
Abstract
Objectives:
To conduct a systematic review of effectiveness, and barriers and facilitators, of initial teacher training to promote health and well-being in schools.
Design:
Systematic review of the literature.
Method:
A total of 20 bibliographic databases were searched, including MEDLINE, EMBASE and the Social Science Citation Index. Studies were included if they reported research into the processes and/or outcomes of initial (pre-service) teacher training to promote health.
Results:
A total of 20 studies met the inclusion criteria, mainly from the UK and Australia. Twelve studies assessed outcomes, commonly using uncontrolled before and after assessment designs. Sixteen studies evaluated the processes of training. Training was diverse in terms of content, format and health topics. The studies demonstrated short-term increases in trainee teachers’ factual knowledge of health issues, a general increase in teachers’ confidence to teach about health and to identify and help children with specific health issues. There was an increase in teachers’ positive beliefs about their role in promoting children’s health. None of the studies assessed changes in pupil outcomes. The training was generally considered acceptable and adequate by trainee teachers. However, some of the trainees felt that they still lacked knowledge and confidence to address sensitive health issues on entering teaching practice.
Conclusion:
This systematic review identified some evidence for the effectiveness of teacher training for health and highlighted factors which facilitate and inhibit effective training. Further evaluation, using controlled trial designs with long-term follow-up of teacher and pupil outcomes, may enable teachers to effectively address the health and education needs of school pupils.
Introduction
Teachers play an increasingly important role in the wider public health workforce. Over many years, English government policy (Department for Education and Skills, 2004) and nationally supported initiatives such as the National Healthy Schools Programme (Warwick et al., 2005) provided leadership to emphasise the important contribution that teachers and others have in promoting health in schools and opportunities for teachers to develop their skills in this area. Despite the current low policy profile of healthy schools’ work, current legislative frameworks nonetheless require schools to promote the spiritual, moral, cultural, mental and physical development of pupils and prepare them for the opportunities, responsibilities and experiences of later life.
Within the English school curriculum, issues relating to health and well-being are addressed in a number of ways, including through Personal, Social, Health and Economic (PSHE) education; spiritual, moral, social and cultural education; science; and physical education (Department for Education, 2013; Hayman, 2014). In Australian schools, health is covered in the Health and Physical Education curriculum. Beyond the curriculum itself, teachers’ health-promoting role includes safeguarding, pastoral care and participation in whole-school approaches to health.
While it has been recommended that PSHE education becomes a statutory curriculum topic in England (Macdonald, 2009), the nature of its provision remains at the discretion of the individual school, and a recent assessment of the quality of provision by the English inspector and regulator of schools, Ofsted, has found it to be variable and in some cases of poor standard, with a third of teachers inadequately trained to teach the subject (Office for Standards in Education Children’s Services and Skills, 2013). Ofsted recommended that all initial teacher training (ITT) courses include subject-specific PSHE education training.
Subsequently, evidence-based guidance to support schools in promoting health has been produced, reinforcing the need for teaching through the PSHE curriculum-specific aspects of physical and mental health (Public Health England, 2015) and the connections between pupil health and well-being and educational attainment (Public Health England, 2014). Current provision in England is therefore mixed, with policies supporting whole-school approaches to health and the provision of subject-specific health education, but little in-service support to developing health promotion in schools. Thus, the role of ITT in developing knowledge and skills in trainee and early career teachers to meet these expectations is all the greater.
In the UK and elsewhere, ITT can be provided by higher education institutions at under-graduate and postgraduate level, with courses comprising a mixture of college-based training and school-based practice teaching experience. In England, it has become common for teachers to train in schools as part of school-based teacher training programmes (e.g. School Direct). Evidence of effective training approaches may help ITT providers to plan and deliver training that equips trainee teachers with the knowledge, skills and motivation to promote health.
