
Abstract
Objective:
The objectives of this study were to examine the efficacy of a group-based coaching intervention on office workers’ leisure-time physical activity (LTPA), to identify potential differences in effects based on age, education, baseline physical activity status (BPAS) and gender, and to determine perceived satisfaction with the intervention.
Design:
The study used a single-group pre- and post-test design with post-tests conducted 8 weeks from baseline. Thirty-nine office workers were enrolled in the study, and 35 were included in the analysis.
Setting:
The intervention was conducted at six workplaces located in southern Sweden.
Method:
The Godin Leisure Time Exercise Questionnaire was used to measure LTPA, and a five-item questionnaire was used to identify perceived satisfaction with the intervention. A repeated measures ANOVA was conducted for the statistical analysis.
Results:
The mean perceived satisfaction with the intervention was 20.1, where 25 was the highest possible score. LTPA increased significantly from pre- to post-test (p < .001). A significant time × age interaction indicated smaller increases in LTPA among older participants. No significant moderation effects were observed for BPAS, education, or gender. The proportion of participants classified as active increased from 17.1% at pre-test to 45.7% at post-test.
Conclusions:
This brief coaching intervention was well received and associated with increased LTPA among office workers, with smaller increases observed among older participants. However, causal conclusions cannot be drawn due to study limitations, and future randomised controlled trials with objective PA measures are needed.
Keywords
Introduction
Physical activity (PA) has been associated with improved mental and physical health, cognitive functioning, and sleep (Arem et al., 2015; Buecker et al., 2021; Pearce et al., 2022; World Health Organization [WHO], 2020). In addition, PA is most beneficial for physically inactive populations due to a diminishing marginal utility (Arem et al., 2015; Pearce et al., 2022). PA is defined as any bodily movement the skeletal muscles produce that increases energy expenditure (WHO, 2020). Adults are recommended to be engaged in aerobic PA for at least 150–300 min per week with a moderate intensity, alternatively 75–150 min with a vigorous intensity (WHO, 2020). Physical inactivity is defined as not meeting the WHO recommendations for PA, which has increased substantially in past decades (Guthold et al., 2018; The Public Health Agency of Sweden, 2024; WHO, 2020).
The overall decreasing amount of PA in the adult population has a substantial economic impact due to healthcare-related costs (Santos et al., 2022), signalling the need to promote PA among members of this population. A major reason for the increasing physical inactivity is the rapid digitalisation of society, particularly within workplaces, as workplaces in modern society are often office-based and associated with high levels of sedentary behaviour and low PA (Prince et al., 2019). Also, adults spend most of their awake time at the workplace, indicating that the workplace may significantly impact adults’ health outcomes. Recent studies found that high PA levels may counteract or eliminate the detrimental effects of sedentary behaviour, and leisure time PA (LTPA) may be particularly beneficial for workers with low occupational PA (Ekelund et al., 2016; Prince et al., 2021). LTPA may also benefit the organisation by reducing absenteeism and presenteeism among employees (Conn et al., 2009; Santos and Miragaia, 2023). Thus, finding strategies to promote LTPA among office workers is urgent.
A potential strategy to promote PA is through interventions, utilising behaviour change techniques (BCTs) to support individuals to increase their PA (Michie et al., 2013). The effectiveness of PA behaviour change interventions may however be moderated by sample characteristics, such as education, age, gender, and baseline physical activity status (BPAS), due to, for example, different motives and preferences for being active or different perceived barriers and facilitators for PA (Bukman et al., 2014; Knapova et al., 2024; Luten et al., 2016; To et al., 2021; Western et al., 2021; Wilcox et al., 2009). Identifying for whom interventions work best has valuable implications, as it facilitates the development of tailored interventions or may serve as information to improve interventions for various subgroups.
