuous development, innovation, and leadership. The findings reveal that global innovation represents the peak of cognitive productivity, while exceptional leadership marks the height of professional excellence. Participants engaged in dynamic processes integrating both. The study provides valuable insights into cultivating excellence in surgery, emphasizing sustained growth, ethical commitment, and effective problem-solving to achieve a lasting global impact.
Plain Language Summary
This study looks at how six internationally recognized surgeons achieved excellence in their careers. Through in-depth interviews, the research explores their journeys from early life to becoming global leaders in surgery. The findings show that outstanding performance is not only about medical skills—it also requires strong personal qualities like adaptability, persistence, and mental strength. These surgeons kept improving themselves by learning from challenges, solving problems, and staying committed to their goals and ethics. Over time, they became innovative thinkers and inspiring leaders. Their stories highlight how continuous growth, creativity, and responsibility can lead to lasting impact in the field of surgery. This study offers useful lessons for anyone interested in how excellence is developed in complex, high-pressure professions like surgical medicine. These insights may be helpful to educators, training programs, and policymakers who wish to better understand and support the development of future surgical professionals, as well as talent development programs that aim to help gifted individuals identify their early career interests and build pathways that align with their strengths.
Introduction
Since the inception of gifted education, research on talent development has often relied on longitudinal studies, notably influenced by Terman’s work (Urbina, 2011). These studies conceptualized talent as general abilities that emerge early in life and gradually become specialized in a specific domain, tracking developmental progress prospectively and chronologically throughout the lifespan (Stoeger, 2009). While such approaches have provided valuable insights into developmental trajectories, they have also highlighted the limitations of relying solely on IQ to predict exceptional achievement and the challenges of committing years of effort without assurance of attaining excellence (Subotnik et al., 2011).
In response to these limitations, the expertise-based approach emerged, focusing on individuals who have already attained distinguished levels of performance (Stoeger, 2009). This perspective emphasizes retrospectively examining how early potential evolved into advanced expertise (Subotnik et al., 2019). It builds on multiple theoretical foundations that offer complementary views of talent development. Bloom’s (1985a, 1985b) three-stage framework of talent development, Gagné’s (2009) differentiation between general abilities and domain-specific talent, and Tannenbaum’s (2009) emphasis on domain-specific aptitudes have all contributed to integrated models describing how talent matures over time. In addition, Ericsson’s (2003) concept of deliberate practice underscores the importance of structured, sustained training as a driver of expertise.
Accordingly, this study aims to examine how early potential crystallizes and transforms into high-level professional excellence and advanced cognitive productivity among surgeons. Adopting an expertise-based approach integrated with constructivist grounded theory, the study seeks to provide a comprehensive understanding of how abilities and predispositions evolve into specialized expertise and sustained professional distinction in surgical practice.
Achieving High Professional Excellence and Cognitive Productivity in Surgical Medicine
Professional excellence and cognitive productivity in surgical medicine is essential for delivering high-quality health care (Norman et al., 2018). This excellence encompasses not only technical skills but also emotional intelligence and effective communication, all of which contribute to better patient outcomes and satisfaction—particularly in dimensions, such as trust in the physician, clarity of communication, emotional support, and confidence in care decisions (Ericsson, 2011). Furthermore, continuous development, mentorship, and collaboration enhance surgeons’ abilities to remain current with medical advances (Ericsson, 2015). While excellence ensures high standards of care, its impact is significantly amplified when combined with cognitive productivity, which supports the generation and exchange of knowledge among practitioners and researchers (Fry et al., 2011). Integrating these dimensions is therefore critical for fostering innovation, improving patient care, and strengthening the resilience of health care systems.
Dynamic Synergy: Endogenous and Exogenous Resources
Csikszentmihalyi (1996) adopts a systemic and phenomenological approach that examines the creativity of distinguished individuals as the product of interactions between individual characteristics, domain knowledge, and field recognition, while also emphasizing the subjective experience of flow. Expanding on this systemic view, Ziegler et al. (2019) distinguish between endogenous resources—like physical, motor, and experiential capital—and exogenous resources, such as economic, cultural, infrastructural, social, and pedagogical capital. These resources must evolve with contextual changes (D. Dai, 2021). Building networks of endogenous and exogenous resources fosters systems that promote professional performance and cognitive productivity (Ziegler & Stoeger, 2019).
Cultural Dimensions and Capital Structures in Surgical Excellence
Hofstede’s cultural dimensions (Persson, 2012)—such as power distance, collectivism versus individualism, and uncertainty avoidance—show that professional excellence is deeply shaped by cultural value systems. In Saudi Arabia, where hierarchical structures and collective orientations prevail, surgical excellence often arises through institutional progression and community recognition, whereas in individualist cultures it is linked to autonomy and initiative.
Bourdieu’s theory of capital (Bourdieu, 1986) likewise emphasizes that distinction depends not only on competence but also on access to economic, cultural, and social capital, embodied through habitus (Nair, 2024). These resources structure opportunities and guide surgeons’ career trajectories.
Crucially, the two frameworks interact: cultural orientations toward hierarchy and collectivism shape how capital is accumulated and valued, filtering mentorship networks and recognition through expectations about authority, gender, and conformity. This makes Hofstede’s dimensions essential for interpreting how the distribution of Bourdieu’s capitals translates into divergent career pathways. For the present study, these perspectives illuminate the cultural and structural conditions that frame surgeons’ trajectories toward excellence, offering a nuanced lens on how professional development is both enabled and constrained by societal systems.
Expertise Pathways: Insights from Talent Development and Surgical Medicine
Bloom’s (1985a) work drew on a coordinated set of qualitative studies, each based on in-depth life-history interviews with a small, selective group of exceptional individuals across six talent domains—concert pianists, sculptors, research mathematicians, research neurologists, Olympic swimmers, and tennis champions—conducted by one or two scholars in each field. Together, these studies informed his three-stage model of talent development: (1) early discovery nurtured by family support, (2) apprenticeship under expert mentorship with intensive practice, and (3) maturity characterized by autonomy and mastery. Within this same work, contributors offered further elaborations: Sloane (1985) emphasized the central influence of family and environment, Sosniak (1985) underscored the sustained commitment required for long-term learning, and Bloom (1985b) reflected on cross-domain generalizations that illuminate broader processes of talent emergence.
Building on Bloom’s expertise-informed framework, subsequent research in talent development has continued to apply the expertise-based approach to examine developmental trajectories across a variety of domains. D. Dai and Li (2020) identified internal and external factors enabling individuals to reach excellence in STEM (Science, Technology, Engineering, and Mathematics), including early maturity, independent learning, perseverance, personal initiative, and parental guidance. Paik et al. (2019) and Olszewski-Kubilius et al. (2019) emphasized the importance of early exposure, staged support, supportive relationships, and psychosocial skills in fostering excellence and shaping expertise trajectories across diverse and critical domains, such as surgical medicine. Subotnik et al. (2019) characterized high-level performance as a dynamic, lifelong process beginning with early ability identification and gradually transforming into specialized competence and recognized excellence. Their work included McWilliams et al. (2019), who offered an applied framework describing talent development in medicine across three stages: competence, expertise, and high productivity and eminence.
Ericsson and Pool (2016) developed the “deliberate practice” model, which explains expert performance across professional domains through structured and targeted training. Building on this framework, Ericsson (2018) emphasized that in surgical practice, excellence depends not on time alone but on systematic review, constructive feedback, and repeated cases combined with deliberate analysis and error correction. More recent studies have confirmed that deliberate practice significantly enhances surgical competence among trainees (Kanoksin et al., 2025; McGaghie et al., 2021).
Although prior expertise research in gifted education has stressed the developmental nature of excellence beginning in early childhood, little is known about how this unfolds in surgical medicine. Most studies have focused on skills acquired during university training and early practice, overlooking formative experiences in earlier stages. Within this context, Hardré et al. (2017) demonstrated that modeling, mentorship, and tacit knowledge transfer in clinical settings are vital for refining skills and shaping professional identity. McDonald (2025) further emphasized that mental, physical, and technical readiness are essential for sustaining high performance and reducing errors in high-risk specialties, such as global health, dental surgery, and neurosurgery. Similarly, Madani et al. (2017) highlighted the critical role of advanced cognitive skills for planning, decision-making, and error management in complex surgical practice. This study seeks to bridge that gap by integrating insights from gifted education and surgical expertise. The central question guiding this investigation is: “How do professional excellence and cognitive productivity develop among distinguished surgeons throughout their scientific and professional careers?”
Research Approach
We applied a constructivist grounded theory approach developed by Charmaz (2006) to explore how professional excellence and cognitive productivity are formed among distinguished surgeons. Unlike traditional objectivist grounded theory, this approach emphasizes the researcher’s active role and acknowledges how their background shapes the analysis. The integration of theoretical and practical experience not only deepens understanding but also generates knowledge that is transferable and informs professional practice. In this way, such integration contributes to a more nuanced comprehension of the complexities inherent in surgical medicine. Moreover, it examines phenomena within broader contexts and incorporates the researcher’s cognitive contributions into the interpretation (Charmaz, 2025).
Method
Participants
We purposively selected participants based on the principle of theoretical utility, ensuring the inclusion of individuals who met the following criteria: (1) holding a senior leadership position in the health care sector or being appointed to high-level international tasks; (2) having extensive contributions and engagements in international scientific journals and conferences; (3) holding a senior consultant position in surgical medicine; and (4) having gained wide social recognition within the medical community.
