
Abstract
Background:
The perspectives of community partners about their experiences working with medical students and how service-learning experiences affect the communities they serve remains understudied.
Objective:
This study addressed gaps in the literature by reporting on in-depth interviews conducted with community partners who participated in a well-established medical school service-learning programme.
Design:
A qualitative study was undertaken using semi-structured interviews and an edited coding strategy.
Setting:
A convenience sample was recruited from a database of organisations working with the medical school’s service-learning organisation.
Method:
Between 2017 and 2020, the researchers conducted semi-structured interviews with community-based organisation partners who worked with medical students through a service-learning initiative in an urban, underserved area of New Jersey, USA. The authors coded transcripts and identified themes after extensive reading, reflection and team discussion of transcripts and coded text. Authors confirmed thematic saturation after 20 interviews with 21 participants representing 18 different agencies.
Results:
Three main themes were developed: (1) medical students as role models, (2) community partners’ role in shaping medical student education, and (3) reciprocity between community-based organisations and the service-learning programme. Participants found that medical students connected well with young clients and motivated them to pursue higher education or healthcare careers especially when they had a shared ethnic or cultural background. Community partners helped medical students better understand ethnically and socioeconomically diverse communities from a whole-person perspective. Participants described collaborative learning and reciprocity between the service-learning programme and community-based organisations as a ‘win-win’ situation – with clients, the organisation and medical students all benefitting.
Conclusion:
Findings illustrate the importance of reciprocity between medical students and community partners. Incorporating partners in the design and evaluation of service-learning programmes is essential to understanding how community and academic health centres can better collaborate to promote health equity.
Keywords
Introduction
In the USA, the Liaison Committee on Medical Education (LCME) recommends that medical education programmes provide sufficient opportunities for students to participate in service-learning and/or community service activities (LCME, 2021: 8). The LCME defines service-learning as having three important characteristics: (1) medical students should respond to community-identified needs, (2) be prepared for the activity and (3) reflect on the experience (LCME, 2021: 26). Reflections should include how the activity pertains to the student’s relationships, the medical school curriculum and students’ roles as citizens and medical professionals (LCME, 2021: 26). Student reflections and other evaluative methods provide medical schools with information about the effect of service-learning on the medical student and the curriculum, but far less is known about the perceptions of community partners working with a medical school and the influence on their organisation (Hunt et al., 2011).
As previously noted by Hunt et al. (2011), many articles about service-learning in medical education describe programmes that range from one-time volunteer activities to longer term formal experiences. A 2015 systematic review of service-learning in medical education summarised how service-learning experiences benefitted medical students (Stewart and Wubbena, 2015). These experiences provided medical students with opportunities to collaborate with community partners, learn to identify community needs, develop awareness of the effects of social determinants of health, recognise the need for social justice for underserved communities and gain a better understanding of health disparities that can be addressed by interventions, community partnerships and policies (Stewart and Wubbena, 2015).
Only a few studies however have examined the community’s experience of medical school service-learning initiatives. In some cases, authors provide information about how community partners are involved with a specific service-learning programme (e.g. Buckner et al., 2010). Another study found that community partners had both educational expectations for students such as learning about their clients and expectations that the students would serve the organisation’s unmet needs (Elam et al., 2003). Others have reported results from participant surveys including satisfaction from working with the students (Waddell and Davidson, 2000) and knowledge gained that resulted in positive lifestyle changes (Averill et al., 2007). Still, others described participant outcomes such as increased use of preventive health services and decreased use of the emergency room as a source of care (Greer et al., 2018; Rock et al., 2014).
To date, the perspective of community partners about their experiences working with medical students and how service-learning experiences affect the communities they serve remains understudied. To our knowledge, no studies have utilised qualitative methods to delve deeply into community partners’ experiences. Qualitative methods are uniquely suited to understand experiences from the perspectives of participants (Creswell, 2007). The current study seeks to address these gaps in the literature by reporting on in-depth interviews conducted with community partners who participated in a well-established medical school service-learning programme. We sought to understand community partners’ experiences of service-learning activities and the meaning of these experiences for the communities they served.