The workplace is considered an ideal setting for promoting PA due to high accessibility and the possibility of reaching diverse people. Thus, finding efficacious workplace interventions to promote PA is warranted (Wills, 2023). Interventions conducted in the workplace setting aiming to increase adults’ PA levels have shown promising, albeit inconclusive results, but more research is needed to determine the most efficacious and effective BCTs (Conn et al., 2009; Gawlik et al., 2023; Krebs et al., 2019b; Lock et al., 2021; Madden et al., 2020; Malik et al., 2014; Ramezani et al., 2022; Taylor et al., 2012). However, interventions utilising a combination of BCTs that focus on motivational (e.g. goal-setting, autonomy support) and volitional determinants (e.g. action-planning, self-monitoring, problem-solving) may be useful strategies for promoting PA among employees (Gawlik et al., 2023; Krebs et al., 2019b; Lock et al., 2021; Peng et al., 2022; Sun et al., 2022). Evidence also indicates that group-based, utilising face-to-face communication, focusing solely on PA behaviour, and social support may be efficacious intervention characteristics (Conn et al., 2009; Gawlik et al., 2023; Krebs et al., 2015; Madden et al., 2020; Malik et al., 2014; Rhodes et al., 2017; Ryom et al., 2023; Smith et al., 2023). In addition, theory-driven PA interventions may help identify themechanisms by which an intervention contributes to its outcomes (McEwan et al., 2019; Rimer and Glanz, 2005; Taylor et al., 2012).
Based on these empirical findings, intervention interventions that are theory driven, motivational and volitional focused and group-based, and which employ face-to-face communication and promote social support within a workplace intervention seems promising. MoVo-work is a workplace intervention (Krebs et al., 2019b) that seeks to integrate motivational theory (e.g. Theory of Planned Behaviour: Ajzen, 1991) with volitional theory (e.g. Health Action Process Approach: Schwarzer, 2008), hence the acronym MoVo. MoVo-work, which consists of both coaching and exercise sessions, is based on the theoretical rationale provided by the MoVo model (Fuchs, 2007) and has shown promising results in earlier studies aimed at increasing LTPA among employees. However, to the best of our knowledge, it has yet to be explicitly evaluated with office workers in a Swedish context (Krebs et al., 2015, 2019b). Furthermore, evaluating a scaled-down version of MoVo-work focusing solely on the coaching component may provide insight into more scalable and resource-efficient intervention formats.
Relating to the urgency of promoting LTPA among office workers and the heterogeneity in results of PA behaviour change interventions in the workplace setting and for whom it is most effective, more research is warranted. Results from the present study may have high relevance not only for public health but also from a business perspective, where employers may welcome the identification of effective interventions to increase employee health status. In addition, evaluating perceived satisfaction with the intervention is crucial, as a programme or intervention that is not well received by the target group will unlikely be sustainable, independent of efficay and effectiveness (Wills, 2023). Given this, this study aimed to address this knowledge gap by (a) evaluating the efficacy of a group-based coaching intervention on office workers’ LTPA levels; (b) determining potential differences in efficacy based on age, education, BPAS, and gender; (c) determining perceived satisfaction with the intervention.
Method
Study design
A quantitative intervention study based on a quasi-experimental one-group design with pre- and post-test was conducted.
Study participants and setting
In this study, it was determined to detect a medium effect size (d = 0.5) based on changes in PA levels, requiring a total of 34 participants, according to a power analysis conducted in G*Power, using a significance level of .05 and a statistical power of 0.8.
Inclusion criteria were workplaces in south Sweden and office workers who wished to increase their LTPA levels. As this was a group-based intervention, at least three participants per workplace were required to be enrolled in the study. Forty-seven office workers were initially approached and eligible for participation, of which 39 provided informed consent and were enrolled in the study (i.e. 83% recruitment rate). Twelve participants had a higher LTPA than the predetermined inclusion criteria at baseline (i.e. reported more than two weekly strenuous/moderate exercise sessions) out of whom six participants were classified as solely moderately active, indicating that these could potentially gain significant health benefits by increasing their activity levels (Godin, 2011). Thus, it was decided to keep these participants in the study in order to achieve an adequate sample size and power. Three participants from one company dropped out of the study during the intervention, and one participant from another company was lost to follow-up, resulting in a 10% attrition rate. Thirty-five participants completed both pre- and post-tests (see Figure 1). The intervention was conducted in six office workplaces, in three municipalities in southern Sweden between March-June 2024.
