
Abstract
Gestational diabetes (GDM) is a condition occurring during pregnancy with significant short and long term negative sequelae for both mother and child1,2. Epidemiological analyses have identified ethnicity as a risk factor along with age and body mass index3,4, with Hispanic women having an adjusted relative risk factor of 2.4 (95 per cent, CI 1.48, 4.04) as compared to white women 4 . Hispanic women constitute a patient group standing to benefit from prenatal services aimed at reducing their risk for the development of impaired glucose tolerance during pregnancy5,6.
Dietary changes, exercise and insulin supplementation as appropriate are recommended as methods for helping pregnant women achieve normal levels of glucose tolerance7,8. The few studies completed to date with Hispanic women on pregnancy, diet and exercise have found misconceptions of the value of regular exercise in reducing a woman’s risk of abnormal metabolic status 9 , and identified the importance of social support for maintaining healthier behaviours during pregnancy10–12. No information could be found in the published literature as to how Hispanic women conceptualize their diet as a risk factor for GDM or what alterations in dietary habits they would be willing to initiate13–15.
The purpose of this study was to explore pregnant, low income Hispanic women’s beliefs and understanding about gestational GDM and diet through a two-phased mixed method of inquiry 16 . Women were asked about their knowledge and attitudes related to GDM and their health behaviours during pregnancy. Of particular interest was assessment of the type of carbohydrates that the women reported eating and their attitudes towards dietary change since quantity and type of carbohydrates consumed during pregnancy has been correlated with infant birth weight17,18. Feedback from this group was used to develop educational messages targeting specific eating behaviours related to a healthy prenatal diet and evaluated by a second group of women receiving prenatal care at the same clinic.
Methods
Sample
All participants were Latina women in their second or third trimester of pregnancy, reporting a healthy pregnancy and whose primary language was Spanish. Eighty-five per cent had recently immigrated from Mexico. The 94 participants, ranging in age from 18 to 31 years, were recruited in two periods between May 2006 and May 2008 from a Midwest Federally Funded Community Health Center serving the uninsured and underinsured for a community of approximately 150,000 people. Prenatal care is provided to an average of 150 pregnant women per year, 67 per cent of whom are Hispanic and Spanish speaking. The study group recruited represents 70 per cent of the eligible pregnant Hispanic women within the recruitment periods.
Procedures
Two separate recruitment periods were used because information was first sought on women’s views of pregnancy, GDM and diet. For both groups (n = 48 and n = 46), in-person interviews were conducted in Spanish by the bilingual first author. Consent forms were read by literate patients or read to those women with reading difficulties and in all cases were signed with either a name or an ‘x’ signifying consent for completion of the questionnaires and a one-on-one taped interview. The study was approved by the University of Illinois Institutional Review Board and the clinic administrator.
Women recruited for phase two completed a 10-item questionnaire about their motivation to change behaviours and their beliefs about whether or not they could execute small dietary changes. The participants were then shown a flyer illustrating the amount of carbohydrates in tortillas and fruit juice in comparison to a candy bar and told of the importance of drinking one glass of water before each meal to decrease the amount of juice being consumed and minimize the amount of tortillas eaten. Feedback about the educational material was solicited in a 5 to 20 minute interview. Of the 46 participants in the second phase of the study, 12 (26 per cent) were available at the clinic for a two to four week follow-up. These women were asked to react to the suggestions they had been given about dietary change and whether they had tried to implement any of these changes into their daily routine.
Measures
Knowledge of diabetes was assessed by the completion of a 19-item survey using the Diabetes Knowledge Questionnaire (DKQ) as a template 19 . Questions on risks, outcomes, and symptoms of GDM were based on information about the disease found in Williams obstetrics, maternal–foetal medicine 20 . Potentially unfamiliar terms were explained as follows: gestational diabetes = diabetes diagnosed during pregnancy; carbohydrates = tortillas, bread, fruits, and sugar; alternative medicine = the use of herbs and teas or any kind of treatment that you do not find at the health center; glucose tolerance = ability to eat sugars without the sugar in your blood going too high; and macrosomia = a very large baby.
An 27-item attitudinal questionnaire assessed the following seven domains: beliefs about the outcomes of pregnancy (seven items), attitudes towards diet or exercise (five items), the husband’s or family’s role in planning meals (six items), fatalismo (three items), confianza, trust in provider (three items), attitudes towards alternative medicine (four items), and intentions about changing diet (four items). All questions were reviewed by native Spanish speakers in the community health clinic and two professional Hispanic educators. Items were coded using a 7-point Likert scale (1 = I strongly disagree; 7 = I strongly agree).
