
Abstract
Objective:
To discuss how the effects of culture, economy, and geographical location intersect to form a gestalt triad determining health-related disparities in rural areas.
Methods:
We critically profile each component of the deterministic triad in shaping current health-related disparities in rural areas; evaluate the uniquely composed intersections of these disparities in relation to Human Papillomavirus (HPV)-related cancer prevention in three isolated rural Georgia counties; and develop implications for future leadership in rural healthcare research, policy, and practice.
Results:
The deterministic triad of culture, economy, and geographical location is unique to a rural community, and even if two rural communities experience the same health disparity, each community is likely to have a discretely different composition of cultural, economic, and geographic determinants.
Conclusion:
The deterministic triad presents a challenge for health policymakers, researchers, and practitioners trying to develop health-related interventions that are equitable, efficacious, and practical in low-resource rural communities. The situation is worsened by the limited opportunities for employment, which leads to greater disparities and creates propagating cultural norms that further reduce access to healthcare and opportunities for sustainable health promotion.
Before and after the United States (US) Food and Drug Administration’s (FDA’s) approval of the Human Papillomavirus (HPV) vaccine for girls, research contributed heavily to scientific knowledge about the public’s attitudes and perceptions with regard to HPV. 1 However, much of that research focused, often exclusively, on HPV vaccination in urban areas among people who sought medical attention at urban healthcare clinics. Although some studies were done in rural areas, they were done principally before or soon after FDA approval of the HPV vaccines. 1 In addition, few if any studies focused explicitly on the HPV vaccine-related knowledge, attitudes, and beliefs of parents with children, either boys or girls. 2 Consequently, a substantial gap exists in the knowledge base upon which health policymakers and health professionals form programmes to increase HPV-related cancer prevention among rural and underserved boys and girls before their first sexual encounter.
A new line of research has begun to fill this knowledge gap, and findings show that local culture, geographic location, and economics intersect to form a gestalt driver of health-related disparities. 3 While conducting HPV-related cancer prevention research in three rural counties in Georgia (Burke, Lincoln, and Screven), we wanted to develop a culturally relevant intervention that was anchored in sound evidence and tailored to the communities we were studying. The resulting quantitative and qualitative analysis of data gathered during our research in Georgia’s rural Burke, Lincoln, and Screven counties is published in detail elsewhere. 4 Describing, recognizing, and understanding this triad of geographic, economic, and cultural health disparities is, we believe, essential to the development of practical and equitable interventions to prevent HPV-related cancer in isolated rural communities.
Background
Ferris and colleagues have documented the overall limited parental acceptance and knowledge of the HPV vaccine as well as the low adherence rates to a three-shot vaccine series. 5 Adherence rates are frequently lower in rural than in urban areas, and the US Centers for Disease Control and Prevention (CDC) has noted that the HPV series uptake rates in Burke, Screven, and Lincoln counties in Georgia were particularly low (17%–18%), much lower than both the overall Georgia rates and the national rates. 6 The findings from these studies and others show a need for education on HPV transmission and general HPV vaccine knowledge beyond what public health officials first thought would be needed in rural areas. 7 The need to address HPV-related cancer prevention in rural areas is clear, but the complexity and interaction of culture, economics, and geography must be taken into account when any strategy to prevent HPV-related cancer is being developed.