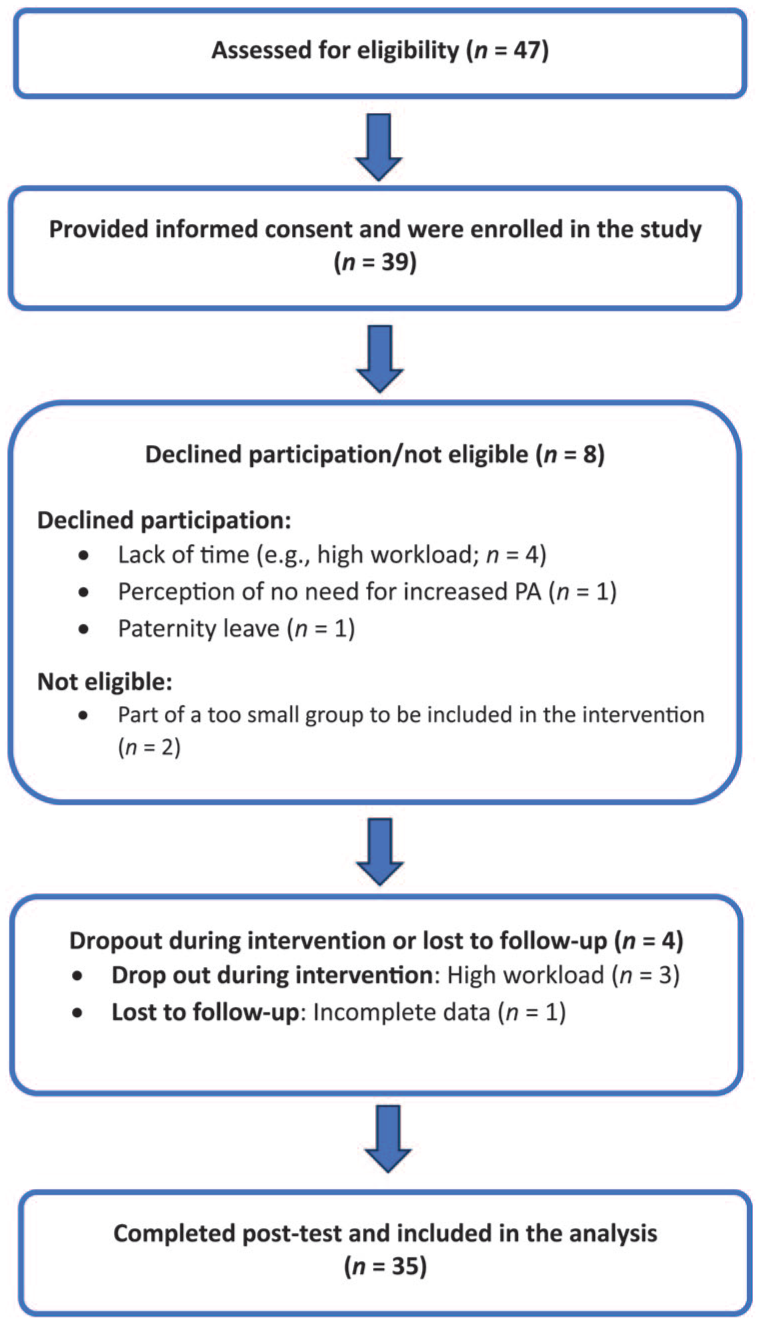
Participant flow diagram.
Procedure
Office workers were recruited through a convenience sampling by telephone and email contact with the manager or HR department at the selected companies. Leaflets describing the study were emailed tocompanies’ representatives (manager, HR department), who disseminated them to office workers. Office workers interested in participating contacted their companies’ representatives, who then emailed the responsible researcher (OA) with the contact information of those workers. Eail contact was initiated with interested office workers, providing details of when and where the sessions were scheduled, and participant information sheets and consent forms where distributed. Participants were encouraged to ask any questions regarding the intervention and participation to the researcher (OA).
Intervention
The intervention consisted of four group-based coaching sessions for 20–30 min each and a brief individual phone call based on the coaching element of MoVo-work. Sessions were delivered in a manner aligned with a standardised course instructor manual (Krebs et al., 2019a) once a week, face-to-face, at the workplaces, with three to nine participants in each coaching group.
Prior to the intervention, the manual had been translated from German to Swedish using Google Translate. Minor linguistic adjustments were made during the translation process: where direct translations that did not fit well in the Swedish context, they were replaced with conceptually equivalent terms more appropriate for Swedish language use. Participants who were unable to attend the workplace due to geographical barriers could participate digitally via Microsoft Teams. The intervention content, presentation structure, and materials were identical in both in-person and digital sessions to minimise variability in delivery. Although no formal fidelity checklist was used, the intervention was delivered according to the predefined structured manual to ensure consistency in delivery across sessions. Written information regarding the meeting content and task instructions was emailed to those who missed a meeting. The coaching sessions were delivered by OA, who holds a bachelor’s in social science with a major in pedagogy.
