
Abstract
Background:
Long-term behaviour change in type 2 diabetic patients may provide effective glycemic control.
Purpose:
To investigate the key factors that promote behaviour change in diabetic subjects using the transtheoretical model.
Methods:
Subjects were selected by purposive sampling from type 2 diabetes outpatients. Self-administered questionnaires were used to collect the data related to the stages of behavioural change. HbA1C* values were measured to evaluate glycemic control. Data were analyzed with analysis of variance (ANOVA), multiple regression and multinomial logistic regression.
Results:
Routine management of diabetes was a key factor in behaviour change, which correlated indirectly with HbA1C values through compliance and was positively affected by social support. Undermining from family or friends was directly associated with HbA1C.
Conclusions:
Based on factors influencing stages of behaviour change in diabetic subjects, tailoring a programme to help patients balancing life-style with diabetes, strengthening the patients’ perceived confidence in routine management, and establishing a patient-friendly environment as well as support systems may show promise for changing the behaviours in all diabetic patients.
Introduction
Type 2 diabetes is a major global public health challenge facing the 21st century. 1 It is estimated that, globally, there are currently 245 million people with diabetes and within 20 years that number will increase to 380 million. 2 In order to achieve effective diabetes control, patients are being educated to eat a healthy diet, exercise regularly, monitor blood glucose, and take medications as prescribed. However, many healthcare professionals have expressed frustration and concern that, regardless of their best efforts, patients do not regularly monitor their blood glucose, do not follow the recommended diet and exercise programme, and do not comply with doctors’ orders.3,4 To date, fewer than one-half of all diabetic patients receive appropriate care and enjoy a good quality of life.5,6 In addition, more than 95% of diabetes care is done by the patient. 3 Long-lasting behaviour change is needed for patients to achieve more effective self-care, but this change is complex and not easily achieved by the patients because it requires a strong intention to change, 4 and also more emotional and psychological support. 7 In consideration of improving the overall quality of care for diabetic patients, the psychological factors and supporting mechanism are of great importance.
Bandura 8 proposed that a change in human behaviour is not just determined by a single factor but by the results of interaction among three factors, including personal factors, environmental influences and behaviour. Behaviour change, in other words, is explored from multiple perspectives, emphasizing the importance of individual cognition process on behaviour change. Social cognitive theory, which recognizes that social interactions and experiences influence an individual’s cognitive development, has been widely applied to health behaviour and other fields. Social support is an important step in the self-regulation process of social cognitive theory 9 and self-efficacy is the core of psychological determinants of behaviour. 10 Previous studies have reported that social support has a positive impact on glycemic control and adherence,11,12 and plays an important role in helping patients make and maintain meaningful behavioural changes successfully.11,13,14 Yet, to sustain the behavioural changes persistently, patients should adhere to the belief – that is, the self-efficacy – which relates to achieving glycemic control and good compliance.15–17 According to the study of Nakahara et al., 18 social support influences HbA1C values indirectly through increased self-efficacy. Self-efficacy directly reinforces adherence, and adherence correlates directly with HbA1C, so psychosocial interventions may be useful for long-term good blood glucose control in patients with type 2 diabetes.
The transtheoretical model is another model that can be applied in intervention designed to assess behaviour change in people with diabetes. Characterized by treating behaviour change as a dynamic process, 19 it includes five stages of change that individuals progress through when changing behaviour: (1) pre-contemplation; (2) contemplation; (3) preparation; (4) action; and (5) maintenance.20,21 These five stages of behaviour change rarely follow a linear path from beginning to end,22,23 and may be more like a spiral pattern of change by beginning at any one stage and moving around through different stages. 21 The majority of previous studies that have applied the transtheoretical model to the field of diabetes have demonstrated significant positive effects; that is, increases in the frequency of self-monitoring of blood glucose levels in diabetic patients who accepted interventions based on the transtheoretical model,24,25 significantly higher percentages of patients improving exercise behaviour, 26 improved eating behaviour of participants after intervention, 27 and significantly lower mean HbA1C values in later stages of change rather than earlier stages. 25 Therefore how or what factors have contributed to maintaining behaviour change continuously, without resulting in relapse, is an issue worth probing.
In overview, to achieve effective self-management, it would be helpful to set priorities for implementation and develop effective strategies by further identifying the factors that influence the stages of change. Therefore this research combined the concepts of social cognitive theory and the transtheoretical model to investigate the key factors of behaviour change in people with diabetes. The aims of this study were: (1) to assess the differences in social support, self-efficacy, compliance, and HbA1C values among diabetic patients at different stages of behaviour change, based on their daily behaviours of blood glucose monitoring, regular exercise and diet control; (2) to examine the relationships between social support, self-efficacy, compliance, and HbA1C values; (3) to investigate the key factors that influence daily behaviours of blood glucose monitoring, regular exercise, and diet control at stages of behaviour change; and (4) to provide references for diabetic patients to develop behaviour change strategies.
Methods
Study participants
Subjects were selected from outpatients with type 2 diabetes who had visited the Department of Metabolism of a regional teaching hospital in Hsinchu City, Taiwan, for one or more years. We used a purposive sampling method to recruit eligible patients during all clinic sessions occurring in December 2009. Inclusion criteria were to have a primary diagnosis including up to three diagnostic codes in the International Classification of Diseases, Ninth Revision, Clinical Modification: 250. A total of 317 self-administered questionnaires were collected.