Culture
People’s perception of cancer risk and their level of trust in the healthcare system are affected by the culture of the community in which they live. Therefore it is essential to understand a community’s culture and its effect on health behaviours before designing a disease-prevention or health-promotion programme. Any health-promotion programme must be based on the viewpoint of the community’s residents rather than on the possibly biased viewpoint of an outside observer or researcher. Although most researchers understand that culture extends beyond mere descriptions of race or language, they underestimate culture’s role as a determinant of health disparities. 8
People from minority racial groups suffer disproportionate cancer burdens: compared with whites, their disease tends to be diagnosed later, disease severity is greater, treatment options are fewer, and overall outcomes are worse. 9 By 2050, when racial minorities are expected to be in the majority in the United States of America (USA), a 99% increase in cancer rates is expected for these groups, compared with a 31% increase for whites. 9 However, using such aggregated racial data in clinical practice or health research may hide in plain view those most at risk for health disparities. For instance, aggregating all people of color into one ‘African American’ category precludes any attempt to address issues related to the discrete cultural differences and mores of groups within the aggregated group. Cultural inter-group differences can have distinctly different effects on each group’s access to and use of the healthcare system.7, 10 Categorizing individuals by race creates barriers to efficiently and equitably implementing programs for preventing chronic illnesses, such as HPV-related cancers.4, 11, 12 Therefore the authors are utilizing mixed methodologies to assess the knowledge, attitudes, and beliefs of culturally discrete groups of people in rural Georgia. Without recognizing the health-related risks and perceptions of cultural subgroups, we cannot effectively prevent chronic illness or reduce health-related disparities in rural areas, such as that seen in HPV vaccination rates.
Risk perception
Each culture perceives health-related risk through the values assigned by its members to their health-related experiences and knowledge. 13 Consequently, people frequently trust experts from a similar cultural background more than they trust experts from different backgrounds. 13 Cultural values generate differences in risk perception through biased assimilation and perceived credibility. 13 Biased assimilation is the tendency of people to seek out and approve information that confirms their beliefs. Similarly, cultural cognition theory posits that people will choose to accept or reject information on risk in a manner consistent with their cultural values, beliefs, or spirituality. 13 Consequently risk perception runs along discrete cultural lines, and researchers need to understand a target group’s risk perceptions before developing health education or intervention programs for that group.
Our study’s findings substantiate cultural cognitive theory’s position. Beliefs about the HPV vaccine and residents’ intention to vaccinate were different in each of three rural counties in Georgia, and the differences could be explained by variations in risk perception that were attributable to self-identified membership in cultural subgroups. Indeed, a large body of research supports that culture affects risk perception more than education or socioeconomic status, and culture reinforces personal perceptions about race and gender.14, 15 Therefore in order to help assimilate positive primary prevention behaviours, like HPV vaccination, into a cultural subgroup, we posit that health policymakers, researchers, and practitioners must make an effort to genuinely understand and accommodate the risk perception tendency within that cultural subgroup.
Religion and spirituality
Religion and spirituality are major components of the culture of our study’s predominantly African American population. 16 Past research confirmed our current findings that imply that religious African Americans frequently view illness as a punishment from God.4, 17 During our research in rural Georgia, we also found a disconnect between people’s attitudes about faith and healing and their actual faith and healing experiences, a finding that is similar to findings from rural areas of the Midwest. 18 One qualitative investigation of rural African Americans revealed the role of religion in the culture as well as the importance of church, family, turning health problems over to God, and the concept of an individual’s body as a temple of God. 19 However, another study of young African American women attending a historically black university in the rural south showed that self-reported religiosity was not protective against sexual risk taking. 20 The discrepancy between these two studies once again highlights the need to use measures of self-identified culture and ethnicity in order to learn about a study group’s health-related behavior, which could be significantly different from the overly broad behaviour assumed through broad racial categorization without recognition of cultural subgroups. Consequently, although religion is undeniably a major part of many cultures, the lack of consistent evidence found at a high enough level of cultural refinement precludes assuming that all religion-related research findings can be used when developing health-related intervention and education programs for rural communities. For this reason our current lines of research on rural HPV-related cancer prevention are collecting data on the church systems and faith-based capacity of communities unique to each of the rural Georgia counties. This will allow for the timely transition of our research into equitable and efficacious cancer-prevention and health-promotion programmes developed in and tailored to the cultural makeup of each community.