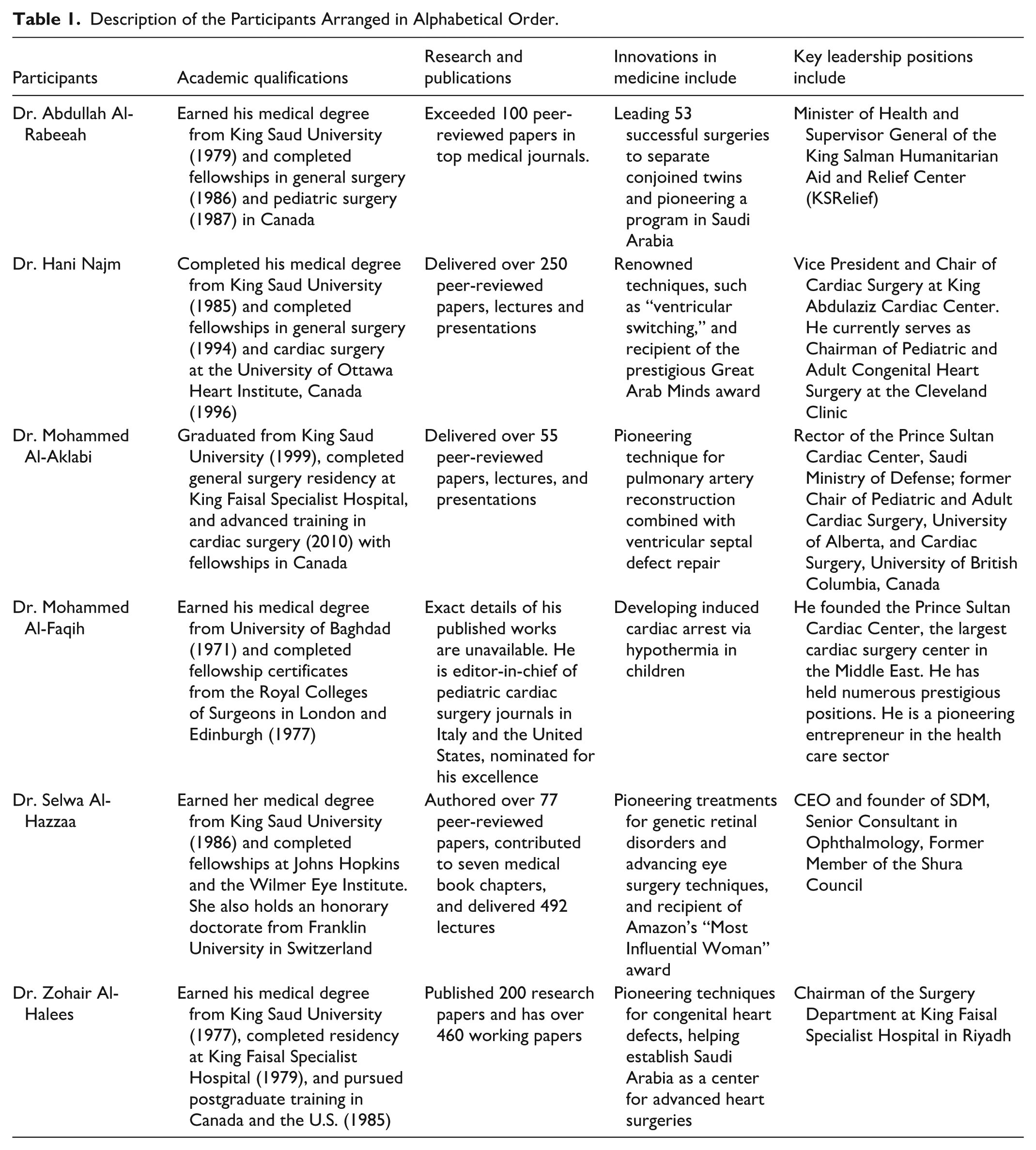
With their explicit consent, the identities of the participants were disclosed to provide a clear and realistic portrayal that extends beyond the descriptive analysis of their professional excellence and cognitive productivity. Renowned scholars, such as Simonton (1994), Goertzel and Hansen (2004), Gute et al. (2008, 2016), and Csikszentmihalyi (1996) have employed similar methodologies by studying eminent figures and explicitly disclosing their identities—an approach with which this study aligns. Table 1 presents a concise overview of the participants’ academic qualifications, scientific contributions, and their roles in innovation and leadership.
Description of the Participants Arranged in Alphabetical Order.
Data Collection
We employed intensive interviewing as the primary method of data collection, following Charmaz’s (2025) approach. Participants with direct experience of the phenomenon were engaged in open-ended conversations to explore perspectives and lived experiences in depth, aiming for rich responses while remaining attentive to unexpected insights, implicit cues, and underlying meanings (Charmaz, 2025).
To guide the process, we used a preliminary interview protocol. As Creswell et al. (2007) note, such protocols consist of flexible initial questions adapted as analysis evolved. The interviews focused on environmental and personal factors shaping excellence, influential figures, challenges, critical skills and characteristics, leadership, cognitive productivity, stages of expertise development, and related themes. In later interviews, particular attention was given to leadership, innovation, and risk-taking.
We used MAXQDA software to manage, code, and interpret the data. We also analyzed written documents—such as CVs, articles, and interviews—to capture experiences across career stages (Corbin & Strauss, 2015). In addition, televised programs and online platforms like YouTube and social media provided further reflections on participants’ professional journeys. Data collection began on May 27, 2023, and concluded on November 27, 2024.
Criteria for Constructivist Grounded Theory
Constructivist grounded theory research does not rely on conventional notions of “validity,” “reliability,” or “objectivity” as defined in quantitative research or in certain other qualitative traditions, where knowledge is not viewed as an objective reality to be discovered but rather as a socially constructed process shaped through interaction between the researcher and participants within their sociocultural contexts (Charmaz, 2025). According to this perspective, quality criteria in constructivist grounded theory focus on interpretive understanding, researcher reflexivity, and acknowledgment of the multiplicity and complexity of meaning (Bryant & Charmaz, 2007; Morse et al., 2002).
Accordingly, this study was guided by four core criteria defining the quality of constructivist grounded theory research: credibility, resonance, originality, and usefulness (Charmaz, 2025). Credibility was enhanced through conducting intensive interviews that relied on synchronizing data collection and analysis, comparing recent codes with emerging categories, adopting inductive coding, and consistently engaging in memo writing. These strategies allowed analytic categories to emerge without imposing prior models. A second grounded theory researcher reviewed selected codes and memos to enhance rigor and consistency. Selected categories were also revisited with some participants to enrich interpretation through interpretive dialogue (Birks & Mills, 2015).
Resonance was achieved by authentically representing participants’ voices and sociocultural contexts and by exploring the depth of their experiences (Charmaz, 2006; Thornberg & Charmaz, 2014). Originality emerged through developing new, data-driven concepts reflecting aspects of the development of high-level performance throughout participants’ educational and professional trajectories, with constant comparison revealing nuanced dimensions of excellence (Morse et al., 2002). Usefulness was reflected in providing insights that can be utilized in future research contributing to the enrichment of the educational and professional fields (Corbin & Strauss, 2015; Glaser & Strauss, 2017).
Procedure
We obtained ethical approval beforehand. In collaboration with experts from the health sector, we created a shortlist of 11 potential participants to ensure a thorough selection process. We searched their names on digital platforms, such as Google and YouTube, to gather publicly available information about their professional paths and CVs, ensuring alignment with the pre-established criteria. Recruitment was conducted via email, phone, or WhatsApp. Formal invitations were extended to several of the 11 individuals who met the criteria. Six distinguished Saudi surgeons—recognized for their excellence locally and globally—responded and were selected for inclusion in the study. We provided each participant with a brief description of the study, outlining its purpose, data handling procedures, and how results would be presented. Given the demanding responsibilities of the target group, we obtained consent in the most convenient manner for each participant—either verbally during interviews or in writing via digital communication. All participants explicitly permitted the use of their names in the study.
We conducted interviews via audio or video calls due to logistical challenges, as two participants were engaged in professional assignments outside Saudi Arabia. Electronic platforms enabled us to conduct four video interviews and two audio-only interviews, each lasting between 45 minutes and 1 hour, allowing for in-depth discussions. We used Google Translate and ChatGPT as supplementary tools solely to improve language clarity and organization, without employing them for research analysis or altering the methodology.