Methods
Setting
In 2015, Robert Wood Johnson Medical School (RWJMS), Office of Community Health began an evaluation of the medical school’s service-learning organisation, the Homeless and Indigent Population Health Outreach Project (HIPHOP). Since 1992, HIPHOP has been the service-learning organisation for RWJMS medical students and other Rutgers University health profession students. HIPHOP was founded by two medical students who wanted to address the gap between community members and the medical system. The programme was designed to create better-equipped physicians and a stronger community using community outreach, health promotion and advocacy for underserved and indigent populations with education, support and care. Guided by its mission, HIPHOP continues to link educational experiences for medical and health profession students with community partners to help address health-related needs in Greater New Brunswick, New Jersey communities.
The HIPHOP is led by approximately 11 medical student steering committee members under faculty and staff leaders (E.J. and S.G.) who have worked with the programme for over 20 years. Over the years, faculty, staff and students have developed long-standing relationships with community partners. Whenever a community partner flags an issue or at the end of each academic year, HIPHOP’s programme director provides community partner feedback to the medical student steering committee and together they adjust programming accordingly. At RWJMS, medical students engage with community partners in required and volunteer activities and events such as leading health education workshops, supporting youth programming and operating a student-run health clinic. All medical students are required to work with HIPHOP programmes during their preclinical years (particularly during their first year), but some continue to participate in HIPHOP programmes throughout their medical school career. The different programmes require varying amounts of time for the students to interact with community members.
Previously, a RWJMS team assessed the perceptions of alumni physicians who were student leaders of HIPHOP and about the influence of the school’s service-learning experiences on their medical careers. This study found that service-learning experiences influenced alumni physicians in their professional development and approach to practice (Hand et al., 2018). In the current study, we aimed to understand community partners’ experiences working with medical students.
Approach