There is a large international evidence base on the effectiveness of school-based health promotion (Bonell et al., 2013; Langford et al., 2014; Stewart-Brown, 2006). However, there has been no published comprehensive systematic review specifically of teacher training to promote health and well-being in schools, to characterise the types of approaches used and their effectiveness, and factors facilitating or limiting their implementation. Such a review would enable recommendations to be made to ITT providers and other stakeholders on effective approaches to teacher training.
The aim of this study, therefore, was to conduct a systematic review of ITT to promote health, to answer three questions:
In what ways does ITT prepare teachers to promote health and well-being in schools?
How effective are interventions to train and support teachers to promote health and well-being?
What are the barriers to, and facilitators of, effective training?
Effectiveness is assessed in terms of changes in factors such as teachers’ knowledge, confidence, skills and ability to address health and well-being in schools, and changes in pupils’ health-related knowledge, attitudes, intentions, skills, behaviour and health.
Health and well-being are two distinct but overlapping concepts. This research adopts a broad definition of the promotion of health, drawing on established models which incorporate educational, organisational, economic and environmental support conducive to health. Specific health issues include any of those that are relevant to children and young people (e.g. sex education, mental and emotional health, drugs, alcohol) as well as broader health-related aspects (e.g. life skills training, youth development, safeguarding and child protection). Well-being can be defined in various ways, but broadly relates to the quality of people’s lives, incorporating physical, emotional, social, psychological and material constructs. Taken together, health and well-being provide a comprehensive framework within which to assess how teachers and schools address the needs of the ‘whole child’.
Methods
The review comprised two stages: (1) a systematic search and descriptive map of the characteristics of teacher training studies (both initial training and continuing professional development), and (2) systematic detailed synthesis of the results of a sub-set of studies prioritised from the descriptive map, focusing specifically on ITT (Shepherd et al., 2013). This paper reports on the systematic detailed synthesis.
A highly sensitive search strategy was devised and tested on MEDLINE by an experienced information specialist. A total of 20 bibliographic databases were searched, including MEDLINE and MEDLINE In-Process, EMBASE, the Cochrane Library, the Campbell Library, CINAHL, PsycINFO, Social Science Citation Index and Education Resources Information Centre (ERIC). Databases were searched from their inception to April/May 2011. No language restrictions were applied.
To be included in the review, references had to report all of the following:
A focus on health and well-being within schools (any aspect of pupils’ or teachers’ health and well-being, but excluding pupils’ existing illnesses);
The initial training of teachers to promote health and well-being in schools (i.e. pre-qualification);
Research into the processes and/or outcomes of (2): Intervention evaluations (any design); Non-intervention research (e.g. interviews; focus groups);
Publication after 1990.
Titles and abstracts were screened according to these criteria by one researcher, and a random 10% sample independently screened by a second. All full papers retrieved for further inspection were screened by one researcher and checked by a second.
Studies meeting the inclusion criteria for the synthesis underwent data extraction using a template designed and piloted for this study. The methodological quality and risk of bias of the studies were assessed using published criteria (Cochrane Effective Practice Organisation of Care Group, 2013; Harden and Gough, 2012). Data were extracted and quality assessment criteria applied by one reviewer and checked by a second.
Study details were tabulated and described narratively. Meta-analysis to assess the effects of training was not possible due to the heterogeneity in the design of the studies and types of training evaluated. To assess barriers and facilitators, a thematic analysis of the process evaluation data was conducted, similar to methodology described by Thomas and Harden (2008). We classified the process evaluation findings according to six pre-defined categories that encapsulate the range of processes that could be assessed (e.g. how acceptable the training was to the recipients). These were then analysed to identify overall themes within the findings.
Results
Characteristics of the studies
The literature search generated a total of 16,620 unique references. After an initial screening of titles and abstracts, full publications of a total of 1,050 (6%) references were retrieved for further screening. Of these, a total of 20 studies reported in a total of 21 publications were included.
