
Abstract
Introduction
The relationship between health and education is well understood by clinicians and health educators. A large body of evidence consistently indicates that patients who gain knowledge and skills improve their ability to manage self-care, enhance decision-making and improve their quality of life1,2. Patient education is a challenge, however, when staff are pressed for time and there are resource constraints. Accordingly, patients and community members are accessing the Internet for standard health information in ever-growing numbers3,4.
While better access to health information is helpful, the quality of the information retrieved varies considerably. All too often an Internet search leaves the patient feeling overwhelmed 5 and yields unreliable, commercial information 6 . Further, information can be characterized as, ‘one size fits all’; all patients receive the same material regardless of illness trajectory, cultural background and treatment plan.
Accordingly, the trend towards tailored or individualized patient education is growing. Results from several recent studies consistently indicate that when quality, interactive Internet-based interventions are provided, participants gain knowledge and improve health behaviours7,8. Patients who receive tailored information report that it is more relevant, interesting and motivating than those who receive general information 9 and they are better able to recall this information 10 .
In response to the need for accessible, quality health information that is tailored to meet individual patient needs, a patient education website called PEPTalk was developed. Just as a clinician prescribes a drug for an illness, health professionals use the PEPTalk database to select health information. Patients visit their clinician as usual, and are ‘prescribed’ those materials that meet their needs at that particular time. Clinicians access the PEPTalk website from a computer in their office, create a patient account, select the appropriate materials and an email message is sent to the patient advising them that an education plan is waiting for them at the PEPTalk website. A paper version of this process is also available.
Patients log on to the Internet from home or a community site and access their ‘prescription’. The site includes text and video materials of complex self-care activities such as wound care, gastrostomy feedings, exercises and preparing injections. Patients and their families are not restricted to those materials prescribed for them; they can browse the entire library as often as they wish. All materials on PEPTalk were reviewed by clinicians, were developed for a Grade 6 reading level and avoid any complex medical terminology. While usability testing has been conducted with the site, PEPTalk has never been implemented in clinical or community settings 11 .
A study was conducted to implement PEPTalk and to examine patient and community group members’ satisfaction and the impact of the health education materials on their health behaviour. Community staff and health providers’ experiences with the new education tool were also examined.
Design
A descriptive study using surveys and interviews was conducted. The study was approved by the investigators’ research ethics board and informed consent was obtained from study participants.
Sample
Three implementation models were introduced with three groups. Group one included patients from a Family Health team and cancer clinic who were ‘prescribed’ tailored health information on PEPTalk by nurses and doctors. Group two included community members from First Nations communities in Northern Ontario who were referred to PEPTalk by community staff; and the third group included personal support workers from a Toronto community agency who were directed to selected materials on PEPTalk by the project team for their personal use or to share with clients.
Data collection
Participants completed the Demographic Survey and Technology Skills and Access Survey which includes items such as age, education, computer/Internet skills. They also completed the Perceived Health Web Site Usability Questionnaire (PHWSUQ), developed by Nahm and her colleagues, after using the PEPTalk website 12 . The PHWSUQ measures three aspects of user experience with health websites: ease of learning the site, the utility of site resources and overall satisfaction. Evidence for the validity and reliability of survey items has been reported by the survey developers. Participants were also asked if the website materials had led to something new or different that they were doing regarding their personal health or their family’s health after using PEPTalk and to describe the impact of their learning on their health. Interviews were also conducted with four clinicians and staff using semi-structured interview guides. Participants were asked to describe their experience with PEPTalk referrals and the impact of the website on their patients’ or members’ health knowledge and health behaviour.
Data analysis
Descriptive statistics were calculated for the demographic survey, the PHWSUQ and physician referral numbers. The interviews were taped and transcribed. The interviews were then coded using each participant sentence as a unit of analysis and a content analyses was conducted to identify major themes within and across participant groups and with the open-ended survey items.
Results
Fifteen First Nations community members participated in the study. Their ages ranged from 21 to 69 years with the majority aged 40 to 59 years. Most had Internet access at home, had a grade or high school level education and ranked themselves as beginner or intermediate level Internet users (Table 1). The mean score for the total website satisfaction survey, the PHWSUQ, was 38.4 out of a possible 50 (SD = 4.5) and scores ranged from 32 to 45.