Between November 2017 and January 2020, we conducted semi-structured interviews to explore community partners’ experiences with medical student service-learning activities. The project was developed by an interdisciplinary research team with two experienced members well-versed in qualitative methods, which includes two physician health services researchers, a community health researcher, medical students and HIPHOP’s programme director. The team developed an interview guide that was informed by a literature review and consisted of a series of open-ended questions and probes (see Figure 1). This study was granted expedited status by the Rutgers Biomedical and Health Sciences Institutional Review Board (Protocol ID: Pro20170000730). The study was granted a waiver of consent and all participants consented verbally prior to the start of the interview. The study follows the Standards for Reporting Qualitative Research.
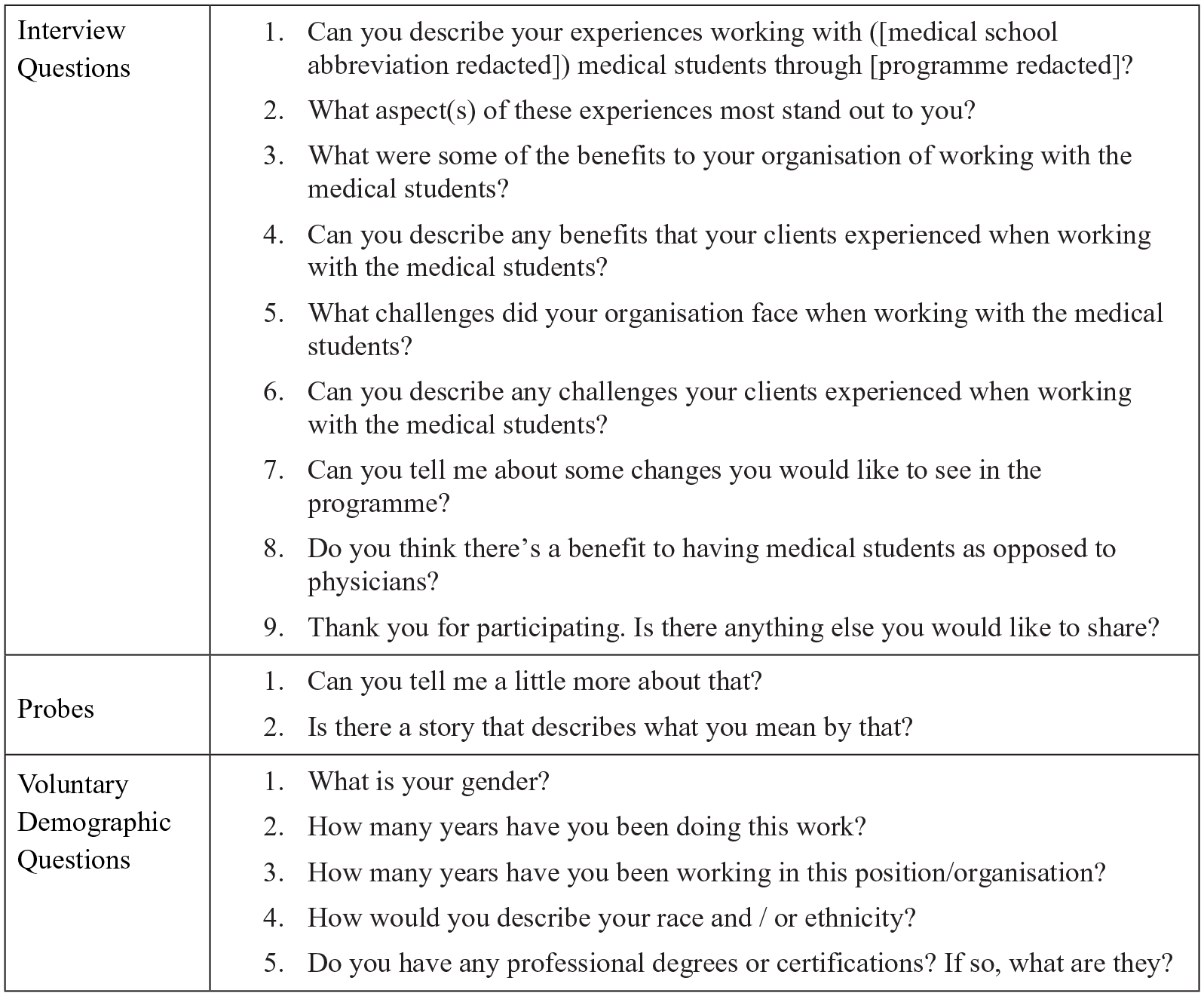
Interview questions and probes from a qualitative study with community organisations that Hosted RWJMS medical students through HIPHOP, 2017–2020.
Sampling
One member of the research team (S.G.) recruited community participants from a database of organisations that were community partners of HIPHOP. To address our research goal, we purposively sampled community organisations that had multi-year relationships with HIPHOP. All participants held leadership positions in their organisations and could comment broadly on their constituents working with medical students. We excluded anyone who had not worked directly with medical students.
Data collection
Four medical student team members (B.B., L.F., E.K., P.P.) were trained in qualitative research methods by the experienced researchers (M.J., M.B.P.) and conducted one-on-one semi-structured interviews with 21 community partners by phone. Interviews were recorded using a digital voice-recording device, and all participants gave verbal consent prior to beginning the interview. Community partners were asked open-ended questions about their organisation and their experiences working with medical students through HIPHOP. The interviewers generally followed the interview guide but were able to reorder questions and add probes based on the flow and content of the interviews. On average interviews lasted approximately 30 minutes and were transcribed and de-identified. These transcripts were then entered into NVivo12, version 12.6.1 qualitative analysis software (QSR International, Burlington, Massachusetts).