The highest percentage of studies were conducted in the UK (n = 9 studies; 45%), followed by Australia (n = 7 studies; 35%). The studies tended to focus on one or two health topics, although a few studies had a broader focus on health in general. Mental and emotional health was a commonly studied area (n = 7 studies; 35%), as was child protection (n = 5 studies; 25%) (Table 1).
Overview of the key study characteristics.

BEd: Bachelor of Education; NQTs: newly qualified teachers; PGCE: Postgraduate Certificate in Education; SRE: sex and relationships education; SCITT: school-centred initial teacher training.
Participants in the majority of studies were pre-service teachers mainly enrolled in postgraduate primary and secondary teaching qualification courses at colleges and universities. In some studies, the teachers had qualified and entered service and were being assessed in relation to the health training they had previously received (Bostock et al., 2010; Cleave and Charlton, 1997; Evans and Evans, 2007; Rossato and Brackenridge, 2009; Weatherby-Fell and Vincent, 2005).
In terms of assessing the ways in which ITT prepares teachers to promote health and well-being in schools (research question 1), the review identified a variable picture. Across the studies, training was diverse in terms of content and was delivered through a variety of formats (e.g. lectures, practical activities). A key aspect of the training courses was the provision of factual information about health, in 15 (75%) of the studies, although the comprehensiveness of the information, as reported by the study authors, varied. In all, 14 (70%) studies were classified as teaching skills that would enable teachers to promote health (e.g. skills for teaching about health and how to develop pupils’ understanding of health and well-being). Training was generally multi-format, comprising lectures/seminars with group work involving discussion or specific tasks. There were five (25%) studies in which teachers had the opportunity to teach health in schools as part of their training (Baginsky and Macpherson, 2005; Chifunyise et al., 2002; Mead, 2004; Taylor et al., 2008; Thomas and Jones, 2005). The duration of training varied from up to 3 hours (Hodgkinson and Baginsky, 2000) to over two school terms with follow-up teaching practice over 2–3 years (Chifunyise et al., 2002). In general, the studies lasted less than an academic year.
Twelve studies (60%) measured outcomes (effectiveness) of training (Table 1). Teacher outcomes were measured in all of these studies, and no studies reported pupil outcomes. Sixteen (80%) of the studies evaluated the processes of teacher training. Eight (40%) studies measured both outcomes and processes. The sample size of the studies varied considerably from less than 10 to around 1,500 participants, with majority including up to 100 participants (Table 1).
The studies varied in terms of their evaluation design (Table 1). In terms of the 12 studies that reported outcomes, the most commonly classified design was an uncontrolled before and after assessment of training in a cohort of teachers (Bostock et al., 2010; Chifunyise et al., 2002; Cleave and Charlton, 1997; Myers-Clack and Christopher, 2001; Speller et al., 2010; Thomas and Jones, 2005; Vincent et al., 2005). The risk of bias of the outcome evaluations was generally high due to lack of control/comparison groups.
The 16 studies reporting processes were judged in terms of their ‘weight of evidence’. The majority (n = 10) were judged medium or high in reliability and/or usefulness of findings (Table 2). Three studies were judged high on either reliability and/or usefulness (Athanases and Larrabee, 2003; Paakkari et al., 2010b; Taylor et al., 2008).
Weight of evidence judgements for reliability and usefulness of findings (process evaluations).
