
Abstract
Objective:
Exercise is beneficial for individuals who have been diagnosed with cardiovascular disease or cancer. Healthcare providers are well placed to discuss exercise with their patients, but their referral practices and the content of exercise recommendations remain unclear.
Method:
Cardiologists and oncologists completed an online survey comprising four closed-ended questions and one open-ended question to assess exercise recommendation and referral practices. Chi-square tests were used to compare the frequency of closed-ended responses, and open-ended responses were coded and analysed using qualitative content analysis.
Results:
Of the 154 surveys, 58 were returned (n = 25; 43.1% cardiologists, and n = 33; 56.9% oncologists). Respondents (Mage = 45.5 ± 11.1) were mostly men (62.1%). The majority of cardiologists (95.8%) and oncologists (78.1%) reported referring patients to hospital-based exercise programmes. In this study, the cardiologists were more likely to refer patients to certified exercise physiologists (χ2(1) = 6.140, p = .021), whereas oncologists were more likely to refer to physical therapists (χ2(1) = 11.764, p = .001).
Conclusion:
Findings reveal that cardiologists and oncologists discussed and recommended exercise to their patients at least some or most of the time; there were differences in the type of exercise professionals they were referred to; and exercise recommendations were variable and infrequently concurred with established guidelines.
Introduction
Cardiovascular disease (CVD) and cancer are the leading causes of chronic disease–related death among adults in the USA (Heron, 2018). Although they are separate diseases with distinct illness trajectories, treatments and side effects, both CVD and cancer have significant personal (e.g. mortality, morbidity) and societal impact (e.g. healthcare system) (Centers for Disease Control and Prevention, 2018). Fortunately, lifestyle factors such as exercise have been shown to improve health-related outcomes among CVD and cancer patients.
Systematic reviews and meta-analyses show that exercise positively impacts many of the negative disease- and treatment-related effects of CVD (Alves et al., 2016) and cancer (Stout et al., 2017). Furthermore, exercise may be protective for future morbidity, co-morbidity and mortality (Li et al., 2016; Reddigan et al., 2011) and has been shown to improve a range of physical (e.g. fatigue, physical functioning, cardiopulmonary health, mobility) and psychological (e.g. depressive symptoms, stress, self-esteem, quality of life) health outcomes for individuals living with CVD or diagnosed with cancer (Lavie et al., 2015; Speck et al., 2010).
As a result of these established benefits, governing bodies such as the American Heart Association (2014) and the American Cancer Society have released exercise guidelines for individuals diagnosed with CVD and cancer (Rock et al., 2012). These guidelines recommend 150 minutes per week of moderate or 75 minutes per week of vigorous aerobic exercise, plus 2 days per week of muscle-strengthening activity. However, studies show that most CVD and cancer patients/survivors are not meeting these guidelines (Gjerset et al., 2011; Tang et al., 2013). Encouraging individuals diagnosed with CVD and cancer to engage in recommended levels of exercise may be particularly challenging, as they often face additional barriers to exercise (compared to the general population), including disease-related physical limitations, and fear or uncertainty about appropriate types and/or the safety of exercise (Bay et al., 2018; Clifford et al., 2018).
Many adults report dependence on their healthcare provider for health-related information and advice and, when unsure or hesitant about starting new programmes, they often consult their healthcare provider first (Salmon and Young, 2009; Street et al., 2009). As a result, healthcare providers can play an influential role in promoting exercise among their patients (Balady et al., 2011; Calfas et al., 1996; Jones et al., 2004). The influence of healthcare providers on patients’ exercise behaviour has been demonstrated in the general population (Orrow et al., 2012; Swinburn et al., 1998) and individuals diagnosed with CVD and cancer (Jones et al., 2004; Tsui et al., 2012). Thus, healthcare providers, specifically those who specialise in care for CVD and cancer (i.e. cardiologists and oncologists), may be in an ideal position to promote exercise to their patients.
System-level structures and referral pathways for exercise rehabilitation have been part of treatment of CVD for many decades (Mampuya, 2012). Calls for exercise as part of standard care for cancer treatment have only recently been proposed (Cormie et al., 2018; Mina et al., 2018), with many suggesting the ‘cardiac-rehabilitation’ model be used as paradigm for oncology rehabilitation (Hubbard et al., 2016). In the USA, there still remains variability in the provision of exercise as part of cancer rehabilitation services (Stubblefield et al., 2013) and uncertainty as to how consistently cardiologists are referring to available exercise-based rehabilitation services.