Current diet was assessed with a 24-hour recall prompted by pictures and models with foods familiar to the participants and available from the USDA National Agricultural Library Food and Nutrition Information Center. Modelled foods included meats, eggs, various vegetables and fruits, rice and beverages. Portion sizes for foods other than food models such as beans, rice, and tortillas that were not represented by models were estimated using handfuls of rice.
Qualitative analysis
Themes from the phase 1 transcribed and translated interviews were identified through a reading of each transcript and then followed by a review with a faculty expert. Codes were constructed first from the questions used to guide the beginning of the interview and then augmented with those themes emerging from the reading of the transcripts. Concepts reiterated by at least 10 participants were considered thematic21,22. The level of agreement between the two coders was 95 per cent. A total of eight theoretical codes/themes were identified from the first group. Themes from the second group of interviews were analyzed in the same manner and resulted in four themes.
Results
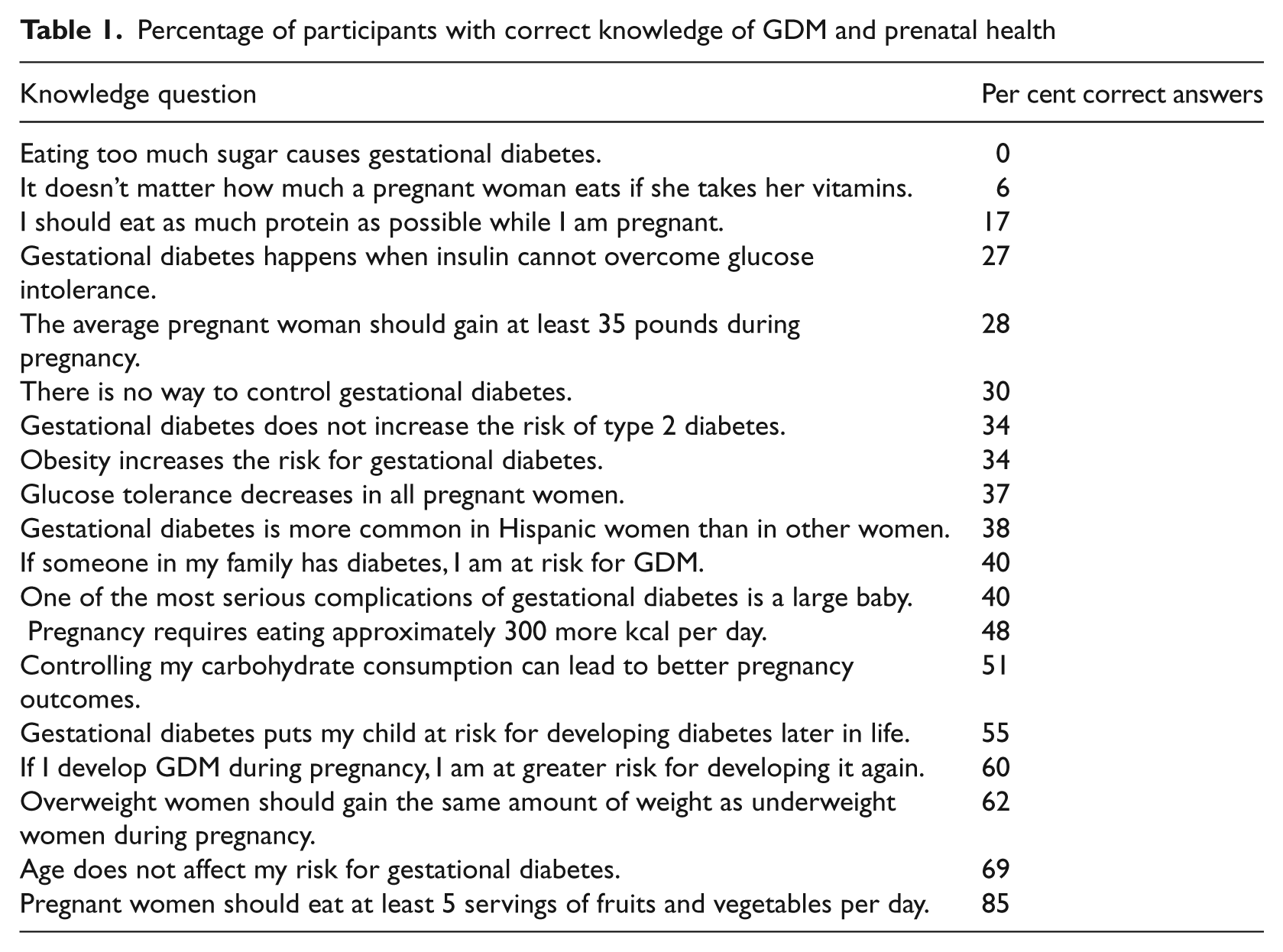
Table 1 summarizes the knowledge questions asked of the first group of 48 women. Fifty per cent or more of the respondents were correct in their understanding of age as a risk factor for GDM, GDM as a risk factor for both maternal and child health, and recommendations for weight gain, fruit and vegetable daily portions and carbohydrate consumption. With regards to nine other questions related to GDM, the majority of women did not understand the relationship between sugar and GDM, familial risk factors, the possibility of controlling GDM, or the relationship between GDM and type 2 diabetes. All of the women thought that sugar was to be avoided for prevention of diabetes, and 94 per cent believed that prenatal vitamins were sufficient in and of themselves as an adequate prenatal diet regardless of weight gain.
