
Abstract
Objective:
To gain retina physicians’ and diabetic retinopathy (DR) patients’ perspectives on needs and opportunities in DR education, and then develop and pilot test an educational video.
Design:
This study utilised qualitative interview data for video creation, and interview and survey data for assessment.
Setting:
This study was conducted in a single large academic medical centre.
Method:
We conducted semi-structured interviews with attending retina physicians and DR patients (Cohort A) which were coded for themes about needs in DR patient education. Using these interviews, we designed and piloted a 6-minute user-centred animated video among a second patient cohort (Cohort B), who completed post-intervention interviews.
Results:
Four physicians and 14 DR patients participated in the study. Themes from Cohort A included accessible information, early management, lifestyle factors and emotional context. Physician themes included effective communication, visual information delivery and individual-level diabetes management. Cohort B commented on the subsequently created video’s improved accessibility, engagement and supplementation of their existing DR knowledge.
Conclusion:
Physicians and patients showed an interest in video education and identified unique educational needs. We used these insights to create a video that demonstrated positive patient uptake. Close attention to retina physicians’ and DR patients’ perspectives can offer a valuable approach in developing materials to increase patients’ health knowledge. Within the context studied, videos may be more accessible and engaging than the use of traditional print-based education materials.
Introduction
Diabetic retinopathy (DR) is a complication of diabetes and a leading cause of vision loss in adults aged 20–74 years (Lee et al., 2015). Appropriate follow-up with an ophthalmologist, screening for DR among patients with diabetes and proper dietary control can prevent vision loss in patients with diabetes; however, patient knowledge and education play an important role in the uptake of these strategies (Lee et al., 2015; Meyer et al., 2016; Ramagiri et al., 2020). It is estimated by the World Health Organization that 50% of adults with chronic diseases in industrialised nations are non-adherent to their respective disease treatment (World Health Organization, 2003). Although the reasons for this are multifactorial, studies have shown that patient education can significantly improve treatment adherence (Bogner et al., 2012).
Patient education in medicine is rapidly evolving beyond conversations in the doctor’s office. With increasing access to the Internet and computers, patient education is being delivered through novel means such as online educational videos, computer education software and informational websites. Unfortunately, web-based information, including websites regarding DR, is seldom subjected to peer review and can even be unhelpful or inaccurate (Kloosterboer et al., 2019; Visser and Snoek, 2004). Furthermore, educational materials in ophthalmology are frequently written at a level that is too complex for most patients to understand (Williams et al., 2016). When used properly, however, video-based education can show positive effects compared to traditional education and can improve short-term health literacy goals among patients (Dahodwala et al., 2018).
There are limited studies assessing the design or impact of video education in DR. A study in the USA among African Americans with diabetes utilised a video as part of its educational intervention and demonstrated improved rates of ophthalmic screening following education (Basch et al., 1999). Another study in India compared the use of educational videos versus a pamphlet and showed increased rates of DR screening among patients who were shown the videos (Ramagiri et al., 2020). Research in Australia has shown similar results after distributing an educational video to an Indigenous population (Meyer et al., 2016). However, in each of these examples, there was no input from patients with DR to the design of the video, nor was there a discussion of the components of the video that made it successful.
‘White board animation’ videos are videos that animate content on a white screen in a manner similar to the way in which a teacher might draw on a white board. Their popularity has significantly grown in recent years, and they are now incorporated by major educational video producers into modules that teach medicine, physics and other subjects. Studies have shown that this type of educational approach may have advantages in information retention, engagement and enjoyment compared to traditional techniques such as slideshows, text and audio narration (Türkay, 2016).
This study provides a needs assessment from retina physicians and DR patients in the Northeastern USA in creating an effective educational video for DR. Using feedback from patients and physicians, we designed a white board animation DR patient education video, which we then piloted among patients to assess its effectiveness and feasibility as an educational tool.
