
Abstract
Objective:
This study evaluated self-trained basic life support (BLS) skills acquired from an e-learning platform to design a complementary in-class training approach.
Design:
In total, 41 students (15–17 years, 29 men) participated in a pilot study on self-training in BLS. After 6 weeks, a compression-only cardiopulmonary resuscitation (CPR) test assessed the skills acquired.
Setting:
A practice-based research setting. All data were collected in Flemish secondary schools in the context of the regular school curriculum.
Methods:
All tests were video-recorded. Data on motor skills were additionally collected on a Resusci Anne mannequin with Skillreporting software®. Quantitative data were analysed by analysis of variance (ANOVA). The qualitative aspects of basic life-saving actions were evaluated using European Resuscitation Council (ERC) guidelines.
Results:
Alerting emergency services, checking for consciousness and placing electrodes can be learned autonomously and be taught by means of pre-instruction. Hands-on training is necessary for compression skills and freeing the airway.
Conclusion:
Self-training in BLS offers insight into a flipped classroom CPR training strategy. Hands-on training should focus on motor skills, including head tilt and compression depth.
Introduction
For victims of sudden cardiac arrest, prompt calling for medical assistance and early cardiopulmonary resuscitation (CPR) are life-saving interventions. The chain of survival describes four life-saving steps in case of collapse: (1) prompt recognition of cardiac arrest and call for medical assistance, (2) early bystander CPR, (3) early defibrillation, (4) early advanced life support and (5) standardised post-resuscitation care (Handley et al., 2005). Three of these four steps may be performed by laypersons, closing the gap between the moment of collapse and the arrival of medical support (Nolan et al., 2010b). For this reason, many organisations have developed training programmes for lay people. Besides offering training in skills and knowledge, training programmes should also aim to create a positive attitude towards resuscitating a victim, should this be necessary.
Several studies have found that for lay people, willingness and attitudes to resuscitation are related to a person’s perceived knowledge about CPR and confidence in their own skills (Hamasu et al., 2009; Kanstad et al., 2011; Nolan et al., 2010b; Taniguchi et al., 2012). In addition, to encourage training and refresher training, programmes must also address aspects of motivation. Perceived competence, assessment and real-time feedback trigger the motivation to learn and correlate with a positive attitude to perform CPR if needed (Kanstad et al., 2011; Kromann et al., 2009). From this perspective, assessment and feedback serve a dual purpose: they assess both theory and practice, and they must result in perceived competence in a real-life emergency situation.
The International Liaison Committee on Resuscitation (ILCOR) stresses the importance of the provision of CPR training at school (Nolan et al., 2010a). Since the committee’s recommendation to include CPR in the school curriculum in 2003, worldwide efforts have been made to realise this goal. Since 2004, the American Heart Association (AHA) has encouraged state legislators to mandate CPR training in school. By 2010, this had been fully realised in 6 of 50 states and partially realised in another 30 states (Cave et al., 2011). The evaluation of skills was unclear in 20 states and absent for 10 states. In 16 of the 51 European countries, first aid forms part of the school curriculum (Bottiger et al., 2016). Mandatory learning outcomes for CPR have been formulated in four European countries (Breckwoldt et al., 2013). In Flanders, the northern part of Belgium, first aid and CPR skills are explicitly integrated into the regular school curriculum as teaching goals for physical education (PE) in the first (12–14 years) and third (16–18 years) years of secondary school. However, teaching goals about first aid and CPR are described somewhat vaguely. Consequently, the school team needs teachers who have a positive attitude and who feel confident about teaching these subjects.
