
Abstract
Introduction:
Children and young people in India have a high prevalence of dental decay. As part of a broader epidemiological study, we interviewed 10 head teachers to understand the status of, and challenges to, inclusion of oral health education in the curricula of public and private schools in Tamil Nadu, India.
Objectives:
The two main objectives of this study were (1) to describe the views of head teachers about the implementation of oral health education in school curricula and (2) to identify challenges to achieving oral health education in public and private schools in Tamil Nadu.
Method:
Qualitative descriptive design, with a purposive sample of 10 head teachers who participated in semi-structured interviews. Thematic coding was used to analyse and report on the data.
Results:
There is a lack of oral health education in public and private schools in Tamil Nadu, India. Four main types of barriers to the initiation and implementation of oral health education were lack of recognition, academic burden, prioritisation of other health needs and policy inequities. Head teachers acknowledged the lack of oral health education in their schools, yet also acknowledged the importance of oral health education in promoting students’ health.
Conclusion:
Health curricula in Tamil Nadu schools lack integration of oral health education. Limited access to the services, cultural factors, policy deficiencies, insufficient awareness among policy-makers, the nature of the education system and lack of research contribute to the current situation. Policy-makers should address these barriers to enable and promote oral health education strategies in both private and public schools of Tamil Nadu.
Introduction
School-based oral health education is fundamental for oral health promotion. Schools provide a platform on which to promote oral health as more than 1 billion children are educated worldwide through them. In principle, good quality health education in schools could benefit school staff, parents and everyone in the wider community (Kwan et al., 2005). Many common oral health diseases are preventable through good quality health education in schools (Kwan et al., 2005); hence, schools have an important role to play in modifying children’s attitudes and behaviours towards health.
In Tamil Nadu, India, there are over 50,000 schools. Of these, about 68% are public schools with an enrolment rate of 99.4% and an attendance rate of 97%. The state government is responsible for school administration, and schools are divided into different types depending on the examinations available to students. All public and most private schools follow the Samacheer Kalvi curriculum or Uniform System of Education. A content analysis of this curriculum suggests that in the primary years of 1–5, the following oral health topics are included: basic information on parts and types of teeth, tooth decay and the importance of brushing (Geetha Priya et al., 2016). In the middle and high school curriculum, health education is taught through the subject areas of Ariviyal Tamil (Tamil language science) and environmental education, but neither of these subject areas addresses the issues of oral health. In 2007, a national rural health mission school initiated an oral health awareness programme in India. This included screening for the early identification and prevention of oro-dental problems (Ministry of Health and Family Welfare, 2005). In Tamil Nadu, as of 2016, only 360 of 1,421 primary health centres provided basic dental treatment, such as fillings, scaling and extractions.
In India more generally, the budget allocated for national oral health care in the most recent 5-year plan was USD2.31 million per year to satisfy the health needs of over 1 billion people. This budget for oral health care should be seen within the context of the annual total public health expenditure of USD16.569 billion for the fiscal year 2012–2013 (Grover, 2014), and this suggests that the allocation of public funding for oral health is very low (7,500 times lower) compared to general health allocations. By comparison, New Zealand, a country with a successful oral health care system, spends USD66 million per year on oral health (Ministry of Health, 2006) to meet the needs of a total population of over 4.6 million (Figure 1).
