
Abstract
Introduction
Professional bodies continue to recognize that ‘the needs of stroke patients are not being adequately met in the UK [United Kingdom] at present’ 1 . Stroke survivors and their caregivers continue to report being inadequately informed about recovery-promoting activities and stroke risk reduction2–6 and dissatisfaction with psychological and emotional support5,6. In response, leaflets are continually produced by health services and individuals working with patients and charities (evidenced by the leaflets and posters found in the wards) on an assumption that information provision will enable people to pursue behavioural activities to promote recovery with reduced health services input. The Cochrane review ‘Information Provision for Stroke Patients and their Caregivers’ 7 highlighted the importance of providing information relating to stroke recovery but questioned its benefits.
Over the last decade, several randomized controlled trials (RCTs) have examined ‘information providing’ interventions for stroke survivors and their families with variable and inconclusive outcomes7–14. Incorporated within the interventions under examination are elements of general information, social support and recovery-promoting advice (behavioural activities), though these are not explicit. Overall, these studies have shown no significant differences in functional limitation outcomes between the intervention and control groups.
One possible reason for this result is that there appears to be little understanding of the mechanism by which these information-providing interventions were expected to influence functional outcomes. In an attempt to address this issue, Johnston et al 15 developed a stroke workbook intervention (SWB) for stroke survivors and their caregivers specifically designed to provide information in such a way as to increase perceptions of control, a variable previously shown to influence behaviour16,17. Using psychological theory, and based on the successful Heart Manual (an intervention for the recovery from myocardial infarction 18 ), the SWB incorporated a range of techniques designed to change behaviour by influencing control cognitions through tailored information, persuasive messages, social support, goal setting, action planning, self-monitoring, feedback, coping training and stress management 15 . Tested in an RCT (Stroke Workbook Outcomes Trial [SWOT]) the results demonstrated that the SWB was moderately effective in reducing functional limitations and maintaining confidence in recovery 15 . However, 42 per cent (n = 38) randomized to receive the SWB appeared not to attempt to perform any of the recommended behavioural activities. It is possible that the full effectiveness of this intervention was masked by this poor adherence. The aim of this study is to examine stroke survivors’ experiences and perceived usefulness of an effective self-help workbook-based intervention designed to improve recovery.
Research questions
Do stroke survivors find a stroke workbook intervention useful and, if so, which components do they perceive to be most useful?
Are some aspects of the SWB perceived to be more or less useful to some sub-groups?
Do general demographic, clinical and psychological variables predict perceived usefulness with the stroke workbook intervention?
Method
Design and procedure
Stroke survivors recruited from the intervention arm of SWOT 15 were the participants for this study. Baseline demographic, clinical, and psychological variables were completed two weeks post-discharge from hospital following an acute stroke, and prior to randomization to receive a SWB as part of the RCT. All participants were screened for cognitive and communication impairment prior to the interview to ensure that they were able to use/comprehend the workbook and to answer questions on the measures. The carers of those with gross communication difficulties were included in SWOT as a carer-only sub-group and were not analysed in this present study 15 . Following the intervention period participants rated their perceived usefulness of pre-determined components of the intervention, and their responses were used to derive an overall measure of perceived usefulness.
The stroke workbook intervention
The stroke workbook is an A4 loose-leaf folder containing 90 illustrated pages and includes text with an average reading level (Flesch Reading Ease score = 70.6). It provides information about stroke and recovery interspersed with behavioural activities using cognitive behavioural therapy techniques ‘designed to allow the patient to attain the coping skills to encourage self-management’ 15 . Task materials such as goal setting, self-monitoring diary sheets, and an audio relaxation cassette tape accompanies the workbook.
Administered by a trained implementer over a five-week period, the SWB was presented at the first home visit, where the participant was advised how to use it. They were encouraged to read and attempt the behavioural activities in the workbook over the first week. A second home visit was then undertaken approximately a week later to support the participant in their use of the SWB and to provide an opportunity for questions and discussions about their progress. The implementer encouraged the participant to continue to use the SWB, to write in the self-monitoring diary, and to listen to their relaxation tape. Additional written information about stroke risk factors and how to minimize them were available to the participants at this visit. The third and fourth contacts were by telephone at weekly intervals where continued support and encouragement to use the SWB was given. The final contact included a home visit where the participants evaluated the workbook. Participants were thanked for taking part and were offered the workbook and relaxation tape to keep.