Data analysis
We used descriptive statistics to summarise participant demographic information. We used an editing coding strategy in which ideas and categories were identified from the data (Boeije, 2002). Seven members of the research team (B.B., L.F., S.G., E.J., M.J., P.P., M.B.P.) read the first five transcripts and discussed patterns in the responses to develop an initial coding scheme. All transcripts were coded independently by at least two members of the team (B.B., L.F., E.K.). We conducted coding comparisons using NVivo software and discrepancies were resolved through discussion and consensus (Krefting, 1991). The research team met regularly and analysed the data by iteratively reviewing transcripts, identifying representative quotes and refining the codebook. Once coding was completed, to identify themes, we searched for key phrases and patterns through extensive reading and reflection on the coded text and transcripts. We suspended interviews once saturation (when no new information is identified) was achieved (DiCicco-Bloom and Crabtree, 2006).
Results
The 21 interview participants represented 18 community organisations providing services and resources to diverse populations from under-resourced (e.g. housing insecure and economically disadvantaged) communities, with different health issues (substance abuse and violence) and at different ages (e.g. youth and seniors). Table 1 provides demographic characteristics of the interview participants.
Self-reported characteristics of the 21 participants in a qualitative study with community organisations a that hosted RWJMS medical students through HIPHOP, 2017–2020.
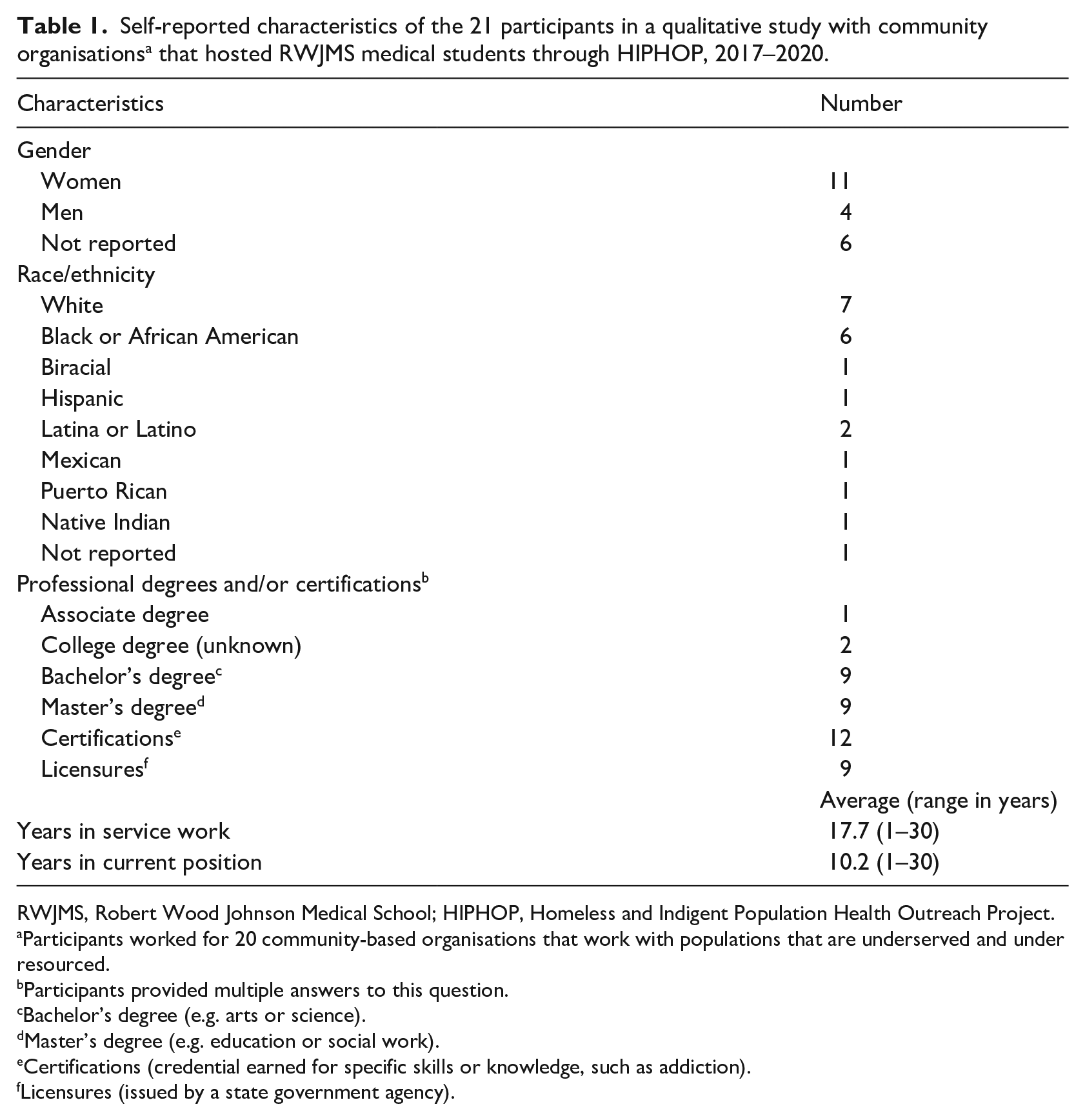
RWJMS, Robert Wood Johnson Medical School; HIPHOP, Homeless and Indigent Population Health Outreach Project.
