
Abstract
Objectives:
Schools can provide an optimal environment for promoting children’s health behaviours. The Whole School, Whole Community, Whole Child (WSCC) model addresses 10 aspects of the school environment that can be used to promote student health behaviours and academic outcomes: namely, Health Education; Nutrition Environment and Services; Employee Wellness; Social and Emotional School Climate; Physical Environment; Health Services; Counselling, Psychological and Social Services; Community Involvement; Family Engagement; and Physical Education and Physical Activity.
Design:
Guidelines for practical use of the WSCC model for school professionals are limited, impeding potential impact on school health promotion. Accordingly, in this article, we seek to demonstrate an application of the WSCC model to a specific school-based practice: recess.
Setting:
School recess.
Results:
An overview of literature and evidence-informed practices details how recess can facilitate WSCC adoption and initial implementation. Areas requiring further empirical research prior to making additional recommendations are also discussed.
Conclusion:
Strategies to enhance learning and health are described, attempting to bridge the gap between research and practice in school settings using the WSCC model.
Introduction
Children spend a significant amount of time in formal K-12 educational settings. It is, therefore, logical to engage school personnel in the promotion of positive health behaviours of students. The Association for Supervision and Curriculum Development (ASCD) and the US Centers for Disease Control and Prevention (CDC, 2014) introduced the Whole School, Whole Community, Whole Child (WSCC) model in 2014 to provide guidance on combining health and learning in a conceptual framework (see Figure 1). The model takes a multi-faceted approach to school-wide health promotion which includes education, policy and collaboration between the school and the community in a manner that prioritises child well-being (CDC, 2014; Hunt et al., 2015; Lewallen et al., 2015; Michael et al., 2015; Morse and Allensworth, 2015).

Whole School, Whole Community, Whole Child model; Centers for Disease Control and Prevention.
Despite much literature about the value of collaborative efforts to promote student health, there is limited practical guidance that outlines how the WSCC model can be put into practice across complex and unique school settings. Thus, there is a need to highlight the evidence behind each component of the model and directly link that evidence to real-world practice. Here we seek to provide researchers and practitioners with an understanding of how the WSCC model can be applied through the lens of a familiar and broadly accessible school setting: namely, recess.
The CDC, the Society of Health and Physical Educators (SHAPE) America, and other national organisations recommend providing 20 minutes or more for elementary school recess daily (CDC, 2013). Recess provides an unmatched opportunity to bolster the well-being of children in myriad ways. It is a time for children to be physically active and refine movement skills through unstructured play (Ramstetter et al., 2010); physical activity accumulated during recess is indicative of overall discretionary activity patterns in that those who are active at recess tend to be active throughout the day (Bailey et al., 2012). Moreover, it is a key opportunity for children to develop social skills through collaborative activities, building on instruction from the classroom setting (James-Burdumy et al., 2013); thus, recess provides a vital opportunity for supporting children’s emotional health. Yet, despite the reported benefits, a Gallup survey of US elementary school principals in 2010 found that 20% of them reported reduced recess time due to standardised testing requirements, 77% of schools take away recess as a punishment and 89% of school discipline problems occur during lunch or recess (Robert Wood Johnson Foundation, 2010). These data suggest a research-to-practice implementation gap, given that recess serves as a vehicle for health promotion during the school day. Accordingly, the purpose of this article is to describe ways in which school recess can help school administration and personnel begin to implement the WSCC model through identifying potential practices grounded in empirical research.
The literature presented here was compiled based on our collective expertise as school wellness researchers and our knowledge of the WSCC model. We conceptualised four domains to encompass the WSCC model’s multi-faceted approach: (a) curricular and programmatic approaches, (b) school policy and environment, (c) strategies to enhance student social and emotional health and (d) involving key stakeholders in programming. Through such work, we do not intend to describe the full body of literature on the best practices during recess; rather, we intend to describe some of the ways in which school administration and staff may use evidence-informed practices to meet the objectives outlined in the WSCC model in their schools. In addition, specific linkages from recess best practices to each of the 10 core components of the WSCC model are identified, as in Table 1, which can be implemented by school staff and administration. Finally, we provide information for researchers on practices that have applicability within the WSCC model but require more investigation.