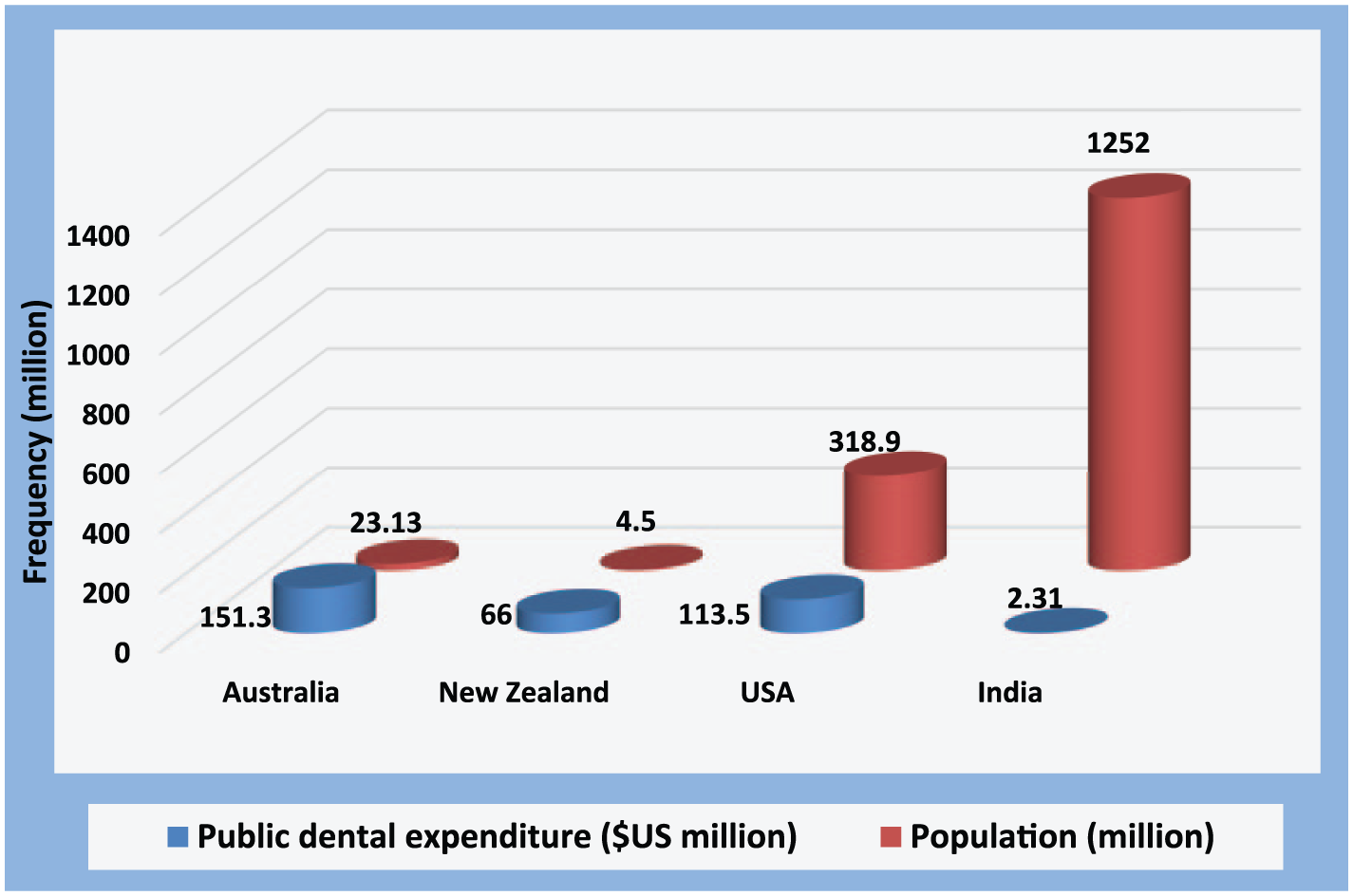
Public dental expenditure in Australia, New Zealand, USA and India (Grover, 2014; Ministry of Health, 2006; Ministry of Health and Family Welfare, 2005).
Oral health inequalities are a concern in India because dentists tend to work in urban areas, but only one-quarter of the country’s population live in urban communities. The dentist to patient ratio in urban areas is 1:10,000 and in rural areas is 1:250,000 (Singh and Purohit, 2013). Moreover, only 20% of primary health centres in India are equipped with dental units (Singh and Purohit, 2013). In this context, limited access to dental treatment requires the majority of the Indian population to depend on oral health education alone to prevent oral health disease.
Oral health education is frequently neglected in the Indian education curriculum (Bhardwaj et al., 2013). The effectiveness of oral health education in schools has been demonstrated in various studies (Bhardwaj et al., 2013; Freeman et al., 2016; Nakre and Harikiran, 2013). In India, children and adolescents make up 40% of the total population (Government of India, 2012), schooling is compulsory until 14 years of age in the state of Tamil Nadu and children are provided with free textbooks, a uniform, a free mid-day meal and free stationery supplies. Consequently, oral health education delivered through the school system would reach a substantial number of the population. Moreover, India’s diversity with respect to language, culture, religion and caste makes school a suitable environment for children to benefit from oral health education in an inclusive manner.