Data Analysis
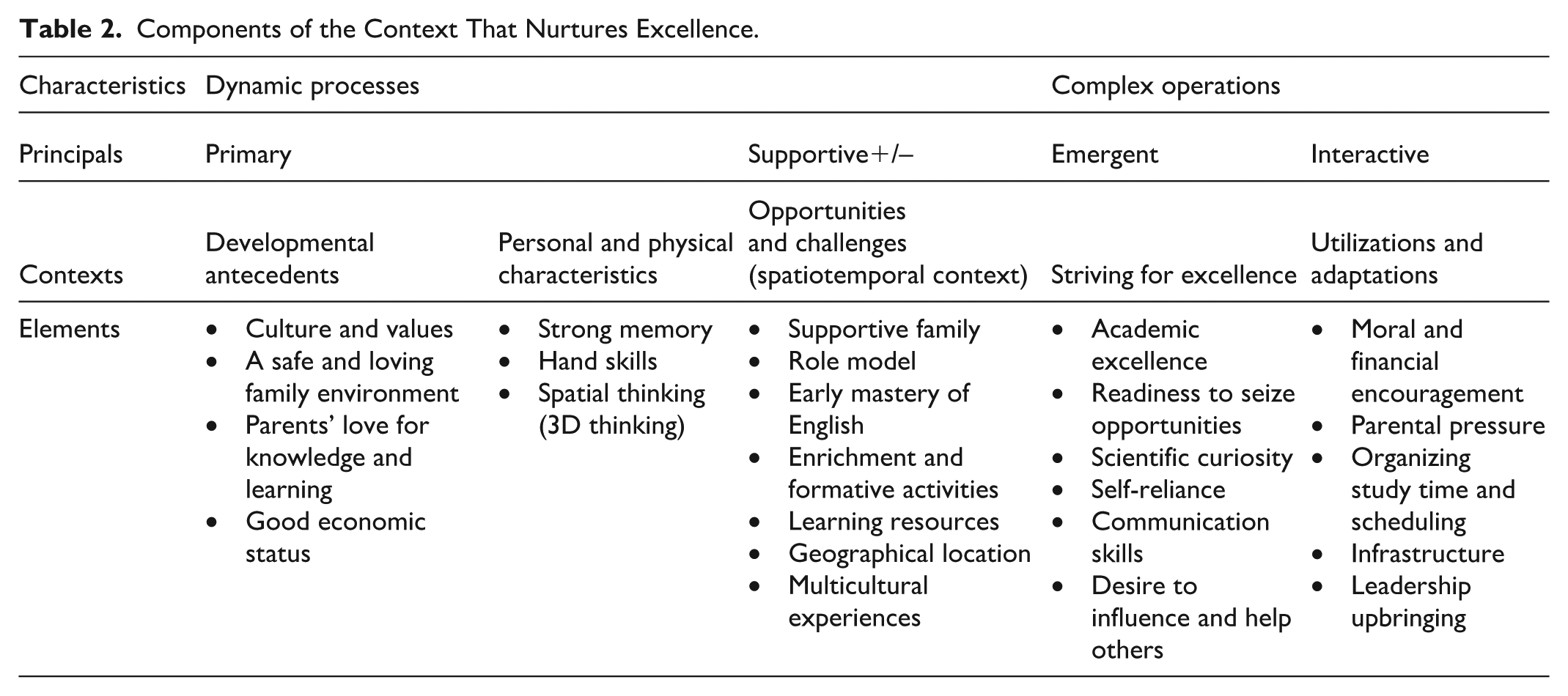
We followed the grounded theory methodology, employing a structured and iterative approach that integrated data collection, coding, and analysis concurrently. We began by conducting interviews and collecting data, using line-by-line coding to identify emerging theoretical insights. This process yielded a large set of initial codes, which were then critically reviewed and refined, focusing on those most relevant to the phenomenon under study. These refined codes represent the elements outlined in Tables 2 and 3.
Components of the Context That Nurtures Excellence.
Components of the Productive Context for Excellence.
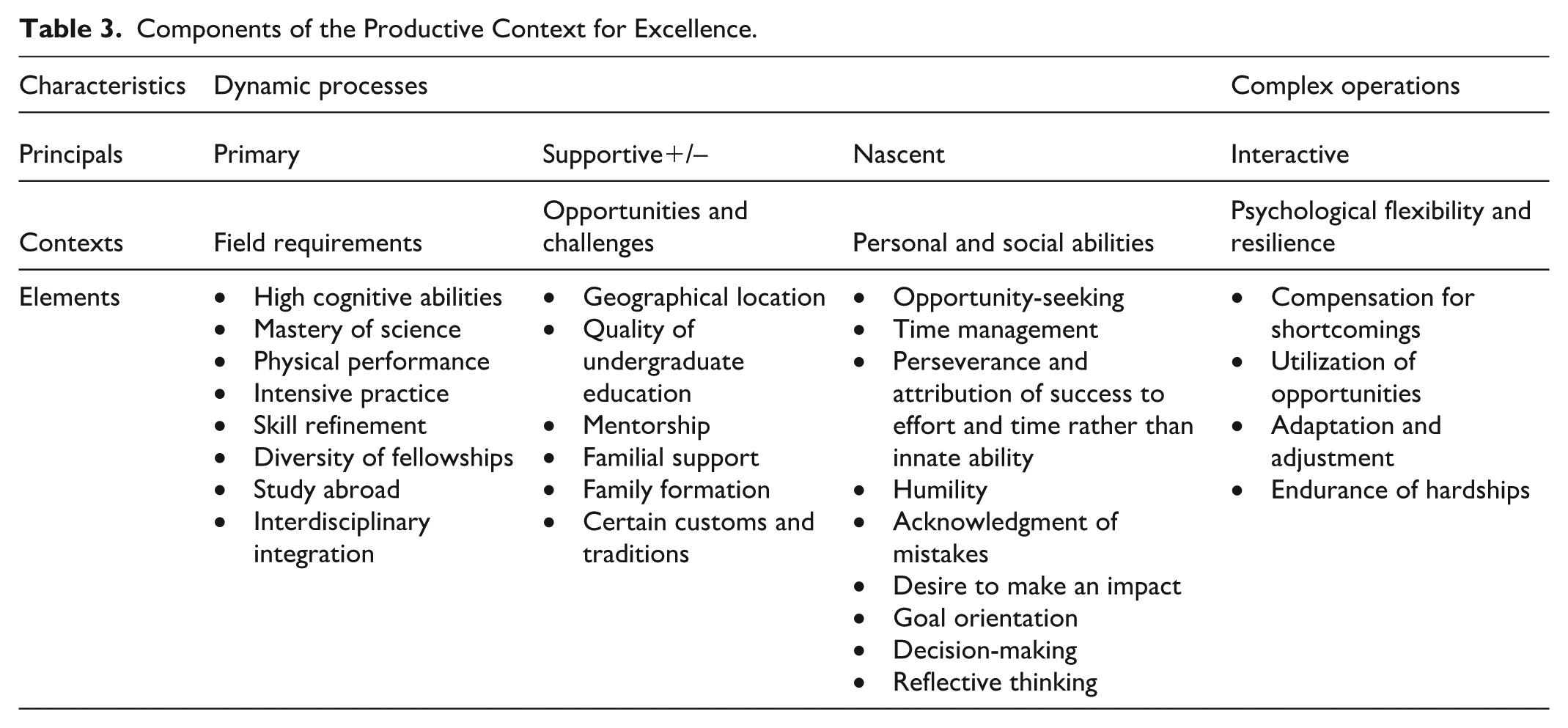
As we progressed, we transitioned to axial coding, which allowed us to clarify definitions of the emerging concepts and explore the relationships within and between these codes. This step enabled us to categorize the codes into coherent concepts that represent contexts. We then proceeded to form broader themes, which comprised the principles and characteristics summarized in Tables 2 and 3.
The following example offers a clearer illustration of the progression from line-by-line coding to axial coding. In this instance, the findings revealed the category of innovation as an integrated contextual factor influencing the attainment of excellence. To further elaborate on the characteristics of this category, we examined its emergence, identifying a set of key elements: high cognitive abilities, mastery of medical and surgical sciences, interdisciplinary integration, acknowledgment of mistakes, endurance of hardships, research and continuous learning, variety of cases, frequency of cases, and complexity of cases. Using axial coding, these components were clustered into three core categories: scientific confidence formation (comprising the first three elements), responsibility bearing (the middle two), and intensive practice (the last four).
These categories collectively informed the theoretical development of what we termed the principle of lowering the risk-taking threshold. As revealed through our analysis, this principle emerged as a unifying pattern across participants and as a central conceptual mechanism for fostering innovation in surgical medicine—particularly within high-stakes, complex cognitive environments, as illustrated in Figure 1. We positioned risk-taking as an intentional threshold in the surgical field, as excellence in this domain may be difficult to achieve without the willingness to engage in calculated risks.

Lowering the Risk-Taking Threshold.
We found that memo writing played a crucial role, as it enabled us to actively link the data collection process with our evolving drafts of preliminary findings. Engaging with these memos allowed us to reflect on the initial codes and categories. This process deepened our analytical thinking and facilitated the transformation of these codes and categories into more coherent and refined constructs. The following are examples of memos written by researchers during data collection and analysis:
Memo 4: Derived from Al-Hazzaa’s account: The role of values and their early cultivation is clearly evident in the previous excerpt. The value of humility, for example, was instilled by her father in his children through his behavior, guidance, and consistent modeling from an early age, following the pattern of a nurturing role model. As a result, the individual later adopted a set of principles that embodied this value, including respecting patients . . .
Memo 20: Derived from Najm’s account: . . . His account of his secondary school experience in competitive Taekwondo offered a compelling lens into how structured, high-level training programs can function as early preparatory cycles for professional excellence . . .
Using constant comparative methods, we systematically compared codes, categories, and emerging concepts—not only against each other but also in relation to developing theoretical constructs. This comparative analysis enhanced our interpretive depth, helping us move beyond descriptive labels toward more abstract and meaningful insights. By examining the relationships between categories, we explored their theoretical implications and considered how they connected to fundamental human experiences, such as social relationships, tensions between individual agency and structural constraints, and institutional dynamics.
To illustrate our comparative analysis, we contrasted Al-Hazzaa’s account of her social capital with reflections by Najm and Al-Rabeeah on the underrepresentation of female surgeons. This analytic step clarified both shared and divergent patterns in the participants’ narratives. This finding also prompted further inquiry to develop a clearer understanding, as will be discussed later.