Methods
Participant selection
Approval for this study was received from the Yale University Institutional Board. Three study groups were recruited for the study: a physician group, a patient Cohort A and a patient Cohort B. Physicians included in the study were all practising board-certified ophthalmologists with fellowship training in vitreoretinal surgery. Participant inclusion criteria for Cohorts A and B consisted of age >18 years and having a diagnosis of DR. Exclusion criteria included other co-existing retinal diseases as well as visual acuity less than 20/200 in the better seeing eye. All participants were recruited at the Yale Eye Center, which is a large academic teaching centre in the Northeastern USA.
Semi-structured interviews
We conducted semi-structured interviews with participants, with interview guides developed by the authors using an iterative approach of constructing and reviewing key questions based on the study objectives. Each question was used as a starting point to begin a conversation on a respective topic. Each interview lasted between 15 and 30 minutes and was conducted by a single trained medical student.
Interviews with the retina physicians were guided by the following six questions: (1) How do you think video technology can be utilised in your daily clinic to improve patient education? (2) What methods have and have not been effective in communicating with your patients? (3) How can we design an animated patient education video that would be most beneficial for your patients? (4) How do you describe DR to your patients? (5) What are the three most important things you want your patients to take away from their education? (6) What are some problems in communication that may impair patient education?
Participants in Cohort A participated in individual semi-structured interviews guided by the following three questions: (1) On a scale of 1–10, how well do you understand the conversations with your doctors about DR? (2) What do you want to know about DR? (3) If a video were to be made on DR to explain the disease to patients like you, what important things would you want it to include?
Patient interviews were conducted prior to the patient’s appointment at the Yale Eye Center by the medical student only with no physician in the room. Explicit disclosure was provided that the interview would not affect their treatment plan, nor would the interviewer discuss the content of the interview with the physician treating the patient, except in an anonymised, aggregated manner in the future.