Despite the important role that cardiologists and oncologists could play to promote exercise among their patients, previous studies have found mixed results with regard to the prevalence of exercise promotion (i.e. discussion, recommendation, and referral) (Dahhan et al., 2015; Kenzik et al., 2016; Nyrop et al., 2016). Previous studies have also examined barriers to exercise promotion, for example, lack of knowledge of appropriate exercise guidelines (Dahhan et al., 2015; Moradi et al., 2011; Nadler et al., 2017; Spellman et al., 2014) and/or referral pathways (Ghisi et al., 2013; Nadler et al., 2017), and various reviews have provided suggestions to enhance healthcare providers’ exercise referral (Arena et al., 2012; Eaton and Menard, 1998; Pender et al., 1994). However, to date, it remains unclear whether cardiologists and oncologists are discussing and recommending exercise with similar frequency, to where/whom they are referring their CVD and cancer patients for exercise, and what kind of exercise recommendations are currently being made.
Therefore, the purpose of this study was to (1) describe and compare the frequency of discussing and providing exercise recommendations among cardiologists and oncologists, (2) compare the types of exercise programmes and professionals to which cardiologist and oncologists refer their patients, and (3) explore the content of exercise recommendations.
Method
Participants and procedure
Following approval from the Colorado State University institutional review board (IRB) for the protection of human subjects (IRB #17-7524H), medical directors at local cardiology and oncology clinics were contacted and asked to email a link to a secure online survey to the practicing interventional and surgical cardiologists, or medical and radiation oncologists at their clinic. Upon clicking the link, interested cardiologists and oncologists were taken to an informed consent page. After providing informed consent, respondents (i.e. cardiologists, oncologists) then gained access to the survey.
Survey
The survey for this study was developed through several steps. First, published studies, which examined similar outcomes were used to create an initial version of the survey (Jones et al., 2005; Park et al., 2015), which was reviewed and revised by one cardiologist and one oncologist. This revised survey was then pilot-tested by an additional cardiologist and oncologist. The final survey comprised questions related to demographic information (e.g. age, sex), frequency of exercise discussion and recommendation, the type of exercise programme or professional patients were referred to and exercise recommendation practices.
Closed-ended questions inquired about the frequency of exercise discussion and recommendation. These were (1) ‘How often do you discuss exercise with your patients?’ Responses were scored on a 5-point Likert-type scale ranging from ‘none of their visits’ to ‘all of their visits’; and (2) ‘What percentage of patients have you recommended should exercise in the past month?’ Responses were scored on a 5-point Likert-type scale ranging from ‘none’ to ‘all’. Closed-ended questions also inquired about the type of exercise programme and exercise professional patients were referred to. These were (1) ‘When you provide a referral to a structured exercise programme, which of the following do you use?’ Response options were ‘hospital-based rehabilitation programme, community-based exercise programme or facility, neither, both’ and ‘other’; and (2) ‘When you refer patients to structured exercise programmes, what type of professionals do you look for?’ Response options were ‘physical therapist, certified exercise physiologist, personal trainer, do not know or not aware of appropriate qualifications’ and ‘depends on patient needs’. For both of these questions, respondents were instructed to select all that apply from the options provided.
Finally, to provide insight into exercise discussion and recommendation, one open-ended question asked, ‘If you recommend exercise to your patients, what is the frequency, intensity, time and type that you recommend?’
Data analysis
Quantitative data were analysed using SPSS (Version 25). Descriptive statistics (e.g. means, standard deviations) were used to describe respondent characteristics, and frequencies were calculated for responses to the closed-ended questions described above. Chi-square tests were used to examine differences in the proportion of cardiologists and oncologists selecting each response for the type of programme and exercise professional patients were referred to. Significance was set at p < .05.