Participants worked for 20 community-based organisations that work with populations that are underserved and under resourced.
Participants provided multiple answers to this question.
Bachelor’s degree (e.g. arts or science).
Master’s degree (e.g. education or social work).
Certifications (credential earned for specific skills or knowledge, such as addiction).
Licensures (issued by a state government agency).
The community partner participants provided unique perspectives and three primary themes emerged from the data: (1) medical students as role models, (2) community partners’ role in shaping medical student education and (3) reciprocity between the community-based organisations and service-learning programming.
Medical students as role models
Most participants working with youth indicated that the medical students provided role models for their constituents because the students were closer in age, shared ethnic and/or cultural backgrounds with clients, and encouraged young people to see themselves in a healthcare-related career.
One participant indicated their clients’ willingness to listen to medical students because they are connected with them.
. . . I think people would be a little probably less intimidated by a medical student . . . because if you’re doing a more age-diverse audience, I think the medical students would make it even more friendly for the younger folks to want to get up and go – or listen to what they’re saying . . .. (Participant 10)
Another participant described how the youth benefitted from interacting with medical students who shared their ethnic or cultural background.
. . . many of the medical school students that are participating in the programme or engaging in the programme, there are minority students . . . [public school] students can actually relate culturally to medical school students that look like them, and so it further helps them to buy into the process of obtaining their education . . . so that they can arise and be in the position, take advantage of an advanced degree and further their goals and their dreams. (Participant 19)
Some participants indicated that their clients were motivated by the medical students to pursue higher education and/or careers in healthcare fields.
. . . we also follow through with our students and find out if what we’re doing has an impact on the careers that they’re pursuing. And I would say maybe about ten of them came back to us and was actively pursuing medicine – whether it was nursing, whether it was becoming a doctor – and they told us, . . . it was because of the experience that they had . . .. (Participant 9)
Community partners’ role in shaping medical student education
Half of the participants indicated that they found value in helping medical students better understand how social determinants of health affected specific populations, and appreciating the value of adopting a whole-person perspective. In addition, participants provided feedback to the programme to help students be better prepared to work with sometimes challenging populations and made recommendations for better educational preparation. The interviews revealed the key role that community partners provide for medical education particularly in assisting medical students when working in ethnically and socioeconomically diverse communities.
. . . two things stood out: the ability to sort of work with medical students in looking at the work that they’re doing from not just a medical lens, but from sort of a social determinants of health in terms of a public health lens or sort of an ecological model . . . So to be able to work with medical students to sort of shape some experience for them as they move through their programme . . . and into their professional life, I think is really impactful and powerful and important. (Participant 2)
Some partners helped educate medical students on the broader context stressing the importance of adopting a whole-person perspective rather than a narrow focus on medical conditions.