Currently, only one-third of all teachers know that CPR is a mandatory subject (Mpotos et al., 2013), and Elchardus et al. (2008) have reported differing attitudes towards CPR among Flemish secondary school teachers. Most teachers (70%) regard it as important for children to learn CPR, while only 44% are convinced that it is the school’s responsibility to offer CPR training. The teachers most willing to teach CPR techniques are primary school teachers, although CPR is part of the secondary school curriculum (Mpotos et al., 2013). One in two Flemish secondary schools currently offers its students CPR training (Van Raemdonck et al., 2014). There is a strong positive intention among secondary school teachers to teach CPR, but the costs and time of training and the availability of training mannequins are barriers. In most cases, it is the PE teacher who provides CPR training in schools. The Flemish Red Cross offers specific training for teachers. Sixty percent of all Flemish teachers have received some training in CPR techniques, but many teachers feel insufficiently competent to teach this topic (Mpotos et al., 2013). Mpotos et al. (2013) argue that a range of teachers should be involved in facilitating CPR training programmes. This perspective is in line with a model of teacher education, whereby beginners gradually evolve learning from being ‘fully guided’ to being ‘fully in control of their own learning’ and where support of the instructor gradually changes to become a ‘guide on the side’ (Goodyear and Dudley, 2015).
Teachers do not necessarily need to be experts in performing CPR in order to coach students in learning how to resuscitate. However, they need to know which items to emphasise in each learning phase and why. This article offers arguments for the implementation of CPR training strategies in a flipped classroom context. Abeysekera and Dawson (2015) describe a flipped classroom as a learning strategy that ‘moves most information-transmitted teaching out of class, using class time for learning activities that are active and social and require students to complete pre- and/or post-class activities, in order to fully benefit from in-class work’(p. 3). De Araujo et al. (2017) attribute teachers’ willingness to flip to the advantages in classroom interaction and to the changes teachers perceive in teacher–student relationships. Recent studies show a growing consensus about the positive effects in learning outcomes and students’ achievements in a flipped learning context at school (Abeysekera and Dawson, 2015; Leo and Puzio, 2016). Flipping can also have a positive effect on self-efficacy, beliefs and intrinsic motivation of students (Thuy Thi Thai et al., 2017). In addition, learners are often found to be more motivated and engaged during the face-to-face teaching moments (Zamzami and Siti, 2016). Finally, this innovation positively affects the learners’ experience and perceptions of their own knowledge (Galway et al., 2014). All these positive effects can be attributed to the fact that flipped learning offers a more student-targeted approach (Aidinopoulou and Sampson, 2017; Galway et al., 2014; Zamzami and Siti, 2016)
Evidence on flipped classroom practices has recently been gathered across a number of research areas, but especially in health education (Abeysekera and Dawson, 2015). Merrill (2002: 45) described four principles of problem-centred instruction: (1) effective instruction activates existing knowledge as the foundation for new cognitive skills, (2) new knowledge or skills need to be demonstrated, (3) the learner then needs to apply the new knowledge or skills and, finally, (4) the learner needs to integrate new knowledge into the real world. These principles are applied at the Kennisdesk Academy® (Doczero, Veghel, The Netherlands), which developed an e-learning module to teach CPR that was used in this study. The module has a theoretical component in which students can read about basic life support (BLS) and where videos are used to demonstrate BLS skills. Through a multiple choice knowledge test and two micro-simulation scenarios, learners can apply their knowledge. The micro-simulation provided by the module offers the transfer to a real-world situation.
In a more recent study, Kim et al. (2014) outline nine design principles needed to create a successful flipped classroom approach. Such an approach should optimise students’ preparation prior to lectures and active learning settings. The Kennisdesk Academy module had been designed earlier, but the same nine principles also apply to it: (1) it was designed as a pre-instruction tool and uses easy-to-access technology, (2) it was designed as a platform to provide exposure prior to class, (3) it also offers structured guidance to the learners, (4) the combination of a knowledge test in the form of a quiz and micro-simulation provides self-assessment for preparation for class, (5) the module also offers instant feedback and (6) students are encouraged to achieve certification (with a score of 90% as an incentive). In our study, (7) there was enough time between the time of instruction and the time of testing (6 weeks) so that students could complete the assignments. Within the study design, there was no connection between in-class and out-of-class activities (8), but, after the test, students were offered a CPR hands-on training session, the content of which was closely linked to that of the training platform. The platform did not provide facilitation for building a learning community (9).
For flipped learning to be successful, the right blend of pre-class, in-class and post-class activities is important in order to maximise learning outcomes. This pilot study aimed to evaluate which aspects of BLS education students can learn autonomously using an online simulation programme but with no hands-on practice on a mannequin. This would help to design an in-class training approach that was complementary to the e-learning module.