A literature review identified seven studies conducted in India assessing the effect of school-based oral health education on oral health outcomes (Ajithkrishnan et al., 2010; Bhardwaj et al., 2013; Chachra et al., 2011; Gambhir et al., 2013; Gauba et al., 2013; Grewal et al., 2009; Parkash et al., 2004). Because school-based oral health education is in the early stages of development, the majority of these studies focused on guideline development rather than on effective oral health education strategies. A few of the studies, however, comprised interventions to test the effect of oral health education on oral health status (Ajithkrishnan et al., 2010; Bhardwaj et al., 2013; Gauba et al., 2013).
School-based oral health education has been shown to have significant effects on knowledge, attitudes, oral hygiene practice and oral health status of adolescent populations. For example, Parkash et al. (2004) investigated the effects of school-based oral health education on children’s attitudes, knowledge and behaviours using a three-phase intervention study in New Delhi, India (Parkash et al., 2004). In the first phase, 1,500 students in the 6–8 and 12–14 year groups were evaluated for pre-intervention oral health status, together with their knowledge, attitudes and practices. In the second phase, oral health education was provided by teachers. In the third phase, a post-intervention evaluation was conducted using the same oral health survey instruments (Parkash et al., 2004). Average Decayed, Missing, Filled Teeth (DMFT) decreased from 1.62 to 1.51 per child as a positive outcome of the intervention, with results being statistically significant (p < .001). Among the sampled senior-aged children, the total number of filled teeth increased from 30 at baseline examination to 224 at the final examination, again seen as a positive outcome related to the intervention. There was also a marginal increase in knowledge, attitudes and practices scores in the final evaluation (Parkash et al., 2004). Hence, targeting children and adolescents using the existing infrastructure and human resources at school can be a clinically effective and economically efficient implementation option in the current Indian context.
Our initial study, conducted among the adolescent population in Tamil Nadu schools, investigated the oral health literacy of adolescents attending private and public schools in both rural and urban areas (Veerasamy et al., 2016b). Only 8% of adolescents had sufficient oral health literacy to understand the importance of protecting their oral health. The prevalence of dental caries was identified as 61.5%, with a mean DMFT of 2.03 (Veerasamy et al., 2016a). Hence, effective oral health education is essential to improve the oral health literacy of the adolescent population and in turn improve oral health outcomes in Tamil Nadu. This study was conducted to explore the views of head teachers regarding the implementation of oral health education in school curricula and to understand whether oral health policies are implemented in private and public schools of Tamil Nadu. The findings will be helpful towards developing school-based oral health education programmes.
Methods
A qualitative descriptive approach was chosen to examine whether policies relevant to oral health education exist and are being implemented, either directly or indirectly, in the Tamil Nadu school curriculum. Data collection involved gathering head teachers’ perceptions, opinions, knowledge and attitudes towards oral health policies and the implementation of oral health education in schools. To ensure the trustworthiness of the study, we followed the criteria for credibility, transferability, dependability and confirmability (Shenton, 2004). Prior to the commencement of the study, ethical approvals were received from the Human Ethics Committee, University of Canterbury, New Zealand, and from the Institutional Review Board, Sree Balaji Dental University, Tamil Nadu, India.
This study was conducted as a part of a larger oral health epidemiological study among an adolescent school population (Veerasamy et al., 2016a). Participants for the epidemiological study were randomly selected from two districts of Tamil Nadu: urban participants were recruited from Chennai city, and rural participants were from Thanjavur district. The Chennai city corporation is organised into 15 zones consisting of 200 wards. Five of the 15 zones in Chennai city were randomly selected. The wards within each zone were also randomly selected and private and public schools in each ward were listed; eight randomly selected schools were approached for permission to recruit participants for the study, and four schools accepted to participate. The Thanjavur district is divided into three revenue divisions, namely, Thanjavur, Kumbakonam and Pattukottai. Eight schools were randomly selected across all revenue divisions, and all selected schools accepted to participate in the study. A quota sampling system was then used to invite head teachers from all selected schools to participate in the study. Four urban (two from public and two from private) and six rural (three from public and three from private) school head teachers accepted this invitation. Two head teachers declined to participate in the study. Hence, the participants for the qualitative interviews were recruited from private and public schools in both rural and urban areas of Tamil Nadu.