. . . opportunity for the [medical] students to have firsthand knowledge of some of the conditions that their potential patients may face and to sort of be aware of some of the barriers to care that they face and to learn about some of the conditions that they have and how their social and physical environments contribute to or exacerbate those conditions and how they as future providers can sort of incorporate some of that information into their practice so that they’ll be more aware and more focused on patient-centred care. (Participant 14)
During the interviews, some partners provided useful feedback, which was used to improve future programme provision and development.
. . . But I wish that – so the students come in pre-trained or trained or taking a class on substance abuse and the different treatment modalities and what does that mean and trauma informed care . . . Same thing with mental illness. We also have clients that suffer from mental illness . . . And sometimes students don’t [sic] know how to manage and sometimes get overwhelmed. (Participant 5)
Similarly, community perceptions about the importance of understanding the organisation and its clients before working with clients were incorporated into programming.
. . . the majority of the HIPHOP students don’t [sic] know what [organisation] does. So, when they come in they have no idea who they’re talking to, which kind of just adds to like this population doesn’t [sic] – not a lot of people really care about them . . . I think if they just go on to [organisation]’s website. I think [organisation] does a pretty good job of explaining the population we serve. (Participant 7)
Reciprocity between community-based organisations and service-learning programme
Two-thirds of the interviews described the collaborative learning and reciprocal benefits between the service-learning programme and community-based organisations. Some community partners indicated that medical students’ participation filled unmet needs in the community. One respondent described how health information benefitted a client.
. . . they presented about sexually transmitted infections and there was something that a client, she hadn’t [sic] realised that what she had was a sexually transmitted infection . . . It was something that she learned there . . . No one’s taught them this before and so that was interesting and humbling to see that, this was the first time that it was actually called a sexually transmitted infection to her. (Participant 6)
Some partners appreciated the reciprocity between the medical school and the community organisations. One participant provided a story illustrating this reciprocity as a ‘win-win’ situation.
‘. . . for the medical students a great way of interacting with a community that they might be serving because they might stay here in the area or they might go into other urban communities and that gives them experience of what is the reality of living in an urban community’. . . . ‘They had a great conversation, and the medical student was sharing with my staff how great he felt of coming to the kids, that he learned from the kids even though he was there to teach, . . .’. (Participant 3)
Another partner described the mutual learning that occurs between their clients and the medical students.
And I like the fact of how HIPHOP has medical students who actually come in, and it’s pretty much volunteering their time to educate a lot of people who don’t [sic] know . . . It’s a great opportunity. . . . I know it’s to help them [medical students] to get to know the community, to understand the clientele, to understand the population that they will be working with, it still works on both sides. It works for the clients and it works for the medical students. (Participant 4)
Notably, one partner recognised the importance of the relationship for the individual, the organisation and the medical students.
. . . The first need is that you are helping the individual that finds themselves desperately in need of food, clothing, furniture . . . The second person who is benefiting is the organisation, because now the medical students are – become volunteers within the organisation, and the organisation is then able to meet the needs of the community. The third person who is benefiting from these outreach activities are the [medical] students . . . And so the [medical] students . . . are also the beneficiaries of this experience, because then it allows them to really see for themselves the faces of the people that are in need that does not look any different than their faces. So, it gives them compassion, it gives them the insight and it allows them to be upfront and close and be able to communicate with families, children and youth who they’re servicing. (Participant 9)
Discussion
This study provides insights into community partners’ experiences working with medical students participating in service-learning. The partners perceived that their organisations received important health education and access to services and they, in turn, provided the medical students with important insights about the community. Importantly, the study offers illustrations of reciprocity between community partners and medical school participants.
Community partners described how the young people served by their programmes formed relationships with medical students and how similarities in age, race and/or ethnicity help some young people envision a future for themselves in the health sciences. Previous work has identified how medical students help expose mentees to healthcare careers, provide guidance and facilitate the recruitment of youth who are underrepresented in medicine to the medical fields (Afghani et al., 2013; Derck et al., 2016; Haggins et al., 2018; Patel et al., 2015). Our findings illustrate how medical school service-learning organisations can provide opportunities for these important interactions.
