
Abstract
Objective:
Teachers face high levels of occupational stress, which can influence their mental well-being and contribute to teacher burnout. Healthy levels of exercise, a good diet and adequate sleep can reduce stress and improve mental well-being outcomes. This study explores the characteristics and effectiveness of lifestyle interventions on teachers’ mental well-being, including burnout; discusses directions for future programmes; and aims to identify the nature of evidence and gaps in the research field.
Methods:
A scoping review was conducted in May 2020 via ERIC, Medline, Embase, PsycINFO, Education Source, CINAHL, SPORTDiscus and Scopus databases. The search included relevant peer-reviewed articles on physical activity, nutrition and sleep interventions reporting teachers’ mental well-being outcomes. A quality assessment tool was used to appraise the quality and risk of bias of the included studies.
Results:
Sixteen intervention studies met the inclusion criteria. All studies incorporated physical activity into the intervention; however, only four included aspects of nutrition or sleep. No studies reported only nutrition or sleep interventions alone. The heterogeneity of interventions and their reported outcomes makes comparisons difficult. In general, the quality of the included studies was low due to small sample sizes, poor study design and incomplete reporting of information.
Conclusion:
Preliminary evidence suggests lifestyle interventions can improve mental well-being outcomes for teachers; however good-quality research is needed to improve the evidence base. Future interventions should have stronger research designs and larger sample sizes and use established measurements for assessing outcomes.
Introduction
Mental health is a state of well-being in which individuals can regulate their emotions, cope with stress and adversity, maintain personal relationships and enjoy life (Galderisi et al., 2015). Prolonged exposure to stress can have a detrimental impact on mental well-being (Quick and Henderson, 2016). Positive lifestyle behaviours such as regular physical activity, healthy eating and sleep are important, not only in reducing the risk of chronic disease (Lee et al., 2012) but also in maintaining positive mental health (Dale et al., 2014). Lifestyle interventions aim to increase participation in healthy behaviours, such as physical activity or optimal sleep, and decrease unhealthy behaviours, such as unhealthy eating or alcohol consumption. These interventions have provided evidence for the relationship between lifestyle behaviours and mental well-being (Dale et al., 2014). Evidence from systematic reviews indicates physical activity interventions reduced stress and depression and improved work-related outcomes such as job satisfaction, self-efficacy and absenteeism among workers (Barr-Anderson et al., 2011; Proper and Van Oostrom, 2019). Other healthy lifestyle behaviours such as nutrition (Young et al., 2019) and sleep (Konjarski et al., 2018) are also associated with mood and can reduce stress levels. Workplace nutrition interventions targeting staff dietary behaviour can result in reduced absenteeism and improved productivity (Schroer et al., 2014). Furthermore, interventions to improve employee sleep duration and behaviour produced increases in productivity and overall quality of life (Redeker et al., 2019). Therefore, positive lifestyle behaviours are important to manage stress, reduce absenteeism, improve productivity and maintain a sense of well-being.
School teachers report relatively high levels of occupational stress and burnout (Thomson and Hillman, 2020). Factors contributing to high levels of stress within the profession include a large workload, increasing administrative work, conflicts with colleagues and parents, poor student behaviour and educational reforms (Thomson and Hillman, 2020). These stressful work conditions negatively influence teachers’ job satisfaction and engagement with work (Herman et al., 2018) and have a negative impact on students’ quality of education (Wentzel, 2010). High levels of occupational stress in teachers contribute to the high attrition rate from the profession globally (Chambers Mack et al., 2019). Some studies suggest that up to 40% of teachers leave the profession in the first 5 years (Weldon, 2018) and a larger proportion consider leaving at some point in their career (Chambers Mack et al., 2019). Teachers who stay can face sustained exposure to stress, which has a detrimental impact on their health and mental well-being, with teachers having poorer physical and mental health compared to a general population (Bogaert et al., 2014). In addition, teacher burnout is associated with reduced quality of teaching, poorer classroom instruction, worse student behaviour and lower student academic achievement (Madigan and Kim, 2021; Wolf et al., 2015). Since teachers have an enormous impact on their student’s academic performance, the well-being of teachers is a major concern for society.