During the first session, participants were given a personal LTPA book, outlining various tasks to be performed (e.g. developing goals, activities, and action plans). At the first meeting, participants identified their outcome goal of becoming more physically active, which was written on a motivational poster that was displayed for the participants in each session. Before the next meeting, participants were asked to identify three LTPA ideas based on three criteria (i.e. autonomous motivating, realistic, and aligned with their outcome goal). In a second meeting, barriers to LTPA and relevant counter-strategies were discussed. Predefined examples of counter-strategies were also presented, and participants individually identified their preferred counter-strategies.
Criteria for action plan design were then presented (plans should be precise: specifying what, when, where, with whom), and participants were reminded to keep in mind their personal PA ideas when choosing an activity. In a third meeting, discussion about social support for PA took place, where examples of support options were described, and participants were encouraged to create a support plan in consultation with a person in their vicinity. In a fourth and final meeting, participants presented their action- and social support plans for the group, and received a template for self-monitoring their activity over the next 4 weeks. Three weeks after the fourth session, participants received a phone call in which a discussion was held about the implementation success rate of the action- and support plans, as well as perceived barriers and counter-strategies. Strategies to deal with potential future barriers were also discussed.
Measures
Baseline measurements were conducted adjacent to the first session in the workplace, measuring demographics and LTPA. Follow-up measurements were conducted 2 weeks after the end of the intervention (i.e. 8 weeks after baseline) by means of answers to questionnaires on LTPA and perceived satisfaction with the intervention, both at the workplace and digitally.
Demographic variables
Demographic information concerning age, gender, and education was collected at baseline. Education was categorised as the highest level attained—elementary school, high school, or higher education. However, due to a small numbers of participants within the elementary school category, elementary and high school were combined together as one category in the analysis.
Primary outcome
Leisure-time physical activity
LTPA was measured using the validated Leisure Time Exercise Questionnaire (LTEQ), which contained questions about the number of times during the last week that had been spent in light, moderate, and strenuous physical activities, respectively, for at least 15 min (Godin and Shephard, 1985). Imprecise answers, such as “2–3 times,” were registered as 2.5 times (i.e. a number in between). Weekly activity score was calculated by multiplying the scores of light activities by three, moderate activities by five, and strenuous activities by nine and adding these together to create a total sum (LTEQ leisure score index). An LTPA classification was calculated by summing the scores from only moderately and strenuously active activities, based on Godin (2011). Scores <14 were interpreted as inactive, 14–23 as moderately active, and ⩾24 were considered active (Godin and Shephard, 1985).
Baseline physical activity status (BPAS) was assessed by a single item from the questionnaire, asking how often the participant performed an activity intense enough to sweat during a week, with the options of never/rarely, sometimes, or often. Due to an uneven distribution of participants across these response categories, and because the variable was to be included as a between-subjects factor in subsequent analyses, the variable was dichotomised into “never/rarely” and “sometimes/often.”
Secondary outcome
Perceived satisfaction with the intervention
Perceived satisfaction with the intervention was measured using a five-item questionnaire (e.g. the content of the intervention corresponds to what I need to do to become more physically active) based on a five-point Likert-type scale. The total sum for the five items was calculated, and higher scores were interpreted as higher perceived satisfaction with the intervention, with 25 being the highest possible score. The perceived satisfaction instrument had high reliability (Cronbach’s α = .86).
Statistical analysis
Data were analysed using IBM SPSS Statistics version 27. A complete case analysis was conducted including participants who completed both pre- and post-tests, regardless of attendance rate. Descriptive statistics were calculated as means, standard deviations, and percentages for demographic variables. Perceived satisfaction with the intervention was summarised using means, standard deviations, and minimum–maximum values.
A repeated measures ANOVA was conducted to examine changes in LTPA from pre- to post-test. Time was independently analysed as a within-subject factor in the first model, while age was included as a covariate in the second model. Furthermore, BPAS (i.e. sometimes/often, never/rarely), education, and gender were examined as between-subject factors. Given the small sample size, moderation analyses were treated as exploratory. Intraclass correlation coefficients (ICC) were calculated descriptively to explore the potential clustering of participants within workplaces.