Participant informed consent was obtained prior to commencing each interview. All interviews were recorded, transcribed and coded for themes by three investigators.
Video development
Using the themes found in the interviews, a script for a video was developed by the investigators. This script was reviewed by the retina physicians previously interviewed and iteratively improved upon prior to creating animations. VideoScribe software (Sparkol Ltd, Brooklyn, NY, USA) and Adobe Illustrator (Adobe Inc, San Jose, CA, USA) were used to animate the video. The animated video was further iteratively improved in consultation with physicians before being finalised.
Video piloting
The finalised video was piloted among participants in Cohort B. Participants self-reported their understanding of DR before and after watching the video. Following video viewing, participants were asked to provide their feedback on the video’s feasibility for implementation, quality and helpfulness. These comments were recorded, transcribed and coded for themes by two independent investigators. Quantitative analysis of demographic variables and knowledge assessment was performed using Fisher’s exact test and paired two-tailed t-tests using RStudio 1.4 (RStudio PBC, Boston, MA, USA).
Results
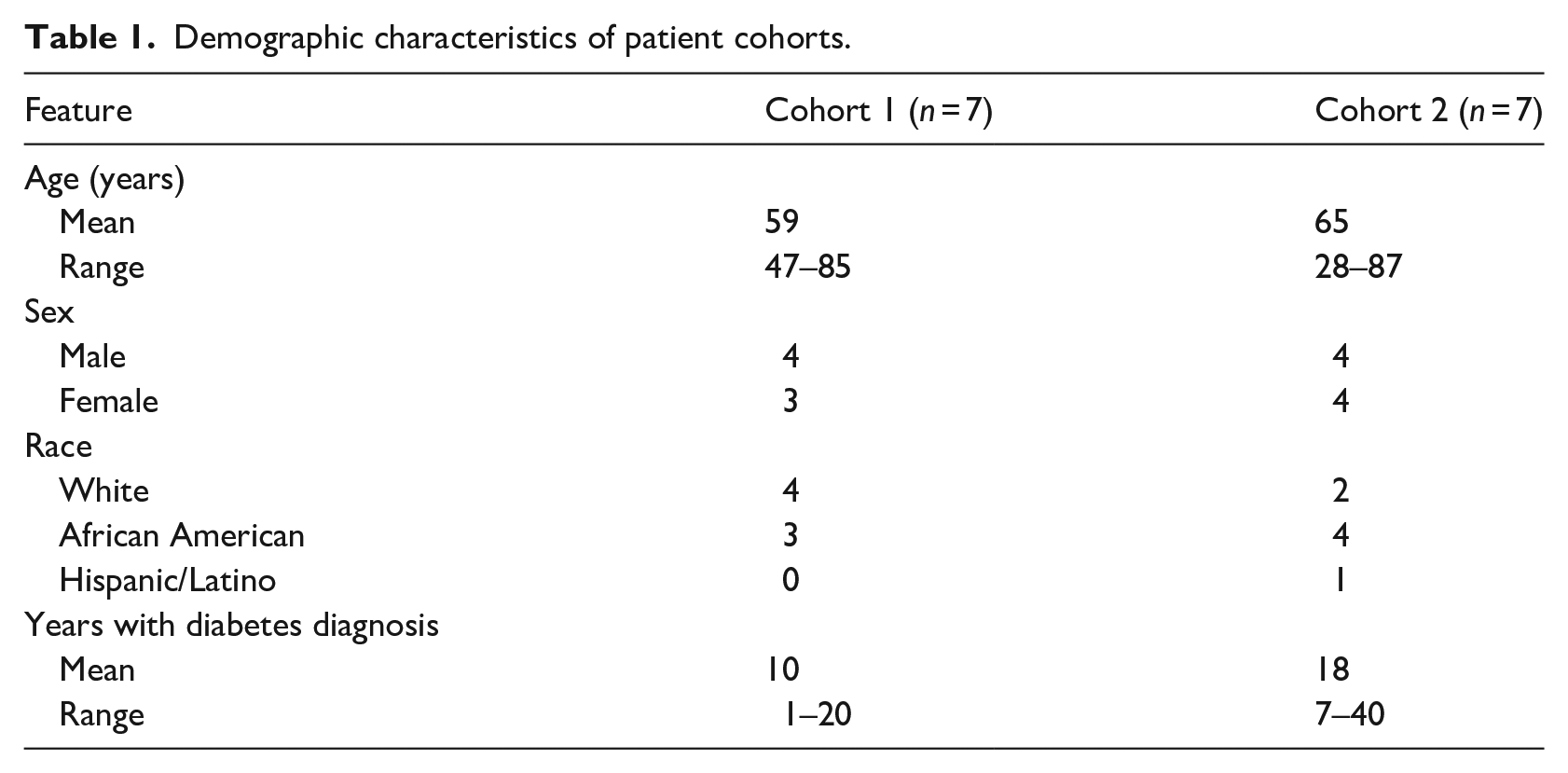
Four retina physicians and 14 individuals with DR agreed to participate in this study. Of the participants with DR, seven were interviewed for initial needs assessment (Cohort A) and seven participants piloted the video (Cohort B). The demographic details of these participants are presented in Table 1. Notably, most participants had long-standing diabetes, with participants in Cohort A having a mean of 10 years since diagnosis (range: 1–20 years) and participants in Cohort B having a mean of 18 years since diagnosis (range: 7–40 years).
Demographic characteristics of patient cohorts.
Participants varied in their self-reported knowledge of diabetes (Table 2). On a 10-point scale (1 [least] to 10 [most]), participants in Cohort A had a mean diabetes knowledge of 6.4, while those in Cohort B had a mean score of 4.4. This number increased to 7.9 after viewing our educational video (p = .038). Furthermore, in Cohort A, 100% of participants expressed interest in the idea of utilising animated videos in DR patient education.
Self-reported patient understanding of diabetes.