Methods
A standardised pilot study was designed to measure learning outcomes from a web-based micro-simulation tool for BLS. Participants were selected via convenience sampling from three different schools that had accepted our invitation to participate in the study. Invited schools were participants in an earlier study on the provision of CPR training at school. Based on their answers to a questionnaire concerning intention to organise CPR training in school within a short-term period, individual schools were invited to participate in the pilot. After their school had accepted, participation was compulsory for students.
All participants were informed about the study, and their parents provided signed informed consent. At the time of the study, the university policy did not require approval by an ethics committee for studies in human and behavioural sciences which fitted in with the normal lessons of the school curriculum. Unregistered students and those with previous CPR training were excluded from the analysis. The Kennisdesk Academy training tool is a web-based simulation platform developed to train individuals in CPR knowledge and skills. It includes a textual and a video-illustrated theoretical component, a multiple choice knowledge test and two micro-simulation scenarios in which learners apply their knowledge. In the training mode, students can practise as often as they like without receiving a score. The later evaluation mode consists of three parts, providing a maximum score of 100%: 10% on theoretical background, 30% on testing cognitive skills and 60% on the video simulation. After each attempt, students receive textual feedback. After achieving an overall score of 90% on the evaluation mode, a training certificate can be downloaded from the system.
Participants were first informed about the use of the simulation platform. They were then asked to train themselves over a 6-week period and to try to become certified. They could choose how frequently they trained and whether to train in theory or skills or both. They were also informed about a 5-minute test that would assess their skills on compression-only CPR with the use of an automatic external defibrillator (AED) at the end of these 6 weeks. The test focused on compression-only CPR because ventilation cannot be taught properly in a short training session and without hands-on time (Nolan et al., 2010b; Van Raemdonck et al., 2014). Data on registration, training activity and training frequency of each participant were retrieved from the web application. The compression-only skills tests were recorded on video. Qualitative aspects about basic life-saving actions were evaluated according to the European Resuscitation Council (ERC) 2010 Guidelines,1 as described in Table 1 by a certified instructor in ERC.
