
Abstract
Objective:
BeweegKuur (Exercise Therapy) is a Dutch lifestyle programme in which participants are referred by a general practitioner (GP) to a lifestyle advisor. To support participants, regional and local alliances are established. The present study explored the successes and challenges associated with collaboration processes in local BeweegKuur alliances.
Design:
A qualitative explorative study.
Setting:
The Netherlands Institute for Sports and Physical Activity (NISB) initiated the Building BeweegKuur Alliances project to support local alliances. The BeweegKuur intervention is implemented by over 30 regional and about 150 local alliances throughout the Netherlands.
Method:
12 in-depth interviews were held with coordinators of the alliances, and four focus groups were held with regional and local alliance partners.
Results:
Collaboration within the alliances is perceived as successful in integrating prevention and care. Challenges include the participation of sectors such as the local municipality and the sports sector, and the transition of BeweegKuur participants to local sports facilities.
Conclusion:
This study identifies three general conditions for successful coordinated action: (a) flexible protocols and management that allow for contextual adaptations; (b) making successes and challenges visible using facilitating methods and tools; and (c) time and funding to overcome differences of culture between different sectors, and to build trust.
Introduction
Over the last decade, so-called combined lifestyle interventions to promote the health of people with overweight and chronic diseases have become commonplace. Combined lifestyle interventions address multiple health issues, such as healthy nutrition and physical exercise, and are often implemented in healthcare settings. 1
BeweegKuur, or Exercise Therapy, is a Dutch example of a combined lifestyle intervention, designed to achieve healthier lifestyles for diabetes and overweight patients. In 2008, the Dutch government commissioned the Netherlands Institute for Sports and Physical Activity (NISB) to develop and coordinate the intervention. In the BeweegKuur, participants are referred by a general practitioner (GP) to a lifestyle advisor – usually a practice nurse or a physiotherapist – who coaches the participant over a one-year period in achieving a healthier lifestyle. Throughout this year, a physiotherapist guides patients to enter an exercise programme, and participants attend individual and group sessions with a dietician.2,3 NISB developed a fixed protocol for the establishment of the BeweegKuur programme, specifying which patients to include and the arrangement of contacts between different caregivers.
BeweegKuur is a multidisciplinary intervention in which collaboration in alliances for integrated care plays a major role. In 2010, NISB initiated the Building BeweegKuur Alliances (BBA) project which aimed to facilitate the 30 regional and 150 local alliances (Figure 1) and to support the building of more alliances. The BBA project consists of training sessions, support by a NISB advisor and funding for regional alliances. The partners in the regional alliances comprise an advisor from each regional support structure for primary healthcare (ROS), a professional from a municipal health service (MHS), and a professional from a sports organization. Regional alliances are tasked with establishing local alliances and supporting them in implementing the BeweegKuur. Local alliances implement the BeweegKuur and guide patients towards local sports facilities. The partners in the local alliances are primary care professionals, e.g. GP, practice nurse, physiotherapist and dietician. In some local alliances, other organizations are represented, such as welfare workers and the municipality. The local alliance is usually coordinated by the lifestyle advisor/practice nurse or the ROS advisor.