Levene’s test was utilised to check the assumption of homogeneity of variances, and the assumption was not violated for any independent variable (p > .05). Based on the Shapiro–Wilk test, the assumption of normality was not met for the LTPA post-data (p < .05). Outliers in the LTPA post-data contributed to positive skewness and leptokurtosis (3.18). Thus, a square-root transformation was applied to the LTPA data, with the newly transformed LTPA data now meeting the assumption of normality (p > .05). Skewness (pre-test: 0.81, post-test: 0.90) and kurtosis (pre-test: 0.74, post-test: 0.94) were within the acceptable range. Statistical tests were conducted on square-root-transformed data to meet model assumptions. However, to increase transparency and facilitate interpretation, the ANOVA results for both the transformed and back-transformed data are presented in Table 2 (together with pre- and post-test means, 95% confidence intervals for mean differences, p-values, and effect sizes).
Changes in LTPA classification (inactive, moderately active, active) from pre- to post-test were examined using the Marginal Homogeneity test for paired categorical data. A significant result indicates that the distribution of participants across activity categories differed between the two time points. A statistical significance level of p < .05 was applied. Effect sizes were calculated and reported based on partial η2, where values of 0.0099, 0.0588, and 0.1379 were interpreted as small, medium, and large effect sizes, respectively (Richardson, 2011).
Ethics
Ethical approval for the study was provided by the Swedish Ethical Review Authority (Reference: 2023-07961-01), and the study was conducted in line with the World Medical Association Declaration of Helsinki (World Medical Association, 2013). Informed consent was obtained from participants, with information sheets about the study being provided by email or in person. Participants’ personal data were stored safely, without access by persons other than the study team, and with the data being used for research purposes only.
Results
Baseline data
