
Abstract
Objective:
The purpose of this study was to evaluate whether participation in a community event developed using Health Belief Model constructs increased intention to follow the American Academy of Paediatrics Safe Sleep Guidelines for infants.
Design:
Observational cohort study.
Setting:
Safe Sleep Community Baby Showers held between Spring 2015 and Spring 2019.
Method:
Women attending the Safe Sleep Community Baby Showers completed pre- and post-assessments measuring intentions based on constructs derived from the Health Belief Model.
Results:
Following the Safe Sleep Community Baby Showers, significantly more of the 812 participants demonstrated positive changes in Health Belief Model constructs, including beliefs about severity and susceptibility (infant is at risk, sleeping with infant can cause death, loose blankets can cause death), benefits (putting infant alone, on back in crib will help protect), barriers (infant will [not] choke on back) and self-efficacy (know what to do). Two barriers did not result in significant change: room for crib (cot) in parents’ room and able to keep infant warm without blankets. Most reported intention to only place infant supine (99%), in safe sleep locations (97.8%) and to include only safe items (86.2%; all p < .001).
Conclusion:
Structuring a community event based on the Health Belief Model resulted in significant increases in participants intending to follow the AAP Safe Sleep Guidelines. Further work is needed to address barriers around blankets and room sharing without bed sharing. Safe Sleep Community Baby Showers can impact Health Belief Model constructs related to the AAP Safe Sleep Recommendations, which may in turn impact behaviour.
Introduction
Sleep-related deaths are the number one cause of death for infants between 28 days and 1 year of age (Moon and Task Force on Sudden Infant Death Syndrome, 2016). Sleep-related deaths include those attributed to sudden infant death syndrome (SIDS) and accidental suffocation or strangulation in bed (ASSB). The American Academy of Paediatrics (AAP) provides guidelines for parents and caregivers to reduce the risk of sleep-related infant deaths, including placing infants alone, on their back, and in a clutter-free crib or cot (Task Force on Sudden Infant Death Syndrome, 2016). However, sleep-related deaths continue to affect nearly 3,600 infants in the USA each year (Centers for Disease Control and Prevention (CDC), 2019].
In an effort to reduce sleep-related deaths, the Kansas Infant Death and SIDS (KIDS) Network partnered with the Wichita Black Nurses Association in 2011. Together, this partnership developed Safe Sleep Community Baby Showers (Ahlers-Schmidt et al., 2014) to promote the AAP Safe Sleep Guidelines (Moon and Task Force on Sudden Infant Death Syndrome, 2016) in communities with high infant mortality rates. Group events were selected for the programme as group educational luncheons for pregnant women had been shown not only to increase knowledge of important information, but also to enhance self-esteem, reduce isolation and promote peer bonding (Canuso, 2003). Group prenatal education has also been successful in increasing breastfeeding by African American women when compared to those receiving individual care (Klima et al., 2009). The planning committee also hoped the group event format would engage high-risk women who were not otherwise connected with services (e.g. prenatal care) as community events might be perceived as less intimidating than individual services (e.g. home visitation programmes).
The goal of the Safe Sleep Community Baby Showers was to use the culture and tradition of such events (Moon et al., 2016) to engage pregnant and recently delivered women. Safe Sleep education at these events was conducted using the 10 minute video ‘ABCs of Safe Sleep’, and presentations by local physicians and community programmes. In addition, a member of the Wichita Black Nurses Association provided a Safe Sleep Crib Demonstration, where a nurse would illustrate how to use a portable crib as a safe sleep environment. Following presentations, participants visited booths to learn about local programmes and resources related to maternal and infant health. Both Safe Sleep Community Baby Showers held in neighbourhoods (e.g. community centres and churches) and at resident physician clinics resulted in significant increases in safe sleep knowledge and intention (Ahlers-Schmidt et al., 2016), although the clinic-based Baby Showers attracted fewer participants from priority groups (e.g. low-income, non-Hispanic Black).
In 2015, the KIDS Network and partners decided to adjust the format of the showers to better meet the needs of participants and community partners. The planning committee, comprised of community members, wanted to revise the event to enhance behaviour change. Funding and staffing limitations, in addition to prior failed attempts to collect behavioural data following the Safe Sleep Community Baby Showers (<10% response rate; unpublished data), suggested follow-up for actual behaviours may not be feasible. In addition, a location change for the events made showing the video challenging. Finally, complaints had been received from both participants and community partners indicating difficulties receiving and conveying information during visits to the booths.
The planning committee decided to restructure the event to (1) better fit the available space, (2) address concerns and (3) enhance the likelihood participants would follow the safe sleep recommendations for their infants. In consequence, the planning committee updated the Safe Sleep Community Baby Shower activities based on the Health Belief Model theory of behaviour change (Becker, 1974; Janz and Becker, 1984). This theory holds that to affect behaviour change, one must address the following six constructs: (1) severity, (2) susceptibility, (3) benefits, (4) barriers, (5) cues to action and (6) self-efficacy. The Health Belief Model was selected after reviewing multiple theory options as it is often applied to prevention-related health concerns, where those at risk are asymptomatic and the intervention goal is to reduce risk factors (Carpenter, 2010). Local foetal infant mortality review (FIMR) data suggested families who experienced sleep-related death had low perception of susceptibility, high barriers to implementation and low self-efficacy. In addition, Health Belief Model constructs have been recommended for safe sleep promotion previously (Moon et al., 2016), and safe sleep interventions have often had limited success due to barriers in implementing the guidelines (Salm Ward and Balfour, 2016). Planning committee members ensured that each of the constructs was addressed (Table 1).