Percentage of participants with correct knowledge of GDM and prenatal health
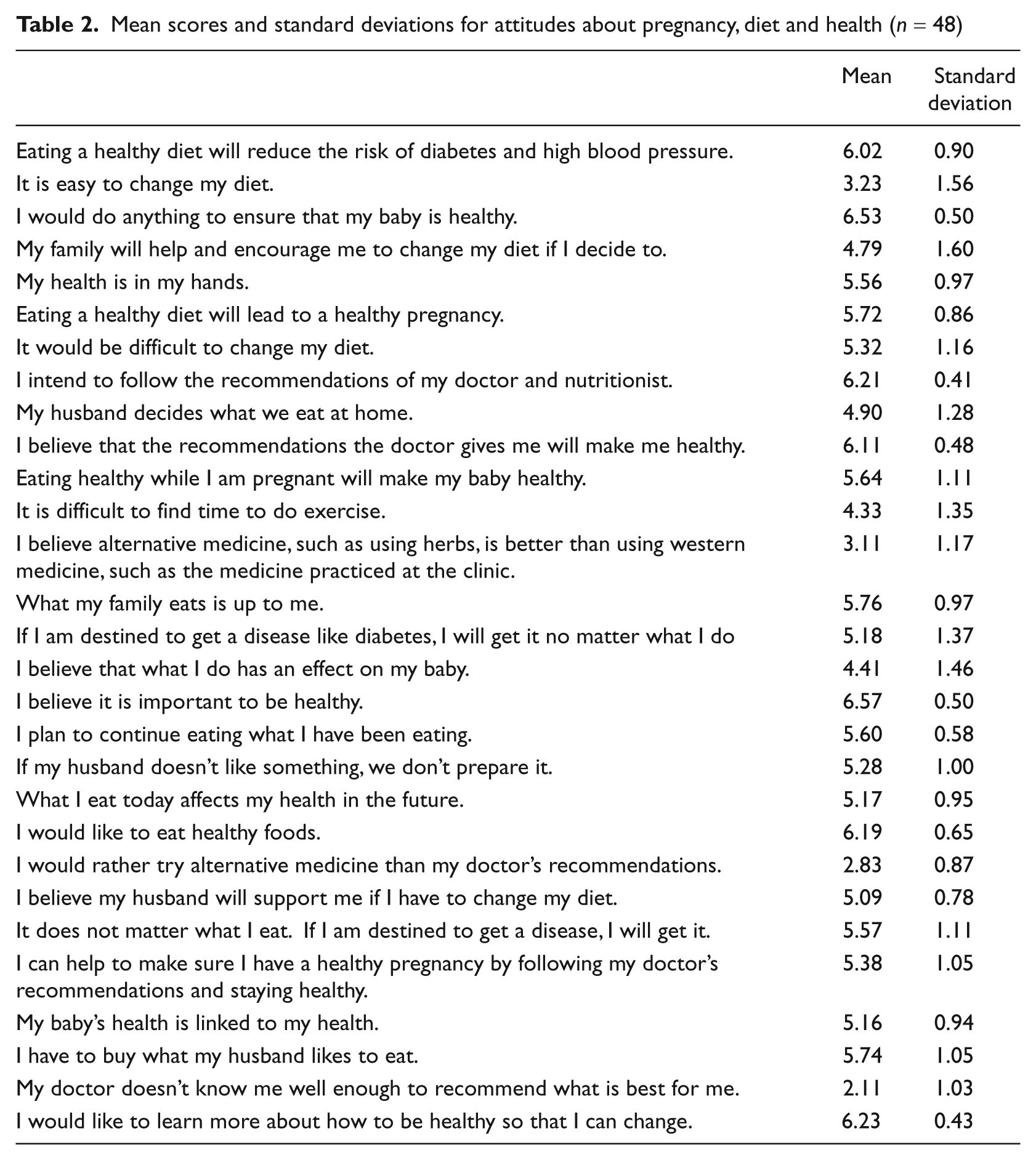
The majority of women wanted a healthy baby and would do anything to ensure their infant’s health (Table 2). They reported themselves to be compliant with physician orders, aimed for a healthy prenatal diet and reported wanting to learn more about how to be healthier. In contrast to these positive attitudes, these same women also believed that destiny dictated whether they would get diabetes and that fate would override other influences like dietary change and exercise in determining who would get a disease. There was also concurrence from two questions about the ease of changing diet, with disagreement that such change could be easily accomplished and agreement that change would be difficult.
Mean scores and standard deviations for attitudes about pregnancy, diet and health (n = 48)
The interviews with this group of women provide a complimentary view of their priorities and challenges with regard to having a healthy pregnancy and prenatal diet. The eight themes are presented here in descending order of the number of women referencing the issue and an illustrative quote linked to each theme is presented below.
All 48 women identified pregnancy as a motivator to be healthy and to make any necessary changes for the health of their baby.
I know I can do whatever my doctor tells me because I have to do it for my baby. Even if it is something hard to do, I know I could do it. … But I just remember that it is for the baby, and I can do it.
Every woman also brought up the role of fate is a determiner of health and disease.
We all have a predestination, right? So if it is our predestination to have a disease such as diabetes, then we will have it … because that is what is supposed to happen.