Of the 39 eligible participants enrolled in the intervention, 35 completed both pre- and post-tests and were included in the analysis, resulting in a 10% attrition rate. Dropouts and completers did not differ in baseline LTPA (dropouts: M = 23.63, SD = 8.18; completers: M = 22.34, SD = 14.42).
The demographic characteristics of the participants are summarised in Table 1. Participants were predominately above 30 years of age (i.e. 94.3%); there was an even distribution of primary/high school- and higher-educated participants, and an even distribution of men and women. Most participants were labelled as insufficiently active (45.7%), followed by moderately active (37.1%), and very active (17.1%), based on predefined categories derived from the baseline LTPA data. The mean attendance rate in the intervention was 4.46 out of five (SD = 0.78). Twenty-one participants (60%) attended all five coaching sessions, 10 participants (28.6%) attended four sessions, three participants (8.6%) attended three sessions, and one participant (2.9%) attended two. Thus, 88.6% attended all sessions or missed only one of them (n = 31).
Demographic characteristics and baseline data.
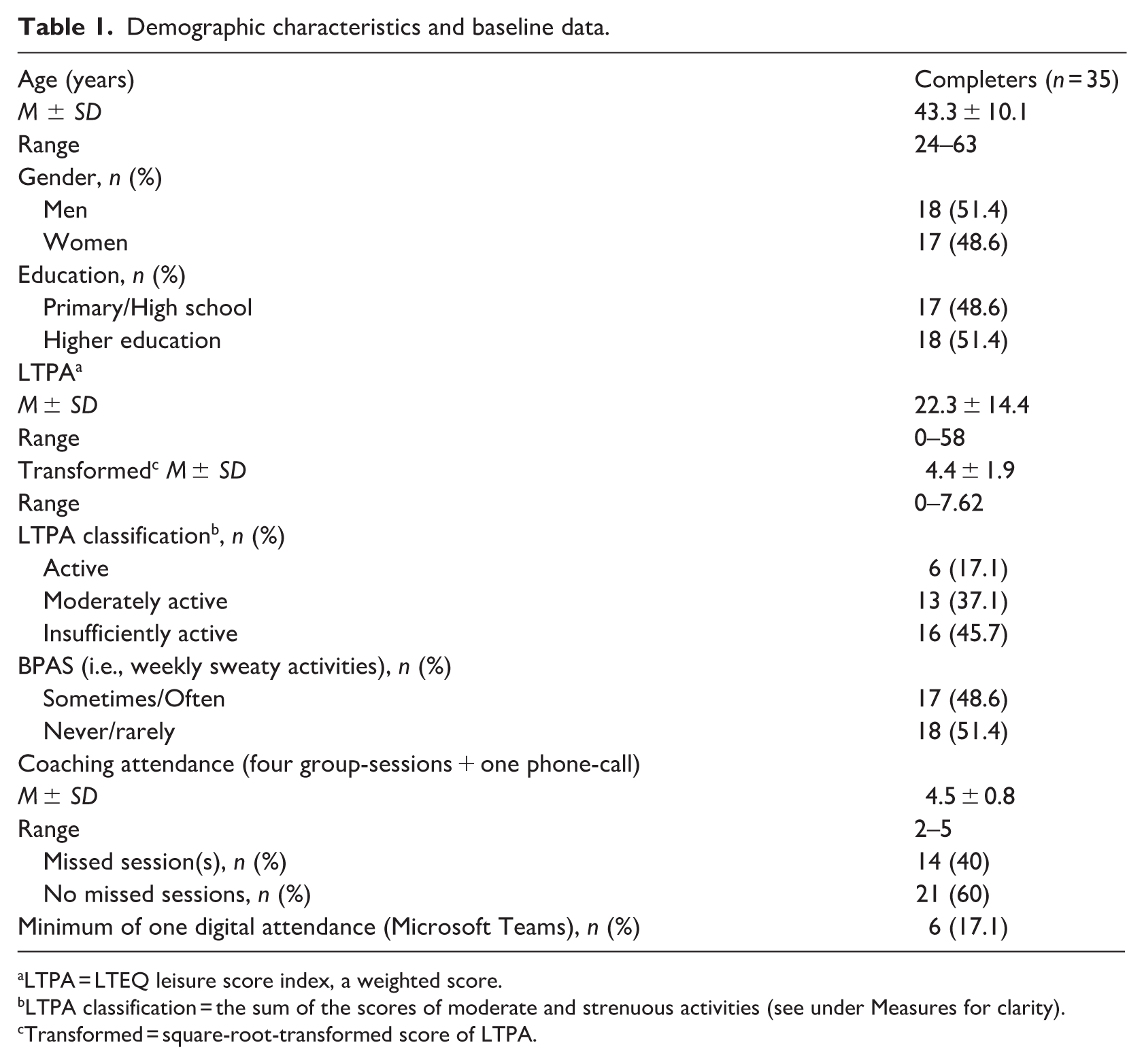
LTPA = LTEQ leisure score index, a weighted score.
LTPA classification = the sum of the scores of moderate and strenuous activities (see under Measures for clarity).
Transformed = square-root-transformed score of LTPA.
The mean perceived satisfaction with the intervention was 20.1 (SD = 2.96) out of 25, with minimum-maximum values of 13–25.
Changes in LTPA from pre- to post-intervention
The results of this analysis are summarised in Table 2. They showed a significant main effect of time on LTPA, F(1, 34) = 18.11, p < .001, partial η2 = 0.35. A significant time × age interaction effect was also identified, F(1, 33) = 5.74, p = .022, partial η2 = 0.15. The time × age interaction effect was negative (i.e. higher age = smaller increases of LTPA). The significant main effect of time on LTPA remained when adjusting for age, although it was slightly attenuated, F(1, 33) = 11.23, p = .002, partial η2 = 0.25.
Results from repeated measures ANOVA.
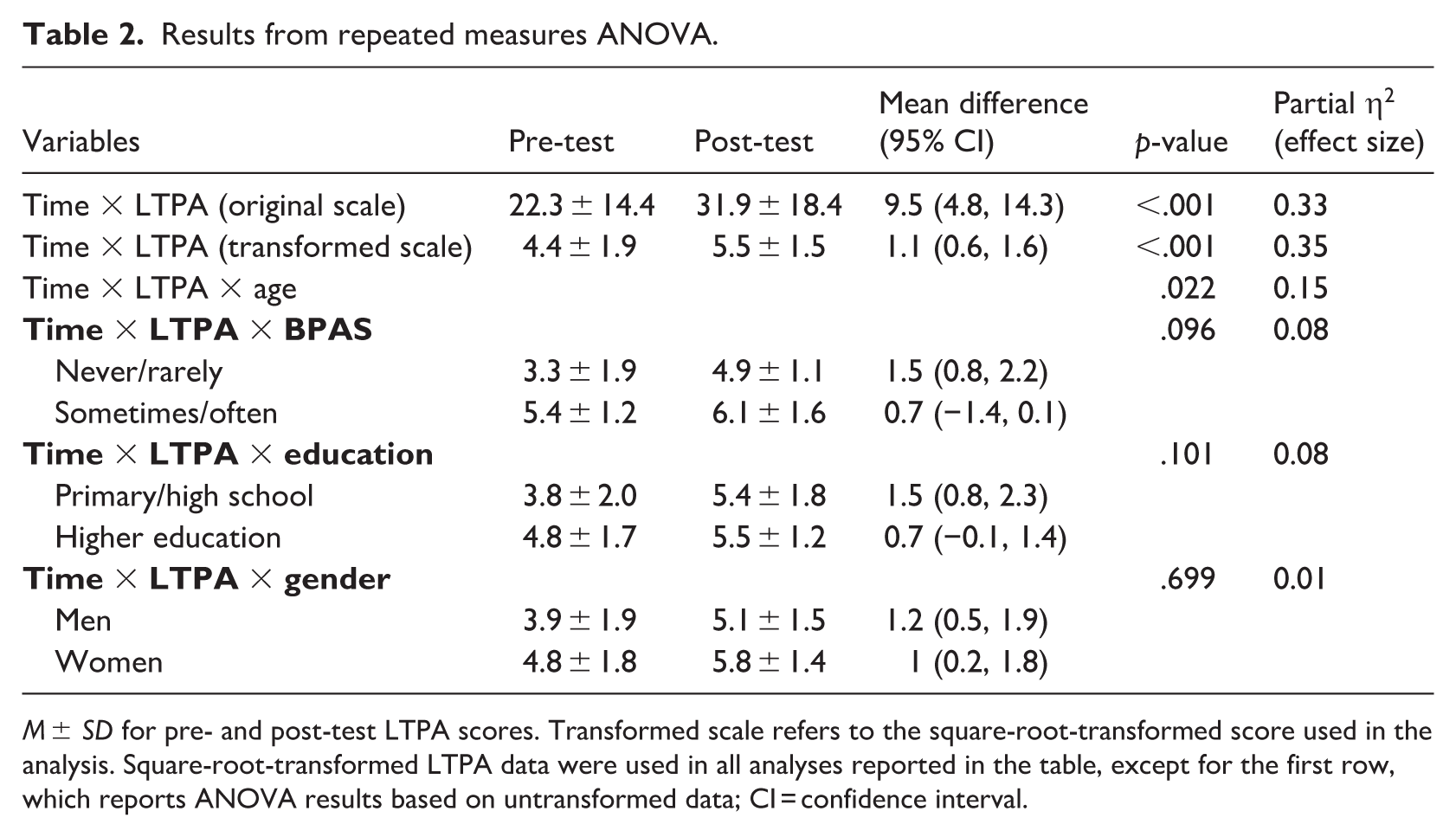