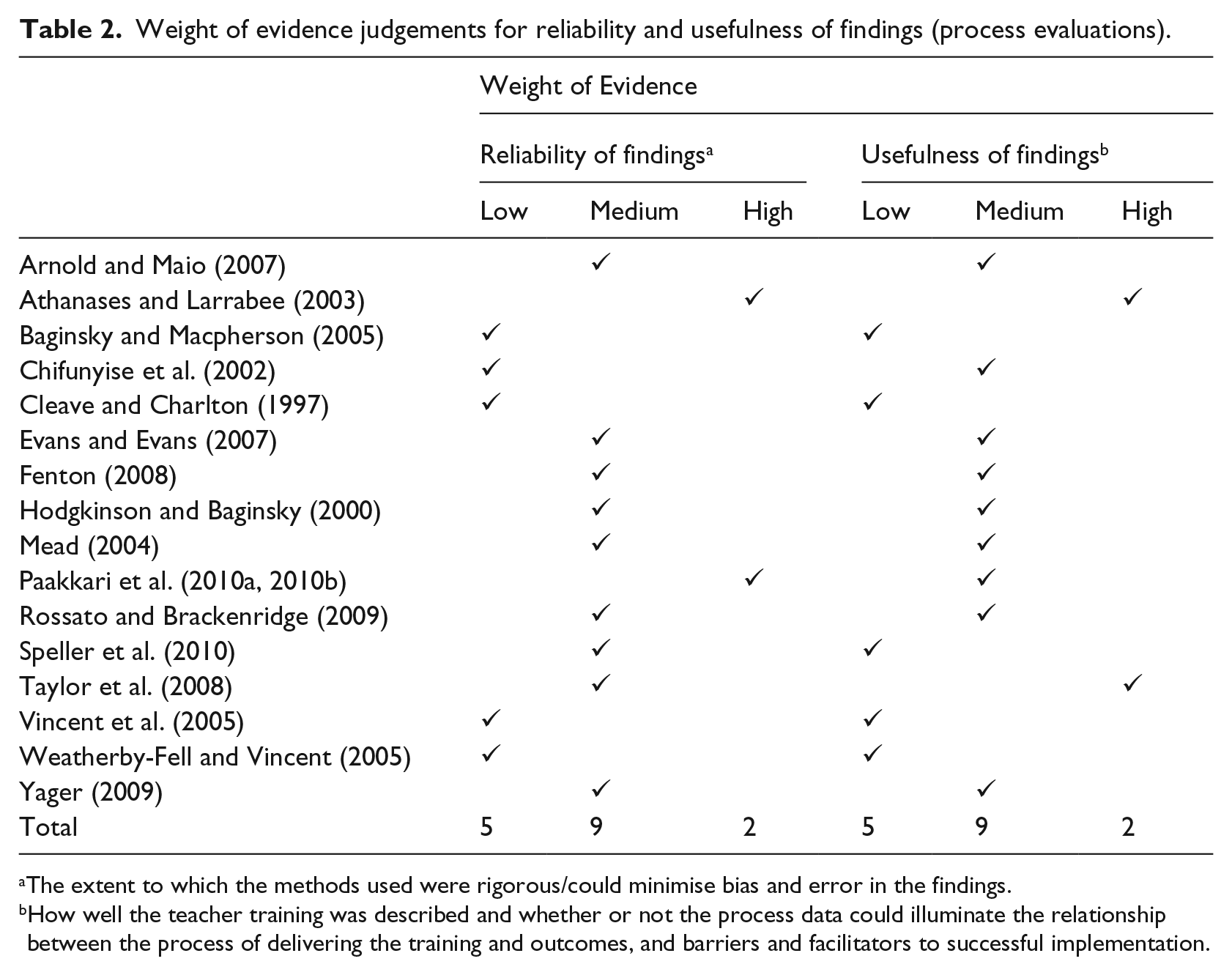
The extent to which the methods used were rigorous/could minimise bias and error in the findings.
How well the teacher training was described and whether or not the process data could illuminate the relationship between the process of delivering the training and outcomes, and barriers and facilitators to successful implementation.
Outcomes of teacher training
In terms of assessing the effectiveness of teacher training (research question 2), the studies measured outcomes in a variety of ways, and results were not always confirmed by statistical tests. The studies demonstrated some increases in trainee teachers’ factual knowledge of health issues following training, in areas as varied as HIV/AIDS (Chifunyise et al., 2002), healthy eating and physical activity (Speller et al., 2010), mental health (Bostock et al., 2010; Vincent et al., 2005; Weatherby-Fell and Kean, 2004), health aspects of PSHE education (Thomas and Jones, 2005) and diversity (Athanases and Larrabee, 2003).