Research scale design
The data used in this study were collected from self-administered questionnaires and HbA1C values of patients’ laboratory assays on the date closest to the study period. The contents of the questionnaires included: patients’ characteristics; compliance; stages of behaviour change; social support; and self-efficacy. The questionnaire was constructed through literature review and referenced according to the diabetes care profile of the University of Michigan Diabetes Research and Training Centre. 28 It was reviewed by an expert panel, including two specialist physicians, two dietitians, one social worker, and one health educator, then amended, pre-tested, and revised before the final version. Detailed items were described as follows:
Patients’ characteristics
Patients’ characteristics included gender, age, education, duration of diabetes, family history of diabetes, and treatment pattern.
Compliance
Compliance was derived from the patients’ perception of following physicians’ orders for taking medicine within one year prior to the study. It was scored by a five-point Likert scale ranging from 1 = rarely compliant to 5 = fully compliant.
Stages of behaviour change
The five stages of change are evaluated according to Prochaska and Diclemente,20,21 who proposed the transtheoretical model. The questionnaire used in this study consisted of three dimensions: blood glucose monitoring, regular exercise, and diet control, for which patients checked the best description of their stage at present for each separate dimension. Questions were stated as previously reported by Byrd-Bredbenner and Finckenor; 29 for example, which statement best describes you? (self-monitoring at least one time per week): (1) I am not monitoring my blood sugar, and I have no plan to do in the next six months; (2) I am not monitoring my blood sugar, but I plan to do in the next six months; (3) I am not monitoring my blood sugar, but I plan to do in the next 30 days; (4) I am monitoring my blood sugar, but I have been doing so for less than the past six months; (5) I am monitoring my blood sugar, and I have been doing so for more than the past six months. For the other dimensions, another action phrase is substituted, such as exercising regularly at least three times every week, 30 minutes/each time, doing diet control every day. The numbering of answers (one through five) corresponds to the five stages of change20,21 as follows: (1) pre-contemplation stage; (2) contemplation stage; (3) preparation stage; (4) action stage; and (5) maintenance stage.
Social support
The questionnaire used in this study was referenced by the diabetes care profile of the University of Michigan Diabetes Research and Training Centre 28 and included three dimensions and 11 items; that is, the patient felt support from his family or friends, emotional support (three items); his/her family or friends did not express critical or negative behaviour, no undermining (three items); and his/her family or friends gave assistance and support, helping relationships (five items). Each item was scored on a five-point Likert scale (from 1 = strongly disagree to 5 = strongly agree).
Self-efficacy
The measurement of self-efficacy in this study was referenced by the Diabetes Self-Efficacy Scale (DSES) 30 and Perceived Diabetes Self-Management Scale (PDSMS), 31 and included five dimensions and 20 items; that is, the patient’s belief of routine management in diabetes care (six items); the efficacy of diet management (four items); the confidence of self-treatment (seven items); the perceived ability of coping with problems (two items); and the regular exercise intention (one item). Each item was scored on a five-point Likert scale (1 = strongly disagree to 5 = strongly agree)
HbA1C measurement
HbA1C data were collected from each patient’s laboratory assay on the date closest to this study, performed by Cation-Exchange high-performance liquid chromatography (HPLC) with demonstrated specificity and sensitivity of < 5%.
Data analysis