Measures
Perceived usefulness
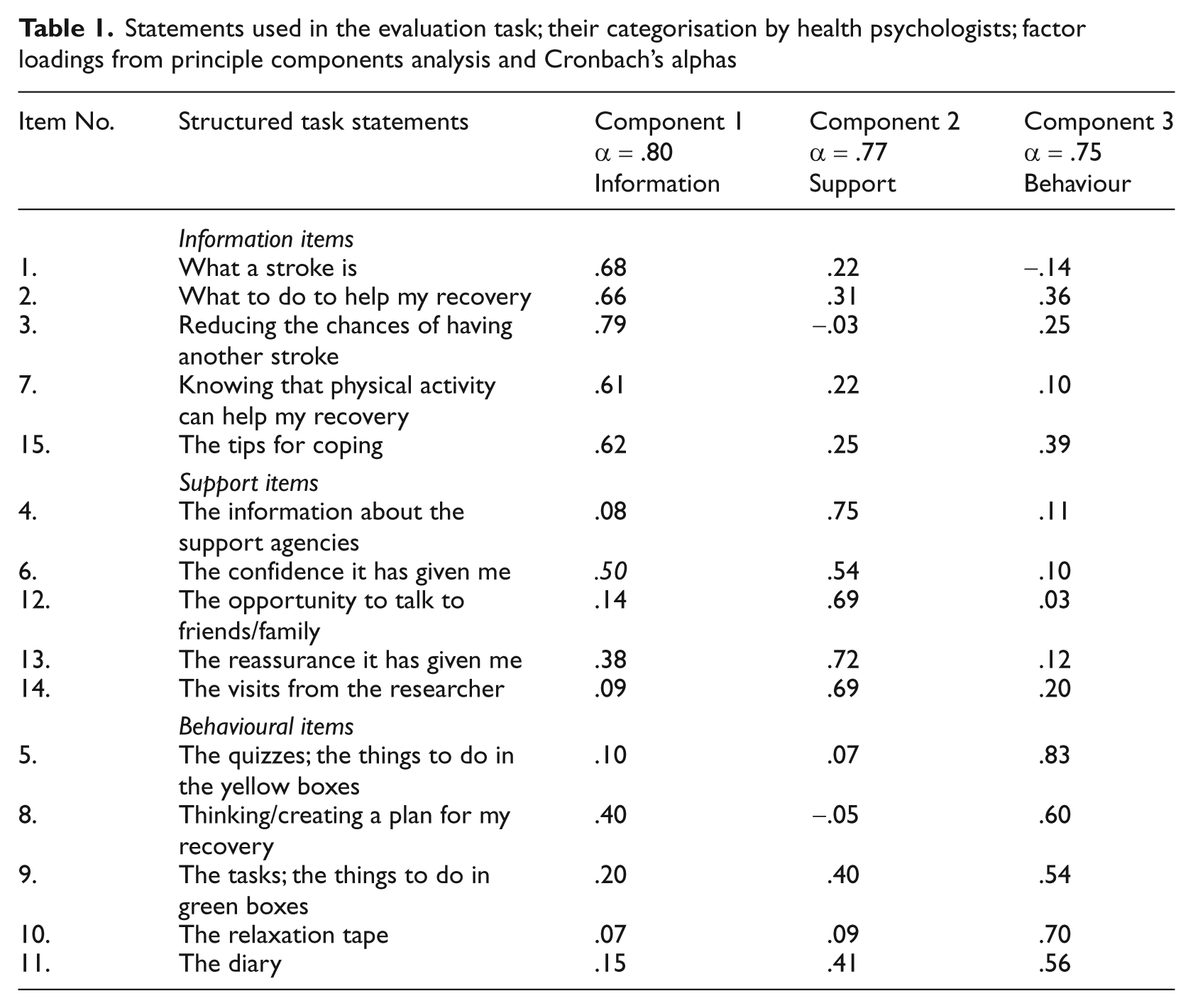
A structured task, specifically designed to evaluate different components of the SWB 19 , was chosen as an alternative to the battery of questions that had been administered in the baseline and outcome interviews and was in keeping with the design of the SWB, i.e. a behavioural activity. Fifteen statements derived and allocated to three a priori categories by a group of six health psychologists were included (Table 1). There was 100 per cent inter-rater agreement that 15 statements fell into three distinct groupings: information (five items), e.g. ‘The information about what a stroke is’; behavioural activities (five items) e.g. ‘Thinking/creating a plan for my recovery’; and the social support (five items), e.g. ‘The reassurance it has given me’ (Table 1).
Statements used in the evaluation task; their categorisation by health psychologists; factor loadings from principle components analysis and Cronbach’s alphas
The statements were written on separate pieces of card and placed in front of the participant who considered each statement separately and decided if this component of the SWB was useful or not useful. All the cards perceived as not useful were scored as 0 and removed from the participants view. With the remaining ‘useful’ cards in front of the participant, they were then asked to re-read each statement and consider ‘how useful’ they perceived each component of the SWB and to place the card into one of three piles: slightly useful (score 1); moderately useful (score 2); or very useful (score 3). The cards rated as slightly and moderately useful again were removed. Finally, the participants put statements rated as ‘very useful’ in rank order of usefulness to establish which item they perceived as being personally most useful.