As our analysis progressed, we found ourselves moving toward increasingly abstract and generalized interpretations through theoretical coding (Charmaz, 2025). By this final stage, we were no longer relying solely on direct quotations; instead, we drew from theoretical insights that emerged through our iterative and comparative engagement with the data. This rigorous process enabled us to develop a nuanced theoretical understanding of the phenomenon, identifying key properties explaining how the broader context and its sub-contexts functioned in shaping professional excellence.
This shift toward abstraction and theoretical integration was reflected in the formulation of dynamism and complexity within professional excellence in surgery. Through iterative clustering of codes, the researchers identified contextual features characterized by fluidity, adaptability, and responsiveness—interpreted as dynamic elements. Others showed dense interdependencies requiring coordination, strategic judgment, and cognitive-emotional regulation—conceptualized as complex elements. These constructs were not directly stated by participants but emerged through layered interpretive work combining study findings with the researchers’ prior knowledge. The development of the present theoretical description was informed by the researchers’ engagement with various perspectives, particularly those advanced in the works of expertise and talent development (Csikszentmihalyi, 1996; Ericsson, 2003, 2018; Subotnik et al., 2019; Ziegler et al., 2019), as well as the broader theoretical frameworks that help explain how cultural and social conditions shape pathways to excellence, drawing on Bourdieu’s (1986) capital theory and Hofstede’s cultural model (Persson, 2012).
Ultimately, the researchers organized these constructs into a developmental sequence of stages and levels, illustrating how dynamic and complex operations interact as aspiring surgeons progress from foundational preparation to advanced excellence. This abstraction is reflected in the fourth category of findings, derived through comparative analysis, which integrates earlier results into a cohesive framework describing the developmental trajectory of professional excellence and cognitive productivity in surgical medicine. Data collection, coding, and analysis were conducted in Arabic, while the final report was written in English and the accompanying quotations translated accordingly.
Findings
This study provides a description of the dynamic processes and complex operations of professional excellence formation in surgery, based on four analytical categories: (1) the contexts and sub-contexts of excellence, (2) the dynamics and complexity of excellence contexts, (3) the dynamics sustaining excellence toward innovation and leadership, and (4) the ascending surgical excellence trajectory (ASET model).
The Contexts and Sub-Contexts of Excellence
The findings reveal that excellence is not merely a set of interacting factors but rather a comprehensive system of integrated contexts. Each context consists of several sub-contexts, and within these contexts, elements interact in various ways, influencing the advancement or delay in the emergence of excellence.
The Nurturing Context for Excellence
This category represents the developmental journey toward excellence during general education. Five sub-contexts emerged within this main context, as outlined and detailed in Table 2.
Developmental Antecedents
This category captures the cultural and familial traditions that shape the broader environment—particularly those of parents and family members—which often begin before birth and continue to influence development throughout early childhood, as seen in the experiences of the distinguished surgeons. Participants demonstrated marked differences in their starting points. The various forms of capital—social, cultural, and symbolic—contributed in distinct ways to shaping the participants’ pathways toward excellence. Each type of capital played a role in fostering environments that supported and stimulated development to varying degrees. Although some participants faced challenges in their early circumstances, these differences did not prevent them from attaining high levels of professional and cognitive excellence later.
For instance, Al-Rabeeah was raised in moderate economic circumstances but benefited from strong cultural and familial capital through parental encouragement, a love of learning, and early exposure to surgical settings—demonstrating an overlap of social and cultural capital. Alternatively, Najm’s upbringing emphasized manual skills, ambition, and achievement, while his selective government school education offered a structured academic environment, together creating a balanced foundation of cultural and social capital. Al-Faqih’s trajectory was shaped by migration, family support, and influential role models abroad, resulting in cross-border cultural capital during a period of limited local medical education. Al-Hazzaa’s background combined cultural and social capital with symbolic capital from early exposure to American academic and linguistic environments, and her self-taught father transformed a traditional merchant legacy into academic ambition. Al-Halees initially faced geographic constraints but, through family guidance, transitioned into medicine and developed a strong sense of purpose and personal drive.
These findings show how different configurations of initial capital—familial support, educational access, and formative relationships—shaped participants’ professional trajectories. However, capital alone was insufficient; it required individual agency to mobilize and transform these resources into sustained pathways toward excellence.
Personal and Physical Characteristics
Although these characteristics have genetic determinants, they possess the ability to develop and grow through dynamic interactions with environmental requirements to achieve excellence and distinction: I had an excellent memory and was considered relatively intelligent. This allowed me to start school at the age of four. (Al-Halees) I demonstrated a talent for drawing, Arabic calligraphy, and crafting. I was naturally inclined toward manual work, such as woodworking. (Al-Faqih) God has gifted me with the talent of three-dimensional thinking . . . Creative thinking in surgery relies on the ability to visualize solutions . . . Talent often manifests early in life, and surgeons are expected to demonstrate a natural inclination for manual work, evident in childhood activities such as tying shoelaces. (Najm)
Opportunities and Challenges
The findings indicated that spatial and educational conditions can serve as opportunities, challenges, or both simultaneously: When I was a child, my father used to assign us various household tasks, which nurtured my passion for manual work and creativity. (Najm) In secondary school, a college visitation program allowed me to visit the College of Medicine. This experience strengthened my passion and motivated me to pursue a career in medicine. (Al-Rabeeah)
In addition, Al-Hazzaa faced cultural barriers to women entering medicine but overcame them with her father’s support. Al-Halees could not study engineering due to local constraints and instead entered medicine, where he developed a passion.
Striving for Excellence
The participants’ statements consistently emphasized these elements. The citations provided throughout the study highlight them or certain aspects of them. The following is an additional example: I remember dedicating additional effort and investing more time in studying during high school to achieve a high-grade point average that would qualify me for medical school. (Al-Rabeeah)
Utilizations and Adaptations
These are characteristics that parents and educators employ to guide their child toward excellence, either by utilizing available resources or developing adaptive characteristics. These characteristics can be dual in nature, including supportive characteristics as well as those that encourage independence: When I was in primary school, my father took a deep interest in my studies. At times, he would even insist that I complete certain tasks, and I recall asking him why he made me do them. His response was always the same: “It’s for your own good.” (Al-Hazzaa) . . . I started school younger than my peers at the time. This made adaptation challenging and often drove me to attempt returning home. However, my father patiently guided me back each time. Moreover, my teacher’s encouragement . . . helped me feel secure and fully engaged in my studies. (Al-Rabeeah)
The Context Shaping Professional Excellence and Cognitive Productivity
Context involves both the opportunities available and how individuals navigate and respond to them. While university education and professional experiences shape development, individual agency, adaptability, and perseverance also play a crucial role. Understanding this dynamic allows for identifying replicable strategies that can support aspiring professionals from diverse backgrounds. Four sub-contexts emerged within this main context, as outlined below and detailed in Table 3.
Field Requirements
Requirements include mastering the sciences and personal and physical skills relevant to the field: A strong interest in basic sciences, coupled with a focus on surgery as a discipline, extensive practical experience, and manual dexterity in surgery, inevitably leads to innovation. Even without the explicit intention to innovate, challenges encountered in practice inspire creative solutions. (Al-Faqih)
Challenges and Opportunities
The findings indicate that surgical medicine presents significant challenges for both genders due to its demanding nature; however, women have historically faced additional obstacles, particularly in balancing professional and family responsibilities. This disparity has contributed to the global underrepresentation of female surgeons. In the Saudi context—particularly in earlier decades—traditional societal norms often regarded medicine as an unsuitable field for women, thereby limiting their participation. As a result, female advancement in surgery often depended on strong familial support alongside personal ambition. Such support was instrumental in helping women navigate societal resistance without direct confrontation. For example, Al-Hazzaa benefited from her father’s progressive vision, which enabled her to pursue medical education, and later from her husband’s support, which facilitated further specialization in a rare surgical subspecialty—ultimately allowing her to achieve excellence. Moreover, as shown in Table 1, all participants were trained at prestigious universities, where sustained mentorship by distinguished professors fostered professional commitment, exposure to complex cases, and the development of research skills.
Personal and Social Abilities
The elements under this heading in Table 3 were derived from various scattered points in the participants’ discussions, with the following being just an example: The surgeon must remain up-to-date with the latest technologies, be prepared for emergencies, and capable of making decisive, split-second decisions, as any delay could lead to dire consequences . . . (Al-Halees)
Psychological Flexibility and Resilience
Distinguished surgeons develop new characteristics that sustain their goals and excellence, including addressing shortcomings. For example, they closed knowledge gaps through specialized studies and often pursued a master’s degree after medical school. Many leveraged study-abroad opportunities, including periods of academic isolation. They also cultivated contrasting traits, such as openness versus isolation, boldness versus respect, risk-taking versus caution, and adaptation versus adjustment: My father raised us to stay true to our convictions while respecting others’ views, teaching us that confidence in our ideas should be paired with wisdom and respect. (Al-Hazzaa)
In addition, the findings revealed that the participants exhibited a notable degree of psychological resilience, which enabled them to cope with challenges, recover from setbacks, and maintain their progress toward excellence.
The Dynamics and Complexity of Excellence Contexts
The analysis revealed that the elements constituting the contexts of excellence are primarily characterized by their dynamic nature, or, to a greater extent, by their complexity. Dynamism refers to the evolution and expansion of elements over time, while complexity involves the interplay of diverse adaptive characteristics, which may vary or even contradict, leading to varied responses aligned with situational demands. The findings indicate that contexts and elements can exhibit both characteristics, with some being predominantly dynamic and others primarily defined by complexity. The following sections further elaborate on the roles of dynamism and complexity within each context of excellence.