Health Belief Model (HBM) Constructs and Safe Sleep Application.
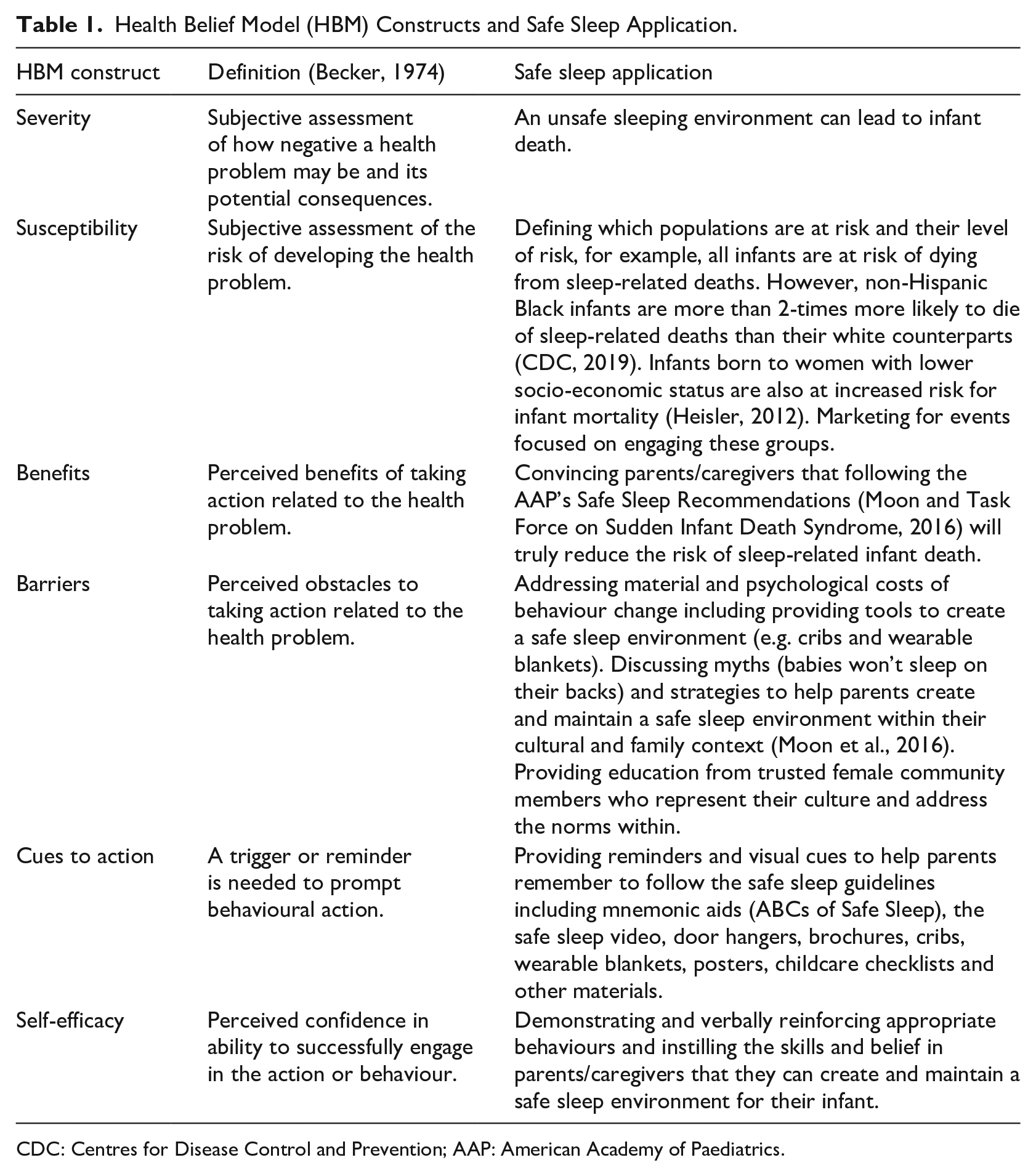
CDC: Centres for Disease Control and Prevention; AAP: American Academy of Paediatrics.
Maintaining the celebratory feeling of a baby shower was also a priority. Planning committee members were encouraged to think about amusement park strategies to reduce the perception of wait time and engage participants who were in the queue to enhance the festive feeling of the event.
The purpose of this study was to evaluate whether participation in a Safe Sleep Community Baby Shower impacted Health Belief Model constructs related to the AAP Safe Sleep Guidelines (Task Force on Sudden Infant Death Syndrome, 2016).