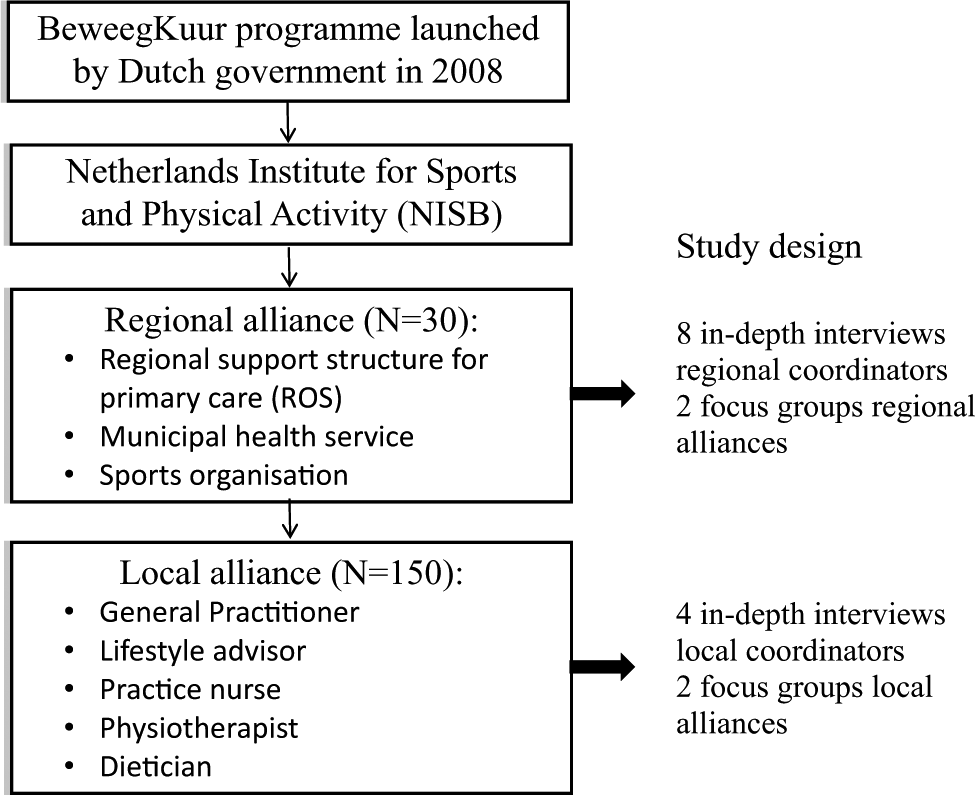
BeweegKuur programme.
To successfully implement BeweegKuur, coordinated action between the health care sector and others sectors such as welfare and sports is essential. However, as Koelen et al. 4 argue, even though working in alliances has many advantages in theory, in practice it involves working with new people, with different backgrounds, knowledge domains, interests and perspectives. For alliances to be successful, they have to deal with these differences. 4 Coordinated action is demanding in terms of effort and time as partners are often not acquainted with one another’s way of working.5–9 In order to provide insight into successes and challenges of collaboration processes, we assessed the functioning of local and regional BeweegKuur alliances so that NISB could use these lessons to improve their support of alliances.
In this study, the concept of coordinated action is used to describe work within the alliances, whereas a coordinated action model (CAM) is used as a framework for assessment. Coordinated action is defined as ‘action in which organizations and clients in two or more sectors work together to jointly achieve an outcome’ [p.i25]. 5 The CAM is based on a review of relevant literature and on lessons learned from a variety of health promotion programmes, and identifies several factors that influence collaboration processes. 5 The model consists of three factors focusing mainly on achieving coordinated action: (a) representation of relevant societal sectors including clients, (b) discussing aims and objectives, (c) discussing roles and responsibilities; and three factors focusing mainly on sustaining coordinated action: (d) communication infrastructures, (e) visibility of contribution and results, and (f) management.
In this paper, the study design and methods are first explained. Second, successes and challenges of collaboration processes in BeweegKuur alliances are described. Finally, the lessons learned about collaboration processes within BeweegKuur alliances are discussed, as well as implications for research and practice on alliances for health more generally.
Methods
Study design
To gain a comprehensive insight into the collaboration processes within BeweegKuur alliances, we conducted a qualitative study, in which in-depth interviews and focus groups were used to complement one an other. Qualitative methods were chosen because they favour involvement and open expression 10 by those who are involved in the BeweegKuur programme at regional and local level.
Study population
Coordinators of regional and local alliances were interviewed. Focus groups were held with all partners of the regional alliances – ROS advisors, representatives of sports organizations, and municipal health services – and all partners of the local alliances – e.g. practice nurses, dieticians and physiotherapists.
Selection and procedure
Alliances participating in this study were recruited by NISB. In total, eight regional and four local alliances were selected by non-probability sampling, 10 while looking for variety in terms of a nationwide spread, composition and duration of the partnership. Using pre-existing groups allows to observe fragments of interactions that approximate natural occurring data. 11 To ensure open communication, in-depth interviews and focus groups were conducted by two independent researchers who had not been involved in the BeweegKuur programme beforehand (AW and LV). The interviews and focus groups were held in October, November, and December 2010. At regional level, eight face-to-face in-depth interviews with coordinators of regional alliances and two focus groups with partners of regional alliances were conducted. At local level, four face-to-face in-depth interviews with the coordinators of local alliances and two focus groups were conducted. The interviewees also participated in the focus groups as the focus groups were held within the same alliance. The in-depth interviews lasted from 45–90 min. The focus groups lasted about one hour. In total, 18 people attended the focus groups, and numbers in the focus groups varied from three to six people. For this study, it appeared that these numbers were sufficient for data saturation.