The open-ended response was analysed using qualitative content analysis (Hsieh and Shannon, 2005). The written responses were de-identified and transferred to an Excel spreadsheet. The authors then independently familiarised themselves with the data by reading the responses several times. Following this, responses were assigned codes according to a classification scheme that was developed using knowledge about the content of existing exercise recommendations. The codes were then sorted into broad categories, counted, and summarised descriptively and narratively. This approach was used to better compare/contrast the responses provided by cardiologists and oncologists (Hsieh and Shannon, 2005).
Results
Of the 154 surveys distributed, 58 (n = 25 cardiologists and n = 33 oncologists) were returned, with a 37.7% response rate. Respondents were mostly men (62.1%) and between 32 and 83 years of age (M = 45.5 ± 11.1). Time in practice was nearly evenly split between ⩽10 years (55.2%) and ⩾10 years (44.8%), and most (67.2%) reported no formal education related to exercise during their medical training. Participant characteristics are displayed in Table 1.
Participant characteristics.
The majority of cardiologists (n = 20, 80.0%) reported that they discussed exercise with their patients at ‘some’ or ‘most’ of their visits. Among oncologists, most (n = 24, 72.8%) reported that they discussed exercise with their patients at ‘few’ or ‘some’ of their visits (see Figure 1). Most cardiologists (n = 19, 79.1%) and oncologists (n = 21, 63.6%) reported that they recommended exercise to ‘some’ or ‘most’ of their patients in the last month (see Figure 2).
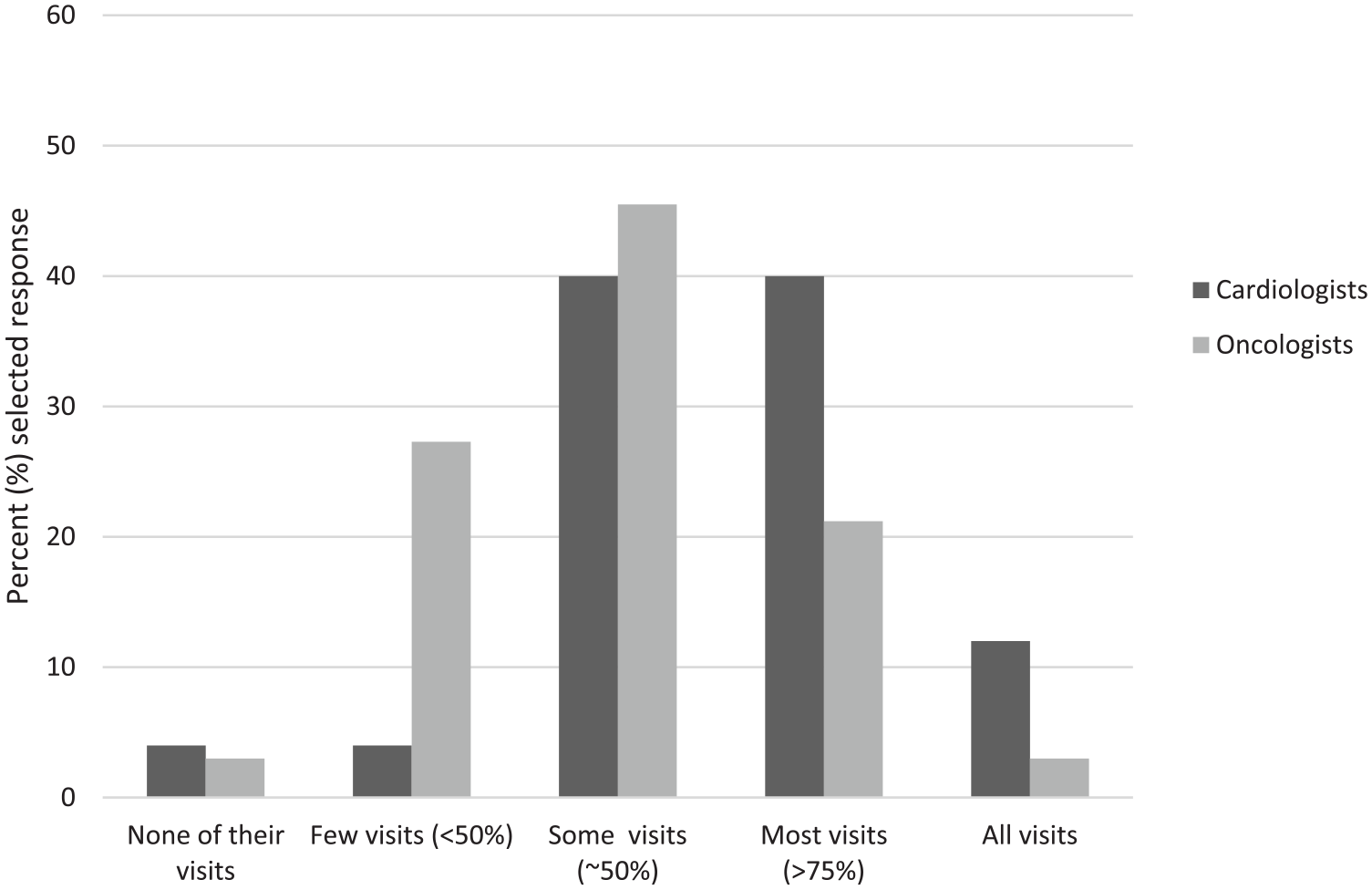
How often do you discuss exercise with your patients?