Geography
Geographic distribution of health services plays an important role in access to healthcare, use of healthcare services, distribution of chronic disease, and treatment outcomes. 21 Poor health, chronic illness, long distance to healthcare services, and lack of car ownership all predict an individual’s difficulty in accessing services provided by general practitioners and hospitals. 22 Moreover, geopolitical dynamics and delays mean that once community health centers are built, they may serve distinctly different geographic populations than they were intended to serve when their location was first proposed. Therefore understanding the geographic factors that affect a rural area’s residents is essential to developing equitable and effective tailored health promotion programmes.
Primary care access and availability
Primary care health professional shortage areas (PC-HPSAs) are areas where the number of primary medical and mental health providers is insufficient for the population; these areas are predominantly rural. The health of residents and outcomes of disease in PC-HPSAs are significantly worse than in non-HPSAs. 23 Moreover, health disparities predicated by provider density are deteriorating most rapidly for the most vulnerable of rural individuals: children, adolescents, and older adults. 24 Unfortunately, state-level policy barriers have further entrenched disparities in rural healthcare by preventing nurse practitioners and physician assistants to fill gaps in rural primary care. This policy barrier is particularly profound in the southern US, and narrowing the geographic divide in healthcare is paramount to ensuring that rural communities have unfettered access to basic primary care services, including vaccinations for children and adolescents. 25
The parents we studied in rural Georgia noted their difficulty in accessing primary care services as a barrier to having their children vaccinated against HPV. Most parents in our study area lived in a county with no pediatricians accepting new Medicaid patients and less than one family/general practitioner for every 2000 residents.26, 27 These figures do not account for residents who have the financial resources to travel into neighboring counties for primary care services; however, the average travel distance from the boundary edges of each of the counties in our study to the closest population centre containing a pediatrician or family/general practitioner is greater than the accepted 30-minute reasonable drive time for accessing primary care. 28 Therefore these figures are a sensitive, specific, and disconcerting record of how inaccessible primary healthcare services are for children, adolescents, and adults in rural Georgia. This represents a substantial barrier to obtaining the HPV vaccine for the rural communities in our study area.
Economics
The economics of healthcare in rural areas is grim: residents earn less than their urban counterparts; county public health offices have a smaller annual tax base through which to fund health-related programs; and hospitals and primary care providers have larger numbers of Medicare or Medicaid patients and fewer resources to invest in new health-related technology. 29 These factors preclude focusing on a single economic leverage point for intervention and necessitate developing a more systems-wide solution.
A linked system
The economic situation in rural areas is inexorably linked to the policies that affect rural healthcare services. The hospital conglomerates that formed in the 1980s and 1990s closed many financially untenable rural hospitals, leaving many rural communities, like those in rural Georgia, particularly vulnerable. To respond, the US Congress created the Critical Access Hospital model as a means to help secure the financial viability of small rural hospitals through a cost-based reimbursement program, but federal budget constraints and political dynamics mean the long-term viability of the program is unclear. 29 The closure of a rural community’s hospital due to budgetary constraints has detrimental effects on the community’s local economy and directly impacts rural citizens through the loss of $703 (4%) in a community’s per capita income and a 1.6% increase in the local unemployment rate. 30 The argument for continuing funding for rural community hospitals is further substantiated by evidence from rural Oklahoma that suggests that, for every dollar generated in rural healthcare services, an additional $0.47 is distributed throughout the local economy via indirect business and household spending. 31 Although these numbers are good indicators of the favorable cost–benefit of rural healthcare services, they do not show the true complexity of socioeconomic factors that can perniciously link the health of rural residents to the economic health of their community.