Demographic profile study First Nations and family health team patients
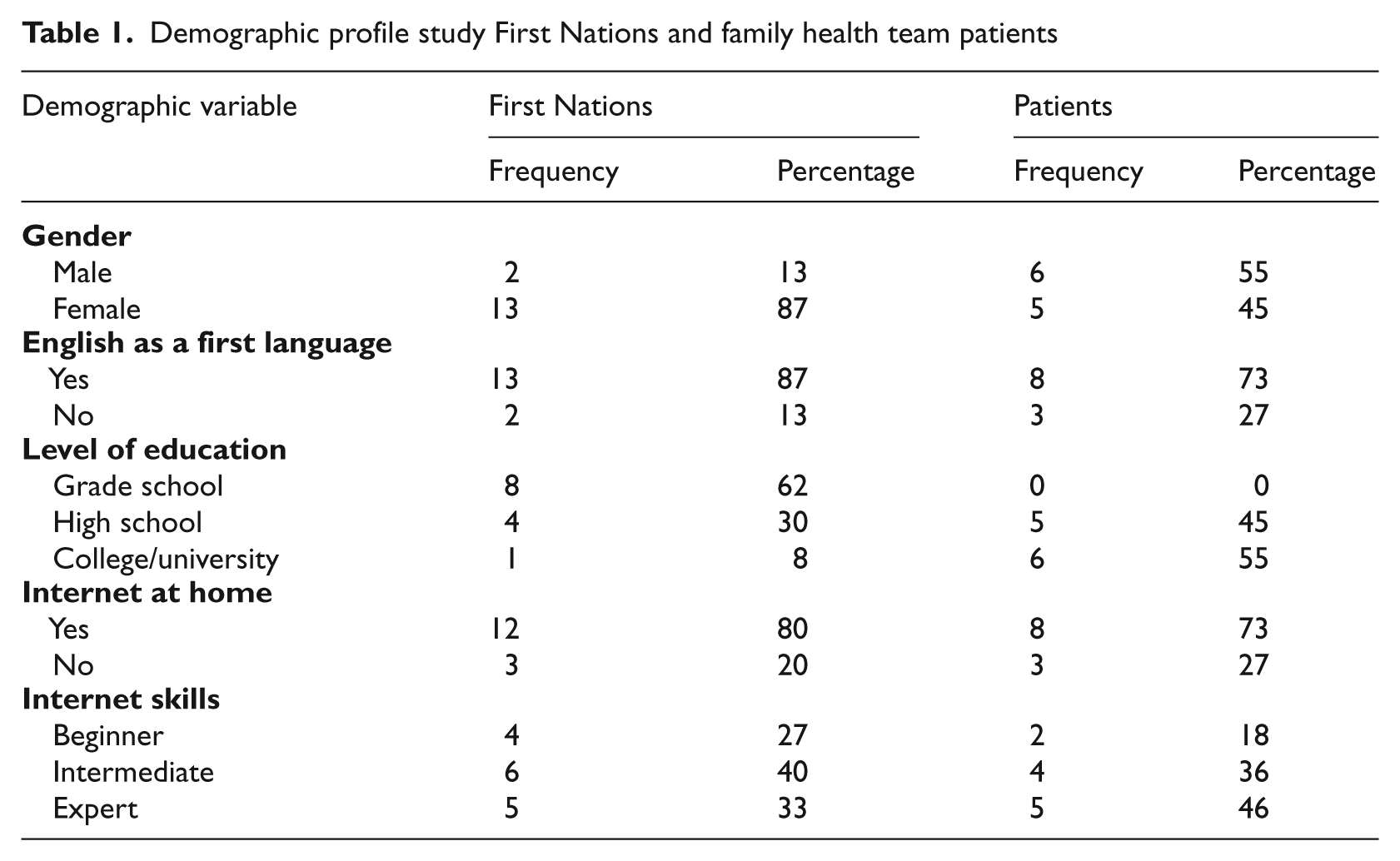
Twenty-nine patients accessed the PEPTalk website for health information, however, just eleven (38 per cent) completed the PHWSUQ. They ranged in age from 21 to 79 years. All had a high school or college/university education and the majority had home access to the Internet. The mean score for the total survey was 40.4 (SD = 4.7) out of a possible 50. Scores ranged from 33 to 48.