Best practices for school recess implementation in relation to the components of the WSCC model.
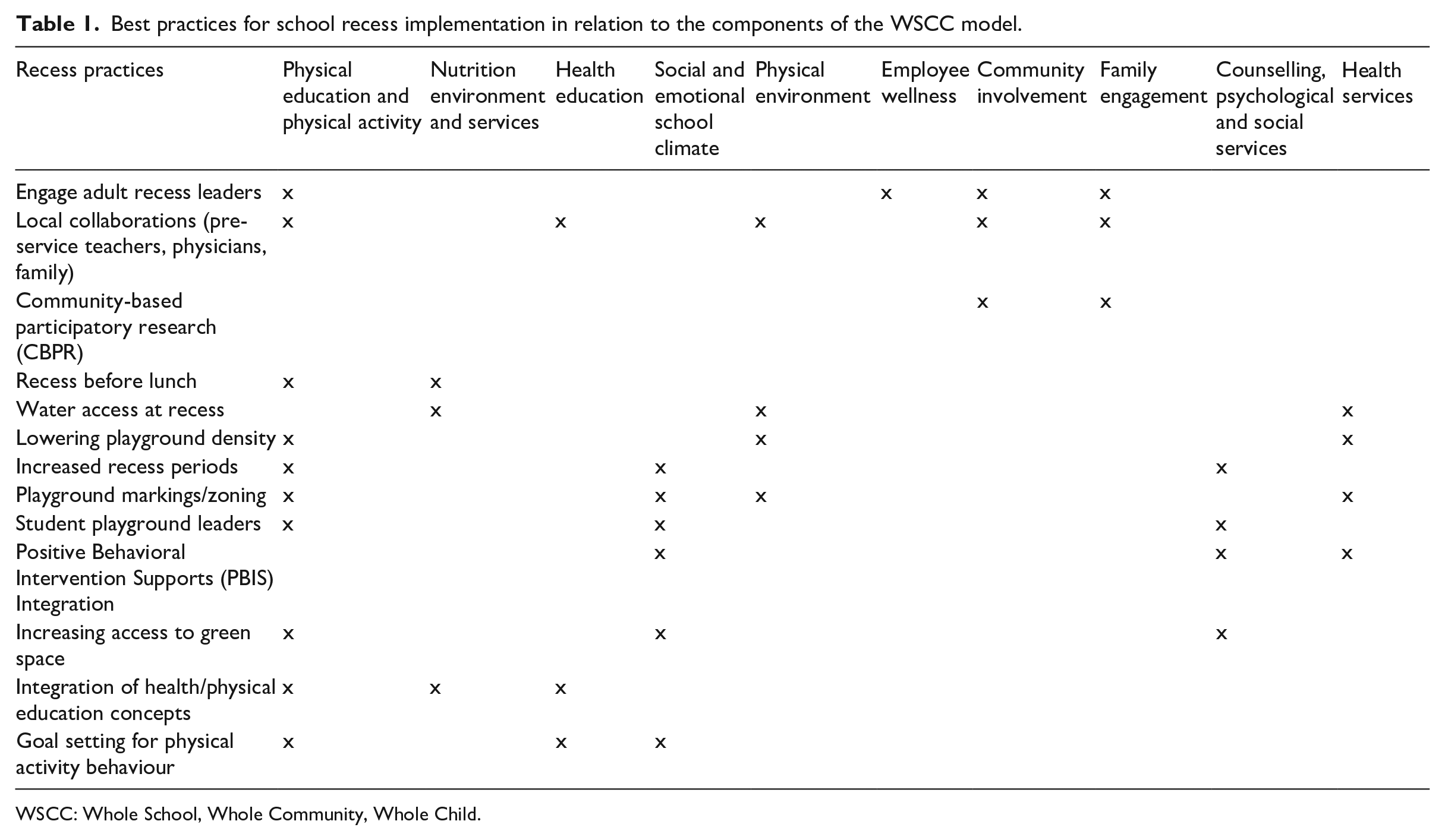
WSCC: Whole School, Whole Community, Whole Child.