Teachers may benefit from lifestyle interventions targeting physical activity, healthy eating or sleep. While teachers generally have low rates of risky behaviour such as smoking and alcohol use (Gilbert et al., 2015), research indicates that teachers have insufficient physical activity (Hoffmann et al., 2013), poor diet (Vio et al., 2018) and poor sleep (Amschler and McKenzie, 2010). Similar to the general population, limited cross-sectional evidence suggests that physical activity is associated with positive mental health and reduced stress among teachers (Bogaert et al., 2014). Therefore, lifestyle interventions could have the potential to both improve mental well-being and reduce chronic disease risk among teachers.
Workplace settings are appropriate for employee health promotion programmes because they can offer the appropriate structure, environment and social setting needed (Holtermann et al., 2021). However, teachers have a unique workplace environment. Interventions during working hours may be challenging due to teachers’ job-related responsibilities, few free hours, differing schedules and students utilising school-based facilities during the school day (Alibali and Nathan, 2010). Thus, current evidence for workplace lifestyle interventions (Schroer et al., 2014) cannot be extrapolated to the teaching population.
Previous research to reduce stress and improve burnout and well-being among teachers has focused on psychological interventions such as cognitive behaviour therapy and mindfulness (Iancu et al., 2018). To the authors’ knowledge, limited research exploring the impact of lifestyle interventions on teachers’ mental well-being outcomes, including stress and burnout, has been conducted. The purpose of this scoping review was to determine the size and scope of the research on the effect of lifestyle interventions on teachers’ mental well-being, including stress. In particular, we sought to (1) describe the characteristics (time of day, duration, lifestyle factors changed) of these interventions; (2) understand whether positive lifestyle interventions impact teachers’ well-being; (3) examine factors associated with intervention completion; and (4) evaluate the quality of research in this area and identify gaps in the knowledge base.
Method
A scoping review was the method of choice for its general purpose of identifying the nature of evidence and gaps in the research field (Arksey and O’Malley, 2005; Levac et al., 2010). An established framework for scoping studies (Arksey and O’Malley, 2005; Peters et al., 2015) and the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews (Tricco et al., 2018) were used to guide the methodology employed in this review to ensure quality and reproducibility.
Identifying relevant studies
Seven electronic databases (ERIC via OVID, Medline via OVID, Embase via OVID, PsycINFO via Ovid Education Source via EBSCO, CINAHL via EBSCO, SPORTDiscus via EBSCO and Scopus) were searched for published papers up to 25 May 2020. All time periods before this date were included. No articles were excluded by publication date. The search terms used are contained in Supplementary File 1. Databases were searched using both subject headings and free-text terms. Relevant keywords included terms related to teachers (e.g. teacher, educator) AND positive lifestyle behaviours (e.g. physical activity, exercise, nutrition, sleep, body mass index, steps, walk, weight loss) AND well-being (e.g. stress, burnout, well-being, mental health) AND interventions (e.g. intervention, programme, evaluation, prevention, professional development, impact, effectiveness, implementation, randomised controlled trial). Reference lists of included studies and identified reviews were also manually searched. Titles and abstracts of identified articles were independently screened by one reviewer (L.C.) to exclude any studies with students as the target population. Another review of the titles and abstracts was then independently completed by two authors (L.C. and P.P.) to exclude irrelevant articles using predefined eligibility criteria. Disagreement between the two reviewers was resolved by discussion and in consultation with a third reviewer (A.B.). Full-text of the potential studies for inclusion was screened for eligibility by the primary reviewer (L.C.) who consulted a second reviewer (P.P.) before excluding/including a study.
Study selection
Inclusion/exclusion criteria were as follows.
Population
The study population was primary/elementary or secondary/middle/high (or international equivalent) school teachers. Studies with pre-service or early education teachers and tertiary education/university teachers or professors were excluded due to the different context and demands faced by these professionals. Studies focused only on teachers with a clinically diagnosed mental illness were excluded.
Intervention
Lifestyle interventions targeting physical activity and/or nutrition and/or sleep. Interventions involving light physical activity, such as T’ai Chi or yoga, were included. Interventions that had a lifestyle component combined with another component (such as mindfulness or resilience training) were included. Mindfulness, resilience training and relaxation interventions without a lifestyle component were excluded. Pharmacological or psychological (e.g. cognitive behavioural therapy) only interventions without a lifestyle component were excluded.
Outcomes
Outcomes that demonstrated measurement of mental well-being (e.g. stress, mental health, burnout, resilience) were included.