Nine community agency staff, their ages ranging from 32 to 59 years, explored PEPTalk as a tool to educate community members. All had access to the Internet at home and all reported that they used the Internet regularly for health information. The total mean score for the PHWSUQ was 48 out of 50 (SD = 1.2).
The First Nations community members’ and patients’ mean scores were very similar for most items (Table 2). Most participants agreed that it was easy to find and read health material and that the material was relevant, useful and had improved their knowledge about health.
PHWSUQ item mean scores based on study site
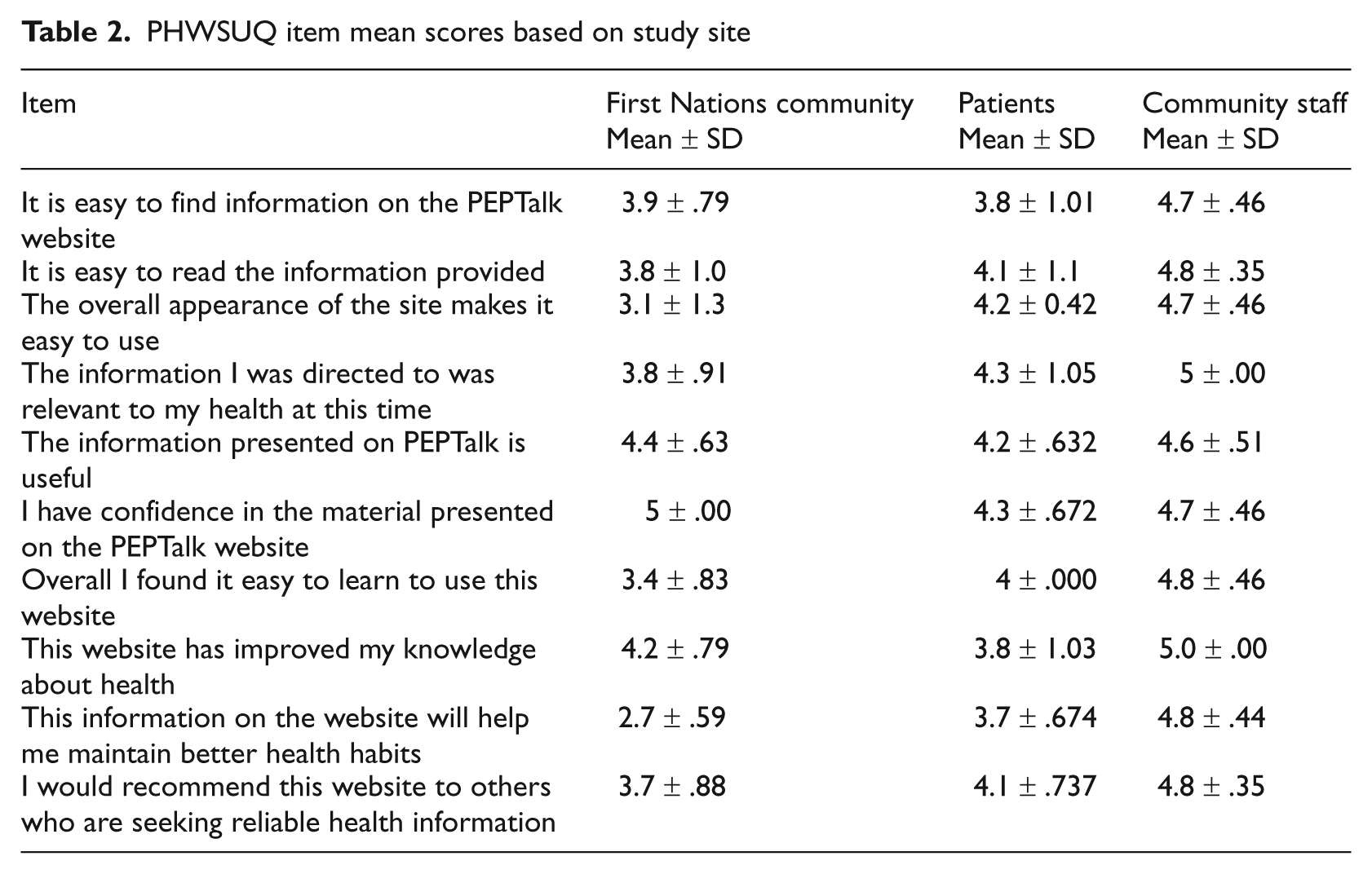
First Nations participants had lower scores for the items ‘The overall appearance of the site makes it easy to use’, ‘Overall I found it easy to learn to use this website’, and ‘This information on the website will help me maintain better health habits’. Patients scored lower for the item, ‘I have confidence in the material presented on the PEPTalk website’.