Validation of the measure of perceived usefulness
The responses to the usefulness items were entered into an exploratory principle component analysis with varimax rotation to establish loadings for three intervention components (information, social support and behavioural activities), to ensure construct validity. The analysis demonstrated a clear and logical pattern as only one item (6) loaded onto two factors (Table 1). The Kaiser-Olkin-Meyer measure of sampling adequacy was .81, indicating satisfactory measure of factorability20 and the internal reliability for each component achieved Cronbach’s alphas of above .70 (Table 1). Inter-rater agreement was achieved for the distribution of the final 15 statements across three components that were labelled ‘information’ (five items), ‘social support’ (five items) and ‘behavioural activities’ (five items). Scores were obtained for each component ranging from 0–15, with the higher score indicating greater perceived usefulness. An overall score was derived from totalling the scores for each component to give an indication of perceived usefulness of the stroke workbook intervention ranging from 0–45, the higher score the greater the perceived usefulness.
Predictor variables
Demographic variables
These included gender, age and the presence of a caregiver.
Clinical assessments
hese included affected side of the body, number of previous strokes, and length of stay in hospital. Initial stroke severity was indicated by the Modified Rankin Scale (MRS) 21 recorded on patients’ admission to hospital. It is a six-item measure of functional independence, where the score ranges from no symptoms at all (0) to dead (6) i.e. the lower the score the more functional independence.
The Barthel Index22,23 was also used; it is a 10-item scale measuring the ability to perform activities of daily living independently with a score range from 0–20, with lower scores indicating reduced ability. Recorded at the baseline interview, this well-validated scale is commonly used with stroke patients 23 .
Psychological variables
The Hospital Anxiety and Depression Scale (HADS)23,24 assesses mood ‘independently of somatic symptoms’. Fourteen items assess anxiety (7) and depression (7), with each item being scored from 0 to 3 giving total scores ranging between 0–21 for each. Higher scores in both sub-scales indicate greater depression and/or anxiety. The HADS is a widely-used and validated measure 25 .
The Recovery Locus of Control Scale (RLOC)16,17,23 was developed to measure perceived control over recovery. Five items assess internal beliefs and four assess external beliefs. Participants respond to statements on a five-point Likert-type scale from ‘strongly agree’ (1) to ‘strongly disagree’ (5). Each item is scored from 1–5 (in the direction of internality) and totalled to give a score between 9 and 45. The total score reflects the strength of the respondent’s perception of control, i.e. a high score indicates a high perceived control. This measure was predictive of disability recovery in earlier studies 23 .
Confidence in Recovery15,18,26; this is a single item asking participants to rate their level of confidence on a scale of 1 (not at all confident) to 10 (totally confident) about making a perfect recovery. This item was predictive of distress in earlier studies 26 .
Desire for the Workbook15,27; this is a single item measure, specifically designed for the SWOT RCT, and asked participants to rate how much they would like to receive the SWB prior to randomization. Participants rated their desire for the workbook on a five-point scale from ‘definitely do not want it’ (1) to ‘definitely do want it’ (5).
Statistical analysis
The data were analysed using SPSS computer program 28 and screened for missing data and normality of distributions 29 . All data appeared to be normally distributed apart from the Barthel Index which was transformed by cubing the scores. All the measures were assessed for internal reliability using Cronbach’s alpha, and an acceptable range of .60–.70 30 was achieved apart from RLOC which just fell below the lower limit.
Baseline differences between groups were assessed using t-tests or chi square and repeated-measures ANOVA to analyse the differences between the three intervention components; information, support and behavioural activities. ANOVA is a stringent analysis and therefore able to account for the validity of the structured exercise which could not be assumed. Artificial sub-groups were created using a median split on each range of scores (continuous data) apart from the HADS. Two similar group sizing pertaining to the lower and higher scores of each scale were created for: age – young/old; impairment – high/low Barthel Index; hospital stay – long/short period; RLOC – high/low perceived control; confidence – high/low confidence, and desire for the intervention – high/low desire. The mood sub-group used the HADS validated cut-off scores of 10 and upwards suggesting probable anxiety or depression 24 . Dichotomous data provided sub-groups of gender, with and without caregiver, retired or not, left or right affected side, and first or previous stroke. T-test and chi were used to examine sub-group differences. Levene’s test of equality is reported when interpreting the t-test outputs and where variance could not be assumed the corresponding t-value was used; this has been noted by observing the lower degrees of freedom 20 . Bonferroni’s correction was used to account for multiple testing and Fisher’s exact results are reported for the chi square where the cells had less than five expected observations.