Study design
Any study design that attempted to evaluate the effectiveness of an intervention, such as randomised controlled trials and quasi-experimental studies, was included. Studies that used either quantitative or qualitative methods of evaluation were included. While not included, systematic reviews were documented, and references were manually searched for relevant individual studies. In addition, only articles written in peer-reviewed journals were included. Studies were excluded if they (1) were not written in English; (2) published after 25 May 2020; (3) full-text was not available; and (4) were dissertations, theses or publications from the grey literature.
Data extraction
Data were extracted and tabulated using a template to guide data extraction and included the following information: author, year of publication, study aim, target population, sample size, description of intervention (weeks of intervention, description of the programme, duration and frequency), evaluation design, results and factors for teachers’ retention in the study.
Recruitment rates were calculated as a percentage of the people initially enrolling in the study of the total number of eligible participants. Completion rates were calculated as the percentage of participants who completed the study of those who initially enrolled. The recruitment or completion rates were recorded as not reported when not enough information was provided to calculate these rates.
Quality appraisal
Two reviewers (L.C. and P.P.) independently assessed the quality of the studies using an adapted version of the Effective Public Health Practice Project (EPHPP) Quality assessment tool for quantitative studies (Thomas et al., 2004). Disagreements were resolved through discussion. The EPHPP