Nurturing Excellence: Dynamism and Complexity in Early Contexts
Dynamic Elements
These elements shape excellence among aspiring surgeons during general education, influenced by environmental and temporal contexts. A supportive family fosters early intellectual curiosity, evolving with exposure to external learning resources, such as field visits and enrichment activities. Likewise, early mastery of English expands access to global knowledge, enabling engagement with diverse educational content.
Complex Elements
These elements involve intricate networks of interrelated elements that young future surgeons must navigate for academic and professional readiness. Balancing parental firmness and support fosters resilience, enabling time management, adaptation to pressures, and achievement in science. Strong communication and collaboration further enhance leadership and problem-solving, requiring adaptive strategies to navigate these interconnections, as illustrated in Table 2.
Overall, dynamic elements are marked by continuous change and interaction, grounded in essential environmental features. In contrast, complex elements arise from interactions between individual and contextual factors, generating new characteristics that require analytical and adaptive skills for effective development.
Professional Excellence and Cognitive Productivity: Evolving Dynamics and Complexity
Dynamic Elements
Shaped by evolving field requirements, opportunities, and personal and social abilities, these elements foster excellence from university education onward. Mastering foundational surgical skills and adapting to clinical challenges represent dynamic processes, supported by mentorship and professional networks that drive continuous growth across training environments.
Complex Elements
These elements involve operations requiring psychological flexibility and advanced adaptability. Surgeons navigate the interplay between technical demands, decision-making under pressure, and collaborative problem-solving in high-stakes contexts. The transition to leadership roles and engagement in advanced research and innovation adds new layers of complexity, as detailed in Table 3.
Overall, interaction between dynamic and complex elements evolves through five stages of professional excellence (Figure 2). Early stages are driven mainly by dynamic processes, while later stages increasingly rely on complex operations.
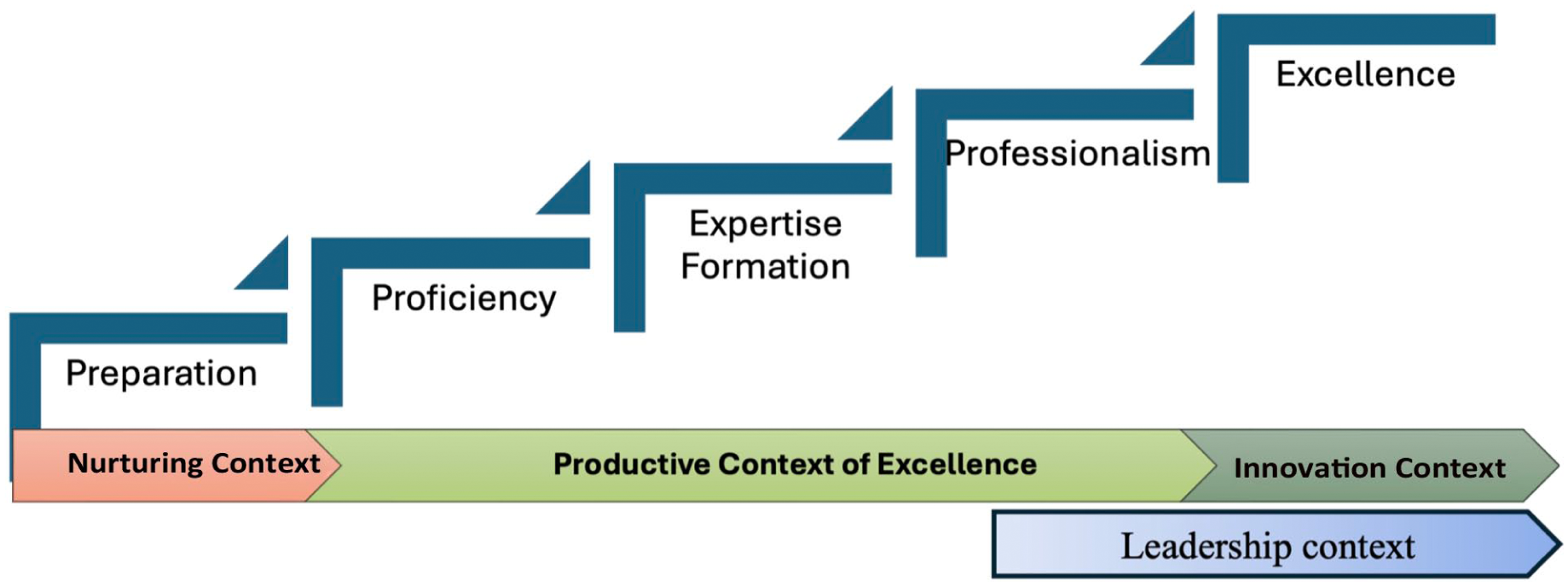
The Stages of Excellence Within the Four Contexts.
Stages of Professional Excellence Formation and Cognitive Productivity
The data analysis revealed five developmental stages through which surgeons progress to attain high-level excellence, as follows: (1) preparation—encompasses the developmental antecedents leading up to the end of the first (preparatory) year of medical school; (2) proficiency—covers the years following the preparatory year, extending through medical school and the internship; (3) expertise formation—includes fellowship periods leading up to board certification; (4) professionalism—begins after receiving board certification and continues until the surgeon attains the level of consultant; and (5) excellence—is achieved when the consultant expands the scope and impact of their cognitive productivity, contributing to advancements in the field locally or globally: The Minister of Health at the time offered me an administrative position. Despite the financial benefits and career advancement opportunities, I declined the offer and requested a room in the hospital to stay on-site and dedicate myself fully to surgery. (Al-Faqih)
The Evolving Cycle 1
As illustrated in Figure 3, this cycle is characterized by gradual development over an extended period. It begins with the onset of passion, which typically emerges at the start of the proficiency stage or at the end of the preparatory year of medical school.
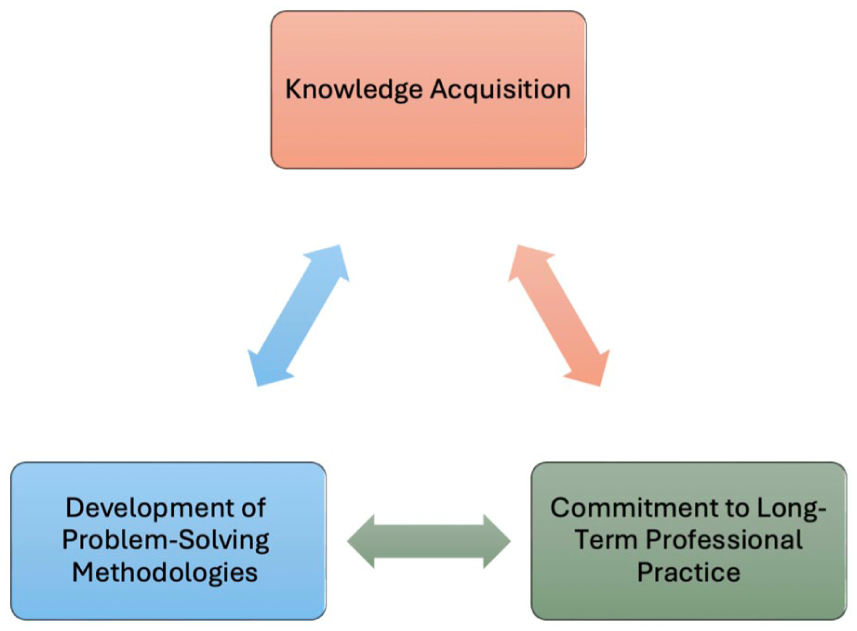
The Evolving Cycle1.
As shown in Figure 4, this cycle repeats multiple times across the three stages—proficiency, expertise formation, and professionalism. Over time, it progresses to a higher level as experiences accumulate, contributing to the development of more extensive and complex knowledge.