Descriptive statistics, such as mean, standard deviation, and frequency were used to investigate the distribution of patient characteristics, HbA1C values and stages of behaviour change. Analysis of variance (ANOVA) was used to analyze the psychosocial factors, compliance, and HbA1C values in relation to the differences in stages of behaviour change. Multiple regression analysis was used to examine the relationship between psychosocial factors, compliance, stages of behaviour change and HbA1C values. Multinomial logistic regression was used to assess the influences of psychosocial factors and compliance in stages of behaviour change. SPSS 15.0 was used for all analyses. A confirmatory factor analysis (CFA) was used to examine the reliability and validity of the self-administered questionnaires.
Results
Study participant characteristics
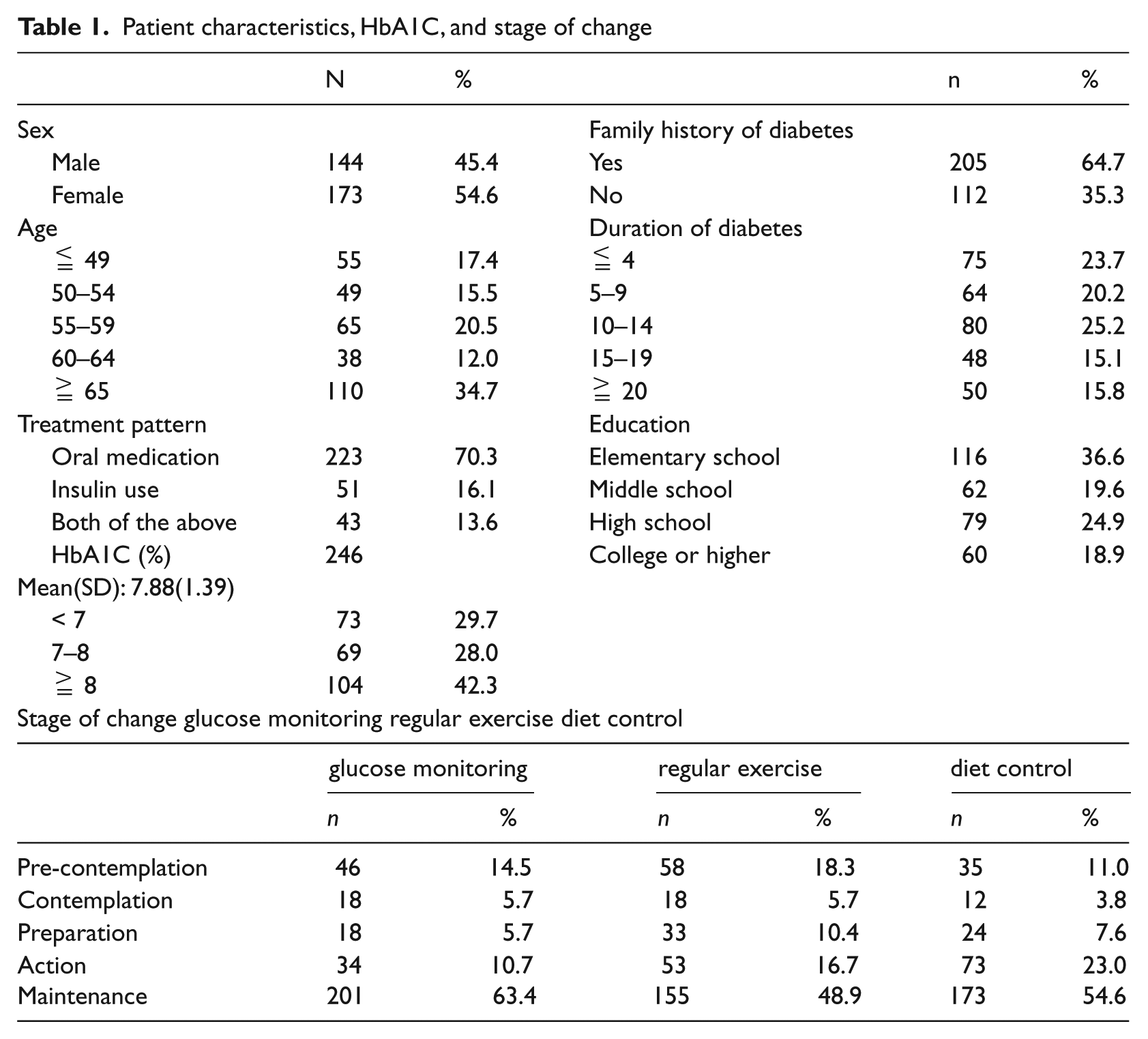
Among the 317 participants, 45.4% were men and 54.6% were women. Those aged >= 65 accounted for 34.7% and those with 5–14 years of duration of diabetes for 45.4%. Those with family history of diabetes accounted for 64.7%, and 70.3% were receiving oral medication. About one-third (36.6%) had a primary school education. Mean HbA1C values were 7.88%, for which 42.3% were higher than 8%. In terms of stages of behaviour change, approximately three-quarters of diabetic patients (74.1% and 77.6% had blood glucose monitoring and diet control behaviours respectively) were in action and maintenance stages, 14.5% or 11.0% were in pre-contemplation stage. Of the diabetic patients, 65.6% had regular exercise and were in action and maintenance stages and 18.3% were in pre-contemplation stage (Table 1).
Patient characteristics, HbA1C, and stage of change
Reliability and validity of the measurement
The variables of psychosocial factors derived from the two main core concepts of social cognitive theory are social support and self-efficacy. Based on the implications, the items in the social support questionnaire were classified into three dimensions and the items in the self-efficacy questionnaire were classified into five dimensions. The confirmatory factor analysis (CFA) was used to examine the reliability and validity of the self-administered questionnaires, the results were as follows: social support included three dimensions (emotional support, no undermining and helping relationships) and 11 items, for which Cronbach’s α ranged from 0.70 to 0.84, the factor loadings by CFA were 0.66–0.91, 0.42–0.86, and 0.74–0.85 respectively. Self-efficacy included five dimensions (routine management, diet management, self-treatment, perceived ability, and regular exercise intention) and 20 items, for which Cronbach’s α ranged from 0.79 to 0.89, the factor loadings by CFA were 0.47–0.89, 0.60–0.96, 0.36–0.81, 0.66–0.99, and 1, respectively. The Cronbach’s α mentioned above were all > 0.70 demonstrating higher consistency of the scales. Factor loadings were almost all >= 0.4, indicating good construct validity.
Differences in social support, self-efficacy, compliance, and HbA1C values at stages of behaviour change
The stages of change in the contemplation and preparation stages represented patients who had already planned but not yet acted, which accounted for a lower percentage of participants, 3.8–10.4% (Table 1); therefore we combined them into contemplation/preparation stage (currently do not but have plans to do) to analyze in this study. Thus the stages became four stages: pre-contemplation, contemplation/preparation, action, and maintenance stages. The results are shown in Table 2, and were determined by ANOVA. With regard to regular exercise and diet control, the scores of social support in later stages of behaviour change were higher than those in the earlier stages and had statistical significance. The scores of self-efficacy and compliance in blood glucose monitoring, regular exercise, and diet control in later stages of behaviour change were higher than those in the earlier stages. Especially self-efficacy showed a gradually increasing trend from pre-contemplation to maintenance stages of behaviour change. HbA1C values in contemplation/preparation stage were higher than those in other stages.