Persistent poverty
There is a dynamic relationship between the health of an area’s economy and the health of individuals living in that area, one dependent upon the other. The relationship between macroeconomic fluctuations and individual health is counter-cyclical for individuals with sufficient access to credit or high pre-recession incomes and pro-cyclical for individuals who lack access to credit or who had low pre-recession incomes. 32 In other words, economic downturns improve the health of the middle and upper classes because they have more time to engage in health-promotion behaviours and they have sufficient access to credit or personal savings to ensure their lifestyle remains healthy. Conversely, economic downturns worsen the health of the low and low-middle classes who do not have sufficient access to credit or personal savings to protect their health from the detrimental effects of diminished or lost income. These adverse effects of poverty are particularly harmful to children, and they can have lasting effects on the child’s health and income as an adult. 33
In the three rural Georgia counties included in our study, 31.7% of the children lived below the poverty line in 2007, immediately before the national economic downturn began. 26 The percentage of children below the poverty line increased and reached 40.8% three years later in 2010, substantially out-pacing the 3.6% increase nationally. 26 This change represents an additional 1080 children living in poverty in these three rural Georgia counties after the first three years of the economic downturn. Given the documented relationship of childhood poverty with adult income and health, the effects of the economic downturn are likely to persist and to affect the long-term health and well-being of the present generation of children in these three rural Georgia counties. 33 The World Health Organization has called for researchers and officials to close socioeconomic-driven health-related gaps, such as this one in rural Georgia, within the next generation in order to mitigate the carryover of disparities from this generation to the next. 34 We are attempting to answer this call in rural Georgia by developing culturally relevant cancer-prevention interventions tailored to the unique social and economic situation within each rural community and county.
Call for leadership and partnerships
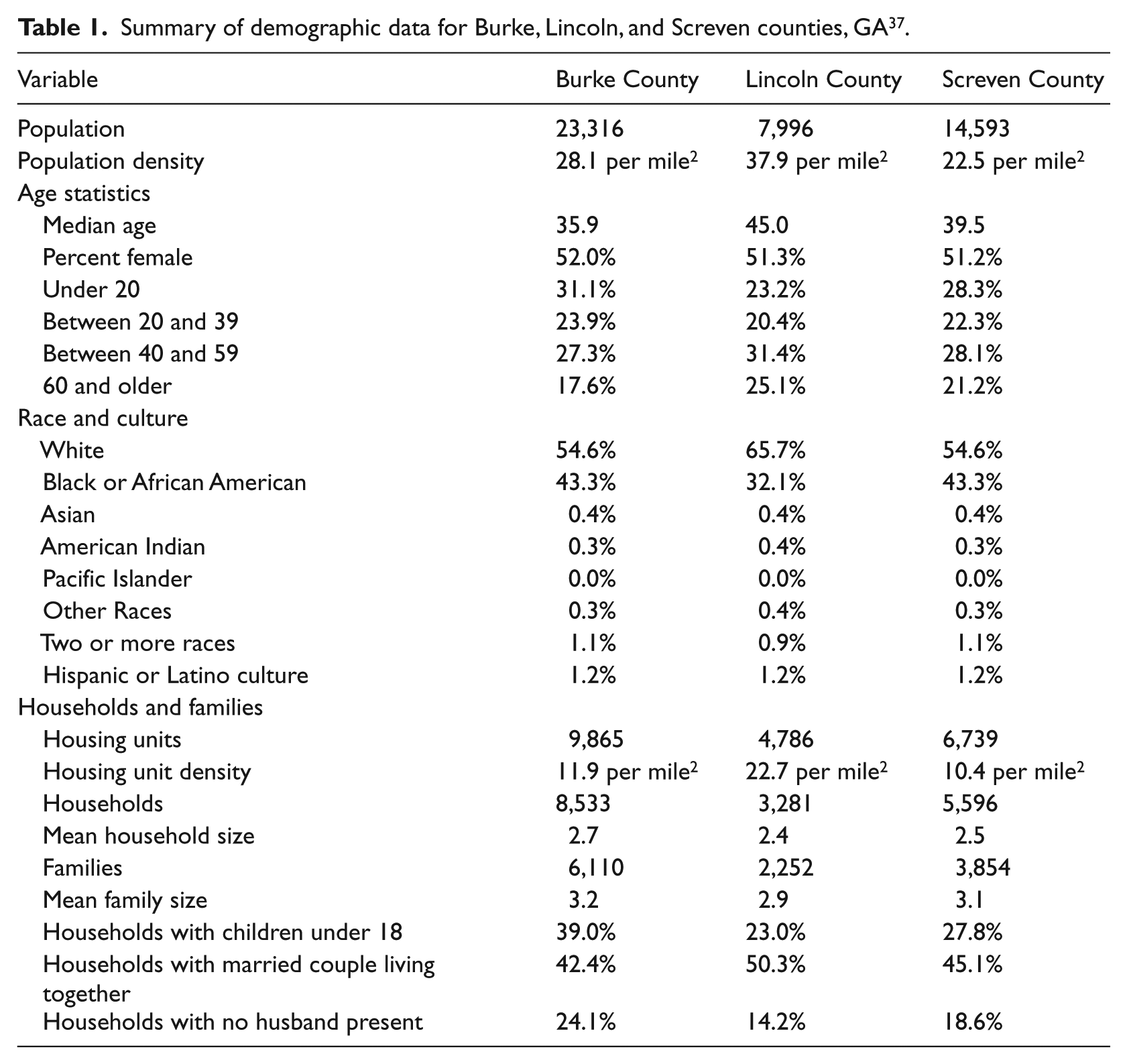
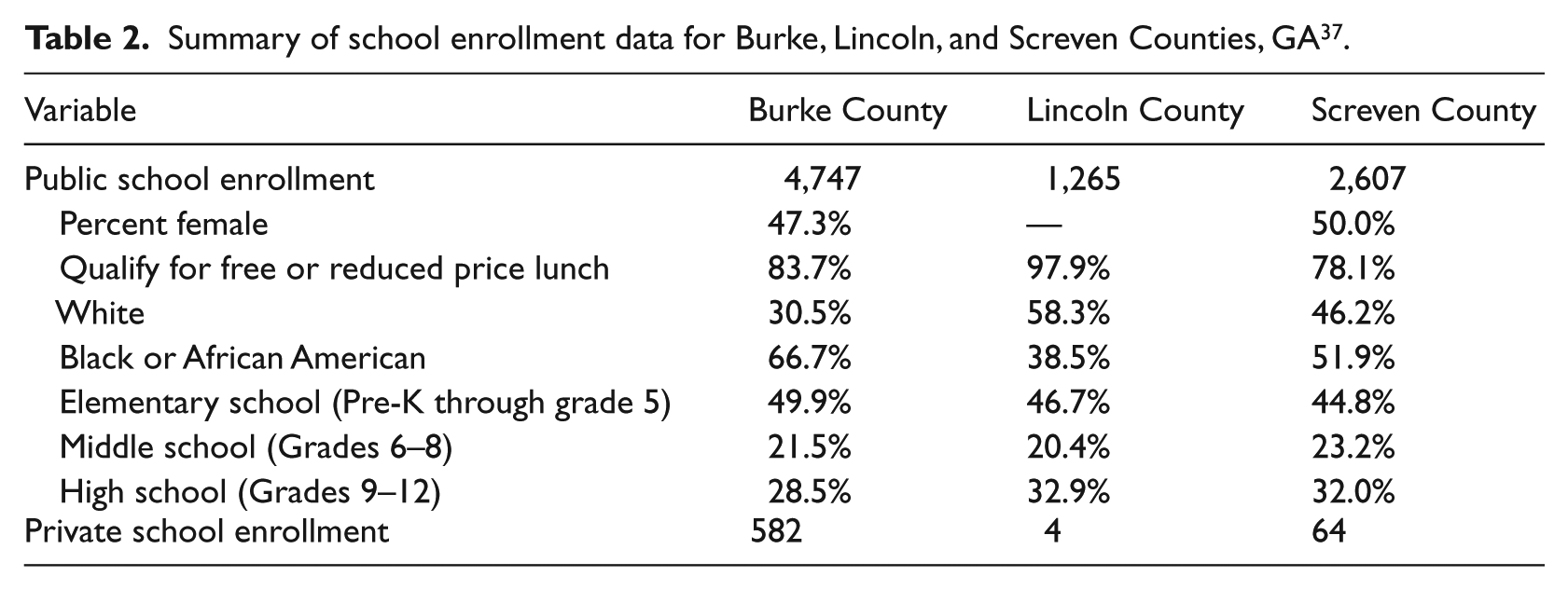
Tables 1 and 2 demonstrate the long road to good health for adolescents who live in the three rural areas in our ongoing studies. These data are representative of rural areas across the US, but the policy and leadership dynamics in the southeast create a scenario that is more likely to beget rural health disparities from generation to generation than it is to prevent them.35, 36
Summary of demographic data for Burke, Lincoln, and Screven counties, GA 37 .