The role of family was central to the possibility that eating behaviours might be changed at home for 40 women, and a more specific dimension of family life had to do with the husband’s influence on the family diet for 40 of the women.
If I had to start eating new foods, I would need my family’s support because if I change, probably they will have to change. And they can help me.
The theme of routine was identified by 36 women, with routine centred around family diet and grocery shopping habits.
… we buy what we need. It is the same all the time. We do not have to decide what to buy. We know what we need.
The importance of health was mentioned by 32 participants as important but also as something the women would like to learn more about.
… it is important to be healthy. Without health you have nothing.
Fifty-eight per cent of this group talked about their intentions to avoid sweets as a way of preventing diabetes. When mentioning the disease, most women referenced fear and/or apprehension.
It is important not to eat sweet things – candies, sweet bread, things with sugar – so that I don’t get diabetes. … I don’t want diabetes. Sometimes I’m scared I will get diabetes, and that is what helps me not eat sugar.
Finally, 21 of the women mentioned the cost and availability of food, especially fruits and vegetables. Women described their frustration with the high cost of certain items but reported adapting to the prices in order to keep with their routine of eating fresh produce.
Fruits and vegetables are expensive. I don’t know why because they are not so good. But we buy some when there are things we like.
From the 24 hour food recall reported in Table 3, women reported eating between 6 and 17 tortillas along with potatoes, sweet bread, fruits, carrots, and juices. Forty-six (95.8 per cent) of the women surveyed reported drinking 12–36 ounces of juice per day and 6 per cent reported having 3–4 servings of diary projects. Four women in this study reported drinking the recommended 64 ounces of water.