There was a reported increase in teachers’ confidence in relation to teaching PSHE education (Paakkari et al., 2010b) and in identifying and helping children with mental health problems (Bostock et al., 2010; Vincent et al., 2005; Weatherby-Fell and Vincent, 2005) or child protection (Baginsky and Macpherson, 2005). Likewise, there was an increase in teachers’ positive beliefs about their role and that of schools in promoting child health (Athanases and Larrabee, 2003; Bostock et al., 2010; Chifunyise et al., 2002; Myers-Clack and Christopher, 2001; Speller et al., 2010; Vincent et al., 2005; Weatherby-Fell and Kean, 2004), including tentative evidence for beliefs about the relationship between good health and effective learning (Weatherby-Fell and Vincent, 2005).
Processes of teacher training
Figure 1 shows the six pre-defined process evaluation categories, on the left-hand side, to which the results of the studies were classified. Analysis identified eight themes that encapsulated the findings, shown on the right-hand side. Selected key themes and the barriers and facilitators to health training in ITT (research question 3) that can be inferred from these findings are presented next.
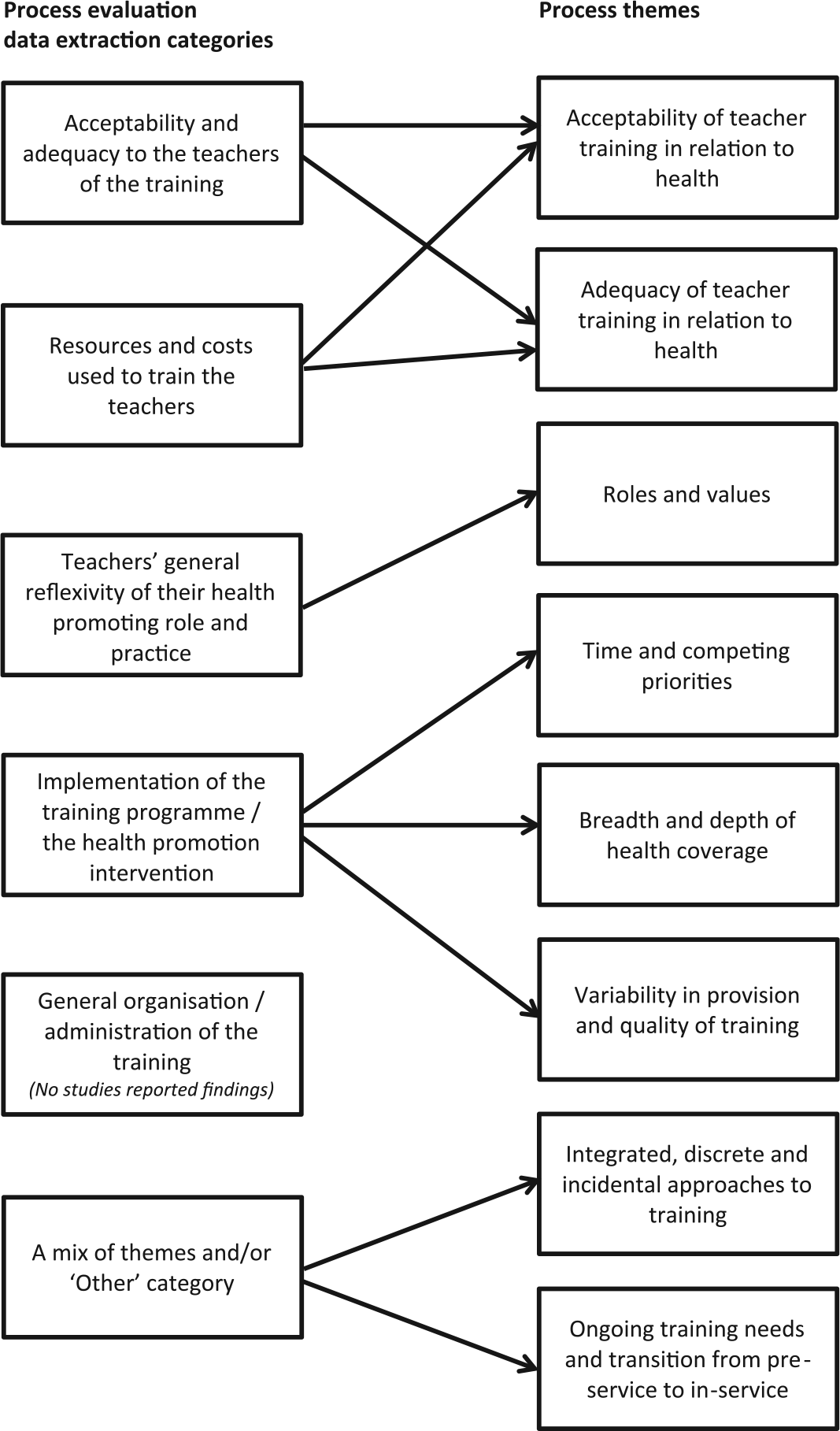
Themes arising from analysis of process evaluations.
Acceptability of teacher training in relation to health
Eight studies reported findings on trainee teachers’ and training providers’ perceptions of the acceptability of the training in health they had received or delivered (Athanases and Larrabee, 2003; Chifunyise et al., 2002; Cleave and Charlton, 1997; Evans and Evans, 2007; Fenton, 2008; Vincent et al., 2005; Weatherby-Fell and Vincent, 2005; Yager, 2009). Acceptability was considered in terms of how the content, format and delivery of the training was considered appealing, enjoyable, meaningful and matched the values and beliefs of the recipients.