Description and definition of variables.
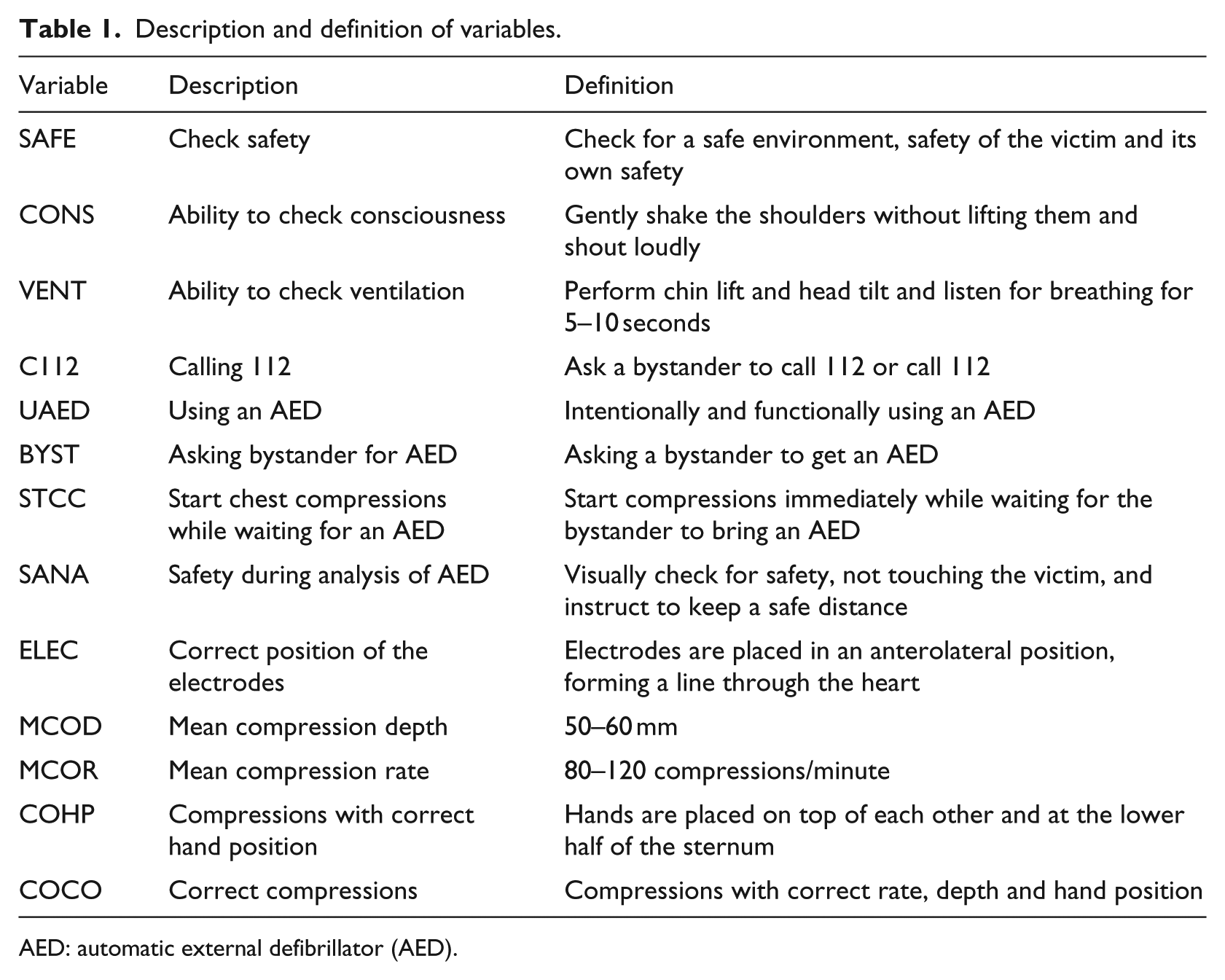
AED: automatic external defibrillator (AED).
To score the skills, the official evaluation form from ERC courses was used. Data on motor skills were collected on a Resusci Anne mannequin using Skillreporting software® (Lærdal, Norway). Quantitative data referring to the variables mean compression depth (MCOD) and mean compression rate (MCOR) were analysed by analysis of variance (ANOVA), the calculation of frequencies and cross tabulation using IBM® SPSS® Statistics version 21.
Results
In all, 41 secondary school students (15–17 years old: 29 men, 12 women) without previous CPR training participated in the self-training programme on BLS with an AED. Of the initial sample of 41 students, 12% (N = 5) did not register on the e-learning environment. These participants were excluded from further analysis. The training certificate was obtained by 47% (N = 17) of the registered participants.
The ratio between the total time spent on the platform and the time spent to certification (TT:TC) showed that all participants almost immediately started in the evaluation mode. The TT:TC ratio was, respectively, 1.00 (N = 14), 1.09 (N = 1), 1.15 (N = 1) and 11.68 (N = 1). In the cases where the TT:TC ratio was high, the time spent on training was high (60 minutes) and the time spent in the examination mode was low (5 minutes). The mean time spent on the platform was 39 minutes for the non-certified group and 71 minutes for the certified group (p = .003). Certified students spent 26 (±6) minutes on the theory, 18 (±2) minutes on knowledge testing and 26 (±4) minutes on the micro-simulation. The TT:TC was 1.05 for the knowledge test and 1.14 for the micro-simulation for certified students. For non-certified students, the time spent on theory, knowledge and micro-simulation was 26 (±5), 4 (±1) and 7 (±2) minutes, respectively. There was no significant difference in practice time for theory, knowledge test and micro-simulation between the certified and non-certified groups.
Table 2 shows the results for the qualitative variables of chest compressions performed on a mannequin. Except for checking breathing, most participants performed well on calling emergency services and on positioning the AED electrodes. All participants used the AED. There were no differences between the certified group and the non-certified group regarding these qualitative variables.
Percentages and frequencies on qualitative variables of basic life-saving actions.