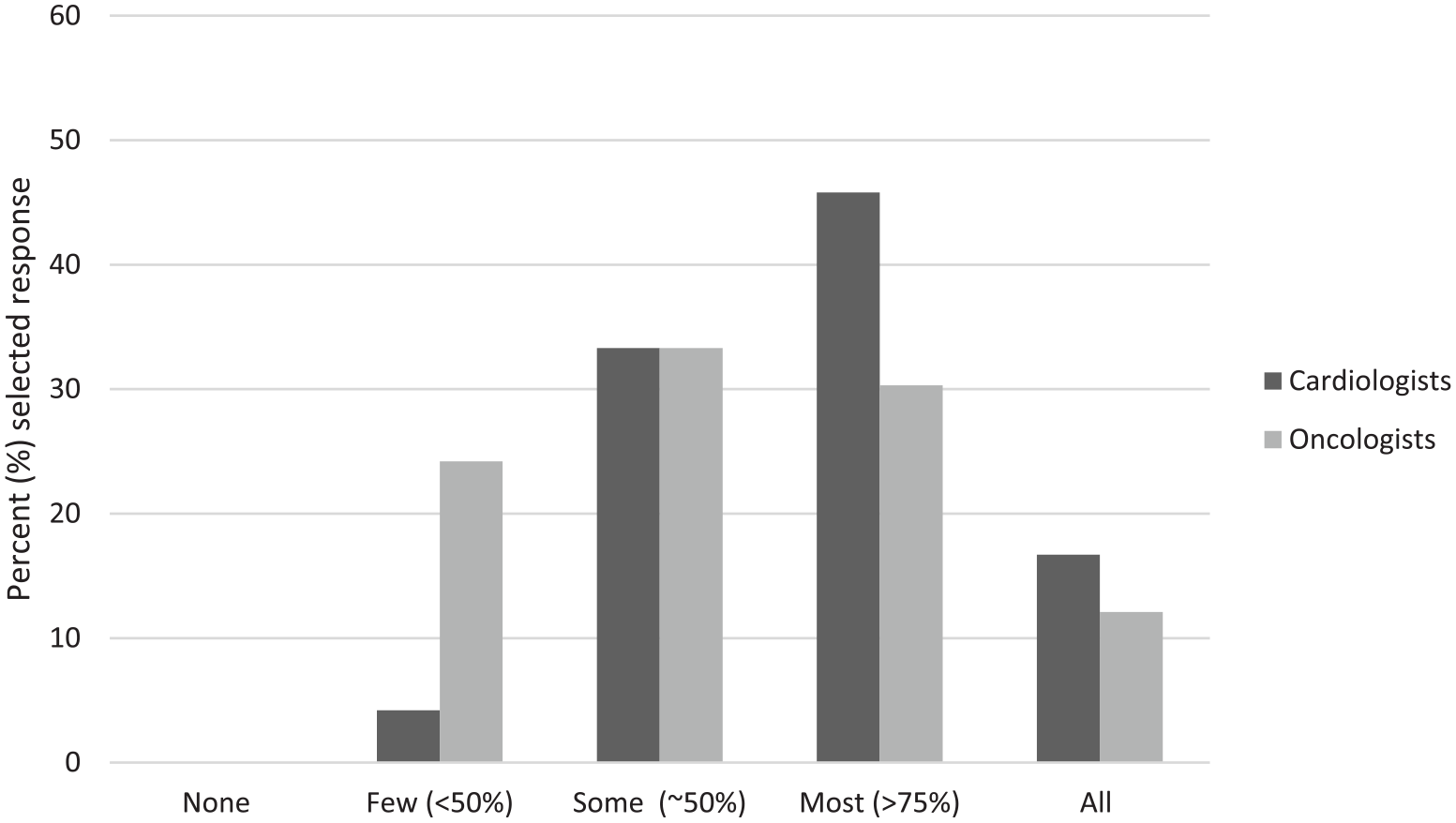
What percentage of patients have you recommended should exercise in the past month?