Methods
Participants
Safe Sleep Community Baby Showers were held twice a year (in March and October) between Spring 2015 and Spring 2019. Events were promoted to pregnant and recently delivered women through fliers distributed to churches serving predominantly non-Hispanic Black congregations, clinics serving low-income women (e.g. faculty/resident clinics, Federally Qualified Healthcare Centres), maternal and child health programmes (e.g. prenatal education programmes, home visitor programmes, the women, infant and children [WIC] programme), social media posts (e.g. Facebook), and through partner organisations such as the local Alumnae Chapter of Delta Sigma Theta Sorority, Inc. Women were encouraged to bring support people (e.g. spouse, mother, aunt or friend) to attend the event with them. Events were promoted as occurring between 11 a.m. and 12:30 p.m., with sessions starting every 15 minutes.
Only pregnant or recently delivered women were eligible to participate in data collection for the programme. Participants for this study are limited to a convenience sample of English-speaking women who provided programme data at Safe Sleep Community Baby Showers, as Spanish-language Safe Sleep Community Baby Showers utilised a different format and are reported elsewhere (Ahlers-Schmidt et al., available on application to the authors).
Instrument
Data collection tools from previous Safe Sleep Community Baby Showers (Ahlers-Schmidt et al., 2014, 2016) were modified to reflect the current literature and assess changes to the events. Both pre- and post-assessments were reviewed for face validity by the Medical Society of Sedgwick County’s Safe Sleep Taskforce, which included obstetric, family medicine and paediatric physicians, researchers and other members. Participants were asked 11 questions developed around the Health Belief Model constructs. Eight items addressing severity, susceptibility, benefits, barriers and self-efficacy were included on both the pre- and post-assessments. An additional three items regarding confidence in following the AAP recommendations were included on only the post-assessment to further assess self-efficacy; response options were ‘less confident’, ‘no change’, and ‘more confident’. Event satisfaction was measured on the post-assessment. Most participants were able to complete the forms in 10 minute or less.
Procedures
Pregnant or recently delivered women were greeted by members of the local Alumnae Chapter of Delta Sigma Theta Sorority, Inc. when they arrived at the Safe Sleep Community Baby Shower. Sorority members asked the attendees to complete the pre-assessment. Attendees were also given blank participant self-referral cards to populate with their information (name, email, phone number). Once complete, the woman was assigned to a ‘tour group’. Each tour group consisted of three to five participants and their support people (no more than eight people per group). A trained volunteer was assigned as the tour guide for the group. The tour guide led the group to 10 to 12 vendor or education booths (e.g. breastfeeding promotion, tobacco cessation, home visitor services) in a predefined order. Each booth gave a brief (3–5 minute) presentation and provided handouts to the small groups of participants. Women who desired more information or to enroll in a programme provided the vendor their self-referral card.
After visiting all booths, the tour group participated in a Safe Sleep Crib Demonstration facilitated by members of the Wichita Black Nurses Association or a KIDS Network certified Safe Sleep Instructor (Ahlers-Schmidt et al., 2017, 2019). The Safe Sleep Crib Demonstration included a safety-approved portable crib, doll, pacifier and wearable blanket which were used to demonstrate a safe sleep environment (doll in wearable blanket, on back, in crib, with no other objects except a pacifier). Additional items (blanket, burp cloth, pillow, hat, stuffed animal, positioner, diaper and wipes) were present and the instructor described why each item was a risk factor for sleep-related death. The instructor also shared strategies for removing the item from the sleep environment. For example, replacing loose blankets with warmer clothing or a wearable blanket. The Safe Sleep Crib Demonstration was not time limited and participants were encouraged to make sure all their infant sleep safety questions were answered.
Following the Safe Sleep Crib Demonstration, participants completed the post-assessment. Participants then received a free safety-approved portable crib and wearable blanket, as well as safe sleep education handouts and materials (e.g. door hangers). These items were intended to address the cues to action construct of the Heath Belief Model. Participants also had the opportunity to receive safety-approved items as door prizes which were donated by the local Alumnae Chapter of Delta Theta Sorority, Inc. Refreshments were served to maintain the festive atmosphere, unite and strengthen community bonds and foster a sense of community. Approximate cost per pregnant or recently delivered woman at the events was $100. A variety of foundation grants, KIDS Network fundraisers and donations were used to cover these costs. This project was reviewed by University of Kansas School of Medicine-Wichita Human Subjects Committee.
Analysis
Pre- and post-data were collected, deidentified and entered into a secure database by programme staff. This de-identified programme data were provided to the evaluation team for secondary data analysis regarding the Health Belief Model constructs. Descriptive statistics were summarised using frequencies and percentages. Univariate comparisons between pre- and post-responses were made using McNemar’s test for paired dichotomous variables. For Health Belief Model items that did not significantly change, chi-square analyses were conducted with demographic variables. In order to estimate the measure of the counts of the discordant pairs, we calculated the McNemar odds ratio statistic and corresponding 95% confidence interval (CI) using SAS programme. All statistical tests used α = .05.
Results
Between Spring 2015 and Spring 2019, nine Safe Sleep Community Baby Showers were held in Sedgwick County, Kansas. During this time 1,273 pregnant or recently delivered women completed the pre- and post-assessments. Of those, 461 were excluded due to selecting Spanish as primary language. The remaining 812 women were included in the analyses.