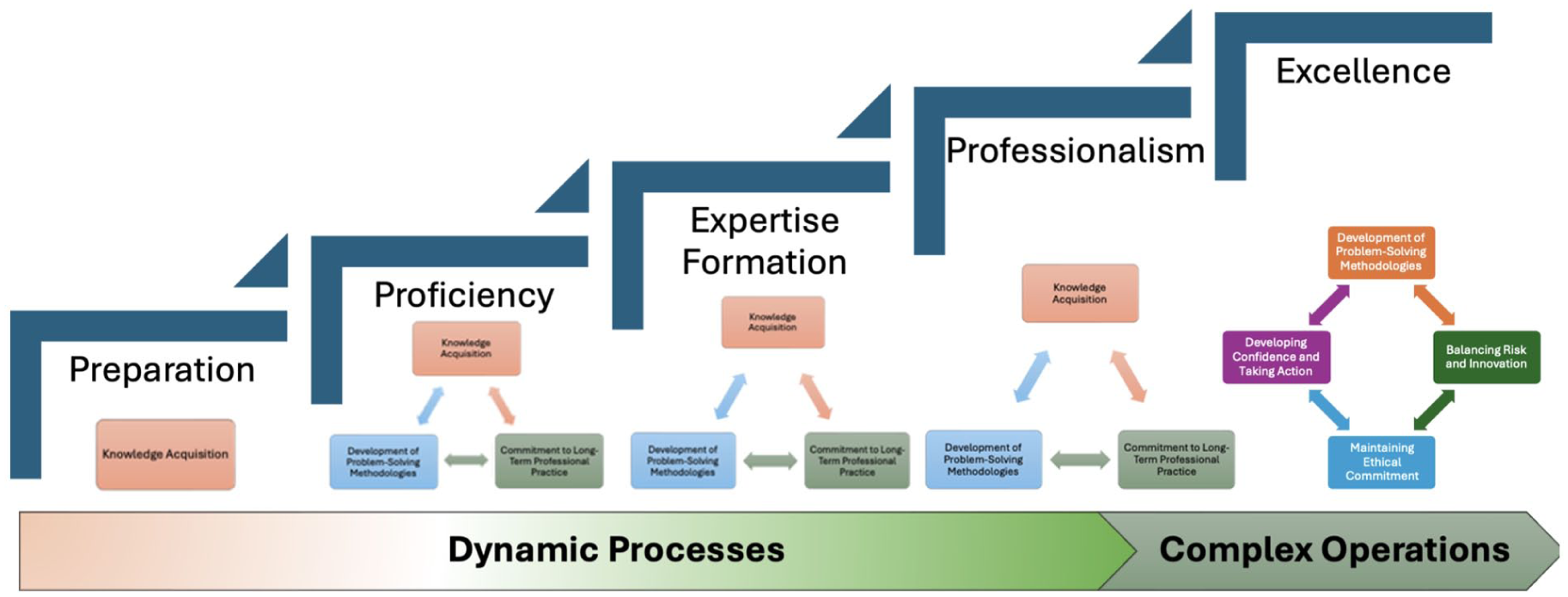
The Evolving Cycles Across the Five Stages.
Dynamics Sustaining Excellence Toward Innovation and Leadership
The fifth stage plays a pivotal role in fostering innovation and leadership in surgical medicine. Surgeons here typically fall into two groups: those who keep striving for excellence through reflection, resilience, and continuous improvement, as seen in this study, and those who stagnate and become complacent (not observed here): A cardiac surgeon progresses through essential stages, beginning with proving their competence by performing surgeries skillfully and achieving successful outcomes. Some surgeons lose opportunities at this stage due to the complexity and sensitivity of the procedures . . . the surgeon advances to . . . developing new techniques based on practical experience. Innovation results from extensive practice and performing numerous similar operations. (Al-Aklabi)
Innovation and leadership create interconnected contexts within a broader framework that drives excellence. These contexts not only interact with one another but also influence and are influenced by elements within their respective spheres and beyond. The interactions aim to maximize the potential for innovation and leadership, ultimately fostering excellence.
Innovation Context
Innovation, the pinnacle of cognitive productivity, requires intensive practice, sustained research, and years of refining surgical skills and decision-making.
Lowering the Risk-Taking Threshold
Although risk-taking is widely recognized as a valued capacity across various professional domains, it constitutes a core skill in surgical medicine—one that is essential for achieving excellence. Attaining mastery in this area is particularly challenging, as it involves the integration of multiple sub-skills operating within dynamic and complex processes. Given its strong and direct association with excellence in surgical practice, it becomes critically important to understand the underlying processes and enabling skills that facilitate the development of this capacity or help lower its threshold.
The findings revealed the presence of dynamic, long-term developmental processes that contribute to the principle of “Lowering the Risk-Taking Threshold” introduced in this study. This principle is structured around three core skills, each branching into two to three sub-skills, as detailed in the “Data Analysis” section and depicted in Figure 1. These dynamic processes serve as foundational capacities that enable surgeons to build professional confidence, enhance cognitive and behavioral flexibility, and strengthen their readiness to make high-stake decisions. Their confidence—shaped through a dynamic cycle of practice—empowers them to initiate complex clinical sequences that meaningfully advance surgical medicine. This progression unfolds at varying paces, beginning in its early phases and continuing through its upward trajectory toward high excellence, both sequentially and cyclically, as illustrated in Figure 4.
In addition, according to the principle of lowering the risk-taking threshold, innovation emerges from the interplay between risk-taking and a steadfast commitment to patient welfare. This process is embodied in a sequence of complex processes inherently tied to surgical practice, in which the surgeon systematically gathers sufficient information to diagnose the condition, anticipate potential outcomes, explore alternative solutions, determine the most appropriate approach, and implement it with skill and confidence. The surgeons in this study consistently prioritize patient well-being over personal reputation, demonstrating a willingness to confront challenges that others might avoid. Motivated by a strong sense of responsibility, they consider even the worst-case scenarios preferable to leaving a patient untreated. This ethical commitment drives their innovative efforts, anchoring them in patient-centered care rather than personal gain.
The Evolving Cycle 2
The second cycle generally begins at the fifth stage, Excellence, where the involved practices become more complex due to the expertise gained from high-quality cognitive productivity. The first phase of this cycle mirrors the third phase of the first cycle, though it is more specific in addressing a challenging phenomenon.
The innovation cycle starts early in a surgeon’s education and matures through experience, culminating in the fifth stage of excellence. At this peak, as illustrated in Figure 5, surgeons utilize their accumulated knowledge to address contemporary clinical challenges and improve patient outcomes, thereby enhancing the potential for significant advancements in surgical medicine.
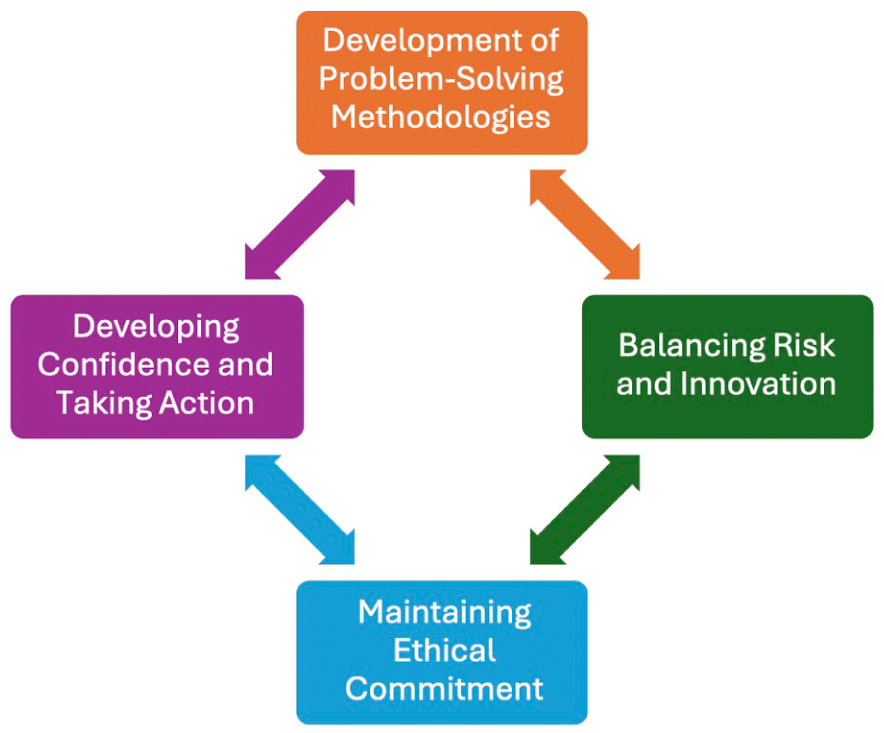
The Evolving Cycle2.
Exceptional Leadership Context
This context includes seven essential requirements: teamwork, valuing others, collaborative decision-making, owning mistakes, logical reasoning, strategic planning, and fostering innovation: True leadership is about attracting exceptional talents to ensure the continuity of achievements, not fearing competition. Real success is when a place continues to thrive even after you leave. (Najm) . . . I also learned the importance of proper planning, continuous review, and precise follow-up. Leadership, including charisma and ethics, requires the ability to take responsibility and make sound decisions, along with the courage to acknowledge and rectify mistakes when necessary. Transparency, justice, and innovation are also key elements of effective leadership success. (Al-Rabeeah)
Exceptional Leadership and Global Innovation
While each context has its specific focus, they interact dynamically and complement each other within the broader context of excellence. In the higher stages of excellence, particularly the fifth stage, the focus shifts toward developing other leaders and ensuring the continued excellence of the institution beyond personal achievements. This mirrors the innovation cycle, where the goal is not just individual creativity but also the collective advancement of the medical field. Together, leadership and innovation form a dynamic and complex system that fosters both individual and institutional excellence. Their interaction ensures that medical professionals not only push the boundaries of knowledge but also create environments that sustain and amplify these innovations for broader impact: Leadership in surgery consists of two stages: the first is leadership in the operating room, where the surgeon leads the team to ensure the success of the procedure. The second is administrative leadership, which involves managing a department or institution . . . A true leader does not focus solely on personal prominence but works to elevate everyone together, improving outcomes and enhancing the reputation of the institution. (Al-Aklabi)
ASET Model
At the conclusion of the findings section, we present an integrative overview that synthesizes the developmental dynamics of surgical excellence. This final theoretical model, illustrated in Figure 6, outlines the key levels through which surgeons progress, capturing the interplay of contextual, psychological, and professional elements. Each level functions not only as a formative foundation for the next, and also as a critical point of cognitive and professional reinforcement.
