
Abstract
Introduction
South Asians living in Canada, European Union countries and the United States are at increased risk for cardiovascular disease, type 2 diabetes, obesity, and metabolic syndrome, compared to Caucasians living in the same countries 1–5 . Historically, these conditions were much less common in South Asian countries (that is, the Indian sub-continent, including India, Pakistan and Bangladesh) but incidence is increasing there as well, in conjunction with the processes of urbanization and westernization 6 . Diet change has been suggested as a primary contributor 7 . Compared to diets in their region of origin, South Asians living in Britain have diets higher in energy and fat 8 , containing more meat, sugar and fast foods 9 , and less vegetables, fish and dairy products 9 . In Scotland, immigrant South Asians’ diets had a more atherogenic profile than the diets of British-born South Asians or the general population, with higher energy, per cent energy from fat and per cent energy from saturated fat 10 . A Canadian study, in contrast, showed that South Asian Canadians consumed less total fat than Canadians of European, Chinese and Aboriginal origins, but higher amounts of sugar and total carbohydrate 11,12 . Despite the variations in findings, this body of research suggests that diet contributes to disease burden in migrant South Asians and provides evidence for the need for health promotion and nutrition education services for this group.
Provision of culturally sensitive health education programmes requires not only that such programmes are attentive to observable characteristics of the target group, such as language and foods commonly eaten, but also that they incorporate understanding of cultural, social, environmental and historical influences on health behaviours 13 . Yet some South Asians in western countries have reported that dietary advice does not take into account how their food practices are shaped by culture or migration 14,15 . Many programmes attempt to rectify ‘deficiencies’ in knowledge or ‘incorrect’ dietary practices, rather than building on the beliefs, attitudes and behaviours that already exist within communities to promote healthier lifestyles and improve quality of life 15,16 .
Some qualitative researchers have begun to address this need by examining social and cultural factors associated with dietary practices of first and second generation South Asian migrants. Findings have highlighted use of, preferences for and beliefs about traditional South Asian foods compared to ‘western’ foods 17–20 , as well as the cultural significance of foods for entertaining and celebrations 21,22 . Much of this research has been conducted in Britain and has examined food practices from the perspective of individuals rather than within family contexts. Few studies have explored food practices within the context of everyday family food decision-making, such as the perspectives of family members from different generations regarding the meanings of food, health and well-being that influence everyday family food decision-making. With one exception 19 , no research has addressed the cultural meanings of food practices for South Asians in Canada.
We therefore conducted this study to examine the meanings of food, health and well-being that are embedded in the food practices of Punjabi families living in Metro Vancouver, Canada. With an estimated population of 90,000, South Asians comprise 4.5 per cent of Vancouver’s total population, the second largest visible minority group in Vancouver after Chinese 23 . Most members of this community are Punjabi Sikhs, originating from rural areas in the Punjab region of northern India. The community has existed since the early 1900s, with most immigration having taken place since the 1970s.
Materials and methods
The data presented in this paper were collected as part of a larger qualitative study of family food decision-making in specific ethno-cultural groups in Canada 24–26 . Following approval from the University’s Research Ethics Board, Punjabi families living in Vancouver were recruited through key informants and snowball sampling. Purposive sampling recruited families from varied circumstances, including time living in Canada, family structure, education and occupation. All participating families identified themselves as of both Punjabi background and Sikh religion. These identities reflect the majority of Punjabi families who have settled in Vancouver, yet differentiate from more generalized ‘South Asian’ or ‘Indo Canadian’ identities. While the two ‘Punjabi’ and ‘Sikh’ identities are often used interchangeably by the community itself, there are intergenerational differences in how the religious aspects are drawn upon 27 .
To allow exploration of intergenerational influences, each family included at least one woman aged 25–55 years and two others over 13 years who were willing to be interviewed. Because many families lived in multigenerational households, participants included middle-generation adults, their children or children-in-law (here referred to as ‘youth’) and their parents or in-laws (here referred to as ‘elders’). Family members were generationally categorized based on life-stage and relationship in the family, so that an ‘adult woman’ was a woman who had children and/or parents/parents-in-law living with her in the family. This woman was also considered the main food provisioner in the family, although she sometimes shared this role with her mother/mother-in-law. Of the 12 participating families, three were nuclear families with an adult male, adult female and one or more children, one was a single mother with young adult children, and eight were multi-generational.