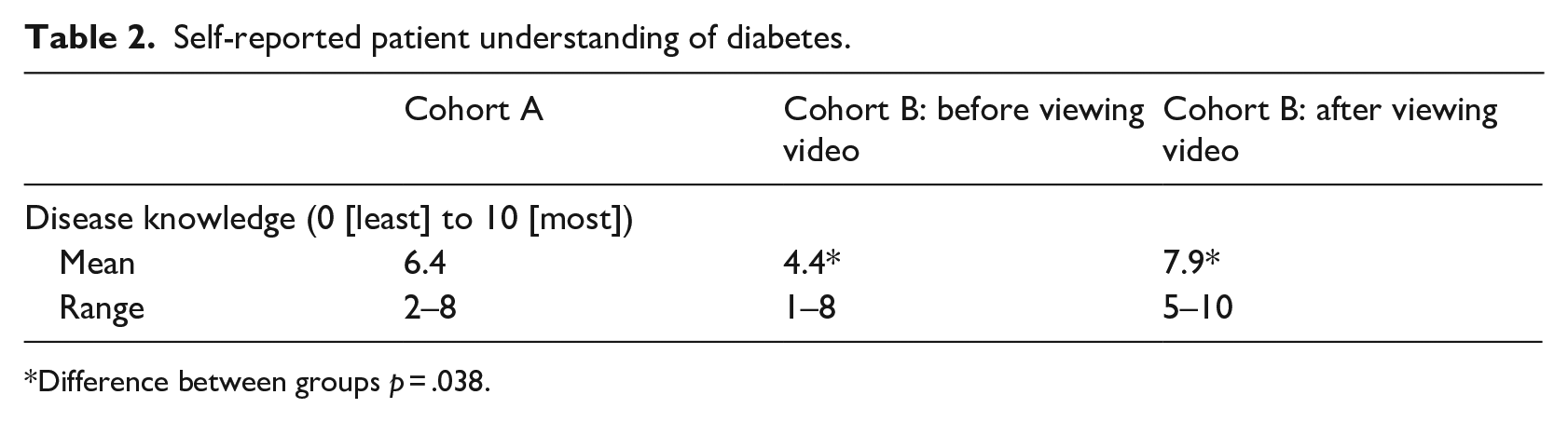
Difference between groups p = .038.
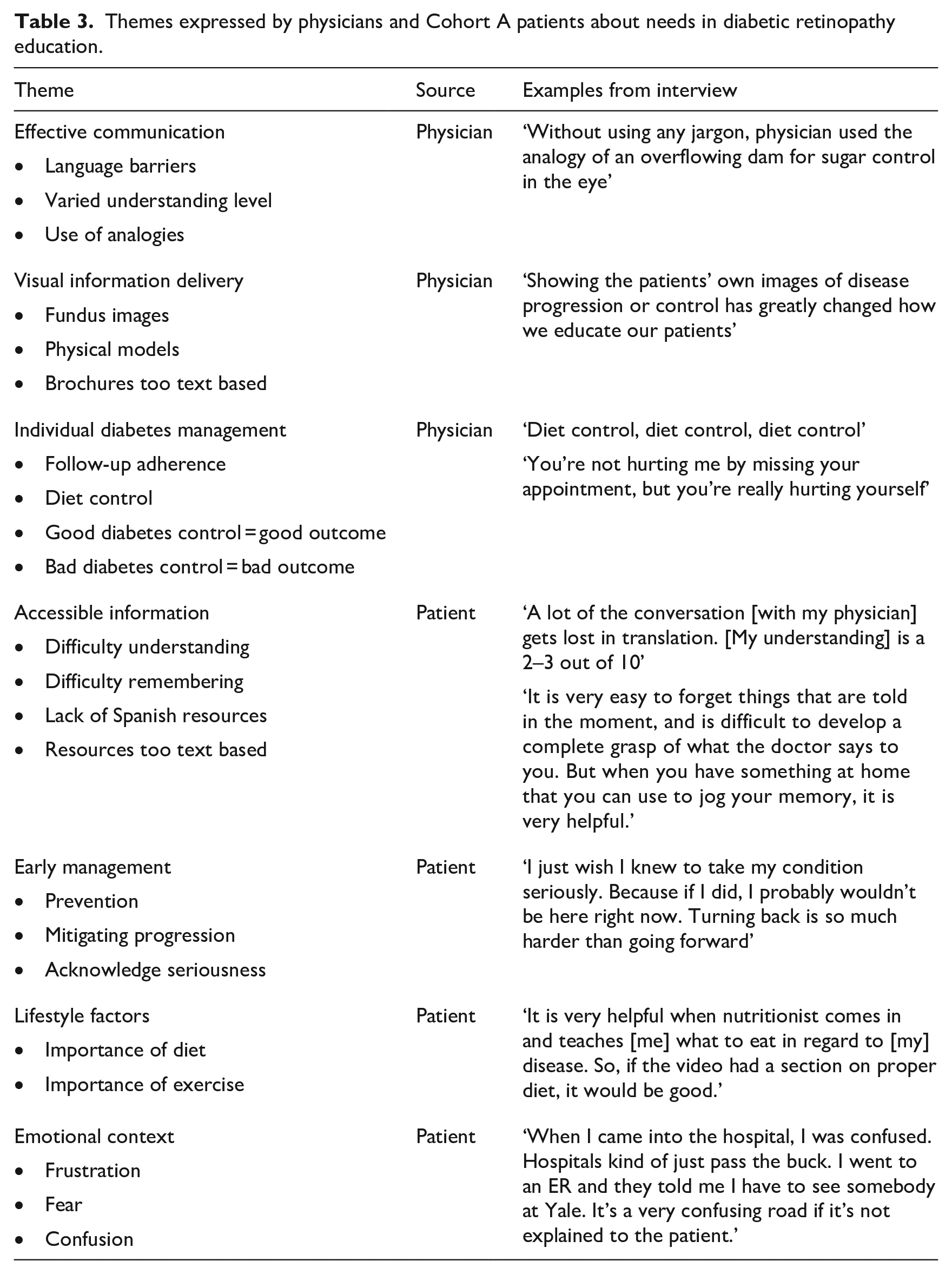
Themes collected about needs in an educational video in Cohort A included accessible information, early management, lifestyle factors and emotional context (Table 3).
Themes expressed by physicians and Cohort A patients about needs in diabetic retinopathy education.
Accessible information
Participants emphasised the need to make any educational materials accessible to a range of patients. Several participants reported difficulty understanding both doctors’ explanations and self-discovered online resources. Participants noted in particular the paucity of information in Spanish. One participant noted that due to language barriers, ‘a lot of the conversation gets lost in the translation’. Another participant explained while some text-based resources exist, they are difficult for her to read and understand due to her lack of schooling.
Early management
Several participants noted that patient education should emphasise the early management of one’s diabetes. Participants described the importance of preventing disease altogether and of mitigating disease progression early. Participants noted that understanding the gravity of the disease early makes it easier to control. One participant said that early intervention is crucial because DR will ‘sneak up on you’.
Lifestyle factors
Participants noted the importance of education about lifestyle factors such as diet and exercise. One participant described the benefit of speaking to a nutritionist about a healthy diet in the context of diabetes. Another participant reported that avoiding sugary foods was discouraged in her family and highlighted the need to thoroughly discuss the dietary implications of living with diabetes.
Emotional context
Many participants described the emotional context surrounding their diagnosis and treatment. Participants described frustration with tests taking too long, with not seeing immediate results following treatment and with the worsening of their disease.
One participant expressed feeling constantly confused by the hospital. Another participant explained her fear, saying ‘[my] main concern now is regarding [my] eye. [I am] afraid of what is going to happen’.
Themes from interviews conducted with retina physicians included effective communication, visual information delivery and individual-level diabetes management (Table 3).
Effective communication
Retina physicians described tailoring their language to fit a patient’s needs. The physicians said that since patients come in with differing knowledge bases, they direct conversations to a patient’s level of understanding. One retina physician described the importance of using clear communication during a patient’s first visit, saying: ‘if you don’t spend the time up front to explain what’s going on, then you’ve lost the patient already’. He added that many patients will not ask questions or admit to not understanding. To aid patient understanding, several physicians described using simple analogies to explain pathological processes in DR. Retina physicians also noted the challenge that language barriers pose, even with the use of an interpreter. Furthermore, they noted that many currently available educational materials are tailored to a much higher level of understanding than that of many of their patients, rendering these resources useless. One physician also emphasised that patients often do not process information in the moment at the clinic, pointing to a potential benefit of a resource that can be referenced after the patient has left the doctor’s office.