These studies reported on the perceived acceptability of the training overall (Athanases and Larrabee, 2003; Chifunyise et al., 2002; Cleave and Charlton, 1997; Evans and Evans, 2007; Weatherby-Fell and Vincent, 2005; Yager, 2009) and the resources used to deliver the training (Fenton, 2008; Vincent et al., 2005; Yager, 2009). In the main, the training was considered acceptable and was well received by trainee teachers.
However, one study, Athanases and Larrabee (2003), reported that a minority of trainee teachers had difficulty reconciling the topic under discussion (sexuality and diversity) with their religious beliefs. The findings of this study, along with those of Chifunyise et al. (2002) who evaluated a HIV prevention training programme in Zimbabwe, however, also highlighted that the creation of a non-threatening atmosphere was helpful for trainee teachers to discuss these sensitive topics.
Adequacy of teacher training in relation to health
There was variability in trainee teachers’ views of the adequacy of the training they had received. Two studies (Cleave and Charlton, 1997; Evans and Evans, 2007) suggested that postgraduate trainee teachers (along with newly qualified teachers in one of the studies (Cleave and Charlton, 1997)) were generally positive that the training they had received in communication skills for working with children experiencing cancer in their lives (Cleave and Charlton, 1997) and in incorporating PSHE education into their English teaching (Evans and Evans, 2007) had met their needs. However, after training, some of the trainee teachers felt that they still lacked knowledge and that further knowledge-based input would have been useful (Evans and Evans, 2007). Other authors reported that, after receiving training in PSHE education (Evans and Evans, 2007), child protection (Baginsky and Macpherson, 2005; Fenton, 2008; Hodgkinson and Baginsky, 2000; Rossato and Brackenridge, 2009), sexual diversity (Athanases and Larrabee, 2003) and mental and emotional health (Taylor et al., 2008), some trainee teachers had on-going concerns about their ability to teach health and to deal with sensitive issues in practice.