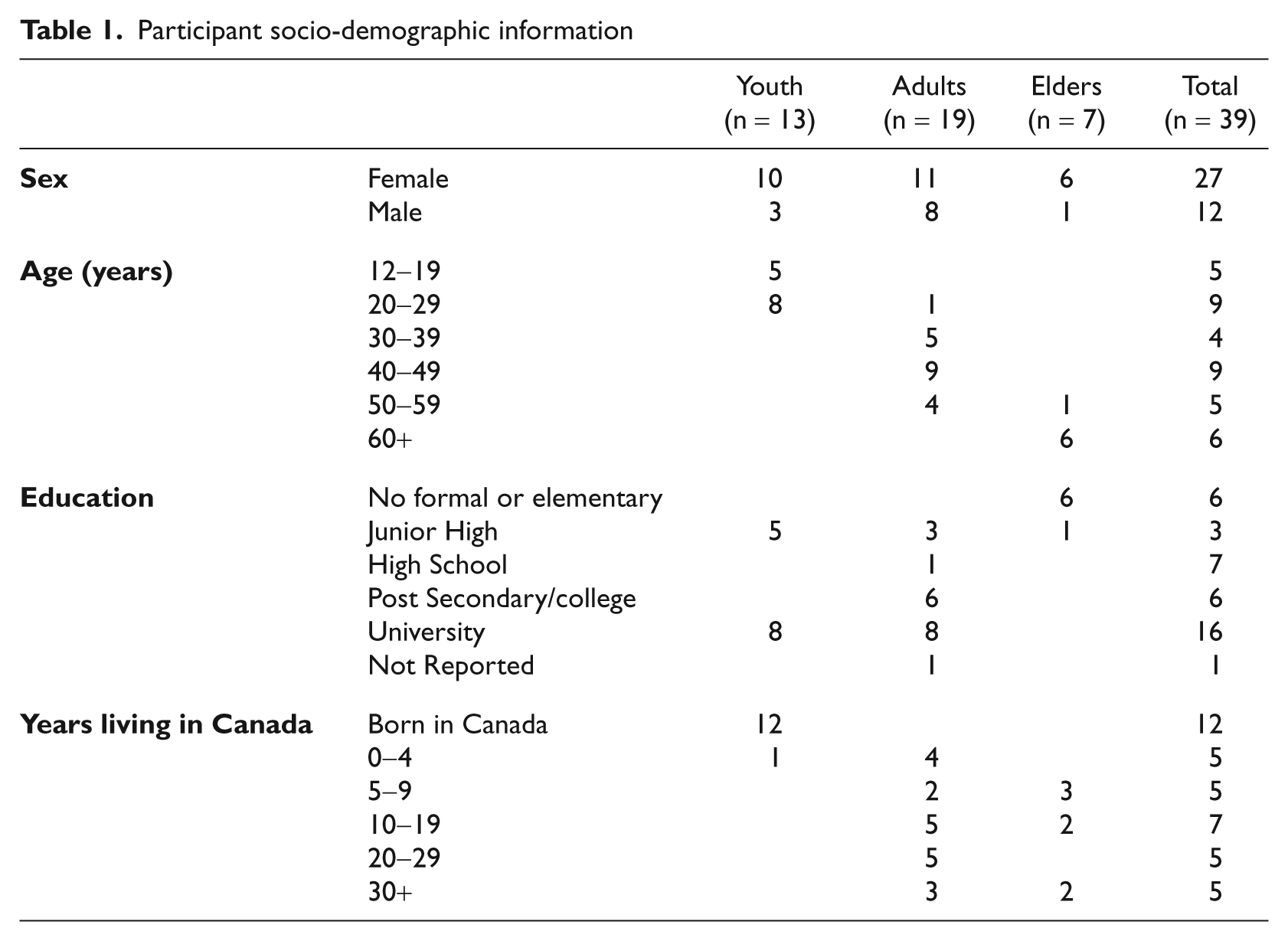
As shown in Table 1, 39 individuals were interviewed, including 13 youth, 19 adults and 7 elders. The sample included a disproportionate number of women, partially because of our requirement that each family include an adult woman who was willing to be interviewed, but also because the women in each family were more inclined to agree to be interviewed. All youth were in public school or university, or had completed university. All but one youth had been born in Canada; one teen had emigrated from England four years previously. Adults tended to be well-educated, with some post-secondary education. Most had migrated to Canada from India, although three adults had emigrated from England four to 13 years previously. The elders had little or no formal education and had emigrated from India five to 36 years previously. Most families had multiple wage earners, with relatively high household incomes.