In India, each school is administered by one head teacher who is solely responsible for institutional planning and management. He or she decides how to use the available resources and how to initiate steps to mobilise these resources and involve teachers, parents and other organisations to achieve quality education for students. Hence, head teachers were invited to participate in an interview and were given an envelope that contained the research information, consent forms and a list of the questions that would be asked in the interview.
Face-to-face interviews were held at each head teacher’s school, at their convenience. Written informed consent to participate in the interview was received prior to the interview. The interviews were audio-recorded with the permission of the participants and conducted in either Tamil or English depending on the participant’s preference. Only one head teacher opted to be interviewed in English. The interviews ranged from 15 to 25 minutes in duration and were recorded using Evernote software on an iPad. Data were transferred to a computer on the same day. Field notes were taken before and after each interview, and these were used during analysis of the data. These notes contained details needed to understand the school culture and infrastructure. Both the field notes and interviews were coded with pseudonyms to preserve the school and individuals’ anonymity. The interviews were transcribed and later translated into English by the lead researcher. Head teachers were given an opportunity to read their interview transcript and provide further comments. None of the head teachers who reviewed their transcript requested changes. Qualitative findings are reported below using recommended guidelines from the Standard for Reporting Qualitative Research (SROR) (O’Brien et al., 2014).
Analysis
Braun and Clarke’s (2006) thematic coding and analytical framework was utilised as follows. Interviews were initially analysed question by question in two phases. First, each interview transcript was coded and analysed to identify categories and themes specific to the original research questions, namely, what is the extent of oral health education occurring in schools? What are the head teacher’s views on implementing oral health education? And, what other challenges are there in implementing oral health education in Tamil Nadu schools?
The responses provided by the head teachers were organised and analysed through a sequence of organising, summarising and interpreting the data (Braun and Clarke, 2006). By reading and re-reading the transcripts, codes were identified. The codes were then categorised according to whether the respondent was from a private, public, rural or urban school to enable a description of differences and similarities between school type and location.
During the interviews, it was noted that head teachers displayed a lack of awareness of what oral health encompasses. In response to this, the interviewer was careful to identify whether any ‘hidden’ oral health–related policies were incorporated into the school curricula. For example, a sugar-free policy was incorporated into one school’s curriculum for health reasons, but the head teacher reported that he or she did not have any oral health policies.
In the second phase of the analysis, new ideas which did not specifically relate to the original research questions were identified from the data, analysed and coded separately. One of the new ideas that emerged during the second phase of the analysis was the lack of food and other basic needs in schools, especially for adolescent women.
Finally, in the verification phase, conclusions were drawn from combining all the categories in the first two phases of analysis. Four overarching themes were identified.
Findings
On completion of 10 interviews, it was evident that oral health education was not well recognised in any of the schools. A lack of awareness regarding oral health was repeatedly identified among head teachers’ responses, as was a lack of awareness for the need to implement oral health policies. Hence, it was concluded at this point that data saturation had been achieved.
All of the head teachers had more than 20 years of teaching experience, and all had worked as a head teacher for 5–22 years in their current school or in schools with a similar curriculum. The four key themes that emerged were lack of recognition, academic burden, prioritisation of other health needs and policy inequities.