To examine relationships between the predictor variables and perceived usefulness, Pearson’s correlations were calculated for continuous data and point bi-serial analysis for the dichotomous. Multiple regressions were performed on variables with correlations with probabilities less than or equal to .22 (Hosmer and Lemeshow 1989 cited in Hair et al 1998 30 ) to see which combination of variables were the best predictors of perceived usefulness of the intervention. Multicollinearity was examined for each regression model using VIP (variance inflation factor) and was within acceptable levels 29 .
Results
A sequential cohort of 303 stroke patients who were cognitively intact and fluent in English from a geographically-defined area, admitted to Ninewells Hospital, Dundee, between September 1998 and May 2001 were invited to participate in SWOT. Two hundred and three participants gave their consent and 103 participants were randomly allocated to the intervention group. There were no significant differences at the p < . 05 level between the intervention and the control group in relation to the baseline demographic, clinical and psychological variables 15 .
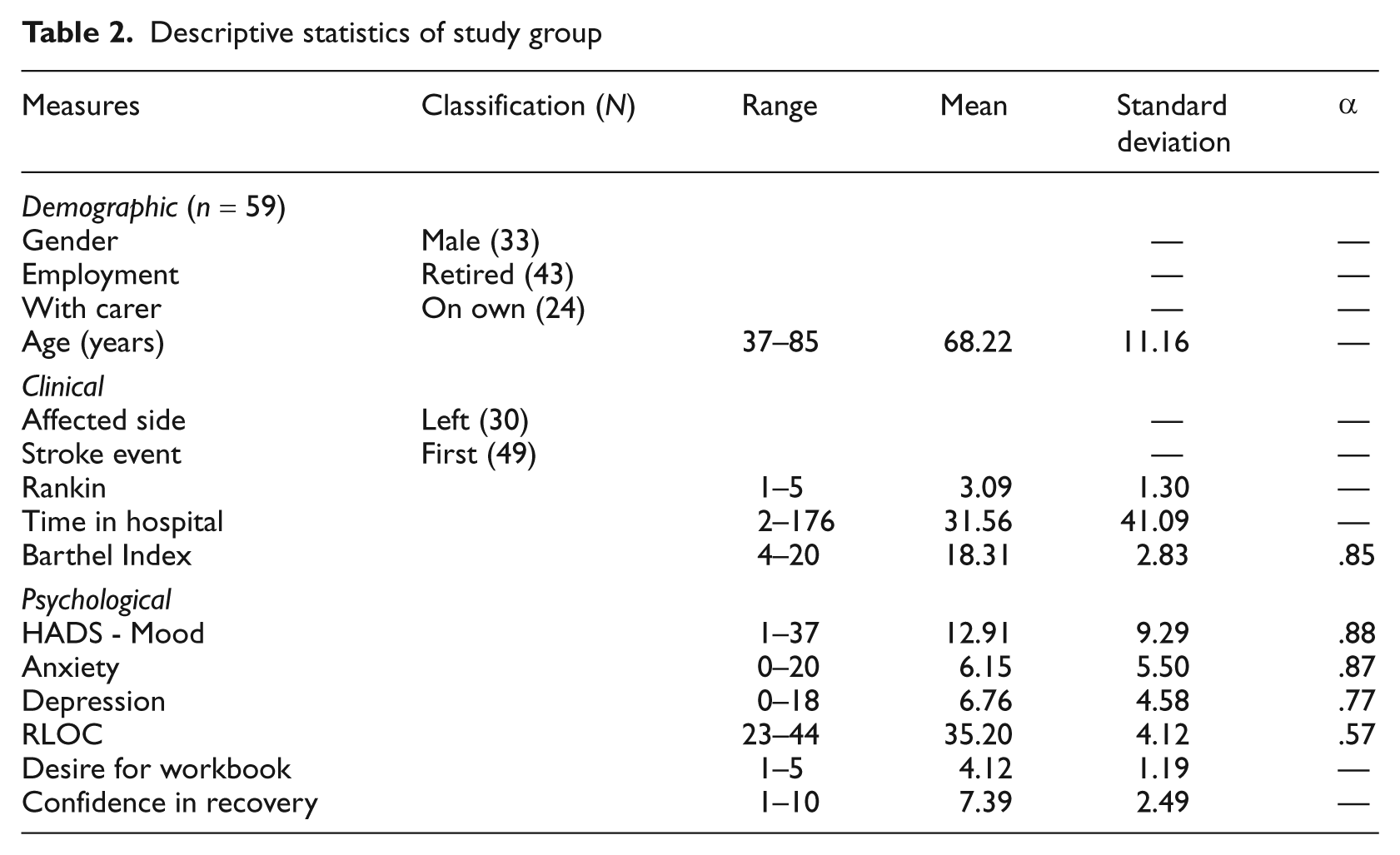
Of the 103 participants offered the intervention, the data from 10 could not be included as they became ill or died by follow-up and two never received the workbook due to an administrative problem. Of the 91 participants receiving the workbook, 13 participants chose to withdraw from the intervention before the end of the five-week intervention period (13/91 = 14 per cent) with three declining the workbook prior to seeing it and 10 participants starting to do some of the activities in the workbook but declining to proceed with it by the second week. Seventy-eight participants went on to complete the five-week intervention with 59 participants fully completing the evaluation exercise. The descriptive data for these 59 participants (Table 2) did not significantly differ from the 19 participants who did not complete the evaluation exercise.