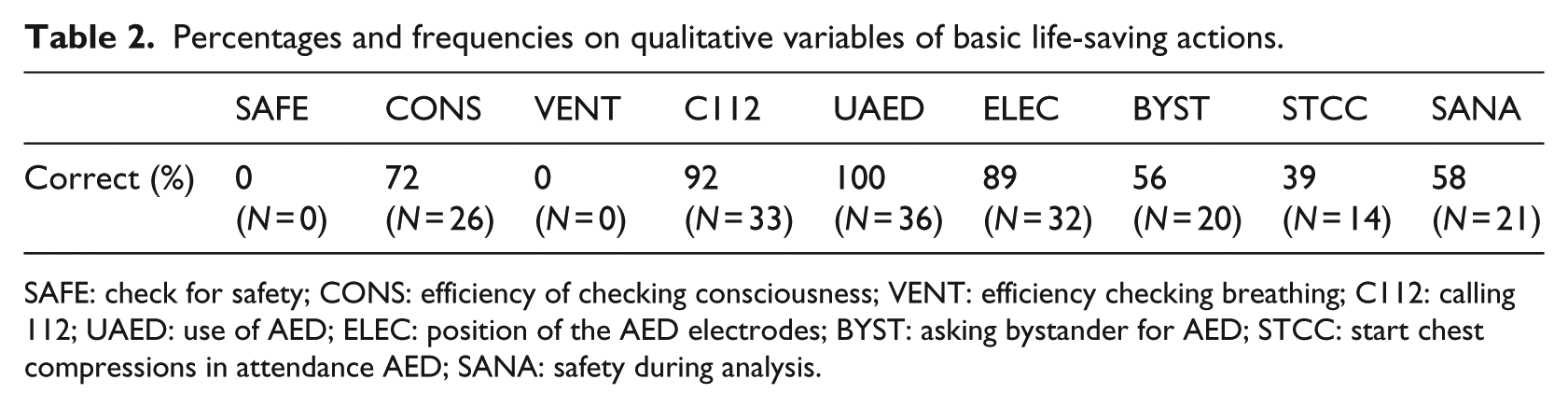
SAFE: check for safety; CONS: efficiency of checking consciousness; VENT: efficiency checking breathing; C112: calling 112; UAED: use of AED; ELEC: position of the AED electrodes; BYST: asking bystander for AED; STCC: start chest compressions in attendance AED; SANA: safety during analysis.
No one checked safety before starting the BLS actions. The main error made in checking consciousness was slapping the victim on the face (14%; N = 5). Checking for breathing was ineffective because none of the participants tilted the head backwards in order to open the airway. Chin lift was performed by 25% (N = 9) of the students. Almost half of the students (42%; N = 15) checked for breathing for less than 5 seconds, which is too short to be effective. In the case of seven students (19%), the moment of starting chest compressions was not registered due to a technical error and their results were excluded. Motor skills on chest compressions are shown in Table 3.
Means, standard deviations and frequencies for compression depth and rate.