Analysis of self-reported prenatal diet according to recommended daily allowances (RDA) (n = 48)
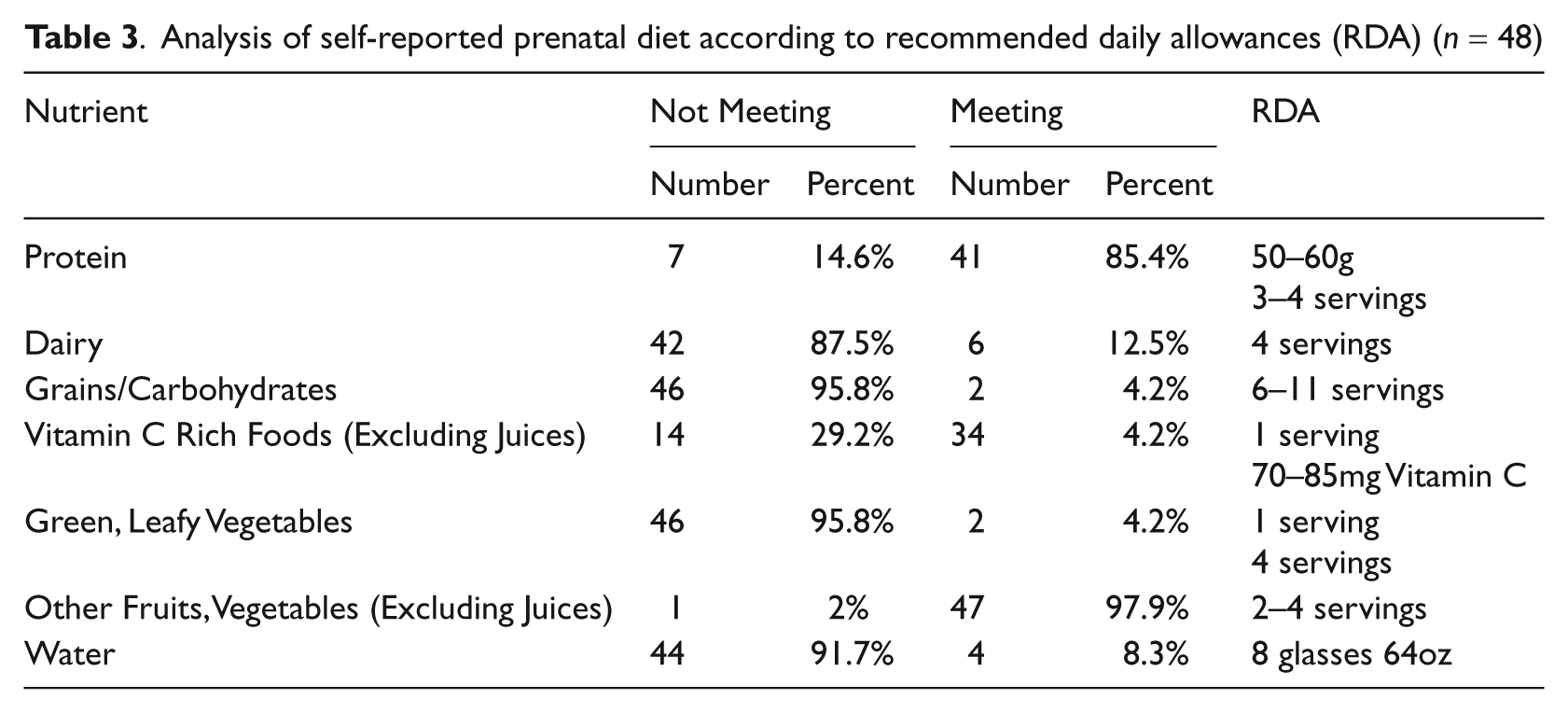
Women reported preparing food in vegetable oil, especially corn oil. No one measured the amount of oil used, but several participants could report using enough to cover the bottom of the pan and using oil at least twice per day to prepare food. In addition to vegetable oil, fatty meats such as chorizo (sausage) and red meat were a part of the average diet. Participants reported eating approximately two portions of meat in a meal. The majority of women reported eating at least two servings of fruits, but few women reported eating green, leafy vegetables. All 48 women reported taking their prenatal vitamin daily.
With the second group, the majority of the 46 women were willing to try different behaviours for the sake of their baby but were hesitant to change their diet. Echoing the values of the first group, all of the women agreed they would do anything for a healthy pregnancy. Most women (91 per cent) agreed that they had followed the recommendations of their doctor. Seventy-four per cent agreed that they wanted to eat healthily, but 82 per cent reported they did not want to change their behaviour. Thirty-nine (85 per cent) agreed that they were interested in a class to help them to be more healthy. Only 13 (28 per cent) believed that changing their diet would make them healthier. While the majority of the women (69.6 per cent) reported they believed they could begin to drink more water, only 31.9 per cent reported being ready to eat fewer tortillas.