Curricular and programmatic approaches
Health education and physical education provide opportunities for students to acquire skills to be physically active and engage in health-promoting behaviours for a lifetime (SHAPE America, 2014). Studies have demonstrated the effectiveness of linking physical/health education to recess by integrating curricular education concepts, such as goal setting, self-monitoring, and play and team-based activities into recess activity (Huberty et al., 2014; Larson et al., 2018; Miller et al., 2018). Early articles written about the WSCC model emphasised the importance of integrating educational components with health, and thus it is important to recognise the ways in which ‘core’ educational subjects can be integrated, not just from health and physical education (Lewallen et al., 2015; Michael et al., 2015). In a WSCC approach, recess is not a replacement for physical education, rather it allows students to practise the physical fitness, motor skills and social-emotional development skills derived from physical education class. Thus, a practical strategy for physical education/classroom teachers or paraprofessionals could be to modify activities and curricula developed for physical education to include a focus on rules and equipment that are also available at recess, in an effort to facilitate social play and participation. In addition, physical and health educators can promote the use of autonomous goal setting and suggest recess as a discretionary time period that can be used to facilitate goal attainment (Larson et al., 2018).
School policy and environment
Schools can also implement practices aligned with the WSCC model during recess through the modification of policies and physical environments (i.e. playgrounds). Policies and environmental factors at recess strongly influence the quality and intensity of children’s activity, engagement, enjoyment, safety and social interaction. For example, reducing playground density can increase the quality of children’s engagement (D’Haese et al., 2013), which may also have implications for health services, as changes in density may reduce injury prevalence and subsequent burden on school staff (London et al., 2015). Moreover, results from reviews (Escalante et al., 2014) and primary studies (Huberty et al., 2014) have demonstrated that adding equipment and playground zone markings, as well as training teachers and peers to be encouraging on the playground, can increase student engagement during recess. These strategies may be particularly important for children from minority backgrounds (Siahpush et al., 2012), girls (Bleeker et al., 2015) and children with disabilities (Sit et al., 2019). This research demonstrates the importance of considering the needs of all students in efforts to modify policies and environments to improve child well-being. Accordingly, school administration and salient members of a school wellness committee could discuss the logistical and pedagogical implications of lowering playground density by scheduling fewer classrooms to be outside at any given time or increasing the amount of space available for play through the ‘zoning’ of activity spaces. This would maximise the use of space available and might be particularly important for schools in urban contexts where space is a premium (Stanley et al., 2012).
In relation to the WSCC component of nutrition environment and services, one key to promoting student engagement during recess is the availability of drinking water (CDC, 2013; Kaushik et al., 2007). The CDC (2013) stresses that schools should maximise access to clean drinking water as a part of high-quality recess so that students are more engaged. Research has supported this by demonstrating the positive impact of providing water to students on their subsequent water consumption (Kaushik et al., 2007). An additional practice that has been recommended is scheduling recess before lunch (Chapman et al., 2017; Hunsberger et al., 2014). The primary rationale for this is to minimise food waste by increasing consumption and to enhance student behaviour during lunch (Getlinger et al., 1996; Hunsberger et al., 2014). A recent study found that students who had recess before lunch had greater residual energy intake (intake minus expenditure from physical activity) and consumed more calories than those who had recess after lunch (McLoughlin et al., 2019). Although reducing plate waste has important health and financial implications, further research is needed to support the required scheduling overhaul to achieve this practice. School personnel and administration may conduct informal research on the impact of scheduling recess before/after lunch by comparing the number of food items chosen and consumed at lunch for each condition, or consulting with classroom teachers in relation to their perceptions of student energy and concentration levels when returning to the classroom to help them understand the needs of their stakeholders (Hunsberger et al., 2014). Finally, research shows a clear and undisputed need for adequate time for children to eat lunch (Cohen et al., 2015, 2016); thus, scheduling at least 20 minutes for sitting lunch time should be a priority for school administration as a means of enhancing nutritional behaviour in students.