In-depth interviews and focus groups
The topics addressed in both the in-depth interviews and the focus groups were based on the CAM. 5 In the in-depth interviews, open-ended questions were asked about the role and experiences of the interviewees within the alliance, and the mission, goals and results of the alliance. The questions were formulated following the principles of appreciative inquiry (AI). 12 Positively formulated questions build on strengths and assets of interviewees, thereby stimulating participation in the research activities.12,13 AI has been used successfully in health promotion approaches14,15 and also as an interview tool. 16 Examples of questions include: ‘Can you describe a success gained by the alliance?’ and ‘What will the alliance ideally look like in two years?’.
Information obtained in the in-depth interviews on the specific characteristics of the alliance was used to prepare for the focus groups. In addition, as part of the focus groups, the coordinated action checklist (CAC) was used. 15 The CAC is based on the CAM model and assesses collaboration processes and achievements of the alliance. Items in the CAC are also formulated according to the AI principles, for example: ‘I feel involved in the alliance’. In the focus groups, first, partners were asked to score the 25 items on a five-point scale. The CAC was used to facilitate discussion and dialogue, hence the overall scores have not been calculated. The individual scores were used for probing and sharing opinions and ideas. If action points arose, dealing with them was actively facilitated by the researcher.
Data analysis
The CAM guided the data analysis. The in-depth interviews and focus groups were audiotaped with the permission of the interviewees and the participants, and transcribed afterwards (intelligent verbatim style). The results of the interviews and focus groups were analysed using the qualitative data analysis programme ATLAS.ti (version 6.2) for transparency. An iterative top-down and bottom-up analysis of the in-depth interviews and focus groups was performed, based on a combination of content analysis 17 and domain analysis. 18 The first three authors discussed the coding process for each step, resulting in a clear and complete code list. The content analysis was performed in order to describe perceived successes and challenges of collaboration processes. Next, those successes and challenges were analysed to see how they fitted the CAM. A final step was free coding, providing new factors raised by the alliance partners. Scientific quality was assured by triangulation of data sources (alliance coordinators, alliance partners), multiple methods (in-depth interviews, focus groups) and participant check, as transcribed interviews and a report on the focus groups were fed back to the alliances. 19 Because comparable information was derived from the in-depth interviews and the focus groups, all data were added together in the analysis.
Results
The alliances differ in context, composition, partnership duration (ranging from 1–3 years), and number of partners. In all four local alliances, the BeweegKuur programme was being implemented, usually one or two groups of about 10 participants. However, the overall number of patients entering the BeweegKuur programme was low, resulting in a limited number of BeweegKuur groups. Moreover, from these groups, the flow to local sports facilities was limited as well.
Successes and challenges of collaboration processes in the alliances are presented in terms of the CAM Model (Table 1). In addition, factors that arose during the interviews and focus groups are described. Quotes are used to illustrate the views of interviewees in their own words.
Successes and challenges in coordinated action.