checklist includes assessment of selection bias, study design, confounders, blinding, data collection methods and withdrawals. These domains were scored according to the predetermined criteria (strong, moderate and weak). As defined by the EPHPP tool, studies were given a global rating of strong if they had no weakly rated domains, moderate if they had only one weakly rated domain, and weak if they had two or more weakly rated domains.
Results
A total of 1,283 unique references were identified through electronic database searches. After screening the titles/abstracts and full-text (where necessary) of all potentially eligible articles (n = 192), 16 studies met the inclusion criteria (Figure 1).
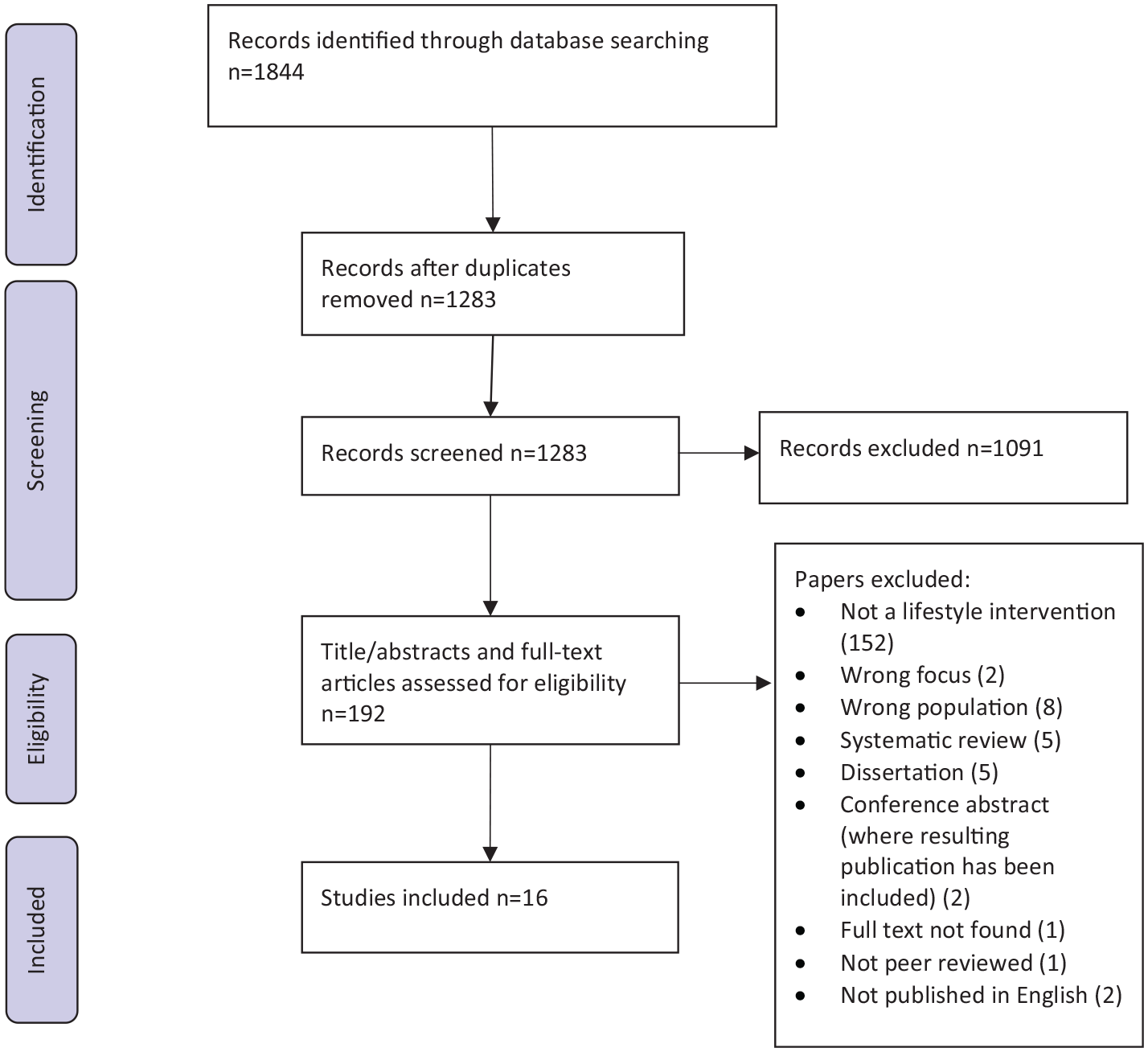
PRISMA flow diagram of the study selection process.
Characteristics of the included studies
The main characteristics of the included studies are summarised in Table 1. All included studies were published between 1984 and 2020. Studies were conducted in the USA (n = 8) (Allegrante and Michela, 1990; Ancona and Mendelson, 2014; Blair et al., 1984; Detert et al., 2006; Harris et al., 2016; Kim and Gurvitch, 2020; Parker et al., 2019; Resnicow et al., 1998), India (n = 5) (Tamilselvi and Thangarajathi, 2011, 2013, 2016; Telles et al., 2018, 2019), Spain (n = 1) (Abós et al., 2021), Australia (n = 1) (Taylor, 2018) and Taiwan (n = 1) (Liu et al., 2015). Eight studies used a quasi-experimental evaluation design (Abós et al., 2021; Allegrante and Michela, 1990; Ancona and Mendelson, 2014; Blair et al., 1984; Harris et al., 2016; Kim and Gurvitch, 2020; Liu et al., 2015; Telles et al., 2018), one was a clustered randomised controlled trial (Resnicow et al., 1998) and eight were pre/post studies with no comparison group (Detert et al., 2006; Parker et al., 2019; Tamilselvi and Thangarajathi, 2011, 2013, 2016; Taylor, 2018; Telles et al., 2019). The sample sizes of the studies ranged from 5 (Taylor, 2018) to 302 (Telles et al., 2019) with a median of 42 participants.