Summary of school enrollment data for Burke, Lincoln, and Screven Counties, GA 37 .
During the past decade, rural policy initiatives began many reforms intended to decrease rural health disparities. 35 For instance, telemedicine programmes were tested as a viable means of extending specialty and subspecialty knowledge to rural areas, but the viability of these is challenged by logistical and billing barriers that rural infrastructure is not always capable of overcoming. Similar challenges found during other tests of changes to rural healthcare systems led policy analysts to call for developing networks that span professional silos and collaborate inter-professionally for the benefit of rural communities. 35
Our work promoting HPV vaccination in rural Georgia has revealed each of the aforementioned promoters of rural health disparities: culture, geography, and economy. While each of the these three elements is capable of producing rural health disparities independent of the other two, they interact in a gestalt triad to produce rural health disparities that are more pernicious than the mere additive effect of all three. Consequently, the authors believe that overcoming this triad of rural health disparities necessitates strong leadership to: (1) ensure that medical coverage is available regardless of an individual’s insurance status or race; (2) create culturally relevant models of health education, diagnosis, treatment, and care in areas with particularly high mortality rates for diseases like cancer; and (3) conduct community-based participatory research to produce results that can be directly translated into innovations for delivering sound healthcare. Through our research in rural Georgia, we hope to equitably translate our findings into the development of culturally relevant cancer prevention interventions, clinical surveys, and health education materials that promote engaging in primary prevention behaviors like HPV vaccination.
Similar collaborative pursuits in areas other than cancer and HPV-related disparities are also needed in order to fully overcome the triad of culture, geography, and economics and close the rural health gap. Leadership is essential to developing innovative initiatives, and programs in Oregon and Maryland are laudable for their efforts to gain community and industry involvement in the development of financially viable and socially necessary integrated partnerships between community-based primary care practices and public-health programs.38, 39
Leadership is also needed in public policy offices as new evidence suggests that, while equitable access to healthcare is socially justified, socioeconomic inequalities in mortality persist even with universal health insurance and access to healthcare early in life. 40 Consequently, researchers, clinicians, and policymakers must seek to forge a collaborative framework for partnerships between social institutions, similar to the authors’ work to partner with faith-based and school-based organizations.
Conclusion
Rural health disparities, along with the barriers to overcoming them, have their roots in the triad of culture, geographic location, and economy of rural communities. Understanding of each individual cultural, geographic, or economic element is necessary, but it is not sufficient unless the compounding effects of all three are also accounted for. Efforts are underway in rural Georgia to respond to this triad through HPV-related education and cancer prevention interventions tailored specifically to the sociocultural, geographic, and economic determinants of the area’s rural health-related disparities. Early responses to recruitment and engagement during our research show promise and the ability to be expanded to other rural communities. Similar leadership and partnerships are necessary in other areas of health in order to equitably close the rural health disparity gap.
Footnotes
Funding
This work was funded in part by the Robert Wood Johnson Foundation (#67983) and the National Institutes of Health and National Institute of Nursing Research (#1R03NRO13558-01).