Lack of recognition
Seven of the 10 head teachers said their school did not have any policies relevant to oral health: Frankly speaking, we don’t have anything special for oral health. (HT1 Chennai Private) There is no specific policy for oral health, but the general health screening included everything. Like skin, eyesight related illness (including provision of free spectacles), general health etc. But … see … nothing special for oral health. (HT3 Public Rural)
Three head teachers indicated they had oral health policies in their schools. Further questioning revealed that a nearby private dental university and private dentists through the Indian Dental Association (IDA) funded some oral health screening in their schools. Hence, none of the schools had implemented any oral health policies; however, they allowed private dental schools and dentists from the IDA to offer occasional oral health screening to the children in their schools. No regular oral health check-ups were provided to their students, and the head teachers acknowledged that the dental screenings were ineffective without a proper follow-up: I feel the check-ups are done just to account of coverage by IDA. I don’t think the check-ups provide any intensive care. We don’t do any sort of follow-ups to those dental check-ups as we don’t even have enough time for academics. (HT5 Rural Private)
Most of the head teachers reported that emphasis should be given to oral health education in the school curriculum. Ideas about the nature of oral health education differed between the head teachers irrespective of the schools with which they were involved. One of the head teachers indicated that awareness of both health and oral health education should be increased. Another head teacher indicated that oral health education should be included in the high school curriculum as parents tend to ignore the oral health of older children. Another head teacher expressed that oral health education should be discussed as part of an existing science-based language: Though a lot has been included in the latest curriculum, it is all about health and hygiene only. Not enough emphasis has been given to oral health. (HT3 Rural Public) No! None of the syllabus covered oral health education … Neither the curriculum has covered it … We never gave any oral health education other than asking them to brush their teeth. (HT7 Urban Public)
One of the head teachers acknowledged that even general health education needed to be improved and sufficient efforts should be made by the government to include oral health education in the curriculum: In my opinion, the extent of general health education itself is not adequate. The Government should take enough steps to improve both health education and the oral health education. (HT7 Urban Public)
Academic burden
When teachers were asked their opinions about improving oral health education in the current school curriculum, half of the head teachers agreed that oral health education should be enhanced. Conversely, other head teachers reported that improving oral health education in the curriculum would become a burden for children, and there would not be enough time to concentrate on health and oral health education due to the volume of academic assignments and examinations: The students have already a lot to do at school. I think what they have is more than enough for now. (HT2 Urban Public) Students cannot be overloaded … In our country we do not have much dental issues as in developed countries. I think already our curriculum covers what they need to know for their age. I also think still our eating habits are good … the kids do not have any access to sugar rich food as in developed countries. (HT6 Rural Public)
One of the head teachers emphasised the burden of teaching three languages in Indian schools and added that most Western countries do not have this problem: Basically, time would be a constraint … We are in position to concentrate on teaching English apart from Tamil and Hindi. Language learning wouldn’t be an issue in most of the western countries but it is definitely a big burden for our country where our children have to learn to write and speak the national language, international language and also our mother tongue. (HT5 Rural Private)
In the later interviews, head teachers were explicitly asked questions regarding academic burden and the possibility of space within their curricula to include oral health education. These head teachers indicated that the number of examinations and pressure to score high marks were issues for 10th and 12th standard students but not for all. They conceded that there would be enough space to include oral health education in the curriculum for other students: The fact is, apart from 10th and 12th standard kids, there is no study pressure or workload for the other grades … the reality is we have not taken any interest in teaching oral health education. (HT 10 Rural Private)
Hence, the majority of head teachers reported that oral health education was not currently emphasised in the school curriculum. It was also noted that both health education and oral health education were not generally included in private school curricula. Some of the head teachers who were initially interviewed were concerned that adding oral health education into the curriculum would increase the workload not only for students but also for school management and teachers.
Prioritisation of other health needs
The majority of head teachers from public schools said there were many unmet health needs in Indian schools which they prioritised ahead of oral health. For example, one head teacher explained, Many students faint during the morning prayer assembly. A few of them even miss their lunch. And many of them can only afford supper. I have noticed a few students having the noon meal inconspicuously, even though they are not enrolled and eligible for it. I just ignore it because they can’t even afford a single meal for the day. (HT3 Rural Public)
The teachers indicated that including oral health education was beyond the current requirements and needs of the children. One head teacher stated that oral health education was not needed because none of his students complained of oral health issues; this teacher also believed that Indians have better oral health compared to Western communities.