Characteristics of included studies.
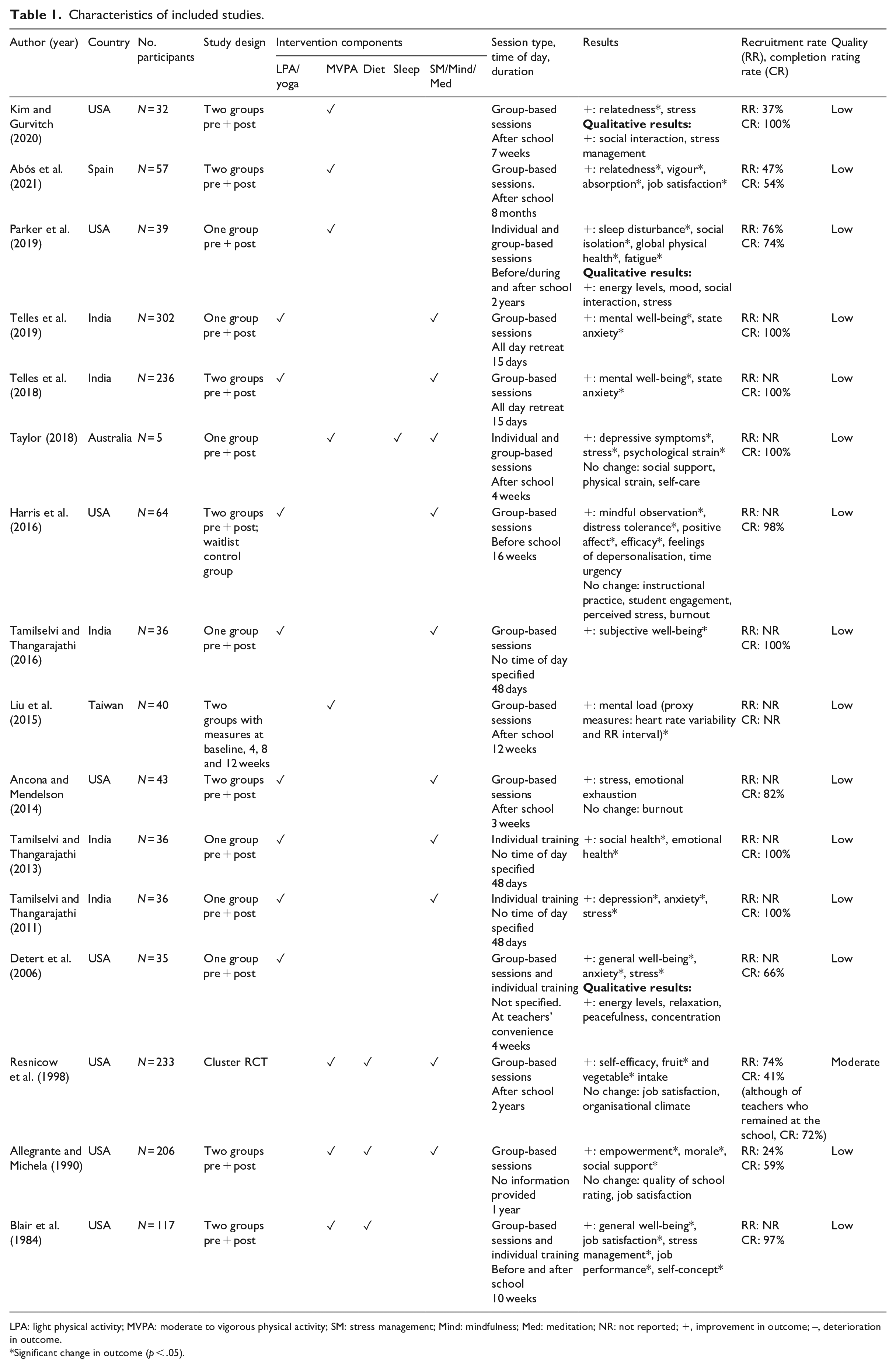
LPA: light physical activity; MVPA: moderate to vigorous physical activity; SM: stress management; Mind: mindfulness; Med: meditation; NR: not reported; +, improvement in outcome; –, deterioration in outcome.
Significant change in outcome (p < .05).
All studies incorporated physical activity into their intervention. Four included aspects of nutrition (Allegrante and Michela, 1990; Blair et al., 1984; Resnicow et al., 1998) or sleep (Taylor, 2018) (Table 1). Eight (50%) studies involved yoga (Ancona and Mendelson, 2014; Harris et al., 2016; Tamilselvi and Thangarajathi, 2011, 2013, 2016; Telles et al., 2018, 2019) or T’ai Chi (Detert et al., 2006), forms of light physical activity. Seven interventions incorporated moderate-to-vigorous physical activity sessions (Abós et al., 2019; Allegrante and Michela, 1990; Blair et al., 1984; Kim and Gurvitch, 2020; Liu et al., 2015; Parker et al., 2019; Resnicow et al., 1998). One study offered workshops on the benefits of exercise (Taylor, 2018). Ten studies (63%) had multiple components, including mindfulness (Harris et al., 2016; Taylor, 2018; Telles et al., 2018, 2019), mediation (Tamilselvi and Thangarajathi, 2011, 2013, 2016), stress management (Allegrante and Michela, 1990; Resnicow et al., 1998; Taylor, 2018) or discussed nutrition (Allegrante and Michela, 1990; Blair et al., 1984; Resnicow et al., 1998) or sleep (Taylor, 2018) as other lifestyle behaviours important to health.