Visual information delivery
Several retina physicians noted the educational value of sharing a patient’s fundus photo with them, either showing their progression across time by displaying images taken from multiple visits or showing the state of their disease by juxtaposing the patient’s photo next to a ‘normal’ fundus image. Retina physicians described increased patient engagement and understanding when presented with these images. Physicians also described the highly text-based nature of available educational brochures and pamphlets. They noted that the lack of visual engagement makes these pamphlets difficult to understand for patients with low medical knowledge.
Individual-level diabetes management
Finally, retina physicians emphasised that patients should be encouraged to recognise the serious importance of managing their diabetes well. Retina physicians noted the individual-level responsibility that patients must take to control the disease. Several physicians stressed that patients must maintain regular follow-up visits with both their ophthalmologist and their primary care physician or endocrinologist. Retina physicians also highlighted the importance of diet control in managing diabetes. In explaining the value of good diabetes management and, conversely, the consequences of poor management, one physician said: ‘If you follow your sugars, letting me know if there are any changes, and follow up as scheduled, there is a higher likelihood your vision will not deteriorate’.
We incorporated this feedback and employed a user-centred design (UCD) to create a 6-minute animated video which we then uploaded to YouTube (Figure 1). This video was iteratively improved with feedback from the retina physicians who were previously interviewed.
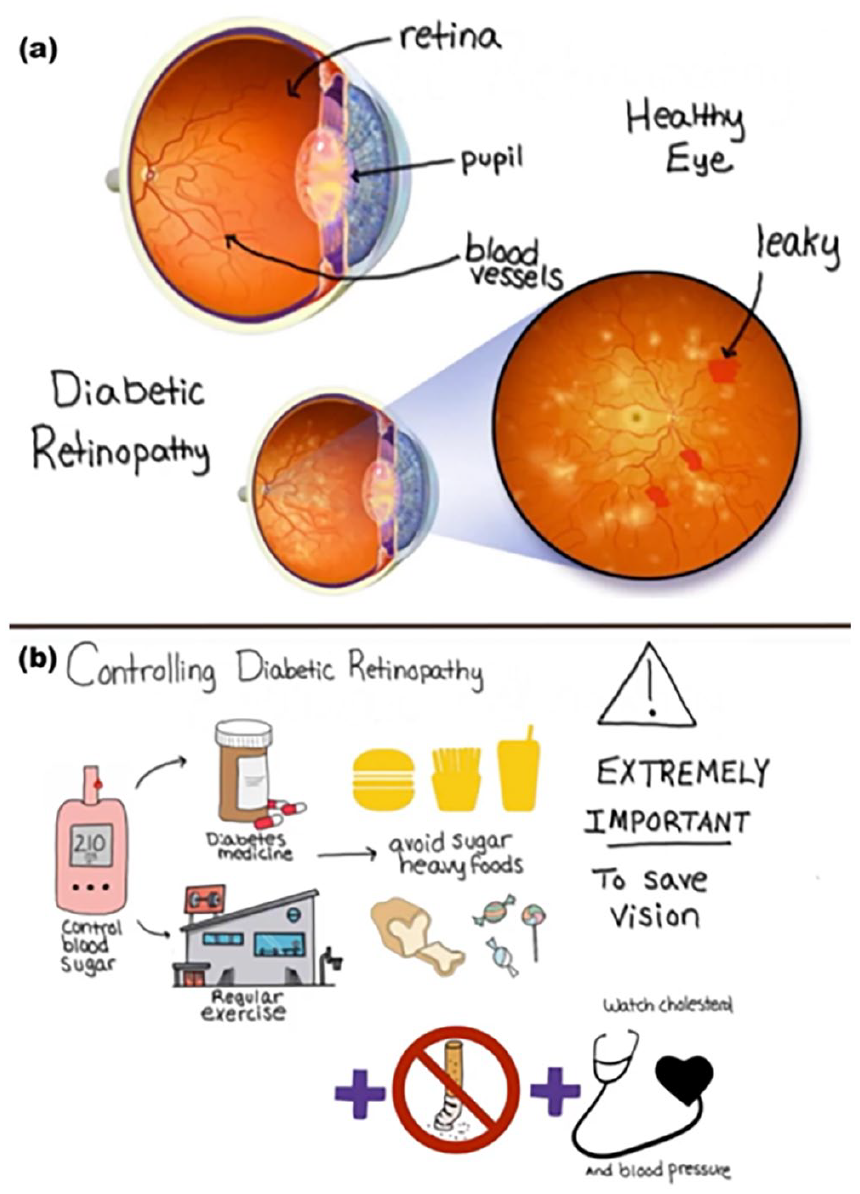
Screenshot of the white board animated video demonstrating (a) an explanation of fundus photos and (b) an explanation of dietary and lifestyle measures to control diabetes.