In terms of the type of exercise programme patients were referred to, the majority of cardiologists (n = 23, 95.8%) reported referring to a hospital-based exercise programme, and about half reported referring to a community-based programme (n = 13, 54.2%). This pattern held for oncologists, as the majority (n = 25, 78.1%) also reported referring their patients to a hospital-based exercise programme, and over two-thirds reported referring to a community-based programme (n = 22, 68.8%) (see Figure 3). There were no significant differences in the type of exercise programme patients were referred to between cardiologists and oncologists.
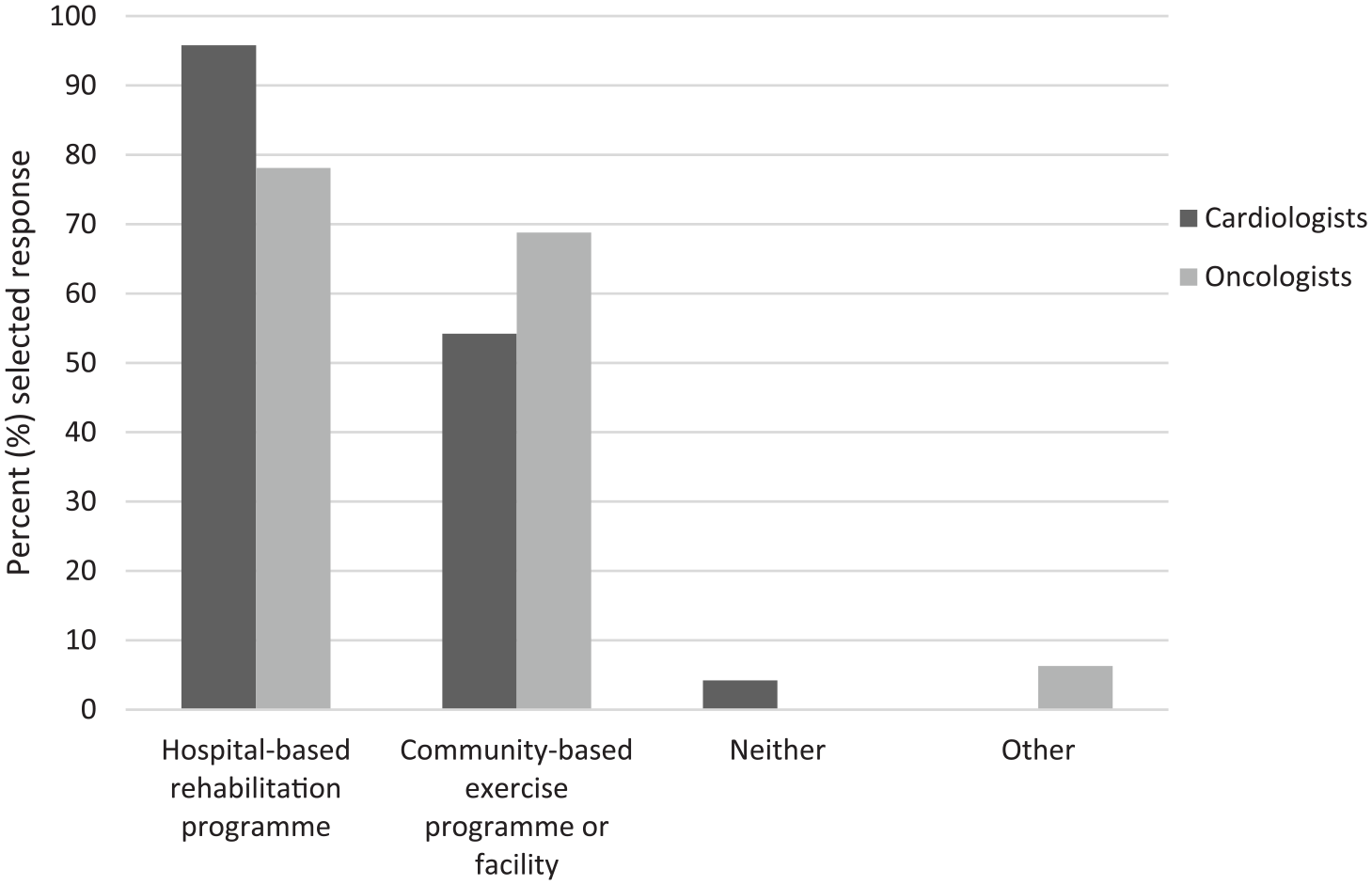
When you provide a referral to a structured exercise programme, which of the following do you use?