Descriptive statistics of study group
Research question 1: do stroke survivors find a stroke workbook intervention useful?
Participant’s scores ranged from 0, indicating not useful, to 45, indicating very useful, with only one person perceiving the SWB not to be useful (Figure 1).
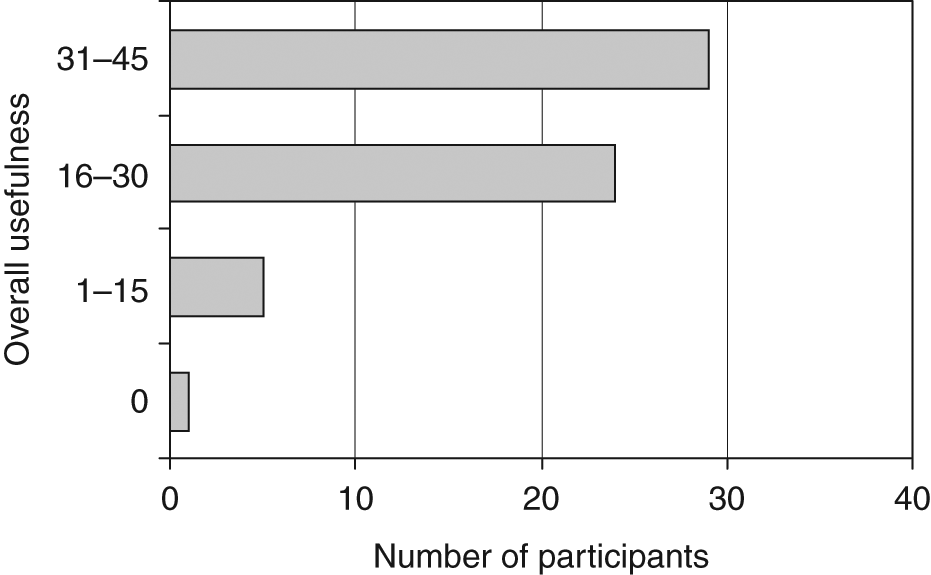
Distribution of perceived usefulness scores of the stroke workbook intervention
Research question 1a: which components of the stroke workbook intervention did stroke survivors’ perceive to be most useful?
The information and support components were perceived significantly more useful than the behavioural activities (F (2, 116) = 60.79, p = .001), (Figure 2). Post-hoc tests show that differences do lie between information and social support (p = .001), information and behavioural activities (p = .001) and social support and behavioural activities (p = .001).
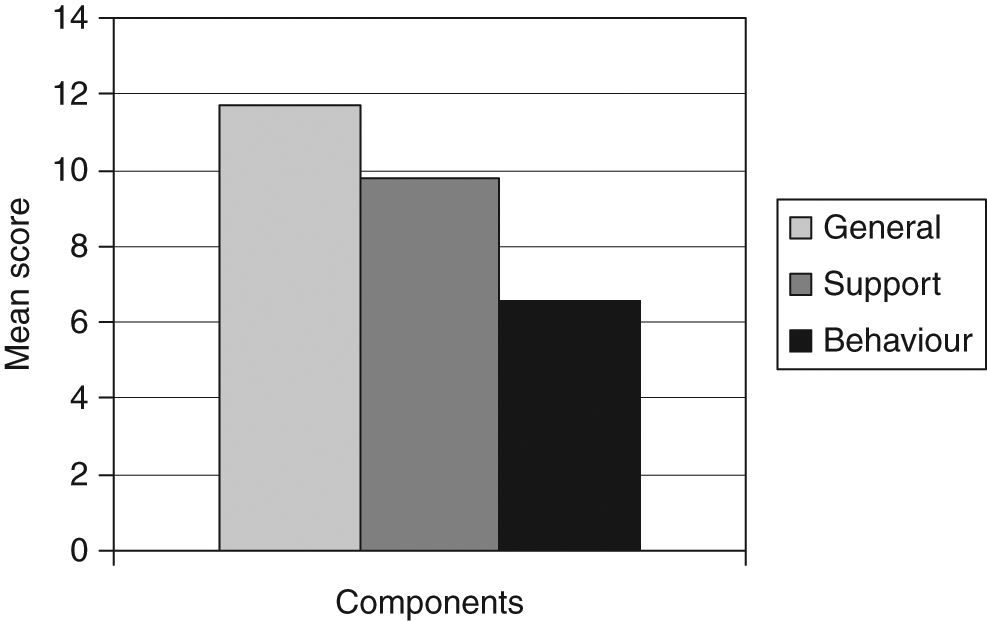
Mean scores of perceived usefulness for each component of the stroke workbook intervention
Participants were asked to choose which they considered to be the most important aspect of the intervention. Thirty-three per cent rated item 1, ‘information on what a stroke is’ as being the most important (Figure 3).