Demographics
Participants identified as non-Hispanic Black (n = 246; 30.4%), non-Hispanic White (n = 246; 30.4%) or Hispanic (n = 203; 25.1%). The highest proportions were single (n = 385; 47.9%) with a high school diploma or GED (n = 330; 41.0%). At the time of the Safe Sleep Community Baby Showers, the majority reported having Medicaid (n = 467; 58.1%) as their primary payer and receiving prenatal services from a private provider’s office (n = 343; 42.8%) or hospital clinic (n = 203; 25.3%) (Table 2).
Safe Sleep Community Baby Shower Participants Characteristics (N = 812).
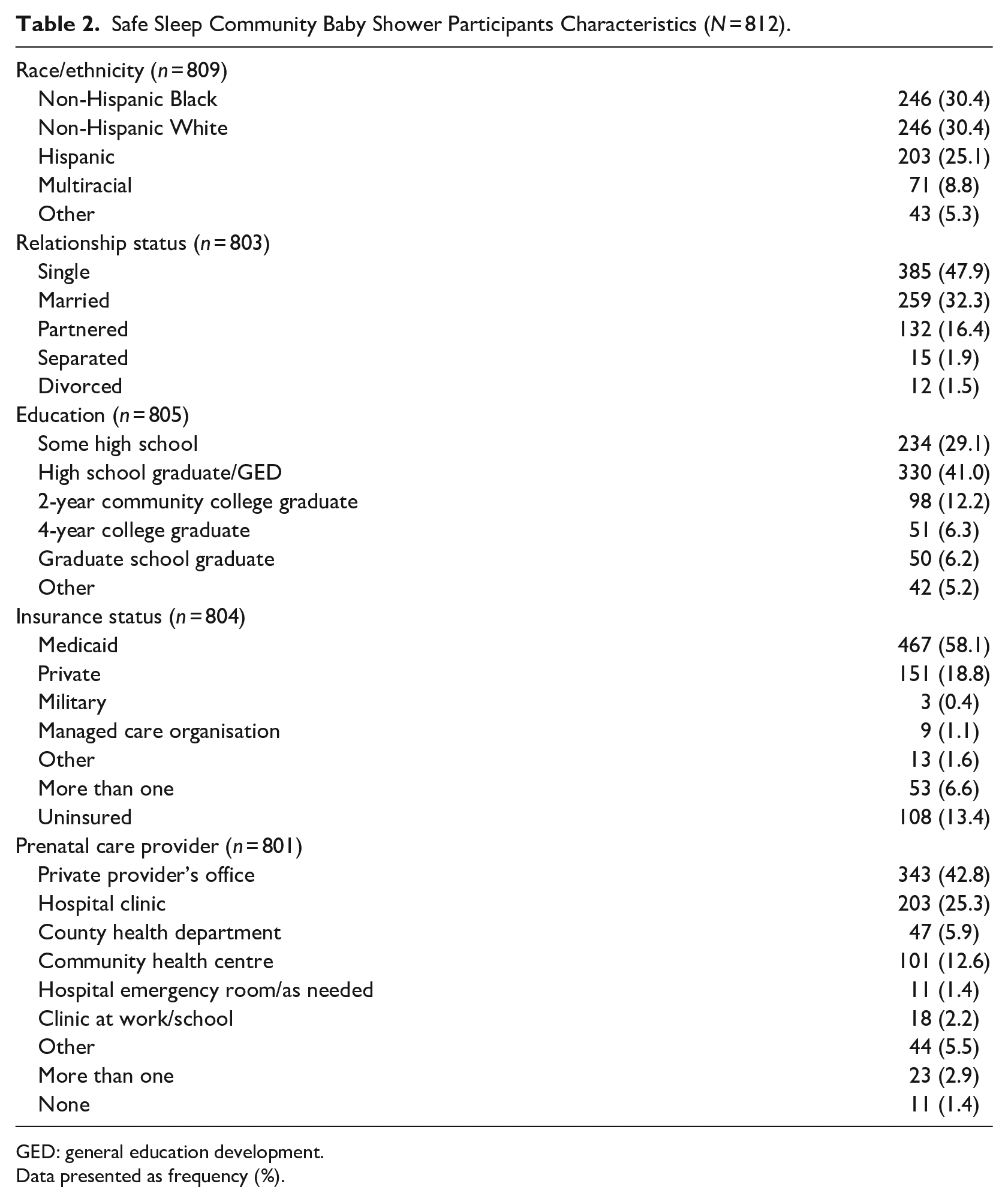
GED: general education development.
Data presented as frequency (%).
Changes in health belief model constructs
Following the Safe Sleep Community Baby Showers, significant changes in beliefs were reported between pre- and post-surveys in the desired direction for severity and susceptibility (infant is at risk, sleeping with infant can cause death, loose blankets can cause death), benefits (putting infant alone, on the back in crib will help protect), barriers (infant will [not] choke on back), and self-efficacy (know what to do) (all p < .001) (Table 3).