Physician and patient feedback informed the following specific UCD elements to enhance accessibility: we produced a script for video narration that was at a ninth-grade level on the Flesch-Kincaid readability index; employed large font and minimal text in the video; used multiple diagrams, fundus photos and animations; employed a high contrast colour scheme including black text on white screen; used metaphors for eye anatomy and narrated the video at a slow pace. Text was written out slowly and displayed for an extended time to let all readers follow along. By drawing the text in a white board format, we also improved the ease of following along, as compared to static slides which can be difficult to read.
The video was presented to participants in Cohort B. One hundred per cent of participants found the video to be effective in teaching them about DR. Specifically, when asked about the helpfulness of the section describing DR using fundus photos, five out of seven participants strongly agreed, whereas one participant agreed and one was neutral.
Themes extracted from interviews with participants in Cohort B following viewing the video are presented in Table 4. Participants commented on the increased accessibility of educational videos versus print material. They felt that video-based education engaged them more compared to traditional print education, which they were more accustomed to reading. They also felt that despite their previous understanding of the disease, they still significantly increased their knowledge about DR through the animations and explanation of fundus photos in the video. Of note, participants felt that an educational video alongside a print brochure would be most effective.
Themes expressed by Cohort B patients after viewing the educational video.
Discussion
In this needs assessment and pilot study of a novel animated video to educate patients about DR, we showed that retina physicians and patients demonstrated great interest in video-based patient education. Furthermore, we showed that retina physicians and patients have a specific list of needs that, if addressed appropriately in a video, could result in improved patient engagement and self-reported understanding of their disease.
Prominent themes on needs assessment in DR reported by physicians included effective communication, visual information delivery and individual-level diabetes management. Thus far, there is limited research in the USA that systematically studies each of these topics. Tailoring language to the physician’s perceived level of patient understanding is common. Metaphors, for example, are frequently used to simplify concepts in medical education. Medical students and patients are often educated with analogies to glaucoma as an overflowing sink or DR manifesting with leaky vessels (Baker et al., 2013). The effectiveness of these strategies, however, has not been studied in DR. Similarly, while many physicians use visual representations such as fundus photos to personalise education for patients and empower them to learn about their disease, the effectiveness of this strategy has not been studied among patients with DR or in any other disease in ophthalmology. Studies do suggest that providing patient education may increase patient knowledge about DR and increase compliance to follow-up examinations (Beaser et al., 2018; Moinul et al., 2020). However, these studies provided participants with large amounts of information encompassing several learning objectives. While these educational interventions did include information about the link between poorly controlled diabetes and vision problems, further research should be done on the effectiveness of specifically emphasising diabetes management through medical, dietary and exercise regimens to patients. Each of these topics merits additional study to elucidate how effective they may be in isolation and in conjunction. In our pilot study, we combined these techniques in a video and showed that the resulting product was highly favoured by patients and improved their subjective disease understanding on a 10-point scale from 4.4 to 7.9 (p = .038).