Head teachers did not consider oral health policies or oral health education to be a priority for the children. Most of the head teachers felt oral health education was unnecessary when children, particularly girls, were struggling to meet basic needs, such as regular food and other simple health requirements: Girls in our school eat very little and sometimes do not bring lunch … Girls experience poverty as well as lack of care by the parents … Mainly because the parents care more for the sons than the daughters … The food consumed by our school girls is very low both in quantity and quality … (HT 4 Rural Public) Some kids could not even have energy to stand in the assembly for 10 minutes … Software companies provide sakarai pongal (Sweet rice), cereals and vegetable biryani for all 2000 students twice a week … they also adopted 500 children who are not under the government mid-day programme and give them protein powder, raw sugar and also stationary, including a dictionary, atlas and general knowledge book every year … (HT2 Urban Public)
In contrast to public school head teachers, private schoolteachers were concerned about children gaining more access to junk food. Most of the private schoolteachers reported that the children in their schools did not have problems accessing enough food: In my opinion, I would say they get more access to healthy food than we got in our childhood … now-a-days we have tremendous variety of food … (HT 1 Urban Private) We do not face such issues in our school because the majority of kids in our school are from above the average socio-economic status. (HT 10 Rural Private)
Access to healthy food was the most important issue described by public school head teachers in both urban and rural areas.
Policy inequities
One private school head teacher indicated that health education was not a priority in his or her school, despite the fact that health education was mandatory: No not for the private schools … Unfortunately we do not focus on these important things and concentrate only on academic marks, scores and grades. (HT 1 Private Urban)
However, all of the public school head teachers indicated that they provided general health education and health care for students: We do have yearly health check-ups. It is so effective that one of our students underwent a heart surgery which was identified, diagnosed and treated successfully due to amazing health services at school. (HT 2 Urban Public)
A head teacher at a Chennai public school spoke about the twice-yearly routine dental screening organised through private dental universities in the area. She mentioned that she was amazed by these services because she had experience of working in different parts of Tamil Nadu, and it was only in her current school that children were benefiting from dental screening and referral services: I worked in different parts of Tamil Nadu. I am amazed about all these because only in the current school I have seen such dental screenings and follow-ups. (HT2 Urban Public)
The public school head teachers indicated that teachers had annual training for health awareness in regard to HIV, tuberculosis and cancer. Private schoolteachers reported that they did not have any policies to train teachers to provide either health education or oral health education: No such trainings for the private school teachers. (HT 1 Urban Private) I feel there is a lack of awareness among the teachers … they really need some training to impart it to the students … but we are not fortunate enough. (HT5 Rural Private)
Various issues, such as lack of interest among students in respect to health education, lack of staff and difficulty in appointing designated staff to manage and deliver oral health education to students, were also indicated. Furthermore, head teachers described a lack of awareness among policy-makers about how to initiate and implement oral health education in the school curriculum: Someone should be there to suggest including oral health education to the committee … Just like you suggesting to me … I think someone should suggest policy makers to implement such schemes … Now health education is in hands of science teacher … (HT7 Urban Public)
One head teacher identified that health education has not been added into the curriculum due to lack of awareness among policy-makers, and hence, adding oral health education to the curriculum would increase the time it would take to bring it into practice: Our Ministry of Health has proposed health education in schools but it is being delayed because of lack of awareness among policy makers. (HT10 Rural Private)
Discussion
Our study aim was to identify the status of current oral health education in private and public schools in rural and urban areas of Tamil Nadu. Findings suggest that oral health education is generally ignored in both private and public schools. Most of the head teachers interviewed for this study believed oral health education should be mandatory for students; however, public school head teachers considered oral health education as less important because essential basic needs such as access to enough food were not being fulfilled.
This study revealed that private schools, which accommodate higher socio-economic populations, are gaining more access to both junk foods and nutritious foods. In contrast, public school head teachers indicated that classroom hunger was still a significant issue in their schools in Tamil Nadu. Recently, the Tamil Nadu Government launched a restaurant chain throughout the state, providing healthy and hygienic food to the public at low cost (breakfast: USD0.02; meals: USD0.08). This programme was initiated after data collection took place for this study. This initiative is now addressing classroom hunger, but the assumption that every student has access to, and is using, this programme requires further investigation.
The schools located closer to dental colleges had the advantage of frequent oral health screening together with follow-up for treatments. A few schools had dental screenings conducted by the IDA, but head teachers indicated these were insufficient because follow-up treatments were not provided, and oral health issues identified in the screenings were not treated. Janakiram and Taha (2016) argued that screening for dental decay and other oral health diseases without any follow-up treatment is unethical practice. This is particularly true for those who do not have affordable access to a dentist for further treatment as they, therefore, cannot benefit from routine oral health screening. Even though dental screenings are considered part of oral health awareness programmes, enabling policy could be implemented whereby follow-up treatment is made accessible for child and adolescent populations. Hence, the current practice of screening only to diagnose dental caries by dental universities for dental education purposes, and by the IDA for oral health promotion, should be reviewed.