Six studies reported that trainee teachers felt that more practical experience of teaching PSHE education (Evans and Evans, 2007) or training in practical strategies for dealing with issues, such as pupil well-being (Taylor et al., 2008; Weatherby-Fell and Vincent, 2005) and child protection (Baginsky and Macpherson, 2005; Fenton, 2008; Rossato and Brackenridge, 2009), would have been useful in the training they received or in their future training. However, in two studies some trainees believed that while training was helpful, they would learn better from their own experience once they were working within schools (Evans and Evans, 2007; Taylor et al., 2008).
Findings from two studies (Athanases and Larrabee, 2003; Fenton, 2008) suggest that it is important for the content and delivery of training to engage trainee teachers on a personal level. Three studies also suggested that in some cases training did not fully meet teachers’ needs as they felt that the delivery methods needed to be more personally relevant, in terms of addressing different levels of teaching experience within the group (Fenton, 2008), previous training experience (Baginsky and Macpherson, 2005) and age (for mature students) (Yager, 2009).
Roles and values
There were mixed findings across the studies about the extent to which trainees assimilated responsibility for health into their roles as teachers and on their understanding about their role as health promoters. Three studies reported limits to the degree with which trainees accepted a health-promoting role (Hodgkinson and Baginsky, 2000; Rossato and Brackenridge, 2009; Speller et al., 2010). For example, Rossato and Brackenridge (2009) have examined how child protection came to be covered in sports degrees and physical education ITT degrees following the introduction of the UK Government initiative Every Child Matters. They found that trainee teachers generally did not feel prepared for their role in child protection following ITT, and they saw their role as one of identifying potential problems and referring the issue to others who were more knowledgeable.
Four studies (Fenton, 2008; Taylor et al., 2008; Weatherby-Fell and Vincent, 2005; Yager, 2009) reported that health training had a positive impact on trainee teachers’ attitudes towards, and their understanding of, their health promotion role. For example, in one study (Taylor et al., 2008), after receiving training in pupil well-being that was ‘infused’ into their ITT course (including two school placement experiences), trainee teachers generally felt that they had developed a greater awareness of the importance of their and schools’ roles in health promotion and an increased understanding of the complexities of student well-being.
Variability in provision and quality of training
Four studies surveyed teacher training providers about how health topics were covered in their courses (Arnold and Maio, 2007; Hodgkinson and Baginsky, 2000; Rossato and Brackenridge, 2009; Speller et al., 2010), and one surveyed trainee teachers about their experiences of teaching or observing PSHE education and citizenship on school placement in the UK (Mead, 2004). The findings show variation in the provision and quality of training across different providers (Arnold and Maio, 2007; Hodgkinson and Baginsky, 2000; Speller et al., 2010), course types (Arnold and Maio, 2007; Speller et al., 2010) and school placements (Mead, 2004; Speller et al., 2010).
Mead (2004) found variability in primary trainees’ opportunities to teach and discuss PSHE and citizenship on school placement. For example, only up to 23% of the trainees reported having the opportunity to teach sex and relationships education. Opportunities depended on the nature of the placement schools.
Discussion
The evidence base for ITT for health is diverse in terms of the content and delivery of training. A staple element of training is the provision of information on health (in varying comprehensiveness), as reported in three-quarters of the studies. Training to enable teachers to develop the health-related behaviour skills of pupils was a feature of just under three-quarters of the studies. The training therefore resonates with health behaviour theoretical models that acknowledge the need to influence skills, in addition to information, to encourage healthy behaviours (Fisher et al., 1996; Tones and Tilford, 2001).
The systematic review found some evidence for the effectiveness of training, in terms of improving teachers’ knowledge and confidence to address health and well-being, and influencing their beliefs. However, studies tended to measure the impact of training in the short term. The long-term impact of training teachers is therefore unclear and requires further research. This is important as teachers make the transition from trainee to qualified teacher, often a complex process that leaves many feeling anxious and stressed (Howard and Johnson, 2004). The positive impact of any training in health and well-being is likely to be diminished in such circumstances, and therefore, the importance of a supportive environment that is conducive to promoting health and well-being is essential and needs to include appropriate mentoring (LoCasale-Crouch et al., 2012).