Participant socio-demographic information
Individual semi-structured interviews were conducted in the family’s home by a bilingual Punjabi-Canadian interviewer, in the language preferred by the participant. The interview guide included questions about family and individual eating patterns; the influence of food preferences, health concerns, cost and culture; how food decisions were made; and changes over time. Data collection also included two participant-observation components. The interviewer accompanied the family’s usual grocery buyer on a shopping trip to a grocery store where the family usually bought food, to observe the routines, patterns and food decision-making processes that occur while shopping for food. The interviewer also attended one family meal to observe preparation, cooking, eating and clean-up activities of family members. Interviews and shopping trips were recorded and transcribed verbatim, and field notes were recorded for the meal observations. Interviews conducted in Punjabi were translated at the time of transcription by a bilingual transcriber. Adequacy of translation was verified by the original interviewer.
Data were analyzed inductively using a constant comparative method. Themes were generated through in-depth examination of transcripts by sorting, clustering and comparing segments of text to describe, organize and interpret the influences on participants’ food decision-making 28 .
Findings
Food practices in Punjabi Vancouver families
Participants talked about family food choices being influenced by ages of family members, time in Canada, health concerns, preferences and work schedules. However, the main theme emerging from descriptions of what they ate was the contrast between elders’ reliance on traditional Indian foods and young people’s desire for ‘western’ food.
There was consensus amongst participants that eating Indian foods meant eating meals consisting of roti (flat bread), dahl (lentils) and subjee (vegetables). Some participants also mentioned including a meat dish with the meal, but Indian meals were often meatless. Many participants were vegetarian because ‘it’s just the way we’ve been brought up’ or for religious reasons (in this community, many devout Sikhs are vegetarian). Others ate chicken or beef some days of the week, but vegetarian meals the rest of the time. Regardless of whether or not the meal included meat, participants simply referred to eating an Indian meal as ‘eating roti’. There was more variation in how participants described ‘Canadian’, ‘English’, or ‘western’ food. Pasta and pizza were the most frequent examples, but sandwiches, burgers, soup and salad were also commonly mentioned.
Elders preferred to eat traditional Indian foods every day. Eating roti was satisfying for them in a way that other foods could not be. As one elder man said: ‘I stop feeling hungry and am satisfied if I eat roti … It is important for me to eat roti at least once a day.’ In contrast, many teen and young adult participants preferred to eat Indian meals only occasionally. One young man said: ‘Cultural foods – maximum four meals a week. No more. Like, you know, I can’t eat roti seven days a week. Breakfast and lunch, it’s always western food, right, and half of the time dinner is western food.’ Participants in the middle generation were less predictable in their preferences. Some adults found it easy to eat foods from both cultures: ‘I like both Indian and Canadian food; same is the case with my husband, so we both usually eat what is cooked.’ Others, however, craved Indian food: ‘I can’t survive without roti for more than 2 days. I look for roti whenever I can get it.’ Interestingly, both of these adults had lived in Canada for the same length of time: 24 years.
Meanings of food and well-being
Participants’ discussions of the reasons for and effects of their food choices revealed two dominant themes: association of food practices with physical health, and supporting the psychosocial well-being of family members.