Open ended items
The PHWSUQ included four open-ended items where participants were asked to comment on how the site had been helpful and the impact of the health information they had accessed. Participants reported that one of the best features of PEPTalk was that materials were easy to read. Most participants noted that the site helped in one or more ways. It provided new information that assisted with decision-making regarding health and disease management situations such as diabetes and cancer, and family health concerns such as pregnancy, newborn care, parenting and eldercare. One participant noted, ‘It’s a good reference tool to make sure I am feeding her [her baby] the right food and the right amounts’.
Patients also noted that the site provided ongoing access to reliable information, and would serve as a reminder or incentive to try a new health promoting behaviour. One patient noted, ‘I’m following a back exercise regimen on regular basis now’. Another commented, ‘Instead of waiting for a doctor’s appointment, I can look up answers to my questions and just being able to go back and see what was it I was told but forgot already’. Another noted, ‘I thought it was a good resource from a trusted health professional to confirm all the information that is available on the web or that is passed to you from others’.
First Nations participants asked for more culturally specific material, including diet, exercise, and mental health material aimed at youth. Design recommendations included making the site more visual: ‘It looks very academic’. Several reported trouble downloading videos as they had low bandwidth in their communities.
Interviews
Interviews were conducted with four clinicians and community staff to understand their experiences with PEPTalk. Two were experienced family practitioners who regularly access websites and print materials or give patients URLs to review at home. They estimated that referring to PEPTalk adds about three to four minutes to a clinical visit: ‘If I’m running behind, it’s very difficult for me to incorporate it.’ They acknowledged that their time, however, might previously have been spent visiting the Internet and printing materials.
The primary advantage reported was that PEPTalk offers reliable, evidence-based information that they were comfortable sharing with their patients. Their patients felt more secure knowing that the materials had been vetted by their own doctor. While they believed that PEPTalk could positively affect a patient’s health, the education materials had to be integrated into the overall health care plan. One physician noted, ‘Information on its own, without an action plan or follow-up does not change patient behaviour’. The physicians also noted that PEPTalk requires patients to be active participants in their care. Instead of simply accepting a brochure, the patient has to log on to PEPTalk, create an account and then access the materials prescribed. This multi-step process is too much for those who are tired or anxious. The physicians supervise many new residents every year. Putting their top ten most frequently used topics on PEPTalk meant that their residents would have easy access to reliable, quality patient information. They also noted that ideally PEPTalk would interface with the electronic medical record. This would provide documentation regarding patient education which would have recordkeeping as well as legal benefits.
One clinician, a cancer clinic nurse, noted that his patients and their families are required to carry out some very complex feeding and wound care activities after surgery, on discharge home. The ability to review self-care videos, as often as needed, was reported as the most helpful aspect of PEPTalk.
A First Nations site facilitator recommended that search functions be improved on the site. Searching for health topics indexed by medical terminology, when English is not your first language, is a frustrating experience. The suggestion was made to set up an index of topics where users could click and select. The login process was identified as a barrier, partly for technical reasons, and also because it adds a step to accessing the site. The login and the issue of open access to information were also raised. The First Nations tradition is one of openness and sharing of information. Participants can understand the rationale for security and privacy for an individual’s personal health education account on PEPTalk; however, they wondered about the possibility of opening access to the library of materials on PEPTalk.
Discussion
Patient and community members’ satisfaction with PEPTalk, a website that houses ‘vetted’ health information, was measured through surveys and interviews. The mean score for the website satisfaction survey for patients was 40.4 (SD = 4.7) out of a possible 50, indicating that most patients were very satisfied with PEPTalk. The mean score for First Nations users was 38.4 (SD = 4.5), indicating a moderately satisfactory experience. Participants from all sites reported that they found the information presented on PEPTalk useful and relevant and that they had improved their knowledge of health.