The duration of the interventions varied from 15 days (Telles et al., 2018, 2019) to 2 years (Parker et al., 2019; Resnicow et al., 1998) with a median duration of 7 weeks. Of the 12 studies that reported the time of day when the intervention occurred, 6 provided the intervention sessions after school (Abós et al., 2019; Ancona and Mendelson, 2014; Kim and Gurvitch, 2020; Liu et al., 2015; Resnicow et al., 1998; Taylor, 2018), 1 was conducted before school (Harris et al., 2016), 2 were a mixture of before and after school (Blair et al., 1984; Parker et al., 2019), 1 allowed the teacher to complete at their convenience (Detert et al., 2006) and 2 were delivered as an out-of-school retreat (Telles et al., 2018, 2019).
Study quality
In general, the quality of the included studies was poor (Table 1). Fifteen studies were deemed to be low quality (Abós et al., 2019; Allegrante and Michela, 1990; Ancona and Mendelson, 2014; Blair et al., 1984; Detert et al., 2006; Harris et al., 2016; Kim and Gurvitch, 2020; Liu et al., 2015; Parker et al., 2019; Tamilselvi and Thangarajathi, 2011, 2013, 2016; Taylor, 2018; Telles et al., 2018, 2019), with one of moderate quality (Resnicow et al., 1998). The low quality was mainly due to the small, non-representative sample sizes used, inadequate reporting of statistical analysis (e.g. lack of control for confounders), lack of blinding and poor study design (e.g. non-random allocation, no control group).
Teacher outcomes
Due to the low quality and heterogenous nature of the included studies and the measurement of various, different outcomes, this review cannot provide clear evidence on the effects of positive lifestyle behaviour change interventions on the well-being of teachers. Instead, evidence of trends for these outcomes is described below.
Overall, lifestyle interventions were reported to improve mental well-being (Blair et al., 1984; Detert et al., 2006; Tamilselvi and Thangarajathi, 2016; Telles et al., 2018, 2019), depressive symptoms (Tamilselvi and Thangarajathi, 2011; Taylor, 2018), anxiety (Detert et al., 2006; Tamilselvi and Thangarajathi, 2011; Telles et al., 2018, 2019), depersonalisation (Harris et al., 2016), and adjustment (Tamilselvi and Thangarajathi, 2013) and reduce mental load (Liu et al., 2015). Five of the six studies that measured stress reported significant decreases (Ancona and Mendelson, 2014; Blair et al., 1984; Detert et al., 2006; Tamilselvi and Thangarajathi, 2011; Taylor, 2018), while one found no change (Kim and Gurvitch, 2020). One study measured burnout and reported no change (Ancona and Mendelson, 2014), although participants reported increases in energy levels (Detert et al., 2006; Parker et al., 2019) and vigour (Abós et al., 2019). Improvements were seen in efficacy for classroom management (Harris et al., 2016) and absorption in work (Abós et al., 2019). Results for job satisfaction were mixed with two studies reporting increases (Abós et al., 2019; Blair et al., 1984); however, two studies found no change (Allegrante and Michela, 1990; Resnicow et al., 1998). There was evidence of improvement in social aspects of well-being with reduced social isolation (Parker et al., 2019), improved feelings of relatedness (Kim and Gurvitch, 2020) and relationships with colleagues (Kim and Gurvitch, 2020; Parker et al., 2019). However, Taylor (2018) found no change in perceived social support.
Of the 45 well-being outcomes reported, 28 (62%) showed significant improvements, 12 (27%) showed a non-significant improvement or improvements were reported qualitatively, and 5 (11%) showed no change (Supplementary File 2). No adverse effects were reported.
Factors associated with completion
Five studies reported the recruitment rate which ranged from 24% (Allegrante and Michela, 1990) to 76% (Parker et al., 2019) with a median of 61%. Eleven studies did not provide information on participant recruitment rates. Fifteen studies reported the programme completion rate which ranged from 41% (Resnicow et al., 1998) to 100% (Kim and Gurvitch, 2020; Tamilselvi and Thangarajathi, 2011, 2013, 2016; Taylor, 2018; Telles et al., 2018, 2019) with a median of 98%. One study did not report the completion rate (Liu et al., 2015).