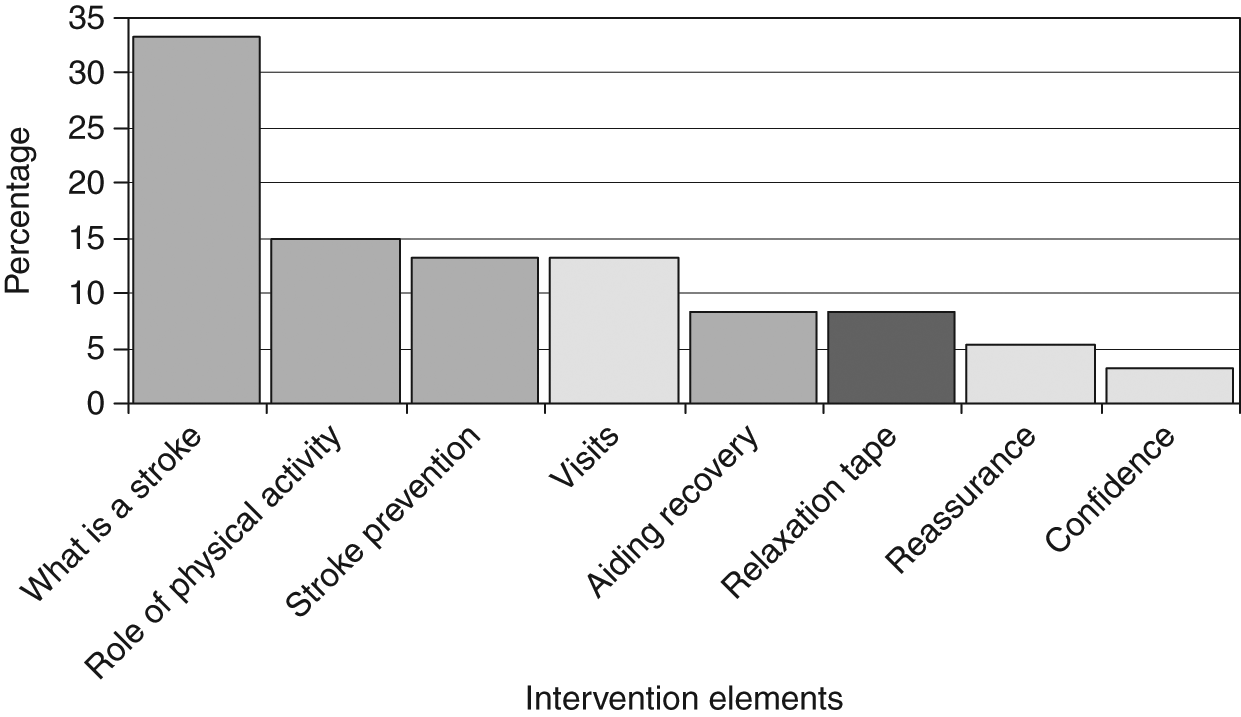
Percentage of responses to indicate the most useful aspect of the SWB
Psychologically, no significant differences were found for mood and confidence in recovery sub-groups. Participants who had above median levels of perceived control rated the support component higher than those with below median RLOC scores (t(57) = −2.06, p = .04). Participants who had a high (above median) desire for the intervention found all the components of the workbook significantly more useful than those with low desire (information t (24.41) = −3.19, p = .004, social support t (57) = −2.68, p = 0.004 and behavioural advice t (57) = −4.18, p = .001). However, when Bonferroni’s correction was applied due to the number of t-tests (n = 24), those with high desire found the behavioural component significantly more useful than those who were low in desire (p < .002).
Research question 3: do general demographic, clinical and psychological variables predict perceived usefulness with the stroke workbook intervention?
Correlations with the intervention components were examined (Table 3) and multiple regression analysis produced three significant models, suggesting that desire for the intervention alone explains 22 per cent (adjusted R square = .22) of variance in information and 10 per cent (R square .10) in support. Both desire for the intervention and depression explains 33 per cent (adjusted R square .33) in behavioural activities (Table 4).