Physical well-being
All participants were aware of, and discussed frequently, the relationship between food and the body. Some participants’ beliefs reflected a nutritional science approach to food and health focusing on long-term implications of specific ways of eating. Many comments included general references to ‘being healthy’, while other statements were about diet affecting risk for specific diseases like diabetes and cardiovascular disease. For example, when asked how healthy she thought her eating habits were, one woman responded:
I have a sweet tooth so I tend to eat sweet stuff, cakes and stuff. I eat more than I should probably. [But] overall it’s not bad. I am eating vegetables and stuff, but I probably should be cutting back on more of the greasy stuff [because] in my family there’s a history of heart problems so that’s a bit of a concern as I’m getting older.
Participants with this long-term approach to food and physical well-being described ‘healthy eating’ in ways that reflected official Canadian nutrition guidelines: eating more fruits and vegetables, reducing fat intake and choosing from different food groups. They also used the language of nutritional science, referring to specific, often invisible, components of food that they saw as ‘bad’ (such as sugar, fat and cholesterol) or ‘good’ (such as vitamins, minerals and fibre):
Healthy eating would be making sure that you eat proteins, a certain amount of carbohydrates and getting your minerals and vitamins in, and then making sure that you’ve got enough of each of the servings per each of the food groups again.
Within this way of understanding food and health, there was a tendency to equate healthy eating with ‘Canadian’ foods, and to criticize Indian foods as unhealthy. Participants talked about needing to use oil instead of ghee or butter in their cooking, using low fat instead of whole milk, and the high sugar content of Indian sweets. As a 21-year-old woman said:
I guess the way we make our food and stuff, like it’s all enriched with oil and salt and all that. Even though we do have lots of vegetables and stuff but even our sweets are very sweet, like they’re over packed with sugar and so I guess that doesn’t always promote healthy eating.
At the same time, these participants also identified some Canadian food, particularly ‘junk food’ and ‘fast food’, as unhealthy.
In contrast to the nutritional science approach to food and physical well-being, some participants employed knowledge based on wisdom passed down for generations in their culture, and their own bodily experiences. They believed traditional Indian foods are healthy because they have eaten that way ‘from the beginning’ and have always been healthy. The focus was on fairly immediate effects of food on the body, such as providing satiety, energy and strength. When a 70-year-old woman was asked what she thinks is ‘good’ about the way she eats, she talked about the importance of eating roti:
Roti has a lot of strength in it. Dahl and subjee. They have a lot of strengths. … It is very good for the health. … Whatever I eat, I am able to digest, I am okay. It doesn’t bother me. So why should I have any concerns?
Participants also spoke of foods having hot and cold qualities, not related to temperature, but to their ability to be cooling or heat inducing within the body. A 62-year-old woman explained that ‘If you eat cold things then your body contracts and you feel sick, but if you eat hot foods then you feel better and do not fall sick’. Ginger tea was frequently mentioned as a remedy for ‘bai’, a condition variously described as ‘indigestion’, ‘nausea’, ‘sour burps’, ‘excess water in your mouth’ and ‘backache, stomachache or knee ache’. Some participants also talked about eating ‘pinni’, a mixture of ground flax seeds, nuts, moongi flour and black pea flour, to provide energy and aid memory. One adult woman commented:
They say that the black pea flour and moongi flour are very good for health. My mum and other elders. My mum says that the flax seeds also help to reduce cholesterol and are also good for health and even nuts like almonds are very good for health. So this continues from generations. So the main thing is that if the person who eats the foods feels the difference, then it is worth it. If someone says to make it, and I make it, but the person does not feel any difference, then there is no point to making it.
Elder participants generally (but not always) talked about ‘healthy’ aspects of eating in traditional terms, while teens and young adults who were educated in Canada tended to express the scientific way of thinking about food and nutrition and often either rejected traditional beliefs (eg, stating that they do not believe in remedies for ‘bai’) or had no knowledge in this area (eg, many youth did not recognize the term ‘bai’ when asked about it). Some adults from the middle generation drew exclusively on one or the other discourse, as with ‘Mr. Singh’ (interview excerpt Figure 1), who appeared to have no familiarity with the nutritional science approach. Most middle-generation adults, however, related to both ways of thinking about food and physical well-being, often drawing on them in a ‘mix and match’ fashion, as in the quote above where the woman refers to flax seeds having specific benefits for reducing cholesterol (nutritional science approach) as well as to the importance of both received wisdom from elders and one’s personal experience of one’s body as sources of knowledge (traditional approach).