Some factors contributing to completion rates for teachers were the following: team-based nature of physical activity made teachers feel accountable for sessions (Kim and Gurvitch, 2020); teachers elected to be in the intervention rather than the control group (Allegrante and Michela, 1990; Kim and Gurvitch, 2020; Liu et al., 2015; Taylor, 2018); the government or school selected teachers to participate (Tamilselvi and Thangarajathi, 2016; Telles et al., 2018, 2019); provision of incentives (Harris et al., 2016; Parker et al., 2019; Resnicow et al., 1998); the intervention was provided at a convenient time (Taylor, 2018); designed to be completed in work clothes (Harris et al., 2016); and spousal support was encouraged (Blair et al., 1984) (Supplementary File 3).
Factors related to dropout or non-participation in the intervention included the following: teacher turnover (Parker et al., 2019; Resnicow et al., 1998); lack of time (Abós et al., 2019; Ancona and Mendelson, 2014; Parker et al., 2019); family commitments (Abós et al., 2019; Parker et al., 2019); motivation (Parker et al., 2019); self-consciousness (Parker et al., 2019); disability (Parker et al., 2019); work responsibilities (Abós et al., 2019; Ancona and Mendelson, 2014); and the intervention designed for participants to continue with practice in isolation after workshops (Detert et al., 2006) (Supplementary File 3).
Discussion
This review synthesised the available evidence concerning the role of lifestyle interventions, targeting physical activity, nutrition or sleep in improving teachers’ well-being. While all studies incorporated physical activity into the intervention, not all included aspects of nutrition or sleep. No nutrition or sleep interventions, independent of physical activity, were identified, indicating the need for future research in this area. The heterogeneity between interventions and the measurement of outcomes made comparisons difficult; however, initial findings are promising. Lifestyle interventions may have a variety of positive impacts on teachers, including improved mental well-being, anxiety, stress, energy levels, relationships with colleagues and job satisfaction. Importantly, no detrimental effects on any outcome were reported.
This positive finding is supported by previous research in other workplaces. Reviews have found physical activity interventions can improve stress, well-being and work-related outcomes in office (Abdin et al., 2018) and healthcare workers (Bischoff et al., 2019). Lifestyle behaviour change interventions also have a variety of physical health benefits for participants, which can prevent chronic disease (Dietz et al., 2016). Some evidence from a recent systematic review suggests dietary and physical activity interventions may improve the health behaviours of teachers, although further studies are needed to confirm this (Nathan et al., 2020). Therefore, it is recommended that lifestyle interventions continue to be conducted with teachers to determine their effectiveness on aspects of teachers’ well-being. Since reduced teacher stress may improve teaching quality (Wolf et al., 2015), future research could also examine the association between lifestyle interventions and teachers’ educational performance.
While the results of this review are generally positive, it is important to acknowledge the substantial limitations of the studies identified. Most (n = 15) were rated as low quality using the EPHPP Quality assessment tool for quantitative studies (Thomas et al., 2004). Studies had small, non-representative sample sizes, limited study designs and inadequate reporting. An adequate sample size and rigorous study designs, such as cluster randomised controlled trials, are necessary to generate policy-relevant evidence on effective interventions (Moher et al., 2012). In addition, important statistical information, such as possible confounders and recruitment rates, was poorly reported. Considering the importance of this subject for stakeholders, including departments of education/school districts, schools, teachers and researchers, much of this research is not useful, and better designed representative, scalable interventions are needed to generate appropriate levels of evidence of effectiveness.
Information on the completion rate was reported in most studies (n = 15) with an average of 85%. The average completion rate for lifestyle interventions among teachers is higher than that reported by other workplace lifestyle interventions (Johnson et al., 2018), which suggests completion was probably complicated by the small number of participants, short intervention duration and motivated participants. Indeed, completion rates were largely affected by teacher turnover. Four out of five studies with lower completion rates (less than 75%) lasted 8 months or longer and cited teacher turnover as a major contributor to dropout rates. Conversely, the 11 studies with completion rates greater than 75% were relatively short, less than 16 weeks in duration. The exception to this was a study by Detert et al. (2006) which had a completion rate of 66% and duration of 4 weeks. After an intensive 2-day workshop, this intervention asked participants to continue practicing T’ai Chi on their own, which suggests intervention delivery needs to more structured to keep teachers engaged and improve completion rates.