ANOVA of the social support, self-efficacy, compliance, and HbA1C values at stages of behaviour change
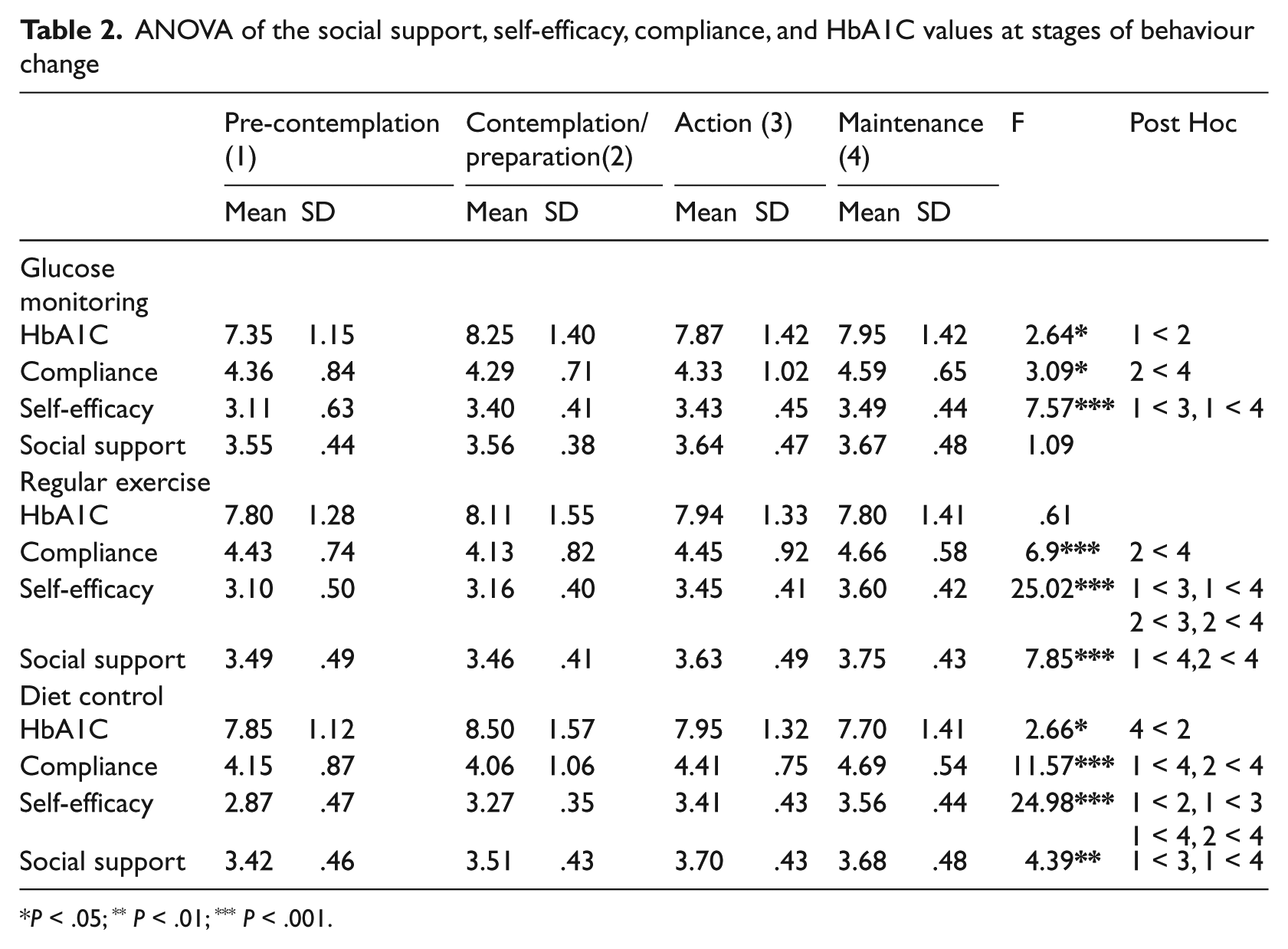
P < .05; ** P < .01; *** P < .001.
Relationship between social support, self-efficacy, compliance, and HbA1C values
First, we identified the impact of social support, self-efficacy and compliance on HbA1C values using multiple regression analysis controlling for stages of change, as shown in Table 3. The greater patients’ compliance, the lower their HbA1C values; and the more family or friends expressed critical or negative behaviour, the higher HbA1C values. Second, we examined the effects of social support and self-efficacy on compliance, and the results demonstrated stronger efficacy of routine management in diabetic patients corresponding to higher compliance. Finally, we analyzed the influence of social support on various dimensions of self-efficacy: the three dimensions of social support (emotional support, no undermining and helping relationships) enhanced the efficacy of routine management; increased confidence of diet management required the support of helping relationships and no undermining from family or friends; the ability of self-treatment depended on emotional support and helping relationships; and the perceived ability of coping with problems relied on emotional support and no undermining which also affected the exercise intention (Table 4), among the relationships shown in Figure 1.