Changes in Beliefs Regarding Sleep Risk and Safe Sleep Practices (N = 812).
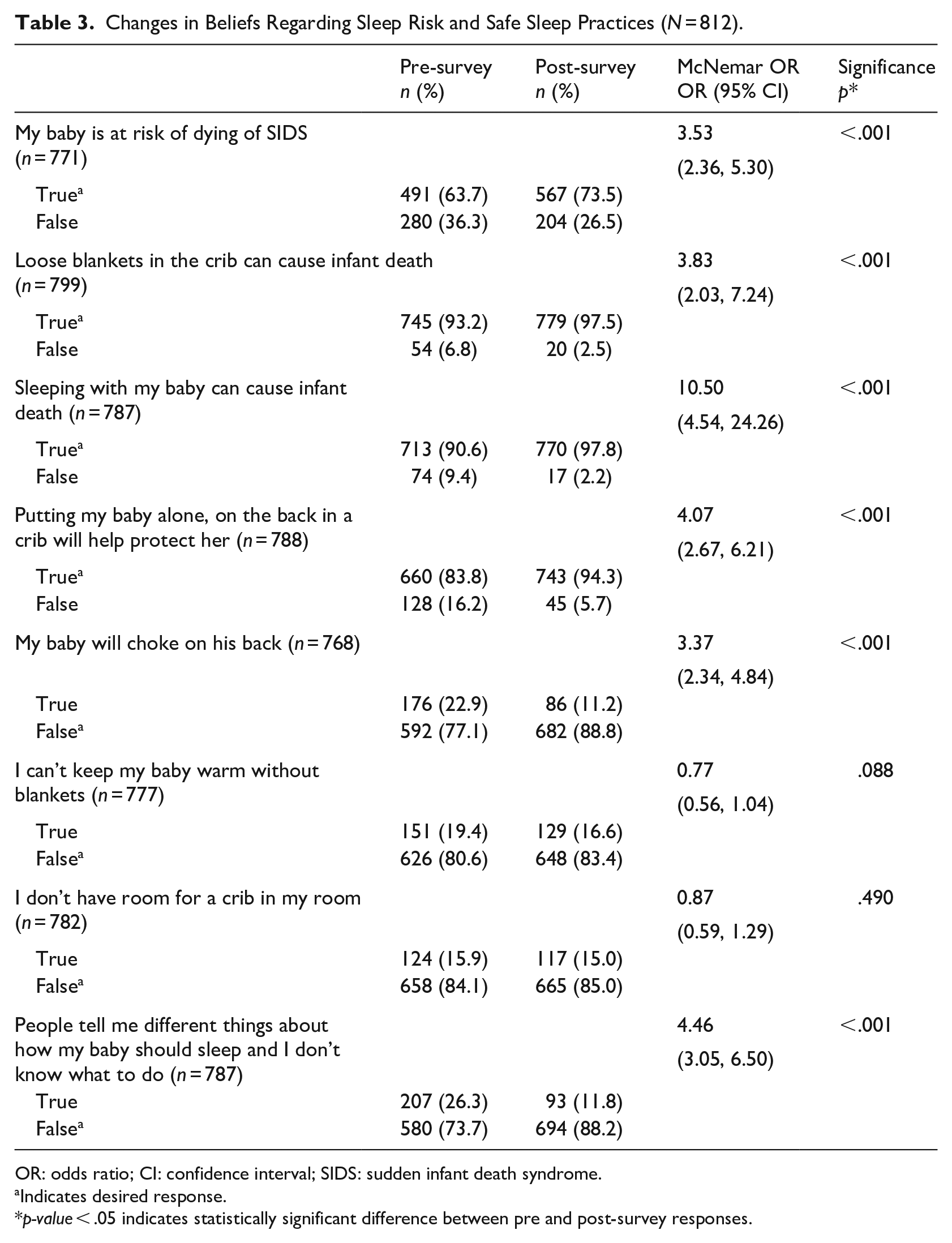
OR: odds ratio; CI: confidence interval; SIDS: sudden infant death syndrome.
Indicates desired response.
p-value < .05 indicates statistically significant difference between pre and post-survey responses.
Significant changes were not seen regarding the barriers of keeping infant warm without blankets and having room for a crib in the mother’s room (p > .05). Participants who reported they could not keep their infant warm without a blanket, were significantly more likely to be Hispanic or non-Hispanic Black (versus non-Hispanic White), have less than a high school diploma/GED (versus 2 year college or higher), be uninsured or on Medicaid (versus privately insured) and receive prenatal services at a hospital clinic or county health department (versus private provider’s office). Participants who reported they did not have room for a crib in their room were significantly more likely to be married (versus single or partnered), on Medicaid (versus other or uninsured) and receiving prenatal care at a private provider’s office (versus hospital clinic) or hospital clinic (versus county health department).
On the post-assessment, the greater proportions of participants reported increased self-efficacy in terms of getting infant to sleep on the back (n = 735; 91.5%), having infant sleep in same room, but separate bed (n = 702; 87.9%) and keeping loose blankets out of the crib (n = 688; 86.2%).