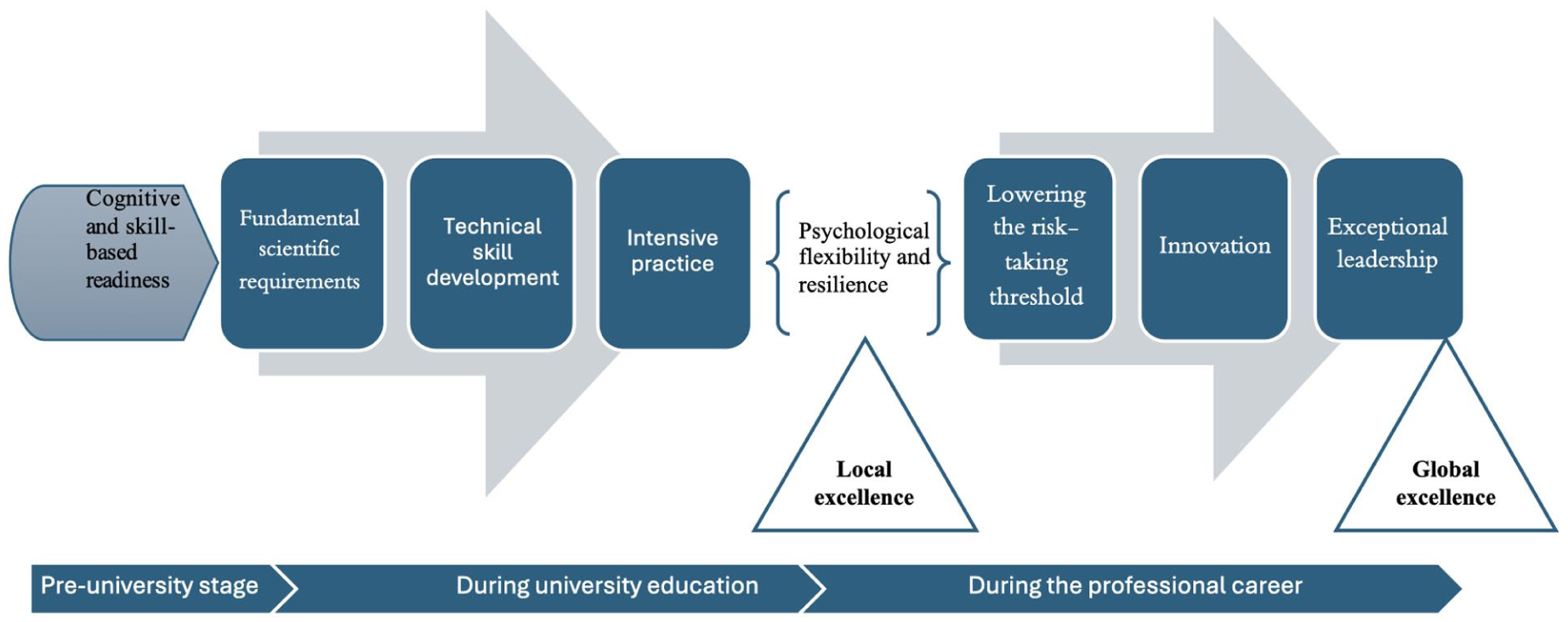
Ascending Surgical Excellence Trajectory (ASET Model).
What distinguishes this theoretical synthesis is that it moves beyond general patterns of excellence across professions to present a domain-specific developmental trajectory for achieving professional excellence and cognitive productivity in surgical medicine. While similar levels may be observed in other fields, their articulation here highlights both their demanding nature and their distinctive temporal sequencing—each level tends to emerge more prominently at specific points in a surgeon’s career trajectory. Moreover, each level operates as a structural prerequisite that lowers the threshold for progression to the next, thereby capturing the sequential and constructive nature of this developmental pathway.
Take, for instance, the level of lowering the risk-taking threshold: this developmental point cannot be reached without adequate accumulation from preceding levels over a relatively extended period. Likewise, the transition to the next level—innovation—becomes difficult without a solid foundation in this critical level. This interdependence underscores the layered and cumulative structure of the model.
Discussion
Excellence among surgeons is framed as a context-dependent trajectory characterized by dynamism and complexity, spanning preparation, proficiency, expertise, professionalism, and excellence. Unlike general frameworks, this domain-specific synthesis highlights the distinctive, interdependent processes that drive excellence in surgical medicine.
The Context and Sub-Contexts Shaping Excellence
The findings of this study highlight the significance of an integrated context for achieving professional excellence. In line with Simonton’s (1994) argument, the personality characteristics observed among distinguished surgeons in this study did not function in isolation but rather interacted in complex ways, contributing to their overall cognitive productivity and excellence. Moreover, our findings emphasize the interaction between individuals and their environments, as these evolving contexts played a key role in shaping the surgeons’ progression from early aptitude to maximal adaptation (D. Dai, 2021). In addition, insights from our study underscore the significance of psychological and social elements and how they interact within domain-specific excellence (Aljohar & Alarfaj, 2024; Plucker et al., 2021; Sternberg et al., 2024). The findings further illustrate how this perspective goes beyond individual characteristics and the immediate environment, pointing to a broader, interconnected system that shapes the context in which individuals develop. Therefore, the unit of analysis is not the person or the environment in isolation but rather the entire context (actiotopes), which includes the individual along with the material, social, and informational environments they engage with (Ziegler & Stoeger, 2019). This integrated context is essential for nurturing talent and supporting sustained excellence.
The Dynamism and Complexity Within the Context Nurturing Excellence
Family Context
Early family experiences provided the initial conditions in which individual potential was identified, encouraged, and developed. These dynamics often involved consistent encouragement, resources, and expectations that framed long-term professional goals, showing how families can act as catalysts for sustained development (Sloane, 1985). Crucially, what mattered was not ideal environments but the interaction of capital resources that amplified experiences and transformed them into formative knowledge. It is this systemic convergence of resources that fosters excellence, rather than their mere presence (Ziegler & Stoeger, 2019).
Although this study found that some participants faced obstacles, such as limited economic, social, or cultural capital that hindered certain educational aspirations, they generally experienced stable and supportive childhoods. This aligns with evidence that many eminent individuals were raised in intellectually stimulating environments with resources and at least one supportive parent (Goertzel & Hansen, 2004). In surgical excellence, such environments likely fostered early commitment to learning, high performance, and sustained motivation. However, the literature also shows that many high achievers grew up amid adversity—family conflict, poverty, illness, or loss—which often built resilience and intrinsic motivation (Goertzel & Hansen, 2004). The absence of such patterns reflects participants’ stable childhood backgrounds. The findings underscored the importance of complex parenting systems that balance differentiation—allowing children to face challenges independently—and integration—providing support when needed (Gute et al., 2008). In our study, such early parenting approaches contributed to shaping surgeons’ adaptability under high-pressure demands and their sustained professional excellence.
Educational Context
One of the most distinctive characteristics of surgical medicine is that it is both a profession and a craft practiced within a high-risk environment (Hardré et al., 2017). This dual nature adds complexity to the educational components it requires. The findings revealed that early engaging educational environments, including authentic, challenge-based programs and early field experiences, significantly enhanced surgeons’ motivation, curiosity, and skill development. These findings align with the study by Duncan et al. (2007), which noted that high-achieving individuals often credited their early supportive environments, where learning and curiosity were highly valued. Such environments provided the foundation for characteristics like perseverance and adaptability, which later became essential in navigating the demands of their careers. Consistent with Portenga’s (2018) emphasis on the role of stimulating experiences, participants described how such exposure facilitated their choice of surgical medicine and helped them develop foundational skills that prepared them for the field. Furthermore, the findings extend Subotnik et al.’s (2018) argument regarding the impact of early exposure to diverse opportunities, demonstrating that these experiences not only enhance critical thinking and problem-solving skills but also foster a mind-set oriented toward innovation and excellence.
The study also aligns with Hardré et al. (2017), which indicated that the development of fine motor skills and manual dexterity is essential in surgical training, as these activities demand cognitive skills related to understanding procedural techniques as well as precise hand-eye coordination. Moreover, Karmali et al. (2018) demonstrated that early and structured surgical skills training using simulation for preclinical medical students significantly improved their competence, confidence, and interest in surgical specialties. However, the findings of this study highlight the importance of exposing students to such opportunities during general education through structured scientific programs in surgical medicine. This training includes simulating basic procedures, such as suturing wounds and closing incisions after surgery, using synthetic models that replicate skin and tissue. This approach helps identify students’ surgical potential and fosters their early interest and creative skills.
These findings further highlight that the interplay between personal characteristics and supportive environments forms the cornerstone of excellence, demonstrating how early educational contexts equip individuals with the resilience and cognitive capacity necessary for excelling in a highly demanding field like surgery.
Dynamism and Complexity in Professional Excellence
Developing Surgical Expertise
The findings of this study indicate that professional excellence develops through a combination of rigorous educational experiences and relational dynamics. Participants emphasized the impact of studying at elite institutions, where academic pressures often challenged their creative resilience and adaptability (D. Dai & Li, 2020; Gute et al., 2016). Although these demands could be discouraging, they were also seen as opportunities to build problem-solving skills and strengthen persistence. Surgical experience further contributed by reducing stress and increasing confidence, which improved performance in simulation-based training (Tjønnås et al., 2024). These results align with the perspective that expertise emerges through varied learning experiences shaped by interpersonal interactions (Norman et al., 2018). Collectively, the findings highlight how individual growth is intertwined with the social contexts that refine and reinforce professional development in surgery.