Multiple regression analysis for the relationship among social support, self-efficacy, compliance, stages of behaviour change, and HbA1C values
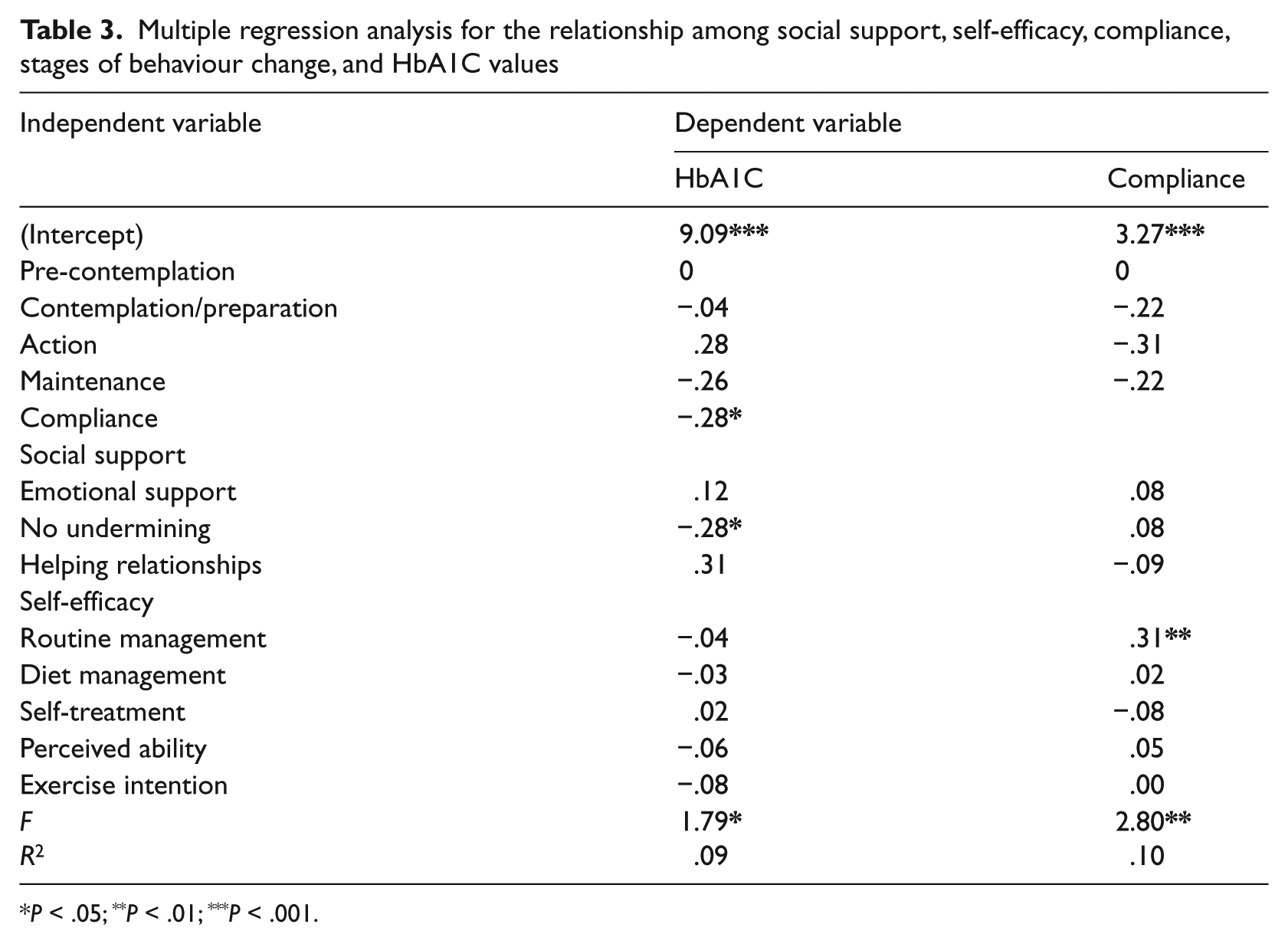
P < .05; **P < .01; ***P < .001.
Multiple regression analysis for the relationship among stages of behaviour change, social support, and self-efficacy
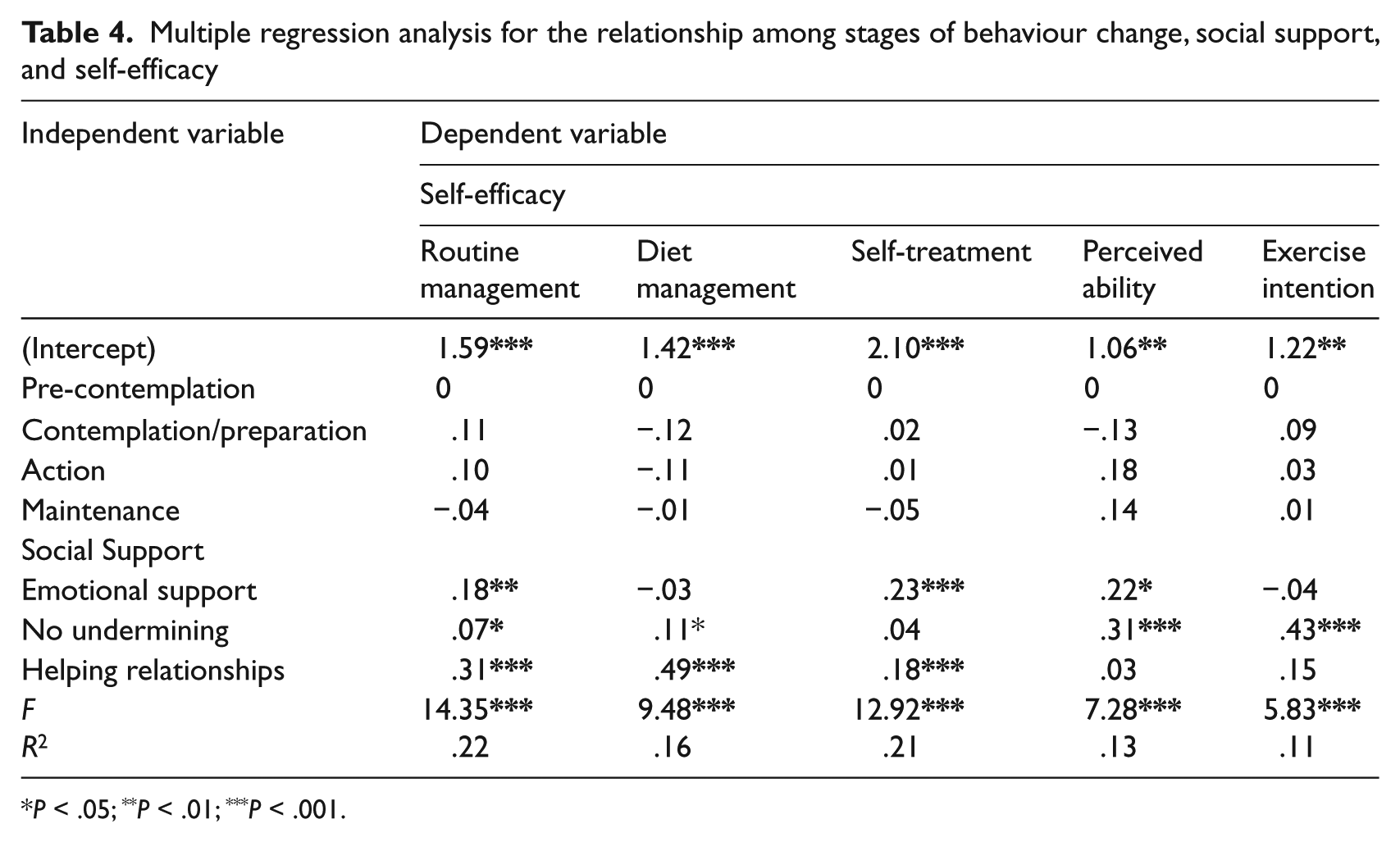
P < .05; **P < .01; ***P < .001.