We also collected themes from participants in Cohort A that included accessible information, early management, lifestyle factors and emotional context. Similarly, prior studies of patients with diabetes, prediabetes and of diabetic nutritional counselling have also identified high patient informational needs regarding course of the disease, lifestyle adjustments, psychosocial wellbeing (including mental strain and support) as well as requests for simple visual resources adapted to their level of knowledge; additional highly prioritised information needs, which were not highlighted by patients in the present study, included diabetes research, treatment/therapy and sleep (Ghisi et al., 2021; Grobosch et al., 2018; Zhang et al., 2019). Participant needs were engaged with in our video by employing a simple white board format with clear language and making the video YouTube accessible, emphasising the asymptomatic nature of the disease and providing basic dietary counselling. The emotional context of DR is an additional issue which warrants consideration, especially as emotional factors such as fear of receiving bad news and fear of painful or unknown procedures have been noted by prior studies as reasons DR patients fail to attend screening appointments (Fairless and Nwanyanwu, 2019; Piyasena et al., 2019). Although not directly addressed in our video, emotional concerns may be discussed by the physician in the office.
The video was received well by participants in Cohort B, who commented on the increased engagement and accessibility this video provided compared to previous resources they have used. Of note, some participants also indicated that a combination of video and printed material may help them remember concepts better than just a video or brochure alone. The application of multiple interventions, such as a video in conjunction with a brochure, has indeed been shown to increase the likelihood of success of media campaigns to change health-related behaviours (Wakefield et al., 2010). Further studies should be done on the most effective way to disseminate a multi-pronged media approach to create an evidence-based education strategy.
Strengths and limitations
Strengths of this study include our attention to both physicians and patients in the creation of our educational intervention. While some evidence has shown that video-based education can improve DR patient knowledge and adherence to screening, few studies have consulted both retina physicians and DR patients to best guide the development of such a video, and our literature review revealed none that did so in a US population (Basch et al., 1999; Meyer et al., 2016; Piyasena et al., 2019; Ramagiri et al., 2020).
Themes gathered from patient and physician interviews guided the development of a white board animated video which was effective in improving patient self-reported disease understanding, engagement and accessibility. While the clinical management of DR differs worldwide, the primary tenets remain the same, and the fundamental knowledge presented concisely and accessibly in our video stands to reasonably benefit all patients with DR. In particular, those who are newly diagnosed, have low health literacy or are socioeconomically disadvantaged may especially benefit from such a resource. While developed at a large US eye centre, this video tool has potential generalisability beyond this setting given the key educational elements regarding sugar and blood pressure control, smoking cessation and follow-up with screening and doctor visits as able, which are applicable in most health settings. The video may be easily adapted, with language translation if necessary, to be appropriate for use in diverse settings and contexts including resource-poor countries. Alternative novel educational media such as virtual reality and interactive mobile applications may appeal to limited audiences; however, while these technologies are not always available in resource-limited settings, our video tool may be implemented widely given the wide availability and familiarity with video sharing platforms. We hope to further study our intervention’s effectiveness in a larger cohort, translate our video into multiple languages and test whether this intervention, in addition to increasing subjectively perceived knowledge about DR, also improves objective tested knowledge, disease outcomes and adherence to follow-up appointments.
This study had several limitations. First, since this was a small single-centre pilot study, we were unable to collect data and opinions from a broad and diverse range of physicians and patients. However, we hope that the initial themes generated from the in-depth interviews in this study can be validated with larger sample sizes in future studies. Second, our study has an inherent selection bias because participants were recruited from the Yale Eye Center. Our sample also consisted of people already presenting to clinics for DR care, and thus these participants are likely to have a greater exposure to DR information than those who are not participating in screening and treatment. Future validating studies might recruit participants through other methods, such as general public outreach, to reach people who are not regularly accessing screening.
Conclusion
In conclusion, we performed a pilot study of video-based education in DR using a thematic framework elucidated from patients and retina physicians. Our prospectively validated video increased diabetes knowledge among people with DR and may be an effective method for delivering accessible and accurate information across a range of relevant contexts and settings.
Footnotes
Acknowledgements
The authors thank the participants who kindly shared their experiences and the physicians and staff at the Yale Eye Center who made coordination of the project possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this publication was made possible by Grant Number 1 K23 EY030530-01 from the US National Eye Institute, a Yale Diabetes Center (grant no. P30 DK045735) and the Doris Duke Fund to Retain Clinical Scientists. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the US National Institutes of Health. This work has been supported in part by an unrestricted/challenge award to Yale Eye Center from Research to Prevent Blindness (RPB), Inc.