The outcome evaluations used uncontrolled designs, limiting definitive conclusions about the effectiveness of the training. Further, more rigorous, primary evaluation is therefore required. Studies should evaluate some of the elements that appear to be promising from the studies included in this review, such as the creation of a non-threatening environment to discuss sensitive issues.
There were mixed findings about the extent to which trainee teachers had assimilated responsibility for health and well-being into their roles as teachers and their understanding about their role after training. Over time, trainees recognised this role but acknowledged that there were limits to what they could realistically achieve in terms of addressing certain health issues. As Thomas and Beauchamp (2011) note, the transition from trainee to qualified teacher is a crucial time in terms of identity development. For many schools, a culture of performativity predominates and this discourse will affect new teachers as they participate in the interactions and conversations that reinforce a particular identity (Sfard and Prusak, 2005). The powerful discourse of academic achievement, performance and improvement may leave little room for non-academic and non-statutory subjects such as health and well-being education within the development of new teacher’s identities. As Mead (2011) argues, pre-service teachers require the opportunities to critically engage with health and well-being issues in a profound and reflective manner so that they are able to make the connections between their own values, their professional knowledge and pupil health and well-being. Doing so will help new teachers to appreciate the importance of health and well-being as an important aspect of their wider role.
Studies also found variation in the provision and quality of training across different providers, course types and school placements. One particular finding was that ITT providers were reliant on trainee teachers receiving health training on their school teaching placement, but that adequate training opportunities on placement were not always provided. The likely increase in time that trainee teachers will spend on training in schools as a result of ITT reforms (Department for Education, 2010), together with increased diversity in types of schools (e.g. free schools and academies), may compound the inconsistency in trainee teachers’ experience of health and well-being in ITT. In this changing landscape of teacher education, mentors and pastoral leads will be of crucial importance if new teachers are to be given the experiences and opportunities to increase their confidence and competence in teaching and managing health and well-being education. Furthermore, positive attitudes towards health and well-being seem to be engendered when confidence and competence are developed, thus increasing the likelihood of continuing to be involved in promoting health and well-being in the future (McNamara et al., 2012).
Conclusion
This is the first published systematic review to focus on ITT to promote health and well-being in schools. The evidence base in this area is diverse, with studies varying in the content, delivery and duration of training. It is not possible to make definitive conclusions about the effectiveness of training on teachers’ knowledge, confidence and skills at this time due to the weaknesses of the study designs used. However, there is tentative evidence to suggest a positive impact for teachers in these areas. None of the studies assessed the impact of training on pupils themselves, highlighting an important knowledge gap. The review identified a range of barriers and facilitators to effective training. Positive factors, such as providing more opportunities for practical experience to address health and well-being in schools, should be taken into account in the planning of future training. Further, more rigorous, research is needed to evaluate the full potential of ITT to enable teachers to address the health and education needs of children and young people.
Footnotes
Acknowledgements
Thanks to the advisory group for their input throughout the course of the project. Thanks also to Debbie Hartwell, Karen Welch and Jo Picot for assistance with the production of the research. This report presents independent research commissioned by the NIHR. The views and opinions expressed by authors in this publication are those of the authors and do not necessarily reflect those of the National Health Service (NHS), the NIHR, the Media Research Council (MRC), the Central Commissioning Facility (CCF), the NIHR Evaluation, Trials and Studies Coordinating Centre (NETSCC), the Public Health Research programme or the Department of Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute for Health Research (NIHR) Public Health Research programme (09/3005/12). It is published in full in the NIHR journal Public Health Research 1(2). Further information available at: ![]()