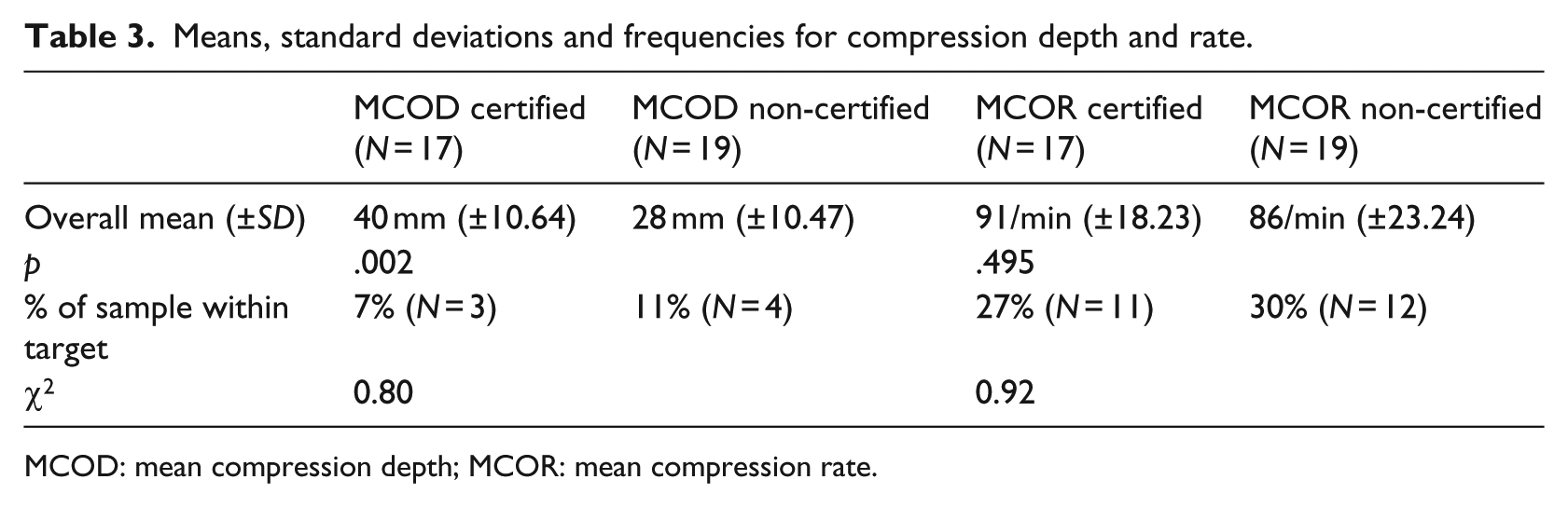
MCOD: mean compression depth; MCOR: mean compression rate.
The mean compression depth was significantly deeper for the certified group compared to the non-certified group, but was too low in both groups. More non-certified students reached the target depth. In total, 18% of the students reached sufficient compression depth. There were no differences in mean compression rate, scoring close to the guideline of at least 100 compressions/minute and within the range of 80–120 compressions/minute. Fifty-seven percent of the students reached the target rate, with a higher proportion in the non-certified group. An overall score for the number of compressions with correct hand position was calculated. Forty-four percent (N = 16) of all participants reached more than 75% of the compressions with the correct hand position, while 47% (N = 17) scored less than 50%. There were no differences for correct hand position between the certified and non-certified groups.
Three students (8%) were able to perform more than 50% of the chest compressions without error, of which two (6%) scored well on 75% or more of the performed compressions. They were all from the certified group.
Discussion
This study shows that web-based micro-simulation with online feedback can be an effective training tool in order to learn ‘what to do’. Referring back to the purpose of this study, it is reasonable to use an e-learning tool such as the Kennisdesk Academy to teach some of the cognitive BLS skills and to teach the use of an AED. This offers the opportunity for a flipped classroom approach. It also provides alternatives if limited time is available for BLS training and if the availability of resuscitation mannequins is scarce.
In our study, the mastering of basic CPR skills, or learning ‘how to do it’, was sub-optimal. Although training time varied greatly between participants, especially in the non-certified group, the average student spent about 1 hour learning the basics of CPR online. Our analysis of the time spent on the several parts of the platform showed that the non-certification of students overlaps with important parts of the platform being barely completed by these students. These included the knowledge test (quiz) and the micro-simulation. To be able to apply knowledge in practice, a minimum training time of approximately 20 minutes is advised for these two parts. For the qualitative variables (e.g. SAFE and SANA), no differences were found between the certified and non-certified groups. This could mean that reading the theory in combination with the video instruction provided was enough to contribute to the acquisition of basic knowledge about BLS.
Participants scored well on most of the knowledge-related basic life-saving actions, especially calling emergency services, using an AED and positioning the electrodes. Items such as checking for consciousness may benefit from the provision of more visual feedback during pre-instruction and from kinaesthetic feedback during hands-on training instead of solely textual feedback. In contrast to knowledge, compression skills cannot be fully mastered without hands-on training, although the results of some important items such as hand position and compression rate were acceptable. The fact that more non-certified students reached the target depth (50–60 mm) compared to certified students may be misleading since the difference was not significant. However, deeper compressions can lead to a lower compression rate (Fletcher et al., 2008). Auditory support during chest compressions can help learners to follow the correct rate for chest compression (Kern et al., 2010), but the learning platform cannot provide auditory feedback because there is no practice on a mannequin. Providing a means to simulate chest compressions may be a way to help substantially more students score closer to the guideline of at least 100 compressions/minute. The better results on compression rate may partially explain the poorer results on compression depth because of the quicker release of the chest (Handley et al., 2005).