This study revealed inequities with respect to health policies between private and public schools. Public schools received highly efficient health coverage, including eye checks, heart surgeries and also monthly blood tests for students, with the exception of oral care. Private schools did not have regular health educational training for the teachers about important health issues, such as tuberculosis and AIDS. Parkash et al. (2004) suggested that the oral health education provided by teachers was effective in reducing dental caries and also in improving oral health knowledge and attitudes. Hence, proper training should be given to teachers in Tamil Nadu to improve their oral health literacy so that they can provide oral health education to students. Private schools have generally ignored both health and oral health education; however, public schools provided efficient health coverage and general health education training to the teachers, with the exception of oral health education. Both private and public schoolteachers should be trained to provide oral health education. Local dental institutions and the IDA could concentrate on training teachers rather than simply providing a periodic screening. A report by the Director of the Central Board of School Education, which was based on a review of health education from 10 different states, indicated that priorities for health education were limited in actual practice (Nazar, 2011). Nazar (2011) was also critical about the lack of commitment by the Health and Educational Department for health promotion delivered through schools, which was also indicated by the head teachers in this study.
Head teachers indicated that a lack of awareness among policy-makers was a major reason behind the non-existence of oral health education-related policies in Tamil Nadu schools. Tandon (2004) suggested that one of the greatest challenges for the Indian oral health care system was the lack of qualifications and training among policy-makers and dental health planners in public health dentistry. Tandon (2004) identified an insufficiently qualified workforce as a major challenge for developing a better oral health care system in India. Difficulty in training teachers and appointing new staff or school nurses to promote oral health education was also repeatedly mentioned as a significant problem among head teachers in this study.
A systemic review on the effectiveness of oral health education on oral health outcomes reported that most successful oral health programmes are labour-intensive and received significant funding and additional support (Nakre and Harikiran, 2013). In this study, the majority of head teachers viewed implementation of oral health education as a difficult task in the current curriculum due to lack of resources and time constraints. Head teachers viewed the current education system’s focus on exams and achievement scores as a burden for students. Furthermore, adding oral health education to the curriculum would increase this burden to both teachers and students. Most of the head teachers identified that the current curriculum was designed in such a way that school subjects deemed less important were taught to students at the expense of more significant issues such as oral health. The Tamil Nadu Ministry of Education and Ministry of Health should implement policies to introduce oral health education in Tamil Nadu schools without increasing the burden to teachers and students. The Ministry of Education could review the Samachir Kalvi curriculum to accommodate sufficient time for health and oral health education. A limitation of this study was the general lack of oral health literacy and insufficient knowledge about oral health education among the head teachers. Although the primary researcher asked questions and provided examples of oral health education, most of the head teachers could not answer them beyond their knowledge about routine health check-ups provided at their school. Hence, future research with school teacher participants should include a health literacy knowledge assessment.
Conclusion
A significant issue identified in this study is the lack of effective oral health policies in Tamil Nadu schools, which has caused schools to ignore the placement of oral health education in the curriculum. The dental screenings conducted in some schools were considered ineffective. This study highlighted a considerable number of school students who were not eligible for the Tamil Nadu government’s mid-day meal policy and were still experiencing classroom hunger. Private schools were lacking in the provision of both health and oral health education, and hence, the Government should strengthen the current health promotion policy to involve private schools. The current academic curriculum, which mainly focuses on academic examinations to secure a place at university, was considered a challenge to the implementation of oral health education in Tamil Nadu schools. The Ministry of Education could review the current curriculum by prioritising oral health education without increasing the burden to teachers and students. Future studies should focus on framing an oral health education model for schools in Tamil Nadu by analysing current oral health education strategies in the schools of developed countries.
Footnotes
Acknowledgements
The authors would like to thank all head teachers for participating in this study. Arthi Veerasamy would like to acknowledge the University of Canterbury Doctoral Scholarship which enabled her to undertake a PhD programme and to be able to conduct the field research in India.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.