Strategies to enhance student social and emotional health
Recess is an important contributor to a positive social and emotional climate, another WSCC component (London et al., 2015). Participation in active games during recess is associated with positive peer relationships, sharing, problem solving and conflict resolution (Fortson et al., 2013). Yet, research has also shown that elementary school students perceive the playground as the most likely place for bullying to occur at school and that those involved (i.e. bullies, victims, bully-victims) have higher odds of feeling unsafe at school (Brewer et al., 2018; Glew et al., 2005). Specifically, Brewer et al. (2018) found that being distracted in class and engaging in fights and conflicts were highly predictive of bullying victimisation. Thus, taking steps to enhance the social-emotional climate within and outside the classroom are essential steps to mitigate these risk factors. To create a positive social and emotional climate through recess, schools can extend their pre-existing behaviour support systems (e.g. through positive behavioural intervention and support) into recess. One strategy is the formation of student leadership committees in which children identify the expectations for fair play, pro-social engagement, behaviour at recess and the inclusion of all abilities (McFadden et al., 2014). By so doing, children can develop social and emotional skills, while also feeling a sense of agency over their environment. These expectations can be taught in classroom lessons or during physical education class, and reinforced through signage on the playground. Classroom teachers and school psychologists/social workers may also wish to collaborate on integrating key social and emotional learning/anti-bullying curricular concepts into the classroom so that they can be applied in the recess setting. One example could be via a ‘fair play’ policy, which is co-created by students and teachers with specific target behaviours that can be applied in both classroom (e.g. learning problem solving and listening skills) and recess playground (e.g. by sharing equipment and play space) contexts (James-Burdumy et al., 2013; London et al., 2015).
In relation to the WSCC component counselling, psychological and social services, recess provides a context to extend programmes implemented in formal curricular settings. Access to green space can improve behaviour and symptoms related to attention-deficit hyperactivity disorder (ADHD), improve attention and memory function, and mediate stress in children (McCormick, 2017). Furthermore, data suggest that access to recess is positively related to classroom behaviour (Barros et al., 2009), that recess-based interventions can improve behaviour over time (Massey et al., 2017), and that recess combined with classroom character curriculum can help with time on task, classroom behaviour and transitions (Rhea and Rivchun, 2018). In a WSCC-based approach, professional service providers may consider advocating for additional recess opportunities for all children, but especially children with psychological and/or behavioural needs.
Several small studies have tested the impact of strategies to increase inclusion of individuals with autism spectrum disorder (ASD) such as fostering peer-mediation techniques where student volunteers serve as recess leaders and work with students with ASD to directly engage them in cooperative play (Locke et al., 2016; Shih et al., 2019). Although these studies are small, outcomes were promising for using peer-mediation and engagement strategies at recess to improve students’ feelings of belonging and enjoyment at recess and also transfer of learning of social skills into the classroom environment (McFadden et al., 2014; Shih et al., 2019). In addition to students with intellectual disabilities, all students can benefit from high-quality recess implementation when aligned to WSCC principles of blending learning and health (Massey et al., 2018a). One example of this application is through The Playworks programme, which emphasises the importance of learning key social-emotional skills through play and has been found to enhance both physical activity and social-emotional skills during and outside of recess (Beyler et al., 2014; Fortson et al., 2013; James-Burdumy et al., 2013). A key message, therefore, is to promote positive peer interactions and pro-social behaviours at recess as a means of fostering the social and emotional well-being of all students during the school day.
Involving key stakeholders in programming
A key tenet of the WSCC model is that students should be supported and challenged in order to learn and make healthy behaviour changes. Engaging staff, family and community members during recess can be a successful means of achieving these facets of the model. Research has shown the positive impact of training school staff to supervise recess and facilitate games that maximise student engagement and activity (Erwin et al., 2014; Huberty et al., 2014). Staff generally perceive themselves as role models for physical activity; however, professional development regarding activity promotion is often somewhat scarce (Huberty et al., 2012). School psychologists, social workers, and other paraprofessional staff may also be well-positioned to provide programmatic leadership and support given their broad reach across the school setting (Volk et al., 2016). It is conceivable that, with additional training, staff such as classroom teachers and paraprofessionals may become more engaged as recess supervisors and/or coaches. Recess and general WSCC implementation leadership should include encouraging and modelling the expectations of engagement and challenge through verbal reinforcement, participation with students in play and pro-social activity during recess (Fortson et al., 2013; Massey et al., 2018a, 2018b).