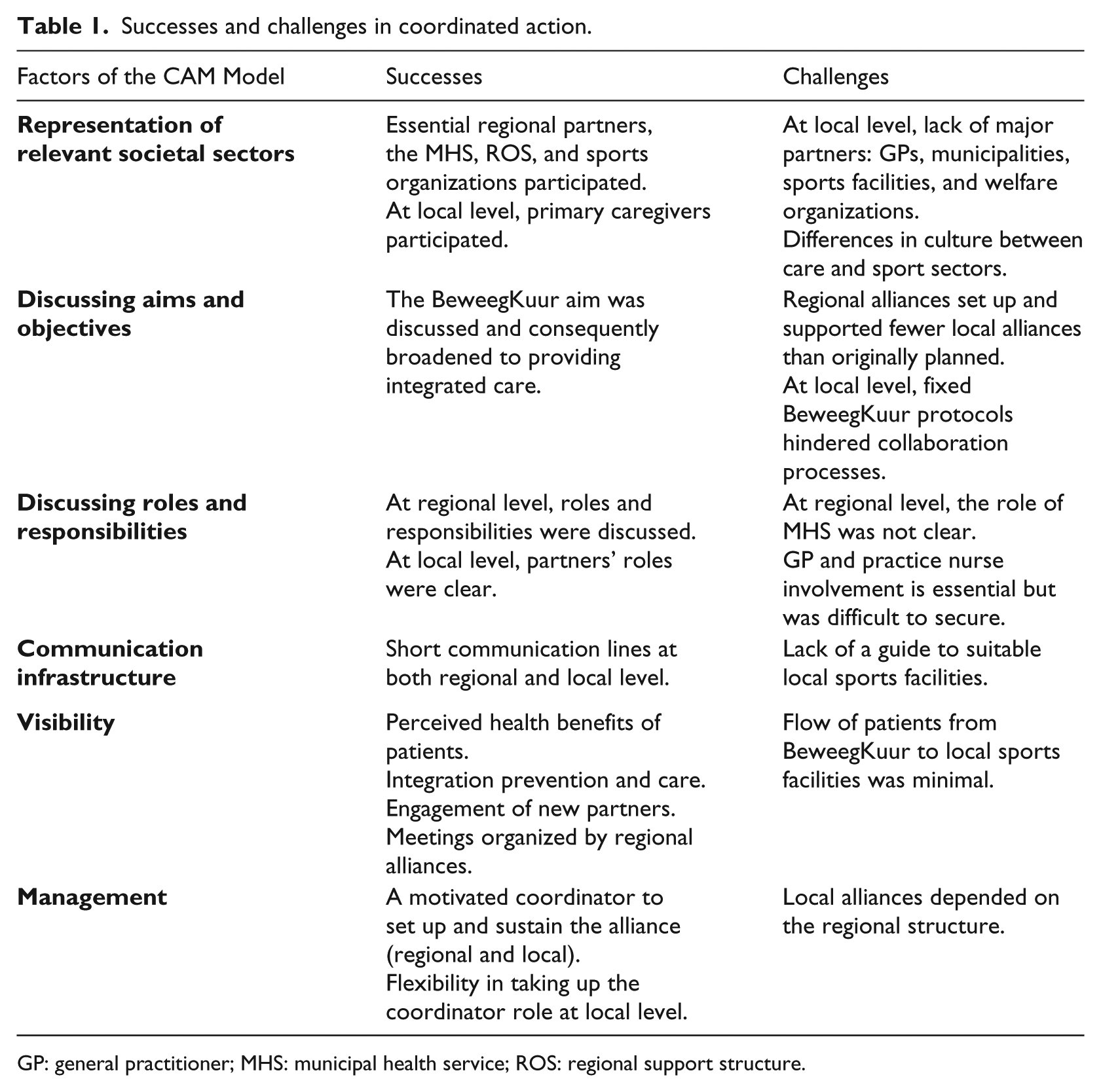
GP: general practitioner; MHS: municipal health service; ROS: regional support structure.
Representation of relevant societal sectors
Interviewees reported that essential partners, the ROS, MHS and sports organizations, participated in all eight regional alliances. At local level, primary care professionals such as practice nurses, dieticians and physiotherapists participated, but there was a lack of major partners like municipalities, welfare organizations, GPs and local sports facilities, who were perceived to be crucial for successful coordinated action. Municipalities, for instance, were seen as crucial for supportive policy and for accessible sports facilities, for example by offering subsidies to BeweegKuur patients. Interviewees indicated that local sports facilities did not participate in the alliances because the care and sports sector have different cultures. For example, the preferred time to meet, by day or in the evening, was different. Also, their target groups differed: primary care patients and members of sports organizations. The sports sector was also not familiar with BeweegKuur participants: comprising obese or overweight people, often in combination with low socio-economic status.
Hardly any action was taken to involve these partners in the alliance because of time constraints. Despite these missing partners, collaboration was perceived as successful in the BeweegKuur programme as alliance work fitted well with the aims of their own profession. The alliance partners brought in their professional expertise and appreciated the input and expertise of other partners.