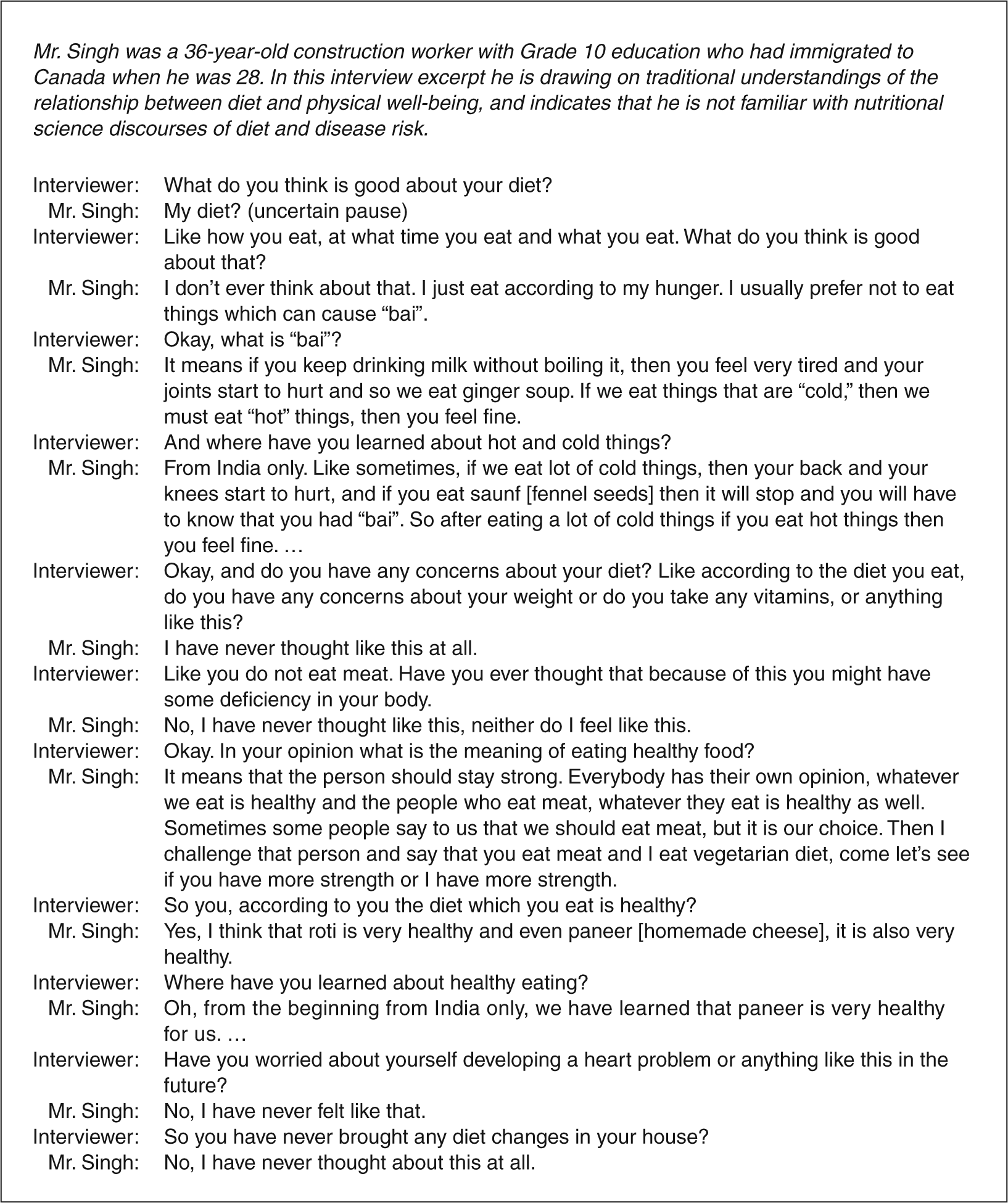
Interview transcript illustrating traditional understandings of diet and physical well-being
Adults who drew on both understandings of food and health expressed contradictory views and confusion about the healthfulness of Indian food. For example, ‘Mrs. Singh’, an educated woman who had been in Canada four years longer than her husband, talked about serving roti to her children ‘as it is healthy food and it is not junk food, and they will remain healthy’. However, later in the interview she said, ‘We do not get all the nutrition from roti, so we eat food from different cultures … sometimes when we cook dahls, we lose its nutritional value as we cook it for a long time’. At the end of the interview, when asked if she had any questions for the interviewer, she said:
Just that we should get information as to what is good and healthy to eat, especially in Indian food, as here we come to know a lot about the English food, as to what is good and nutritious but not for the Indian food. Like how good is dahl for us and how much should subjee be cooked. No one tells us these things.