Correlations between intervention components and demographic clinical and psychological variables with probabilities of ≤.22
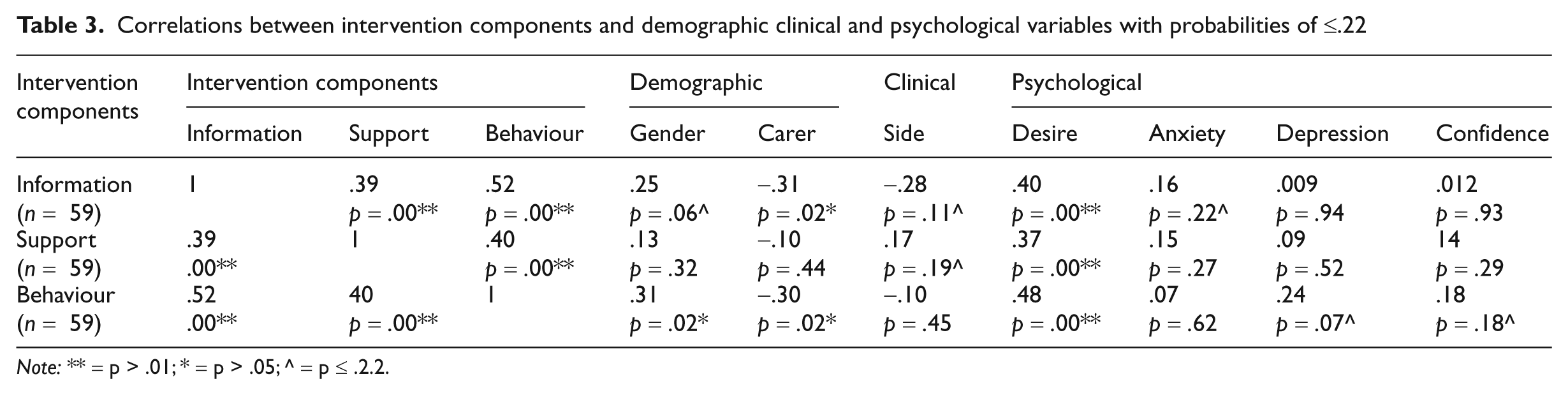
Note: ** = p > .01; * = p > .05; ^ = p ≤ .2.2.
Multiple regression analysis for information, support and behavioural activities: variables, betas and confidence intervals
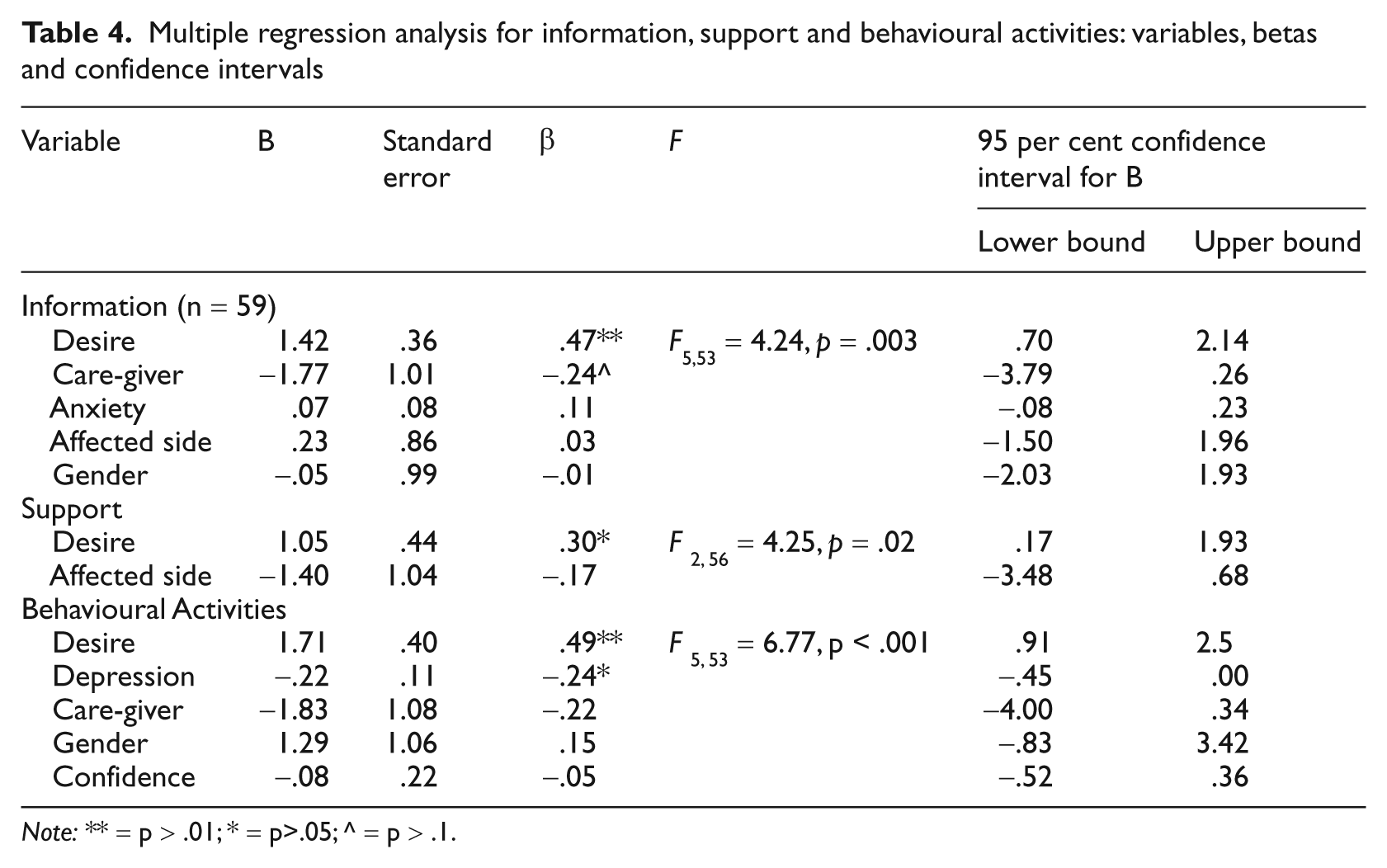
Note: ** = p > .01; * = p>.05; ^ = p > .1.