Changes in safe sleep knowledge and intentions
Prior to the Safe Sleep Community Baby Showers, 645 (80.4%) participants reported they would place their infant only on the back to sleep (Table 4). Of the 157 (19.6%) who failed to endorse back only to sleep, prone (n = 24; 15.3%), side (n = 31; 19.7%), multiple positions (46; 29.3%) and not sure (n = 56; 35.7%) were reported. When asked about anticipated sleep locations, 647 (80.4%) reported they would place their infant only in a safe location (i.e. crib, portable crib or bassinet). Of the 158 (19.6%) who did not identify safe location(s) only, participants reported plans to use an adult bed (n = 81; 51.3%), swing or car seat (n = 28; 17.7%), and do not know/not sure (n = 52; 32.9%). When asked about items already in their infant’s sleep area or that they planned to get for their infant’s sleeping area, 405 (55.4%) reported only safe items (i.e. firm mattress, fitted sheet or wearable blanket). Unsafe items reported by the remaining 326 (44.6%) participants included loose blankets (n = 194; 59.5%), bumper pads (n = 113; 34.7%) and cushions/pillows/nursing pillows (n = 111; 34.0%). Only 494 (68.7%) intended to discuss safe sleep with others who may put their infant down to sleep.
Participant Changes in Safe Sleep Knowledge and Intentions (N = 812).
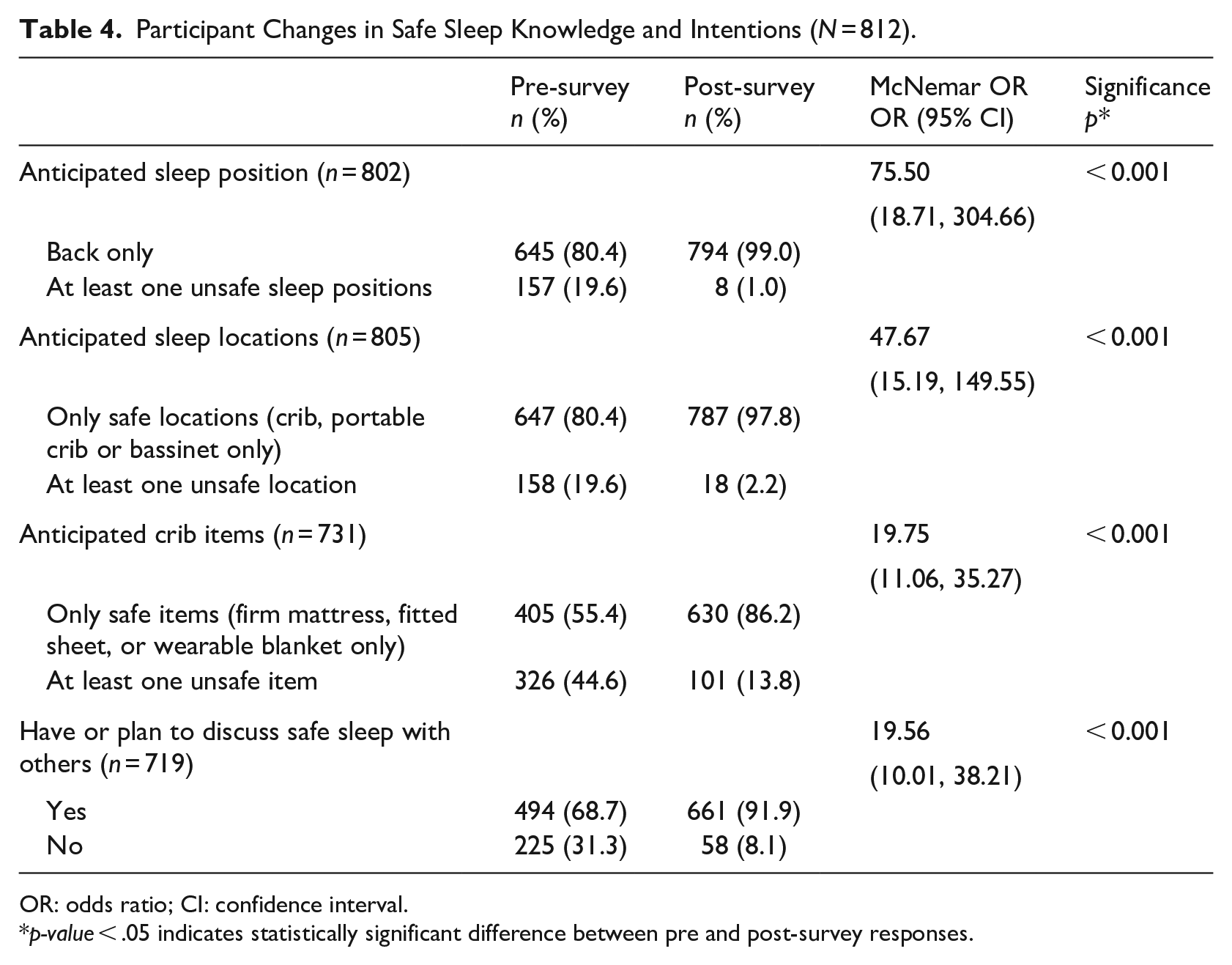
OR: odds ratio; CI: confidence interval.
p-value < .05 indicates statistically significant difference between pre and post-survey responses.