Overall, the scientific approach to food and health was used and valued within the Punjabi Vancouver families. At the same time, other understandings of food and health based on centuries of tradition were prevalent. Individual members of the community differed in the extent to which they used different approaches, depending at least partially on age, education, and time since immigration.
Food, caring and happiness
The second main theme that emerged from participants’ discussions of their food choices concerned a different kind of well-being, the psychosocial well-being of individual family members. When grocery shopping, planning menus and preparing meals, adult and elder women were attentive to the preferences of individuals in the family, ensuring that everyone felt loved and cared for. During grocery shopping trips, they often explained food selections to the researcher by explaining that one or more family members liked and/or had requested that food. One mother talked about feeling stressed when she was shopping because she had to balance the children’s preferences with what she considered to be healthy foods. When asked how they decide what to serve for dinner, many women said they would prepare what their children wanted to eat. This mother of three children (ages 8, 12 and 15 years) described a typical scenario:
Sometimes I ask them [the children] what they want to eat and then I cook according to their wishes. … Mostly they like the same. The same food is cooked for all of them. But one drinks juice, other likes milk, so there might be difference in preferences like this, otherwise they eat the same food. Sometimes if one of them says that he or she doesn’t want to eat roti and says that he or she wants to eat pizza pop then I let him or her eat it.
A grandmother in another family stressed the importance of pleasing those who will be eating: ‘I feel that they should eat and be happy’. While women food-preparers did not talk as frequently about asking the adult men in the household what they wanted to eat, it was apparent that the women were well aware of men’s food preferences. As one woman said, ‘Over the years I’ve got to know their likes and dislikes so I won’t tend to make what they don’t like’.
Discussion
This qualitative study of the food practices of Punjabi families in Vancouver, Canada, contributes to a growing body of literature exploring the social and cultural meanings underpinning the eating habits of first and second generation South Asian immigrants. Findings add to understanding of the varied ways food practices are implicated in constructing ethnic identities, provide insight into cultural influences on health behaviours, and help provide direction for health promotion and public health nutrition practice.
Meal patterns of participants in our study showed the simultaneous persistence of traditional cuisine and significant incorporation of western foods, similar to what has been observed with other South Asian migrant communities 7,17–20,29 . In these studies as well as ours, families served hot meals based on traditional meal patterns most evenings. The western foods commonly consumed as snacks, at breakfast and lunch, and for occasional evening meals tended to be easily prepared foods such as convenience, frozen or take-out products.
A unique aspect of our study was the inclusion of participants from three generations. Although others have noted that use of western foods is encouraged by children and associated with their exposure to these foods at school 19,20 , our inclusion of the perspectives of youth, parents and grandparents highlights how different values and preferences for Indian versus western foods are most distinct between youth and their grandparents: some youth insisted on limiting Indian meals to three or four times per week, while many elders insisted on consuming such foods at least daily. The youths’ insistence on eating ‘Canadian’ foods can be seen as a tangible symbol of their development of a Canadian identity, particularly in their interactions outside the home. At the same time, many of the youth continued to enjoy eating Indian foods frequently (but not daily) at home, and talked about enjoying this aspect of their culture, thus enacting a hybridized Punjabi-Canadian identity 30 . Mothers and grandmothers supported the development of their children’s hybridized identities by accommodating their wishes to not eat Indian food every day. The elders, in contrast, had fewer social interactions outside of their family and community; their almost exclusive consumption of Indian foods can be seen as parallel to their maintenance of a predominantly Punjabi identity.