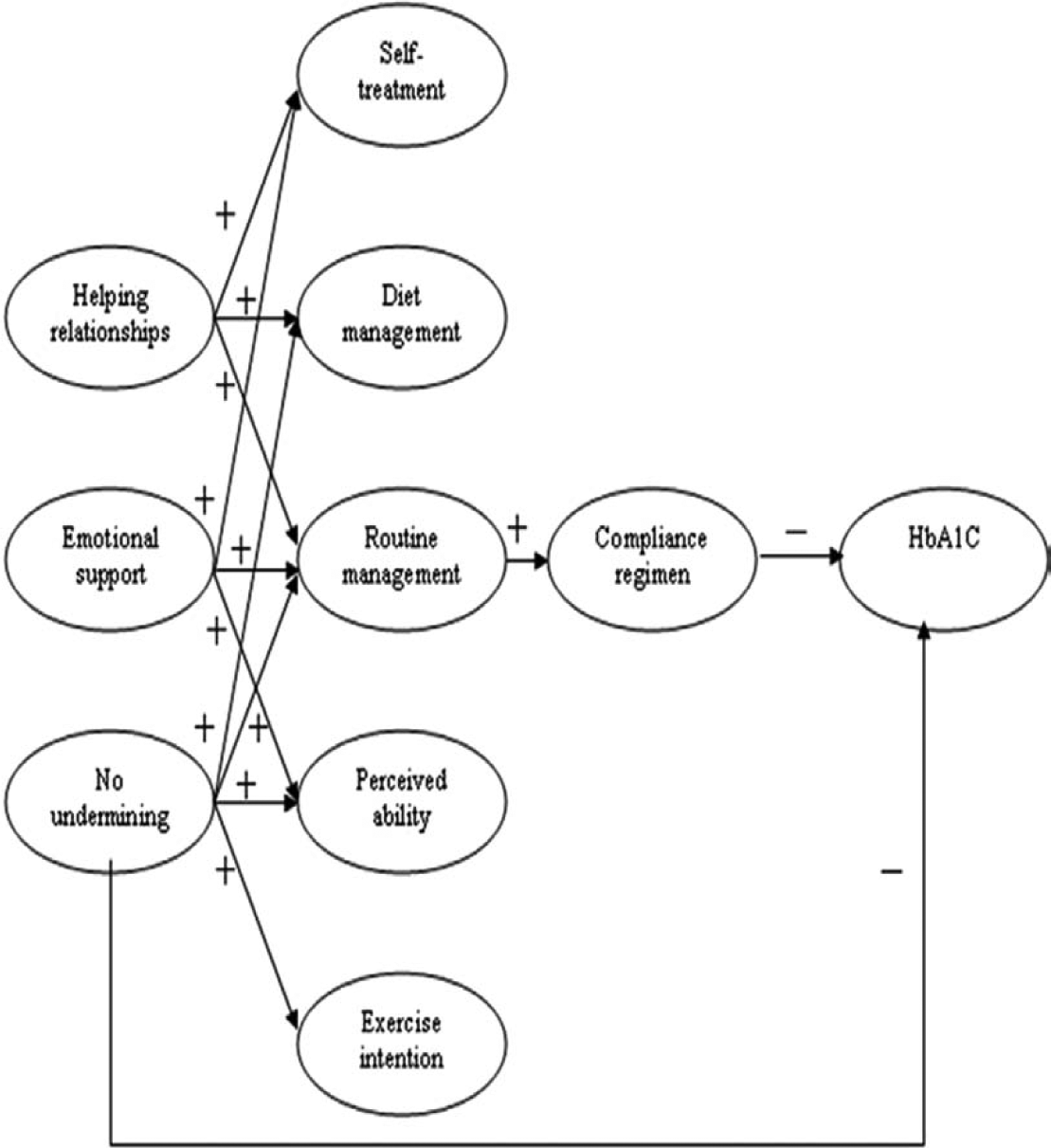
Relationship among social support, self-efficacy, compliance, and HbA1C
Key factors influencing the stages of behaviour change
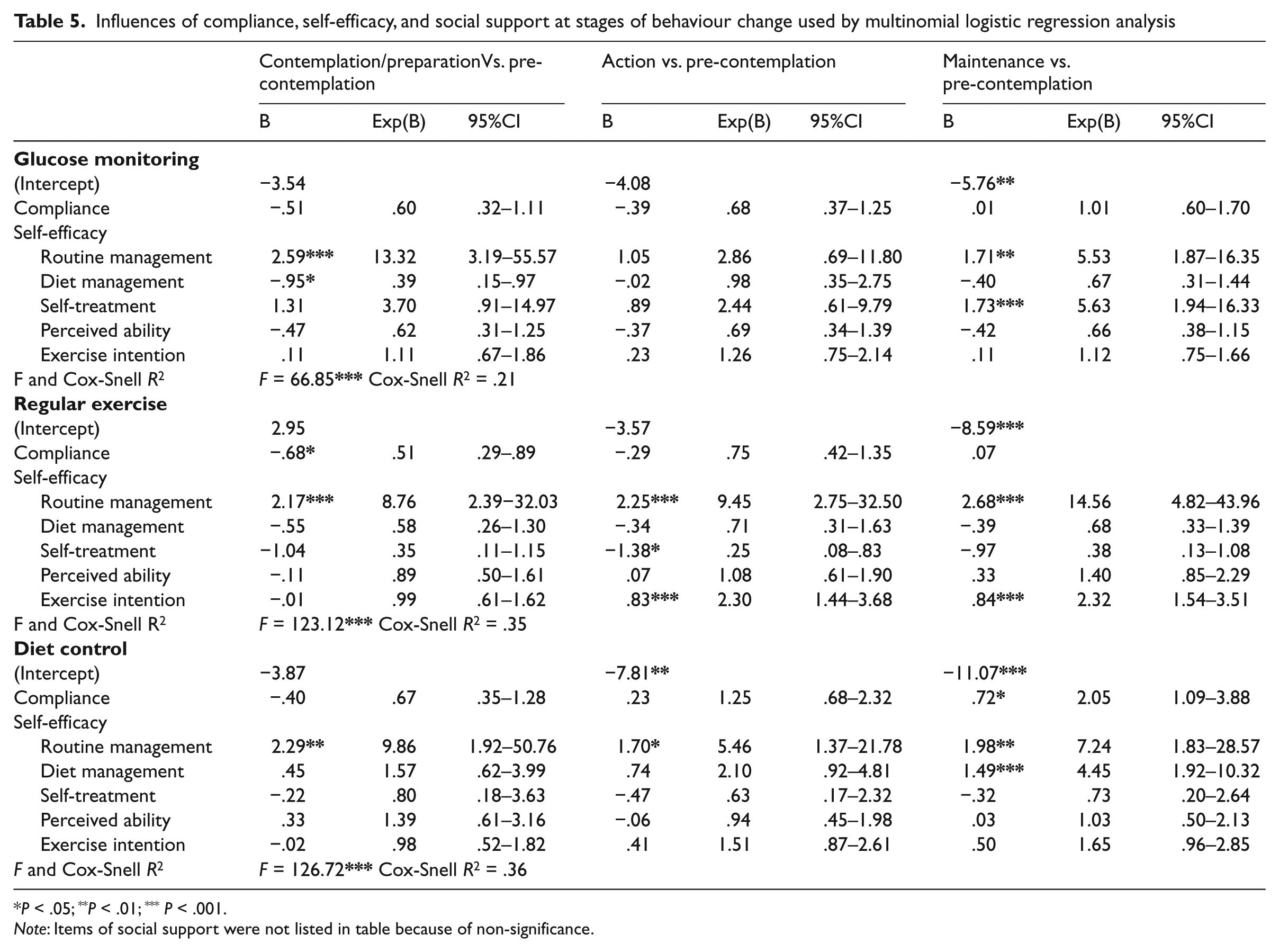
Multinomial logistic regression was used to further assess the influences of psychosocial factors and compliance in stages of behaviour change. As shown in Table 5, the routine management of diabetes was the key factor that influenced the stages of behaviour change in blood glucose monitoring, regular exercise, and diet control. The efficacy of routine management was higher in other stages than that in the pre-contemplation stage, which was 13.32 times higher, especially in blood glucose monitoring. Regular exercise and diet control were 8.76, 9.45, 14.56 times and 9.86, 5.46, 7.24 times higher in other stages than that in the pre-contemplation stage, respectively. Factors affecting the maintenance stage were self-treatment, exercise intention and diet management, which were 5.63, 2.32, and 4.45 times higher by comparing maintenance to pre-contemplation respectively. Social support did not have a significantly direct effect on stages of behaviour change.
Influences of compliance, self-efficacy, and social support at stages of behaviour change used by multinomial logistic regression analysis
P < .05; **P < .01; ***P < .001.
Note: Items of social support were not listed in table because of non-significance.
Discussion
Summary of the main findings
This research combined partial concepts of social cognitive theory and the transtheoretical model to investigate the key factors of behaviour change in people with diabetes. The main findings were as follows: social support, self-efficacy, and compliance had significant differences in stages of behaviour change. Especially self-efficacy showed a gradually increasing trend. HbA1C values in contemplation/preparation stage were higher than those in other stages. Compliance and no undermining from family or friends were both directly negatively associated with HbA1C values. Routine management of diabetic patients was a key factor in behaviour change, which had a direct positive correlation with compliance, and was positively affected by social support (emotional support, no undermining, and helping relationships). The behaviour change of blood glucose monitoring was also influenced by the factor of self-treatment which was further strengthened through emotional support and helping relationships. The behaviour change of regular exercise was also impacted by the factor of exercise intention which was further enhanced through no undermining. The behaviour change of diet control was also affected by the factor of diet management which was further improved by no undermining and helping relationships.