Students also failed to master other more complicated motor actions. The action of how to check for breathing is explained in the theoretical part of the simulation, but it is not performed by the learner in the micro-simulation. This may partly explain the poor results on tilting the head backwards. It would be valuable to stress the importance of this element in the simulation videos. Nevertheless, for ventilation skills, hand-on training is necessary. A previous study already observed the difficulty of learning ventilation skills without practice (Van Raemdonck et al., 2014). Although head tilt seems less important within the context of compression-only CPR, it is an important skill in the decision-taking process to start CPR or not. Instructors and teachers should be aware of the complexity of this skill and should focus on its correct performance during training. Skills concerning compression rate, compression depth and checking for breathing are items that also need special attention during the hands-on training following the online learning process. These results confirm previous findings in the literature (Nolan et al., 2010b). Hands-on time is crucial, especially for the psychomotor skills involved in BLS (Soar et al., 2010).
Limitations
This study has some limitations. The 2010 ERC guidelines on resuscitation were utilised because of the timing of the data collection. However, the most recent guidelines date from 2015. The differences between the 2010 and 2015 guidelines on resuscitation are small and mainly focus on the important role of the medical dispatcher during an emergency call. Guidelines referring to CPR skills did not change. We therefore think that this change is unlikely to affect our results.
There was also a potential for selection bias because participants were selected from schools where teachers and school board were prepared to participate in the study. Because of the small number of participants, we were unable to perform any sub-analyses (e.g. on gender differences). We believe, however, that the inequality in the number of boys and girls in this sample has limited influence. At age 16, physical differences in strength between boys and girls do not play an important role because the body weight of both boys and girls makes them physically capable of adequately performing CPR (Abelairas-Gómeza et al., 2014; Lopez-Messa et al., 2011).
Our study did not use a baseline assessment and control group. We do not believe that the absence of a baseline assessment reduced its validity. Since testing has a learning effect, in this case a baseline assessment mght also create bias in the results (Kromann et al., 2009). To compare findings against a control group, more participants would have been necessary, which was not possible in this case. For students, participation was compulsory, as a part of their curriculum. Some students did not register in the learning platform and/or did not practise much. We did not collect data on the reasons why they did not register or only read the theory. This phenomenon is a natural reflection of ‘in-classroom-realities’ and to an extent may benefit ecological validity.
Since the participants knew they would be tested, their motivation to learn may have been high. We do not believe this affected the results since teachers in a real learning context may also use testing to stimulate training and motivation to learn. Moreover, testing to increase motivation is an acceptable and recommended method for the acquisition of life-saving skills. Such an approach fits with the motivational continuum outlined by Ryan and Deci (2000) in self-determination theory and is different for all participants.
Conclusion
Several basic life-saving actions can be learned autonomously through an online learning tool. They include alerting emergency services, using an AED and learning how to position the electrodes of the AED. As part of a mixed method or flipped classroom approach for BLS, online teaching can engage with several of the cognitive issues involved and can prepare students to use an AED prior to face-to-face teaching
Motor skills, especially freeing the airway, and chest compression skills need extra attention as part of a practical training session. In hands-on training, teachers should focus on the more complex psychomotor skills involved in CPR, specifically the assessment of breathing, limiting hands-off time and immediately starting chest compressions, safety during the analysis of AED use and compression depth. If the school context provides limited opportunities for hands-on training, e-learning in a flipped classroom approach could be a successful way to increase the effectiveness of some of the work that needs to be undertaken.
Footnotes
Acknowledgements
We thank all the schools that participated in this study. Special thanks also goes to Doczero Learning for providing licences at reduced rates for the use of the Doczero Kennisdesk®.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.