With regard to the type of exercise professional patients are referred to, cardiologists most frequently reported referring to a certified exercise physiologist (n = 12, 50%) or ‘elsewhere depending on patient needs’ (n = 11, 45.8%). Oncologists most frequently reported referring to a physical therapist (n = 20, 62.5%) or ‘elsewhere depending on patient needs’ (n = 15, 46.9%). Cardiologists were significantly more likely than oncologists to refer to certified exercise physiologists (χ2(1) = 6.1, p = .013), and oncologists were more likely than cardiologists to refer to physical therapists (χ2(1) = 11.8, p = .001) (see Figure 4).
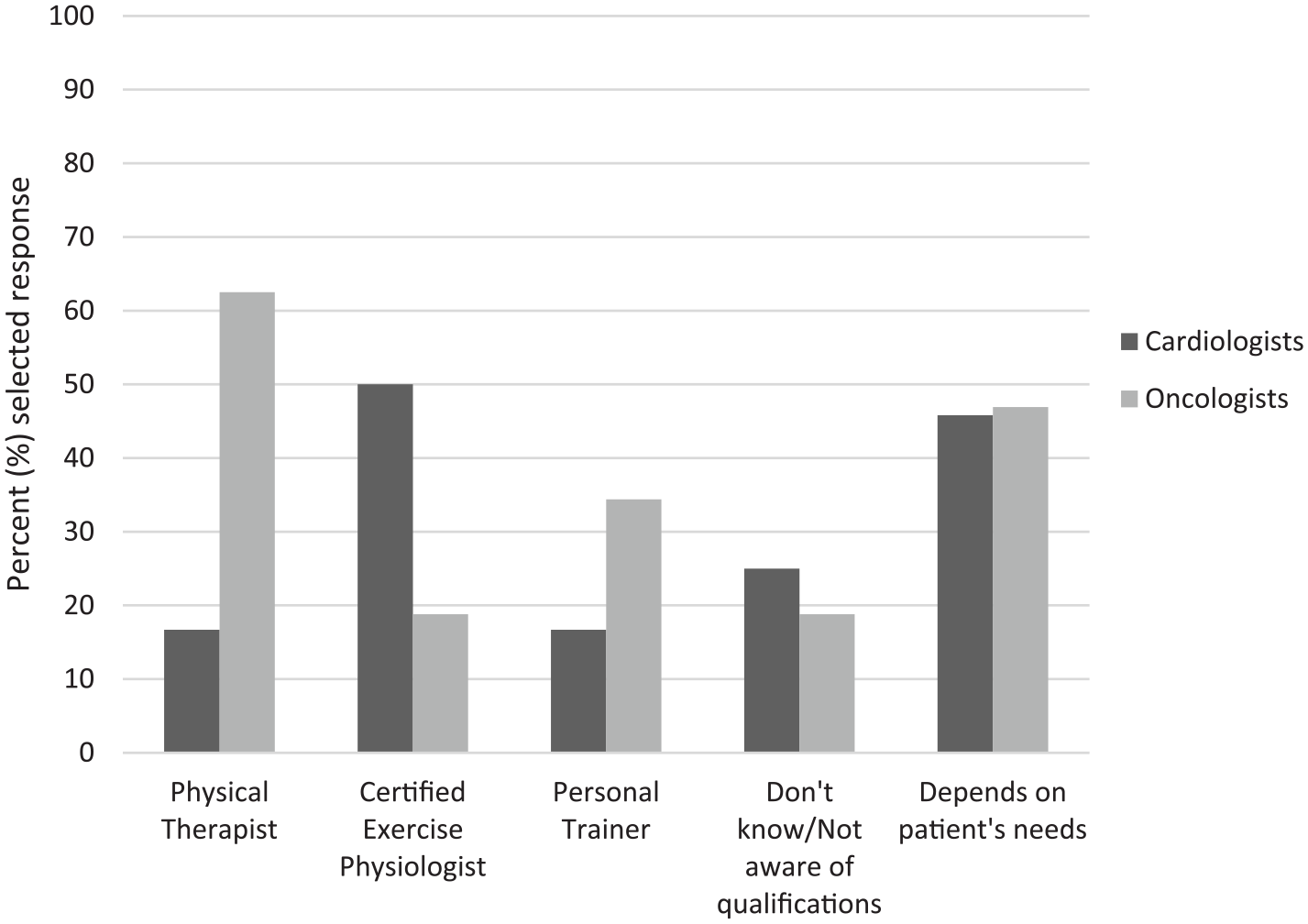
When you refer patients to structured exercise programmes, what type of professionals do you look for?
Of the 58 survey respondents, 53 completed the open-ended question, ‘If you recommend exercise to your patients, what is the frequency, intensity, time and type that you recommend?’ Responses suggest that few healthcare providers deliver recommendations that are consistent with current exercise guidelines and that the content of what is being discussed with patients is highly variable. Specifically, only one respondent (female oncologist) provided recommendations that were consistent with both aerobic exercise and strengthening guidelines: 30 minutes a day of moderate intensity aerobic exercise 5-6 days a week. Also suggest strength training and flexibility training 2-3 times a week.
When considering just aerobic exercise, 18 (n = 9 cardiologists, n = 9 oncologists) provided recommendations consistent with current guidelines, whereas only 8 (n = 2 cardiologists, n = 6 oncologists) mentioned muscle-strengthening activities in their recommendation. Recommendations that differed from guidelines did so primarily based on exercise intensity and time. For example, a male oncologist wrote, ‘30 minutes three times a week moderate intensity’. A male cardiologist stated, Most days of the week at least 20 minutes of moderate intensity exercise; 2-3 days of resistance type training/weights. Ex rx [exercise prescription] modified according to pt [patient] abilities, comorbid illness, etc.