Commonly described barriers to completion experienced by teachers were limited time, work responsibilities, reluctance to take on extra commitments after school, lack of childcare and motivation which have previously been reported by workplace lifestyle interventions conducted in other populations (Kilpatrick et al., 2017). To avoid teachers’ differing schedules, most (n = 10) interventions held sessions outside of school hours or at teachers’ own convenience. Only one study held outside of school hours was limited to before school sessions. Harris et al. (2016) designed before school sessions to be of low intensity so that teachers could complete the activity in their work clothes. This improved participation by reducing the time needed to get changed and increased the appeal of the intervention. Various other factors associated with higher completion were described. Utilising competitive team-based sports kept teachers accountable to turning up to sessions (Kim and Gurvitch, 2020), encouraging spousal participation (Blair et al., 1984), allowing teachers to self-select their activity (Allegrante and Michela, 1990; Kim and Gurvitch, 2020; Liu et al., 2015; Taylor, 2018) and the use of incentives (Harris et al., 2016; Parker et al., 2019; Resnicow et al., 1998) were the strategies used. These strategies have previously been reported to enhance motivation in other health-promoting interventions (Barte and Wendel-Vos, 2017; Teixeira et al., 2012). When planning future lifestyle interventions with teachers, consideration needs to be given to overcoming barriers by incorporating features associated with higher completion rates.
Strengths and limitations
The search of the literature was limited to academic articles published in the English language. Therefore, relevant studies published in other languages or in the wider grey literature may have been missed. However, an extensive search using eight databases from a combination of public health and education was used to systematically search the literature, providing confidence that we obtained most articles on the area of interest (Armstrong et al., 2011). This scoping review assessed the bias of included studies. While scoping reviews generally do not consider bias (Armstrong et al., 2011), it was necessary to comment on the quality of research in this area. This assessment allowed us to make recommendations for future research and ensured positive findings are not overstated. Finally, there is a possibility of publication bias due to preference for publishing positive results over studies with non-significant findings. Generally, publication bias is not assessed in scoping reviews (Armstrong et al., 2011; Peters et al., 2015) and was not evaluated in this review.
Conclusion
The majority of lifestyle interventions included were conducted outside of school hours, and all incorporated aspects of physical activity. Evidence for lifestyle interventions on the well-being of teachers is promising, but due to the small number of studies identified and the extensive methodological limitations of studies reported in this field, firm conclusions to support effectiveness cannot be drawn. Further more rigorous research is needed to provide sufficient quality evidence to inform policy on the use of lifestyle interventions for teachers’ well-being.
Supplemental Material
sj-docx-1-hej-10.1177_00178969211062701 – Supplemental material for Characteristics and effectiveness of physical activity, nutrition and/or sleep interventions to improve the mental well-being of teachers: A scoping review
Supplemental material, sj-docx-1-hej-10.1177_00178969211062701 for Characteristics and effectiveness of physical activity, nutrition and/or sleep interventions to improve the mental well-being of teachers: A scoping review by Lucy Corbett, Adrian Bauman, Louisa R Peralta, Anthony D Okely and Philayrath Phongsavan in Health Education Journal
Supplemental Material
sj-docx-2-hej-10.1177_00178969211062701 – Supplemental material for Characteristics and effectiveness of physical activity, nutrition and/or sleep interventions to improve the mental well-being of teachers: A scoping review
Supplemental material, sj-docx-2-hej-10.1177_00178969211062701 for Characteristics and effectiveness of physical activity, nutrition and/or sleep interventions to improve the mental well-being of teachers: A scoping review by Lucy Corbett, Adrian Bauman, Louisa R Peralta, Anthony D Okely and Philayrath Phongsavan in Health Education Journal
Supplemental Material
sj-docx-3-hej-10.1177_00178969211062701 – Supplemental material for Characteristics and effectiveness of physical activity, nutrition and/or sleep interventions to improve the mental well-being of teachers: A scoping review
Supplemental material, sj-docx-3-hej-10.1177_00178969211062701 for Characteristics and effectiveness of physical activity, nutrition and/or sleep interventions to improve the mental well-being of teachers: A scoping review by Lucy Corbett, Adrian Bauman, Louisa R Peralta, Anthony D Okely and Philayrath Phongsavan in Health Education Journal
Footnotes
Acknowledgements
The authors with to acknowledge Chris Lonsdale at the Australian Catholic University for useful discussion.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the NSW Teachers Federation Health Foundation under Grant 204443.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.