Discussing aims and objectives
All regional alliances discussed the aim of setting up local BeweegKuur alliances, while also discussing broadening their scope towards the provision of integrated preventive care via the BeweegKuur. This meant that the alliance aim transcended that of the BeweegKuur initiative. Discussing the adoption of broader goals was perceived as a success by the alliances, as prevention became part of care, thereby contributing to better quality of care. The broadened aim was supported and sometimes even required by municipal health policy: If I approach the municipality, they tell me: I do not want to only discuss the BeweegKuur programme with you, I want to discuss also the combined lifestyle interventions. How can we influence citizens’ health by a healthier lifestyle? Interview, ROS advisor regional alliance
Regional alliances were required to develop local alliances in order to achieve the mandatory number of 3000 locations in 2012 as set by NISB. However, the alliance partners often considered this requirement unachievable because of limited time and human capital being paid for by NISB.
In the first meeting, we bickered a lot about the hours. And I got back to NISB about that to discuss whose regular task it is. Focus group, ROS advisor regional alliance
At local level, aims were not discussed as the aims had been set in the BeweegKuur protocol. However, the fixed protocol sometimes hindered joint discussion and the development of aims and objectives, especially in local alliances where collaboration was already successful. The protocol was perceived as too strict in the sense that the division of labour between primary care professionals and the number of consultations with patients were fixed, and the protocol was perceived as too time-consuming because of administrative aspects: We try to organize it effectively, and then you clash against it as our hands are tied. Interview, Physiotherapist/lifestyle advisor local alliance
Discussing roles and responsibilities
At regional level, roles and responsibilities of the ROS and Sports Service were clear. The role of the MHS in the alliance was not always clear to partners, except that the MHS was involved in health policy in the municipalities: In my opinion, the role of the MHS is still not clear. What exactly is the role of the MHS and what role had NISB intended for them. And I notice that they also themselves cannot make their role clear. Interview, ROS advisor regional alliance
At local level, partners’ roles were clear as prescribed by the BeweegKuur protocol. The tasks related to the expertise and profession of the partners. Practice nurses often participated in the programme as so-called lifestyle advisors but faced time constraints. The role of GPs was experienced as both crucial and hard to secure – crucial because GPs referred patients to the BeweegKuur programme – difficult to achieve because GPs had limited time.
The overall number of patients referred to the BeweegKuur by GPs was low. The BeweegKuur programme was perceived by them as an extra task without an extra allowance. Partners argued that GPs were not aware of the effects of the BeweegKuur programme and needed to be convinced of this: My opinion is that it is especially important that a GP joins the alliance. We really enjoy this since this forms the basis. Interview, physiotherapist local alliance
Communication infrastructure
Short communication lines were reported as a major success factor in both regional and local alliances. Short lines of communication facilitated care of patients by multiple professionals. Personal encounters established those communication lines and facilitated further contact by phone or e-mail: With both practice nurses I have contact via e-mail and telephone, and once in a couple of weeks I personally meet to check all data of patients (….) and that sort of issue. That works out perfectly; we have a fixed time for meetings. Interview, physiotherapist local alliance
Additionally, other personal encounters facilitated and motivated partners: I met the two ladies [at the NISB course], the acting representatives. So that was an ideal timing. We travelled together to the course for two days in the car. A good start was made. Interview, ROS advisor regional alliance
According to partners, a guide that listed available and suitable local sports facilities might help to increase the flow of patients. All alliances prioritised the development and updating of such a guide.
Visibility
The main successes perceived were the actual health benefits for patients and the integration of prevention and care. Perceived health benefits for patients, such as weight reduction, increase in physical activity and reduction in medicine intake, strongly motivated partners: What I enjoy is that I see that people change, that it really has an impact. I didn’t expect that. For example, there is a lady whose weight has gone down by 12 kilos. She says that her personality has changed because she looks different now. That she is more assertive, that her lifestyle completely changed, that she is more confident in herself. Interview, physiotherapist local alliance
The integration of prevention and care was also seen as being facilitated by the BeweegKuur: What I like is that prevention is going to be more part of the care sector. Thus, that I notice that caregivers make that move. They really want to offer something to the people. People who are really struggling with overweight and so on. Interview, ROS advisor regional alliance
Other successes were achieved, such as the engagement of new partners such as sports organizations and an increase in the number of meetings with those partners. These successes also motivated partners because they reflected their efforts or, in the words of one partner ‘bear fruit.’ In one alliance, the engagement of an enthusiastic professional from a municipality was seen as a milestone.