Regardless of whether recommendations were similar to current exercise guidelines, 16 (n = 7 cardiologists and n = 9 oncologists) indicated they adopted a patient-centred and individualised approach when recommending exercise (e.g. considering age, disease-related barriers, physical activity history). For example, a male cardiologist wrote, I take care of HF [heart failure] patients, so I usually recommend brisk walking, water aerobics, or whatever they can tolerate.
Finally, though not explicitly asked within the open-ended question, three oncologists reported that they referred their patients to cancer-specific rehabilitation or exercise services. However, within these three respondents, the service varied, as illustrated by a male oncologist, when he wrote, It varies greatly depending on multiple factors. My general recommendation is to see our Oncology Physiotherapy people.
Discussion
The purpose of this study was to compare the referral patterns and frequency of exercise promotion between cardiologists and oncologists and to gain insight into the content of their exercise recommendations. Similar numbers of cardiologists and oncologists recommended exercise to their patients, and cardiologists reported discussing exercise more regularly than oncologists. Both cardiologists and oncologists primarily referred patients to hospital-based exercise programmes, but cardiologists were more likely to refer patients to a certified exercise physiologist, and oncologists were more likely to refer patients to a physical therapist. Qualitative analyses revealed that exercise recommendations were variable, rarely included mention of muscle-strengthening activities and, in general, were inconsistent with the current exercise guidelines for adults and cancer survivors (Piercy et al., 2018; Rock et al., 2012). Furthermore, only approximately one-third of respondents considered individual factors (e.g. comorbidities, treatment status, exercise history, barriers) when making their recommendations.