Interpretation of results
Studies have shown that social support and self-efficacy were associated with glycemic control;11,12,15–18 however, to our knowledge, the influence of each dimension on the social support and self-efficacy has not been previously investigated and reported in the literature. In our research, we investigated and identified the dimensions that were most critical for influencing behaviour changes in diabetic patients.
However, life-long behaviour change is bound to vary with each individual. To understand the current situation of the patient’s behaviour change and to tailor an optimal action plan could help to increase the probability of successful behaviour change. In this study results demonstrated that social support (except for on blood glucose monitoring) and self-efficacy were significantly higher in the action or maintenance stage than those in the pre-contemplation or contemplation stage. The compliance was significantly higher in maintenance stage than that in contemplation stage. Therefore the majority of studies suggested that reinforced social support, self-efficacy and compliance worked together to maintain good blood glucose control,18,32 some researchers also reported positive results by applying the transtheoretical model to behaviour change in patients with diabetes.24–27 Helitzer et al. 33 proposed that stage of behaviour change may be a good predictor of attendance in diabetes prevention programmes. However, the HbA1C values (except for on diet control) were not significantly lower in the later stages of behaviour change than those in the earlier stages. The HbA1C values, in any case, on blood glucose monitoring, regular exercise, and diet control behaviour, were 8.0% higher (which signified a poor glycemic control) in the contemplation/preparation stage than in other stages. This unexpected finding might be due to the fact that this study was a cross-sectional study, which had the difference between the time the HbA1C values were collected and the time of the patients’ completion of the questionnaire with their perception of stage of behaviour change. The other possible explanation was that the patients recognized that having an HbA1c around 7.0% was within the range of acceptance in pre-contemplation stage, so they had no intention and no plan to make behaviour changes. Yet when higher values were obtained for HbA1C, patients became alert of the severity of their illness, and took action towards behaviour change. This finding coincided with the health belief model that patients’ perceived severity of illness could contribute to taking preventive action. 34
Social support includes multiple dimensions and self-efficacy as well.35,36 The question is which dimensions within the social support and self-efficacy are most critical for influencing behaviour change. In order to identify the path of relationships among variables in detail, multiple regression analysis was further used in controlling the stages of behaviour change, which showed that compliance and no undermining (one dimension of social support) had direct negative effects on HbA1C, while routine management (one dimension of self-efficacy) had a direct positive impact on compliance, the routine management was also influenced directly by social support (Figure 1). This result was consistent with the findings by Rhee et al. 37 which stated that patient adherence was directly associated with substantial improvements in HbA1C values, and Nakahara et al. 18 stated that social support influences HbA1C values indirectly through increased self-efficacy, which directly reinforces adherence, and adherence correlates directly with HbA1C. As compared to previous studies, our study further clarified the impacts of various dimensions on the social support and self-efficacy; particularly no undermining was directly negatively associated with HbA1C. Rose et al. 17 indicated that the mood status of people with diabetes affected blood glucose control. Therefore social support may improve the psychosocial adjustment to diabetes. 38 However, negative criticism or behaviour (i.e. undermining) may lead to reductions in social motivation. As a result, the vicious cycle of behaviour impeded the adoption of effective self-management behaviours that directly influenced glycemic control. The explanation power of routine management toward compliance was stronger than that of the other four factors, and routine management was positively influenced by social support. This result was in accordance with the findings by Rapley et al. 30 In their review, diabetic routine management, which covered diabetes self-care in general, was the strongest factor on the diabetes self-efficacy scale.
This study, based on the transtheoretical model using multinomial logistic regression analysis, was to investigate the key factors influencing patients’ behaviour in stages of change. The routine management was the most critical factor influencing the behaviours change of self-management (blood glucose monitoring, regular exercise, and diet control) in people with diabetes. The patients’ perceived confidence in routine management may be sufficient to represent self-efficacy. Therefore patients should be able to control blood glucose successfully, even without any further detailed diabetes-related knowledge, as long as they follow through with routine management and patients’ training programme enhancing self-management confidence. 17 This would further help patients progress through the stages of behaviour change to an advanced stage without going backwards. 19 Finally, with the increased access of support from family, friends, workplace, community, and the media, 39 and appropriate assistance in a timely manner, 7 glycemic control for diabetic patients could be achieved effectively.
Strength and limitations
There are some limitations to this study. First, study participation depended on the patient’s consent so there may have been a selection bias. Second, the questionnaire itself may have been biased, despite expert review. Third, results from a single hospital may not be generalized. Fourth, time effect on HbA1C was not considered in this study.
Conclusions
In this study, social support, self-efficacy, and compliance demonstrated differences in stages of behaviour change in type 2 diabetic patients. Routine management was a key factor in maintaining lasting behaviour changes, which had a direct positive correlation with compliance, and was positively affected by social support. Therefore the behaviour change strategies should depend on individuals’ stages of behaviour change to understand the specific demands in depth and the need for a social network is necessary to develop a tailored self-management plan. In addition, strengthening the social education of positive support to patients, establishing a patient-friendly environment (especially avoiding negative criticism or behaviour towards the patients), and designing a support system with social resources to improve the patients’ perceived confidence in routine management and find a balance in life-style with diabetes may be the best way to achieve sustainable behaviour change and promote better blood glucose control.