After reviewing the educational flyer, the women were asked to share their thoughts about the educational messages on dietary change. As a group, they talked about four major themes listed in descending order of frequency of occurrence and with illustrative examples. The importance of family in thinking about potential change was the predominant theme, with 39 women discussing family life.
Yes, I believe that including the while family would be good … That way we do it together. It’s not like I’m taking a class by myself or changing what I eat just for me. We can do it as a family.
Thirty-four women talked about their attitudes towards changing eating behaviour, with most of the comments directed toward perceived difficulties.
You asked about eating fewer tortillas … I think that might be hard because we are used to eating tortillas with every meal … Other things … maybe. Of course, I would be willing to do things differently and trying new things if it would help my baby … even if it is hard, I think I could do it. I can drink a glass of water before dinner, sure.
The potential value of educational information was brought up by 31 women with statements about what might be learned about food preparation and the relationship between diabetes and food.
I know someone who had a class about cooking healthier, and they cooked during the class … I think they showed how to use less grease, things like that, and I think that is good because you are doing and learning. I think I would like that.
Lastly, logistical issues were discussed by 48 per cent of the group with an emphasis on the day-to-day challenges of arranging work schedule, transportation and child care.
I have two children, and so I think it would be good to have someone to watch the children … So I don’t have to find someone to help me … or pay someone … that would be helpful.
At the 8–12 week follow-up, 11 of the 12 women available said that they were drinking a glass of water before at least one meal and believed that they were decreasing the amount of juice they were consuming. None of the women reported incorporating drinking water before meals into every meal, nor did they report decreasing the number of tortillas they ate.
Discussion
Interest in having a healthy baby for the women participating in the interviews was keen and they were broadly willing to consider changing their lifestyle to achieve a better birth outcome. Family involvement, especially the husband’s involvement, was central to almost all the participants’ views about food purchase, preparation and consumption. Draft educational materials focusing on carbohydrates and water resulted in some women reporting efforts to increase water intake but no-one reported being able to decrease carbohydrate consumption.
In terms of limitations, the convenience sample of primarily Mexican women recruited from one Midwest Community Health Center may not be representative of the broader Hispanic population, either within the immediate community or more broadly. However, approximately two-thirds of the eligible women approached within the recruitment periods agreed to participate and the clinic is the only medical site locally accepting indigent pregnant women as patients. Educational level and potential problems with comprehension of certain terms poises another limitation, although a concerted effort was made to accurately communicate basic concepts pertinent to GDM.
The self reports of normal pregnancies could not be confirmed because information from the women’s medical charts was not available. It is possible that some women did not report their status correctly, either because they did not want to admit problems or because they did not understand the results of their glucose tolerance test. However, pregnant Hispanic women’s self report of medical conditions and information entered into their medical record has been found to be more reliable than self reports of behaviour 23 . Lastly, only 26 per cent of the women were available for follow-up on reaction to the educational messages. It is unknown how representative their responses are of the broader population. Because of this process of self selection, the findings reported here cannot be extrapolated to the larger population of Hispanic women.
This project illustrates the value of a mixed method approach to delineating patients’ perspectives on a complex health problem such as GDM. The responses show how difficult it can be for a woman to execute dietary changes within the context of her family even when she is pregnant and desires a healthy baby. Endorsement of the importance of healthy baby in the questionnaire was qualified by the statements made during the interview of having to satisfy a husband’s food preferences and fatalism about health.
On the other hand, the in-depth interviews with the second group also revealed a potential for small dietary changes gained with presentation of culturally relevant, straightforward messages about commonly eaten foods. The follow-up discussions with the 12 participants indicated that they were able to incorporate the substitution of water for a portion of the juice they were drinking after only a few minutes of discussion about the amount of sugar in commercial juices as related to the prevention of diabetes. Although this again was a subgroup of those women initially presented with the educational messages, their responses suggest that straightforward, brief messages based on day-to-day dietary habits may have some impact in the clinical setting in achieving positive behavioural change 24 . Looking forward, the preliminary results from the current study could be used to guide more rigorous tests of the impact of such messages for women responsible for day-to-day management of the household. For such evaluations, it would be essential to recruit and randomly assign a sufficiently large sample of women into an experimental and control group design in order to have credible evidence on the impact of the intervention on a family’s food preparation and consumption. Information from such clinical trials on the magnitude of dietary behavioural change potentially achievable would enable clinicians to better assist women in having a healthy pregnancy.