The community’s role in shaping medical student education and the value that community partners placed on this role has not been previously well characterised (Hunt et al., 2011). This study reveals the value that community organisations placed on having a collaborative partnership with the medical school and contributing to medical education by sharing their knowledge of the community, while medical students share their medical knowledge. This study provides some insights into how community partners shaped medical education, including helping medical students better understand the social determinants of health and helping them appreciate the value of a whole-person perspective. Importantly, the study also provides insights into the reciprocity between community partner organisations and the medical school. Community partner organisations and the people they served indicated that the services the medical students provided filled unmet needs (e.g. health workshops on sexually transmitted infections) while medical students were exposed to important contexts (e.g. reality of living in an urban area). Our study offers just one example of how long-term relationships between a medical school and community partners can be valuable, particularly when partners give continuous input into programme development and implementation (Averill et al., 2007; Rock et al., 2014).
Medical schools working with community partners on programming should consider formalising the structures that incorporate community input using both formative and summative evaluation processes that allow partners to provide input throughout the process. Advocates of community-engaged medical education call for medical schools to genuinely engage communities in programme development including providing input into student learning objectives (Strasser et al., 2015). The primary challenge to medical schools lies in how to develop meaningful relationships with community partners within the many demands of a medical education curriculum. The challenge to individual faculty and staff is learning how to work with community partners who have increasingly been asked to do more with less time and fewer resources. A recent effort by the American Association of Medical Colleges (AAMC) indicates movement in a positive direction. The AAMC Collaborative for Health Equity: Act, Research, Generate Evidence recently developed Ten Principles of Trustworthiness (AAMC, 2021) and an accompanying toolkit to guide health care institutions as they work with communities. The principles, which help guide individuals as they seek to work with community partners, were developed with the input of 30 community members from diverse areas across the USA. Understanding and employing these principles is a good first step in guiding academic health centres as they develop long-term relationships with community partners while providing services that meet the needs of a community.
Limitations
Limitations to our study include the fact that HIPHOP is a long-standing service-learning organisation at the medical school with a dedicated director who has built numerous partnerships with community organisations throughout her tenure. In addition, the director and steering committee regularly improve programme activities by incorporating community partner feedback. Therefore, our findings may not transfer to settings with less-established programmes. Questions asked about previous interactions with medical students may have allowed for recall and social desirability bias. The community served by our medical school is a small-to-medium urban area in central New Jersey. As a result, the experiences of communities in larger urban areas, suburban areas or rural areas may differ from those of the community served by our service-learning organisation.
Conclusion
This study highlights community partners’ experience working with medical students through service-learning activities. Our findings illustrate how medical students bring unique value as role models to young people in the community and how community partners can shape medical students’ education through a reciprocal relationship. Incorporating community partners in the design and evaluation of service-learning programmes is essential to further understanding how the community and academic health centres can better collaborate to promote health equity.
Footnotes
Acknowledgements
We thank the participants who took part in the study. We also thank Parth S. Patel for his assistance with data collection and analysis when he was a medical student at Rutgers Robert Wood Johnson Medical School.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Maria Pellerano reports grant funding from Johnson & Johnson Corporate Foundation and personal fees from the Patient-Centered Outcomes Research Institute for grant reviewing and from the University of Massachusetts, Lowell for participation on a grant advisory committee. These sources of funding did not have any role in this study design, data collection and analysis, decision to publish or preparation of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Maria Pellerano is supported by Johnson & Johnson Corporate Foundation. Manuel Jimenez is supported by the National Center for Advancing Translational Sciences, a component of the US National Institutes of Health under award number (UL1TR003017); the US Department of Health and Human Services/Health Resources and Service Administration (HRSA) under award number (U3DMD32755); and the Robert Wood Johnson Foundation through its support of the Child Health Institute of New Jersey under grant number (74260). Eric Jahn is supported by the Hunterdon Health Fund. These funding agencies had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.