Following the events, participants demonstrated a significant increase in intention to follow recommended safe sleep practices. Almost all (n = 794; 99%) reported they intended to place the infant on their back to sleep (p < .001). The 8 (1.0%) remaining participants planned to use prone (n = 3; 37.5%), side (n = 2; 25.0%), multiple positions (n = 2; 25.0%) or were still unsure (n = 1; 12.5%). Most (n = 787; 97.8%) also intended to place the infant to sleep in only a safe sleep location (p < .001). Of the remaining 18 (2.2%), an adult bed (n = 7; 38.9%), swing or car seat (n = 4; 22.2%), and don’t know/not sure (n = 7; 38.9%) were reported. With regard to objects in the sleep environment, 630 (86.2%) intended to include only safe items (p < .001). The remaining participants (n = 101; 13.8%) still intended to have loose blankets (n = 37; 36.6%), bumper pads (n = 36; 35.6%) and cushions/pillows/nursing pillows (n = 24; 23.8%) in the sleep environment. Most (n = 661; 91.9%) planned to discuss safe sleep with others after the Safe Sleep Community Baby Shower (p < .001).
If they had not received a portable crib at the event, 166 (20.4%) participants would have had their infant sleep in an unsafe location. The most common unsafe sleep locations reported were adult bed (n = 109; 65.7%), infant swing or car seat (n = 17; 10.2%), sofa (n = 5; 3.0%) and other (n = 30; 18.1%).
Participant satisfaction
Overall, satisfaction with the events was high. The majority of participants reported being very satisfied (n = 680; 85.1%) or satisfied (n = 92; 11.5%) with a small portion reporting neutral (n = 13; 1.6%) or very dissatisfied (n = 14; 1.8%). Comments from those who indicated very dissatisfied included ‘information is good and my baby will be safe’ and ‘very dissatisfied because it taught me stuff I didn’t know’.
Discussion
The purpose of this study was to evaluate whether participation in a Safe Sleep Community Baby Shower impacted Health Belief Model constructs (Becker, 1974) related to the AAP Safe Sleep Recommendations (Task Force on Sudden Infant Death Syndrome, 2016). Community events such as health fairs often share health and safety information in the form of brief presentations or handouts. However, this low level of educational intervention rarely results in behaviour change. The goal of the Safe Sleep Community Baby Showers was to provide infant safe sleep education in a manner that would increase the likelihood of caregivers engaging in safe sleep practices.
Following the Safe Sleep Community Baby Showers, significantly more participants demonstrated positive changes in items related to the Health Belief Theory constructs, including severity, susceptibility, benefits, barriers, and self-efficacy. Based on the theory, shifting perceptions of these constructs should affect behaviour change and increase the likelihood that the AAP Safe Sleep Guidelines (Moon and Task Force on Sudden Infant Death Syndrome, 2016) are followed for infant sleep. When compared to previous Safe Sleep Community Baby Showers in Sedgwick County, Kansas, knowledge of safe sleep recommendations and intentions to follow them remained high (Ahlers-Schmidt et al., 2014, 2016, 2019), suggesting modifications in event logistics did not detrimentally impact changes in knowledge or intention. Further, most participants were highly satisfied with their experiences at the events.
However, two items related to barriers did not meet statistical significance, though changes trended in the right direction: ability to keep infant warm without blankets and having room for a crib in the parents’ room. In terms of blankets, participants who continued to express concern regarding keeping their infant warm without blankets were more likely to be Hispanic or non-Hispanic Black and have low socio-economic status (e.g. less than a high school diploma/GED, uninsured or on Medicaid, and receive prenatal services at a hospital clinic or county health department). The ability to ensure stable housing and/or consistent ambient temperatures may be more challenging for women with low socio-economic status. Material hardship, or difficulty meeting basic needs such as food, housing and transport, have been found in low-income pregnant women (Katz et al., 2018); clothing (32%), stable housing (23%) and safe housing (15%) were specific hardships reported. For such women, the provision of a single wearable blanket at the Safe Sleep Community Baby Shower would not be enough to overcome these material hardships and additional intervention may be needed to facilitate a sleep environment free of loose blankets. Historical use or cultural practices may also influence the decision to use loose blankets (Moon et al., 2016) and the safe sleep literature continues to identify loose blankets as key component of unsafe infant sleep environments (Erck Lambert et al., 2019; Hirai et al., 2019). However, the majority (86.2%) of participants reported being more confident in their ability to keep loose blankets out of the infant sleep environment following the Safe Sleep Community Baby Shower.
Participants who reported they did not have room for a crib in their room were significantly more likely to be married, on Medicaid (versus other or uninsured) and receiving prenatal care at a private provider’s office or hospital clinic. Married women may have larger mattresses to accommodate two people, but a bassinet or portable crib has a small footprint and shifting existing furniture may allow enough room to permit the infant to sleep in the same room but separate bed, as recommended (Moon and Task Force on Sudden Infant Death Syndrome, 2016). As reported above, perceived barriers are a significant predictor of behaviour (Carpenter, 2010; Janz and Becker, 1984), therefore addressing loose blankets and crib space should be priorities at future events. Differences in demographic and socio-economic indicators related to these barriers suggest targeted interventions for priority groups may be most impactful.