A major barrier was the limited flow of patients from primary care to local sports facilities. According to partners, personal guidance from primary care professionals and close connections between primary caregivers and local sports facilities could have helped to increase the future flow of patients.
The contacts with local sports facilities should be more intensive. I have personal contacts with aqua- fitness and a walking group, but it should broaden. It is desirable that more thought should be put into what to offer so that it becomes more accessible and affordable. Interview, physiotherapist local alliance
Management
The formally organized regional alliances required management to structure the collaboration process. It was frequently discussed who should manage the alliance, mainly in terms of the future perspective on collaboration and lack of funding. In both regional and local alliances, ROS advisors fulfilled a crucial coordinating role, as initially was allocated by NISB, although many partners were convinced that this role also could be fulfilled by the MHS. However, NISB’s aim was that in time local alliances would coordinate themselves. Local alliances to date were strongly dependent on the ROS advisors for coordination, and it was a challenge to share responsibilities.
When you have organised a starting meeting, and actually you hope that they will take it over themselves because you cannot stay to coach everyone. Meanwhile you notice – when leaving such a meeting – that you are thinking ‘If I don’t do anything now, tomorrow the world has not changed’. Interview, ROS advisor regional alliance
At local level, interviewees expressed the need for an enthusiastic coordinator or linchpin.
But that function – the linchpin function – I have the idea that it is more here. And then, to connect the partners, to take care that issues that arise and do not run smoothly get discussed and that actions for improvement are taken. How do you call that role, actually a bit of a management role, or not? Interview, physiotherapist/lifestyle advisor local alliance
In practice, who fulfilled this role depended more on available time and ambition than on profession. Practice nurses in particular, but also physiotherapists or dieticians, were perceived as being well placed to take on this role.
Emerging factors
In addition to the coordinated action factors, funding and time appeared to be important factors. First, uncertainty about funding hampered the development of alliances. Alliance development was stimulated by the budget made available by NISB to pay for human resources. Uncertainty about whether patients’ health insurers would cover the cost of participating in the BeweegKuur programme and lack of clarity about subsidies for coordinated action hampered the development of alliances. The recruitment of new partners, such as primary caregivers and representatives of local sports facilities was no longer seen as relevant, as payment for human resources came to an end. Regional alliances chose to optimally support fewer local alliances than planned. Second, more time than originally planned was needed to develop alliances. Having enough time was key to the development of trust among alliance partners and for the planning and implementation of the BeweegKuur programme.
Discussion
This study set out to assess successes and challenges of collaboration processes in BeweegKuur alliances. In-depth interviews and focus groups based on the CAM model provided insight into the main factors promoting and hindering collaboration around the programme. Findings suggest firstly that the representation of relevant sectors at local level was restricted to a relatively small group of primary caregivers. Secondly, discussion about aims supported coordinated action and resulted in broadening the alliance aim from implementing BeweegKuur to providing integrated care. At local level, collaboration may be hindered by fixed protocols as alliances needed flexibility to implement according to their own needs and context. Most partner roles were clear. However, at the local level the involvement of the GP and practice nurse may be difficult to secure, resulting in a limited number of patients referred to the BeweegKuur programme. Communication infrastructure was facilitated by the presence of relatively short lines of communication and personal contact. A visible factor was the perceived health benefits for patients. However, the flow of patients into local sports facilities overall was minimal. A management structure is required, but coordination need not necessarily be fulfilled by the ROS advisor.
Overall, collaboration within the alliances was perceived to be successful in integrating prevention and care. However, the participation of other key sectors, such as the local municipality and the sports sector, was a major challenge. Collaboration with the sports sector is relatively new in health promotion, but it is seen as an important area to focus on. 20 In the areas of professional sports 21 and development, 22 success in enhancing physical activity in specific populations has been achieved. Our results indicate that personal contact often helps to establish collaboration. Also, a list of available local sports facilities may be useful, as is underlined in another BeweegKuur study. 3 Differences in culture between care and sport are a major challenge for collaboration, particularly given differing organizational values and focus areas 23 and different target groups (primary care patients, members of sports organizations).