Post-hoc power analysis
Post-hoc analysis was performed and showed that this study (n = 59) had power = 0.94 to detect a large effect size (.35), power = 0.56 to detect a medium effect size (.15), power = 0.10 to detect a small effect size (.02) (multiple regression analysis, five predictors with a critical F = 2.38) 31 .
Discussion
Although stroke survivors are reported to be asking for recovery-promoting activities2–5 this study demonstrates that such activities are not perceived as useful as information and support. Stroke survivors overall valued the SWB with only one person out of 59 evaluating it as ‘not at all useful’. The most useful aspect was the information component, especially the section entitled ‘What is a stroke?’. Sub-group analysis demonstrated perceived usefulness for different components of the SWB, but these were not statistically significant apart from desire for the intervention and usefulness of behavioural activities; patients high in desire rated the behavioural components as significantly more useful than those with low desire. Desire was also predictive of perceived usefulness of all components of the intervention and depression additionally predictive of perceived usefulness of the behavioural component.
Information and social support may be perceived as more useful in the early stages of stroke recovery, whereas the behavioural activities may be more important in the later stages. The SWB was implemented two weeks post-discharge from hospital when the stroke survivor may have been adjusting to being back at home rather than their recovery. Reading information requires little exertion whereas behavioural activities may have been too difficult to do, or not understood, and therefore possibly not useful.
Information about the nature of stroke may have satisfied the common search for explanations and attributions32,33 as patients may not have fully understood their condition at the point of discharge. Furthermore, there may be a lack of understanding of the benefits of being actively involved with recovery which may lead to finding the behavioural activities least useful.
Whilst the sub-group analysis following Bonferroni’s correction revealed no significant differences between the components, apart from desire for the intervention, gender and being without a caregiver, were highlighted for future investigation. Significantly, more women were without a caregiver than men, suggesting women manage their recovery without a supportive network and possibly place more value on interventions, as seen in studies observing rehabilitation from myocardial infarctions35,36. Such findings lend support to the importance of gender in clinical research 37 .
Perhaps unsurprisingly, behavioural activities were valued more if the stroke survivor initially had a greater desire for the intervention and were less depressed. Mood has been previously associated with disability outcomes in stroke 38 .
This study incurred a number of limitations. The evaluation task was intervention specific and therefore only partially validated. Satisfaction questionnaires are often used to evaluate health-related interventions. However, in SWOT, a global measure asking about satisfaction with care rather than the SWB intervention itself was used 15 . Satisfaction with an intervention potentially provides information for effective intervention implementation and subsequent uptake39,40, and whilst perceived usefulness may not reflect satisfaction, a few studies have demonstrated a significantly-positive relationship between perceived usefulness and satisfaction in other areas of health care research41,42. Furthermore, the study was restricted by the measures employed by the original SWOT RCT and the creation of artificial sub-groups, and therefore is only indicative of possible avenues for future exploration.
Conclusion
Stroke survivors differentiate information, social support and behavioural advice and appear to perceive advice to become actively-involved in recovery as least useful. Exploring with the patient what information, social support and advice they perceive to be useful may be indicative of their responses to their rehabilitation and recovery. Furthermore by ensuring that future behaviour change interventions are desirable may increase their perceived usefulness and promote better outcomes.
Footnotes
Acknowledgements
Thanks to the patients and carers from Tayside who took part in this study and the Chief Scientist Office, Scotland for funding.