While results for most survey items were similar, they differed significantly for the two groups in regard to items regarding learning to use the site. One aspect where the two groups differed was educational level. All patients in this study had a high school or college/university education. Most participants from the First Nations communities had a grade school education. Educational status might have influenced users’ abilities to navigate the site and has implications for improving the site design and navigation process. The mean score for the PHWSUQ for the community agency personal support workers was 48 out of 50. That very high satisfaction score reflects the keen interest this group has in having access to reliable health information for their own professional development to support client care.
Interview results with physicians were very positive regarding the benefits of PEPTalk. They also suggested that while some patients appear keen to use PEPTalk in the office, when they get home they become busy with other activities and they forget or do not bother to visit the site. It is possible that the requirement for action, which includes logging on to the site, setting up an account and accessing materials is too demanding for some patients.
Participants at the two community sites had a different experience with PEPTalk. They were given a demonstration or one-to-one assistance to get onto the site; individual accounts were not created for these users. This approach worked well as beginning website users received the support they needed for their initial experience.
Implications for further development
The results, supported by other studies, indicate there is a definite need for reliable, quality, evidence-based health information, housed in a way that makes access simple and easy, similar to that offered through sites such as PEPTalk 13 . Online tools will become an important component of public health education and will have significant implications for better utilization of scarce health care resources and empowering people to take active roles in managing their health 14 .
A key issue to address in the ongoing development of these sites is to ensure that a quality assurance system is maintained. Establishing a review board to oversee the addition of new materials and checking that information remains current and is evidence-based, will be key to ongoing success of the system. Regarding website design, it is essential to establish site credentials on the site home page, provide information on the site sponsor/developer, site purpose and outline the quality assurance process.
While emerging tools such as PEPTalk can be very useful, it is critical that we do not create more barriers to health education; the role of a community agency Internet facilitator should be explored; a recommendation supported by recent studies regarding the value of mediated access to verifiable health information 15 . Further, it will be important for clinicians and health providers not to simply ‘hand the patient over’ to sites like PEPTalk, believing that health education has been addressed 16 . The provider’s role regarding interpretation, discussion and follow-up will remain essential, and tools such as PEPTalk need to be part of an overall health education strategy.
Learners’ needs and characteristics should continue to guide design, technology and content choices. Participants in this study appreciated the simple, easy-to-read materials they used. As PEPTalk and similar sites develop, it will be important to ensure that new materials are written for the lay population and that complex, clinician-oriented materials do not trickle onto the site. Future development should include converting some text materials into picture-rich aids, as the literature suggests that printed text is the least effective means of communicating with patients 17 . Ongoing research that tests these new developments is essential and will help to determine if users’ needs are being met.
Study limitations
It should be noted that the results generated from qualitative data collection methods such as the interviews used in this study are not intended to be generalized. Further, the study’s sample was small and self-selected and the response rate for the patient survey was low; results cannot be generalized to the larger population of patients, community members and staff. Participants in this study had some familiarity with the Internet; PEPTalk has not been tested with Internet novices. A further limitation is that self report measures were used to measure patients’ knowledge gains. Further research is needed including a larger study using a randomized controlled trial to investigate users’ knowledge and health behaviour gains in comparison with standard patient education approaches.
Conclusion
These results support the development of websites such as PEPTalk that house basic health information which has been validated by clinicians and where health materials may be tailored to meet individual needs. Tools such as PEPTalk can simplify the health education process and give users confidence in the materials they retrieve. This form of public health education has significant implications for better utilization of scarce health care resources. We anticipate that Internet access and the ability to tailor health materials will promote health education for all, but in particular for those who face traditional barriers related to literacy, education and geography.
Footnotes
Acknowledgements
The authors would like to acknowledge the generous support provided by the Canadian Council on Learning and our partner organizations, without whom, the study would not have been possible: Centennial College, George Brown College, Keewaytinook Okimakanak Research Institute, St. Christopher House and The Centre for Effective Practice staff and clinicians. We also extend our thanks to Dr Jonathan Irish and Romeo Cruz, RN., Wharton Head and Neck Centre, Princess Margaret Hospital for their contribution.