Alliances do not develop just because they are needed. They have to be initiated and built, and several conditions have to be met to sustain them. 4 Based on our results, we see three general conditions for successful coordinated action in the domain of prevention, care and sport: (a) flexible protocols and management; (b) making successes and challenges visible; and (c) time and funding.
Our results indicate that alliances perceived the BeweegKuur protocol as too strict and as hindering collaboration. The protocol is part of the BeweegKuur programme, which is certified as being theory and evidence based.2,24 However, such a top-down protocol does not fit easily with practice, as professionals need to be able to develop a programme using their own insights, local needs and context. 25 Health promotion professionals prefer pre-packaged interventions that are adaptable because the appropriateness of an intervention depends on the specific situation. 26 With regard to management arrangements, similar considerations apply. Professionals allocated coordination and management roles in the BeweegKuur programme were not obvious for alliance partners. Successful management depends more on personal factors such as enthusiasm than on profession. An effective alliance requires sustained engaged leadership. Preferably, there is a leadership style that stimulates participation, 4 that addresses incentive management and which is task-focused. 27
The alliances in our study perceived many successes and challenges just by doing and learning. An important success lay in the fact that the BeweegKuur alliances achieved integration of prevention and primary care. As a consequence, the alliances broadened their aims from implementing the BeweegKuur to providing integrated care. Integrated care should lead to better health outcomes 28 and higher caregiver and patient satisfaction 29 and seems to have positive effects on the quality of care. 30
Funding and time appeared to be preconditions for building trust among alliance partners, overcoming differences of culture, and planning and implementing the BeweegKuur programme. It is recommended to add the factors ‘time’ and ‘funding’ to the CAM model. This is in line with results from other studies: available funding,23,27,31–36 time to build trust, 37 staff time 27 and time to meet and network, 31 all contribute to coordinated action.
A number of limitations of the study have to be addressed: a limited number of alliances – especially local ones – were focused on in this investigation. However, the overall reliability of the study is supported by the emergence of similar results from different methods. Information from the in-depth interviews was confirmed in the focus groups, for example the notion that important partners were absent from the local alliances. The risk of a social desirability effect is always present in focus groups, but possibly limited here since we used pre-existing groups. According to Kitzinger, 11 participants in pre-existing groups are more likely to challenge each other on contradictions in what they say and in what actually happens. Follow-up research might usefully monitor alliances over time to evaluate their sustainability, the results of coordinated action on health outcomes, caregiver and patient satisfaction, quality of care, and the connection between the care and sports sectors to ensure a continued flow of BeweegKuur patients into local sports facilities.
As mentioned earlier, questions for the interviews and focus groups were formulated following the principles of appreciative inquiry. This is a strengths-based approach, useful to uncover strengths and successes but our study shows, in line with other studies, that AI also illuminates challenges.14–16 Additionally, it should be noted that in applying AI principles the focus was more on the ‘discover’ and ‘dream’ phases of work, and less on the ‘design’ and ‘deliver’ phases. This was in line with the aim of the study, i.e. to provide insight into the successes and challenges of the collaboration involved in BeweegKuur alliances.
Conclusion
Overall, our findings suggest that effective regional and local alliances can offer an infrastructure for the integration of primary care, prevention and (to a certain degree) sport, and that working in alliances for health clearly offers added value in terms of quality of care. General conditions for successful coordinated action in the domain of prevention, care and sport include flexible protocols and forms of management that allow for contextual adaptations, making successes and challenges visible by just doing it, and using facilitating methods and tools and time and funding to overcome differences in organizational culture and to build trust.
Footnotes
Funding
The authors would like to thank the Dutch Ministry of Health, Welfare and Sports (VWS) for its financial support and all alliance partners who participated in interviews and focus groups. The BeweegKuur programme was executed by NISB, and the research on collaboration processes around the BeweegKuur was conducted by Wageningen University, which is an external programme partner.