Additional barriers the Safe Sleep Community Baby Shower attempted to address were those related to equity and culture. These events were developed as a grass-roots effort to reduce infant mortality by the Wichita Black Nurses Association and KIDS Network (Ahlers-Schmidt et al., 2014). Event promotion prioritised high-risk geographic areas and partner organisations serving groups with limited access to resources, as pregnant women who are marginalised due to racial or socioeconomic factors often experience risk factors (both modifiable and not) related to social determinants of health (Reno and Hyder, 2018). The Wichita Black Nurses Association and Alumnae Chapter of the Delta Sigma Theta Sorority, Inc. committee members felt Black infant mortality was such a priority that they devoted their time and expertise to the issue. Because of their relationships they are seen by the broader community as trusted gatekeepers and ensure that the events maintain a high level of cultural representation and sensitivity. Participation in the events reflects the success of these strategies as over 30% of the participants were non-Hispanic Black and proportion of births to non-Hispanic Black mothers in the community is less than 12% (Kansas Department of Health and Environment (KDHE), 2018).
The group format of these events further helps develop a culture of safe infant sleep. Prenatal group education events have been shown to enhance self-esteem, reduce isolation, promote peer bonding (Canuso, 2003), and increase infant care behaviours, such as breastfeeding (Klima et al., 2009). In terms of infant sleep, social network norms impact women’s infant sleep practices (Moon et al., 2019). To address this, women are encouraged to bring support persons with them to receive safe sleep education and have questions regarding recommendations addressed by trained experts.
Despite efforts to create a culturally welcoming and festive event to convey potentially life-saving information and materials, a small portion (< 2%) of participants were very dissatisfied. No comments elucidated on the reasons for dissatisfaction, and in fact, due to the nature of the comments, authors believe the participants may have mismarked or misunderstood the scale. Negative comments from previous events have addressed length of wait times, length of time to complete event activities, and ambient temperatures. However, dissatisfaction may also be related to personal beliefs regarding bedsharing.
Positive perception of bedsharing may be due to culture, parenting strategy, or perceived benefits, such as breastfeeding duration and increased maternal/infant interactions, as a recent systematic review of bedsharing reported (Baddock et al., 2019). However, despite these perceived benefits, Baddock and colleagues (2019: 112) acknowledge, ‘. . . if the infant is unable to mount an appropriate physiological or behavioural response to its micro-environment’ bedsharing may introduce additional risk. Future Safe Sleep Community Baby Showers should ensure instructors acknowledge participant exposure to conflicting messages regarding infant sleep and facilitate open discussions during the Safe Sleep Crib Demonstrations in order to address inconsistencies. In addition, instructors should specifically explain and demonstrate the ease of same room, separate bed for every sleep.
Limitations
This study is not without limitations. Events were held in a single Mid-western community, focusing on areas with high infant mortality. Collected data are self-reported which could result in response bias, such as social desirability bias. Data collection forms were developed for programme evaluation and lack rigorous psychometric reliability and validity testing. Data were only collected the day of the event, therefore actual behaviours regarding infant safe sleep could not be assessed. In addition, the lack of a controlled comparison group limits the ability to determine causation for changes in beliefs. Despite these limitations, this study suggests Safe Sleep Community Baby Showers can impact Health Belief Model constructs (Becker, 1974) related to the AAP Safe Sleep Recommendations (Task Force on Sudden Infant Death Syndrome, 2016), which may in turn impact behaviour.
Practice implications
Whether conducting a community event or counselling an individual caregiver, focusing on addressing constructs of the Health Belief Model can facilitate changes in behavioural intentions. Particular focus should be on addressing beliefs and lack of material resources as perceived barriers impact behaviour (Carpenter, 2010; Janz and Becker, 1984). Parental non-compliance with safe sleep recommendations has been attributed to several barriers including fear of choking in supine position, lack of a crib and perceived benefit of bedsharing to promote breastfeeding (Zundo et al., 2017). The current study also identified concern about keeping infant warm without blankets and perceived lack of space for a crib in the parent’s bedroom. Helping infant caregivers develop strategies to overcome barriers could increase adherence to the AAP Safe Sleep Guidelines (Moon and Task Force on Sudden Infant Death Syndrome, 2016) and further reduce sleep-related infant mortality.
Footnotes
Acknowledgements
We thank members of the Sedgwick County Safe Sleep Community Baby Shower Planning Committee for their work on these events, including Emalyn Rogers, Monica Spreier, Jolinda Kelly, Linda Wright, Lynetta Echols, Trisha Richmeier, Libby Baumgartner, Christina Rodriguez, Brenda Salinas and others. We also thank Hayrettin Okut for his assistance with the statistical analyses.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was funded in part by the Kansas Department of Health and Environment’s Bureau of Family Health Maternal and Child Health Services Block Grant #B04MC30614 funded by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS). The information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the US Government.