Underrepresentation of Female Surgeons
The findings suggest that the underrepresentation of female surgeons cannot be separated from cultural context. Early encouragement of scientific curiosity and ambition often favored males, reflecting entrenched dynamics that perpetuate gender bias in Saudi Arabia. This is consistent with research showing how cultural norms and family expectations shape women’s participation in male-dominated professions. For example, Al Hulaibi et al. (2024) found that although female medical students comprised 55% of their sample, they still faced barriers, such as perceptions of male dominance, limited female role models, and concerns about long training and work–life balance. Similarly, Aljuaid and Liu (2023) reported sociocultural barriers restricting women’s participation in cybersecurity, reflecting broader patterns in technical fields. These insights from Arab contexts can be interpreted through Hofstede’s framework: high power distance and collectivist orientations reinforce hierarchical gender roles, while uncertainty avoidance contributes to societal hesitance toward women entering long and demanding professions, such as surgery (Persson, 2012).
A systematic scoping review further demonstrated that women remain underrepresented even in highly individualist contexts, such as the United States, Canada, and Europe, where they comprise only 14–25.7% of surgeons (Bucknor et al., 2018). The review identified barriers, including gender bias, limited mentorship, few female role models, and challenges of pregnancy and child care, alongside difficulties in achieving work–life balance. From Bourdieu’s perspective, these disparities reflect unequal access to social, cultural, and economic capital: women frequently encounter restrictions in mentorship and recognition, while familial or societal expectations shape a habitus that channels them away from demanding professions (Bourdieu, 1986).
What emerges, therefore, is not merely a description of cultural and structural barriers but an interaction between them: Hofstede’s cultural dimensions frame the societal logic legitimizing gendered hierarchies, while Bourdieu’s capitals explain how these hierarchies are reproduced through unequal access to mentorship, networks, and recognition. For example, high power distance sustains acceptance of male-dominated authority structures, restricting women’s ability to accumulate the social capital necessary for advancement. Likewise, collectivist orientations reinforce familial expectations that shape women’s habitus, often channeling them away from demanding professions. At the same time, cases, such as that of Dr. Salwa Al-Hazzaa, illustrate how this interaction can be negotiated differently. She emphasized that her early schooling in the United States—within a cultural context characterized by greater individualism according to Hofstede—together with her father’s strong encouragement and later her husband’s support, provided her with independence and resilience. This unique combination of early exposure to individualist values and sustained familial support enabled her to navigate cultural expectations and achieve distinction. In this way, the two frameworks together explain not only how gender disparities in surgical excellence are continuously produced and maintained, but also how specific forms of capital—when aligned with supportive cultural and familial factors—can enable individuals to overcome barriers and pursue excellence.
Formation Pathways of Professional Excellence and Cognitive Productivity
Early exposure to positive learning contexts and formative relationships with mentors and role models played a critical role in shaping identity and developing core competencies (Hardré et al., 2017). As tasks became more complex, attributes, such as commitment, confidence, and focused self-regulation became increasingly essential (McDonald et al., 1995). Participants described how growth depended not only on accumulating experience but also on engaging in structured, goal-directed training that challenged their limits and incorporated continuous reflection and feedback (Ericsson, 2011; Ericsson & Pool, 2016).
In addition, the findings indicate that progression toward professional excellence and cognitive productivity mirrors the stages identified by Subotnik et al. (2021): transforming abilities into competencies, competencies into expertise, and expertise into creative productivity and eminence. This developmental trajectory aligns with Bloom’s (1985b) and Ericsson’s (2018) emphasis on long-term dedication as a foundation for expertise. Complementing this perspective, D. Y. Dai (2024) offers a comprehensive framework that underscores the diverse pathways to excellence and the dynamic interaction between individuals and their environments, highlighting the plurality of developmental potentials. Our findings combine the stage-based model with the diverse pathways approach, describing the stages of excellence among surgeons and the dynamics shaping their innovation and leadership. While specific stages of development—preparation, proficiency, expertise formation, professionalism, and excellence—can be identified, individuals may still navigate the levels of cognitive readiness, skill acquisition, intensive practice, resilience, innovation, and leadership in unique ways, forging their own distinct paths to professional excellence.
Leadership and Innovation
Lowering the Risk-Taking Threshold
The findings of this study regarding the principle of lowering the risk-taking threshold align closely with evidence indicating that expert surgeons engage in comprehensive mental preparation and scenario planning before undertaking procedures. Rather than relying on descriptive, fact-based knowledge, experts generate forward-looking mental representations of possible intraoperative challenges and adaptive strategies, enabling them to anticipate obstacles and respond flexibly as situations evolve (Ghaderi et al., 2021). This dynamic anticipation reinforces the idea that the ability to take calculated risks emerges not solely from experience but also from sustained, deliberate efforts to refine both cognitive and behavioral capacities.
Such a perspective is consistent with Ericsson’s framework of deliberate practice, which emphasizes the necessity of extended, purposeful training aimed at overcoming performance limitations and developing professional mastery (Ericsson, 2018). Over time, this process supports a gradual lowering of the threshold for engaging in high-stakes decisions, as practitioners accumulate procedural expertise and the confidence to apply it under uncertainty.
In addition, these findings resonate with Csikszentmihalyi’s (1996) observations that creative individuals often combine a willingness to engage in risky, novel endeavors with a disciplined commitment to caution and safety. This interplay of courage and prudence was evident in the surgeons’ prioritization of patient welfare over personal recognition, suggesting that professional excellence depends on an ethical orientation as much as technical proficiency. Together, these theoretical perspectives highlight the importance of environments that foster both deliberate practice and reflective anticipation of risk, supporting the development of expertise grounded in responsibility and care.
Integrated Dynamics for Achieving Professional Excellence
The findings emphasize that effective leadership is not simply an inherent trait but also develops through interaction with the professional environment. While Aguinis (2023) identified leadership as essential for inspiring performance and innovation, this study shows that such leadership actively drives innovation among surgeons by enabling creative problem-solving and supporting adaptation to complex situations. Participants described how strong leaders and mentors helped them leverage challenges into opportunities for growth.
Regarding innovation, the results align with Leone and Reiter-Palmon’s (2022) view that effective leadership creates conditions for solving complex problems in novel ways. The current study further demonstrates that surgical practice and research benefit significantly when continuous support is provided by leaders. The relevance of these findings is also reinforced by Riskin et al. (2006), who noted that although surgical innovation has a strong tradition, institutional support has remained inconsistent. This research extends that perspective by illustrating how leadership, mentorship, and developmental processes together foster environments in which innovation becomes sustainable and embedded within the culture of surgical excellence.
Conclusion and Implications
This study conceptualized surgical excellence as a dynamic, context-dependent process evolving through developmental stages and levels. A key implication may be the importance of early, structured educational environments that balance firmness with care and emphasize experiential learning. Such settings can help individuals build the knowledge, habits, and decision-making skills that are potentially essential for excellence. Scientific enrichment and preparatory programs during general education could shape early professional orientation, while robust mentorship systems and targeted guidance—particularly for women aspiring to surgical careers—at the university level may further strengthen technical competence, psychological resilience, and confidence.
Innovation in surgical education might be fostered through exposure to complex cases, supervised decision-making, and interdisciplinary learning. Programs are encouraged to create safe spaces for experimentation, integrate innovation-focused modules combining clinical practice and research, and develop research centers that promote cognitive productivity and innovation. Embedding leadership development through simulations, tiered mentorship, and interdisciplinary case discussions could help cultivate readiness for leadership responsibilities.
Future research should further explore how mentorship, innovation, leadership, and education interact to shape surgical expertise across diverse cultural and institutional settings. These contexts include value systems, educational philosophies, and family support structures that form the developmental ecosystem for excellence. A cross-cultural perspective may yield valuable insights into how environments influence the motivations and practices sustaining high performance. Subthemes, such as innovation, calculated risk-taking, leadership, and intensive practice merit additional investigation.
Overall, these findings suggest the multidimensional nature of excellence in surgery and point to potential strategies to improve education, professional development, and institutional culture. Adopting these principles may help prepare future surgeons who combine technical skills with innovation, leadership, and ethical commitment.
Limitations
This study focused on six distinguished surgical consultants, as elite professionals often have demanding schedules. Baker and Edwards (2012) argue that six participants can be sufficient in qualitative research with hard-to-reach elites. Charmaz (2025) notes that while larger samples may enhance conceptual saturation, smaller samples can still yield meaningful insights when rigorously analyzed. Despite the limited size, the findings offer valuable contributions. As Charmaz emphasizes, ongoing scrutiny and further analysis in future studies may enrich the conceptual development of this area.
Footnotes
Acknowledgements
The authors gratefully acknowledge King Faisal University for its valuable academic support and encouragement of research that contributed to the completion of this work. The authors also extend their sincere appreciation to the distinguished surgeons who generously shared their time, experiences, and professional insights, which were instrumental in shaping the depth and rigor of this study.
Ethical Considerations
Ethical approval for this study was obtained from the Research Ethics Committee, Deanship of Scientific Research, King Faisal University (approval no. KFU-REC-2023-MAR-ETHICS3230) on March 10, 2023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Open Science Disclosure Statement
The data analyzed in this study are not available for purposes of reproducing the results. The code or protocol used to generate the findings reported in the article is not available for purposes of reproducing the results or replicating the study. There are no other newly created, unique materials used to conduct the research.
Artificial Intelligence Use
Google Translate and ChatGPT were used to improve language clarity and organization. The authors declared they took steps to ensure accuracy of AI-generated content, and that it contained no plagiarism or bias.