Our findings are also unique in identifying two distinct approaches to understanding relationships between food and health. Other studies exploring these concepts with South Asian migrants have focused on adults with diabetes 14,16–18 or cardiovascular disease 15 . These participants were mostly older adult immigrants, and there are similarities between these reports and the traditional understandings communicated by elders and some adults in our study. These include the emphasis on strength-giving properties of roti, and some lack of understanding of the meaning of terms like ‘diet’. Chowdhury and colleagues 17 provide a particularly detailed explanation of how their British Bangladeshi participants classified foods according to their nourishing power (strong/weak) and the ease with which that power could be extracted from foods (digestible/indigestible). The conceptualization of foods as providing strength and energy described there is very similar to that described by some of the Vancouver Punjabi participants. Although the Vancouver participants did not emphasize digestibility as much as the strength-giving properties of food, some did comment about decreased ability to digest ‘heavy’ foods as they aged, and when they were less physically active.
In contrast to traditional beliefs, many younger participants in our study articulated a nutritional science approach to food and health that was mostly indistinguishable from that communicated by European Canadians in another arm of our study 26 and showed familiarity with and acceptance of official Canadian nutritional guidance. Thus, although it has been suggested that in western countries, encounters between health professionals from the dominant culture and clients from minority groups likely involve a meeting of different views of illness and strategies to manage or prevent disease 14 , our findings suggest this is not always the case. Some clients, especially younger people, those with higher education levels and/or those who have lived in the west longer, may share some of the understandings of health professionals, either drawing almost exclusively on nutritional science approaches, or using both traditional and professional knowledges.
Finally, our findings show that many participants thought of their traditional foods as unhealthy, or potentially causing disease. This devaluing of traditional Indian cuisines has been noted elsewhere 14,18 . It appears that despite the nutritional strengths of traditional Indian cuisine, such as the high content of vegetables and low meat consumption, the health messages that have been heard by South Asian immigrants and their children do not emphasize this. Instead, perhaps because most messages about ‘healthy eating’ do not portray Indian dishes, South Asian immigrants tend not to equate their foods with healthy eating. When health professionals do talk about healthy eating and Indian foods, the messages are about cutting back on fat and sugar – ingredients that are increasingly consumed after immigration (as well as in India in recent years), but were not common in the traditional diet.
Overall, our findings have several important implications for health educators working with South Asian immigrants and their families. Educators should consider ways to emphasize the positive aspects of Indian foods and food preparation methods that are considered both healthy by western standards and tradition-maintaining and acceptable within the South Asian community. This could include promoting the centrality of vegetable dishes in traditional meals, and highlighting lower fat ways of preparing these dishes. These health promotion messages should incorporate both traditional and nutritional science approaches, such as emphasizing ways to prepare and provide traditional meals that are satisfying, strength-giving and protective against chronic disease. At the same time, practitioners and policy-makers also need to provide information about ‘western foods’, so that when family food providers are serving foods that are unfamiliar to them, they understand that the degree to which these foods are ‘healthy’ can vary greatly, depending on what ingredients the foods contain and how they are prepared.
Finally, health promotion and nutrition practitioners must take care to acknowledge the diversity within the community, as not all members of the South Asian community define ‘healthy eating’ in the same way even when they are members of the same family. There are other contextual factors, in addition to the familial context, that contribute to differing interpretations of healthy eating, such as the ways in which the beliefs and food practices of members of the community reflect tradition as well as adaptation to the new environment.
Footnotes
Acknowledgements
We thank research assistants Barinderjeet Chane and Lucki Kang and gratefully acknowledge the Canadian Institutes for Health Research for research funding.