Findings are promising for those working in the field of oncology, suggesting that despite cardiology having decades of work integrating exercise-based rehabilitation, it seems both professions frequently discuss and recommend exercise to their patients. However, qualitative findings highlight that the exercise recommendations provided by cardiologists and oncologists are variable and typically do not correspond with established exercise guidelines. There may be several reasons that these providers’ recommendations do not match exercise guidelines. These reasons could include lack awareness of the guidelines, deficiencies in knowledge translation or ‘uptake’ of the guidelines by providers (Nadler et al., 2017), not enough time to devote to exercise promotion, concerns regarding patient comorbidities, or reliance on clinical judgement or previous experiences to provide exercise recommendations rather than general guidelines. Including qualified exercise professionals (e.g. certified exercise physiologists) as part of comprehensive treatment teams could complement the exercise recommendations provided by oncologists and cardiologists, as qualified exercise professionals possess in-depth knowledge of exercise recommendations and have the skills, time and ability to tailor exercise programmes to individual needs (i.e. disease/medical limitations, physical activity history, personal preference, etc.). Although researchers and exercise professionals often advocate for individualised and tailored exercise programming (American College of Sports Medicine [ACSM], 2017; Burr et al., 2012; Twomey et al., 2018; Van der Leeden et al., 2018), the best way to amalgamate this into clinical practice (e.g. infrastructure, costs, insurance coverage) remains in question.
This study also found that cardiologists were more likely to refer patients to a certified exercise physiologist, and oncologists were more likely to refer patients to a physical therapist. Whether this was due to lack of systems in place (i.e. availability of hospital-based cancer exercise programmes delivered by qualified exercise professionals) or because oncologists are unaware of qualified exercise professionals’ credentials to work with cancer patients/survivors (e.g. ACSM’s Cancer Exercise Trainer certification) is unclear. Conversely, considering the use of physical therapists in early models of cardiac rehabilitation, this may also simply indicate the natural progression of integrating qualified exercise professionals into standard of care for cancer treatment (DeLisa, 2001; Mampuya, 2012).
Limitations
This study was not without limitations. Specifically, based on the nature of this study, participants may have self-selected (i.e. those interested in exercise were more likely to participate). As a result, findings may be overly optimistic. Similarly, all results were based on self-report, which is susceptible to recall bias and priming to the topic, which may have resulted in more desirable responses. Future studies could use a chart review approach rather than a survey to gather information about exercise discussion/recommendation or referral; however, this would be contingent on information being reliably recorded in the patient chart and may not capture the specifics of the exercise recommendation or to where/whom patients are referred. Moving forward, researchers may wish to use closed-ended questions related to exercise recommendation content or, incorporate a larger qualitative component via interviews or focus groups. This approach would enable quantitative comparisons between healthcare provider’s exercise recommendations and established guidelines and provide deeper, more thorough information to better understand the decisions that physicians are making regarding exercise recommendations and referral. Finally, the study was limited to interventional and surgical cardiologists, and medical and radiation oncologists in Northern Colorado. Thus, findings may not be generalisable to healthcare providers in other regions or to other healthcare providers working with this patient population (e.g. nurses, physician assistants). Notwithstanding these limitations, the strengths of this study include the complementary nature of both quantitative and qualitative information, and unique perspectives acquired from both cardiologists and oncologists, which enabled comparisons and contrasts.
Conclusion
This study found that oncologists and cardiologists were discussing and recommending exercise to their patients at least some or most of the time, elucidated differences in the type of exercise professional these physicians were referring to, and found that exercise recommendations infrequently concurred with established guidelines. These results provide insight into the variability in referral to available services and gaps in knowledge of exercise guidelines. Future studies should seek to further understand the discordance between established exercise guidelines and recommendations presented by healthcare providers, as well as the facilitators and barriers for referring patients to exercise professionals. Engaging in regular exercise is challenging for the majority of US adults, and individuals diagnosed with CVD and/or cancer may benefit greatly from healthcare providers’ efforts to support their exercise efforts. Finding ways to improve the uptake of exercise guidelines by healthcare providers and more fully explicating the role of the exercise professional may enhance exercise promotion for CVD and cancer patients.