Parent/family engagement is also valuable in providing greater opportunities for students to be engaged and challenged at recess (Grant et al., 2015). Engaging parents and community members is also a key requirement for the US Department of Agriculture final rule mandate which stipulates that they must be made aware of changes in school wellness policy and practice (US Department of Agriculture Food and Nutrition Service, 2016). Their input can also be valuable for enhancing the acceptability and adoption of specific wellness programming, such as high-quality recess (Rausch et al., 2015; Van Lippevelde et al., 2011). Grant and colleagues (2015) involved all parents of students in grades 3 to 6 in a community-based participatory research process to improve recess through improving the zoning of playground spaces and adding an adult facilitator. Results showed a significant increase in student physical activity, suggesting that the co-creation of recess engagement strategies with families may be beneficial for promoting engagement during recess. Accordingly, members of the school wellness committee should solicit parent input as a means to enhance student physical activity and overall engagement for school recess (Grant et al. 2015).
The WSCC model is encapsulated within a surrounding layer of community support. For example, the National Association of Chronic Disease Directors (2017) recommends that school districts work closely with local physicians and community centres. Although limited research has been conducted to understand the impact of physician involvement specifically in recess, a practical way for physicians to take a more active role in children’s health at school may be through ‘prescribing’ play (Yogman et al., 2018). Schools may also collaborate with local organisations such as the YMCA, Boys & Girls Clubs, faith-based organisations, and parks and recreation services to enhance recess through regular volunteer opportunities for members. These opportunities could include facilitating recess activities, providing new equipment or making play area improvements. In addition, experts from these organisations could provide professional development for teachers to supervise recess; such community partnerships may mitigate barriers faced such as lack of staff supervision and/or training for recess facilitation.
Needs for further investigation
Although evidence exists to guide practice across each domain, there are also evidence gaps that limit the implementation of recess-based initiatives. One practice for which there is little evidence related to implementation is indoor recess. Indoor recess is common, particularly in regions with extreme climates or when testing or field trips shorten class periods. Research is limited on practices and/or policies that mitigate challenges for indoor recess such as less space, increased noise levels and equipment limitations (Tran et al., 2013). There remains a need for researchers to collaborate with school staff to identify and study effectiveness and implementation of strategies to improve quality of activity and engagement during indoor recess.
Furthermore, scant research has been conducted that provides practical guidance for how schools can develop community partnerships that improve recess, as well as what factors must be in place for collaborations to be developed and sustained. One area for future research is engaging undergraduate education students (pre-service educators) as physical activity leaders. Although no interventions have been conducted to examine the impact of pre-service teachers as wellness collaborators in schools, initial feasibility work demonstrates potential efficacy (Webster et al., 2017). Such school–university collaborations may already exist through other field experiences and therefore provide a logical extension to engage undergraduate students in wellness roles. Documented efforts to engage in-service teachers in comprehensive physical activity approaches is another solution to enhancing recess and other aspects of the school setting (Dauenhauer et al., 2018). Collectively, these partnerships build a foundation for a philosophical shift in education; trained teachers will then start/resume their careers with a different mind-set about recess, slowly attenuating inter/intrapersonal and environmental barriers to high-quality recess implementation.
Implications for practice
The WSCC model was developed according to research best practices by the CDC and ASCD, and disseminated at the state and district level (National Association of Chronic Disease Directors, 2017; Rooney et al., 2015). However, few strategies have been identified for school administrators and staff to link policy to actual implementation practices. In this article, we have described ways that research on the components of the model can be implemented through recess, providing schools with a potential ‘starting point’ for WSCC adoption. Although we do not provide a full review of the literature in this area, we used our collective expertise to offer salient examples that hold meaning for practitioners attempting to implement the WSCC model. We encourage others to conduct research in this important area, particularly regarding the practices we describe as needing further investigation. As noted in Table 1, many practices are synergistic, and thus have implications for multiple components of the model. By providing advice on how to apply the WSCC model holistically to school recess, we hope to bridge the gap between research and practice, and further the connection between learning and health.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this product was provided in part by Cooperative Agreement Number (5U48DP00498-05) funded by the Centers for Disease Control and Prevention’s Division of Nutrition, Physical Activity, and Obesity (DNPAO) and Prevention Research Centers Program, which includes the Nutrition and Obesity Policy Research and Evaluation Network (NOPREN). The findings and conclusions in this product are those of the author(s) and do not necessarily represent the official position of the CDC or DHHS.