M ± SD for pre- and post-test LTPA scores. Transformed scale refers to the square-root-transformed score used in the analysis. Square-root-transformed LTPA data were used in all analyses reported in the table, except for the first row, which reports ANOVA results based on untransformed data; CI = confidence interval.
No significant time × BPAS interaction effect was observed, F(1, 33) = 2.93, p = .096, partial η2 = 0.08. No significant time × education interaction effect was observed, F(1, 33) = 2.85, p = .101, partial η2 = 0.08. No significant time × gender interaction effect was observed, F(1, 33) = 0.15, p = .699, partial η2 = 0.005. The intraclass correlation coefficient (ICC) indicated that 25% of the variance in the outcome was attributable to clustering at the company level. At the between-person level, 20% of the variance was explained, with the remaining 55% attributable to within-person variation over time.
The distribution of participants within the LTPA classification at pre-test was six active (17.1%), 13 moderately active (37.1%), and 16 insufficiently active (45.7%). In comparison, at post-test, the distribution was 16 active (45.7%), 12 moderately active (34.3%), and 7 insufficiently active (20%). The Marginal Homogeneity test indicated a significant shift in the distribution of LTPA classifications from pre- to post-test (MH = 47, p < .001), with a greater proportion of participants classified as moderately active or active at post-test.
No adverse events were reported during the intervention period.
Discussion
The results indicate that the group-based coaching intervention was well received by the sample and displayed efficacy in promoting LTPA. However, there was a significant time × age interaction effect, in which older age was associated with smaller increases in LTPA. In addition, significant changes in the distribution of LTPA classifications were identified, implying that moderate-to-strenuous LTPA increased the number of participants classified as active almost tripled, and insufficiently active decreased by more than half from pre- to post-test.
In addition to the relatively high mean score of perceived satisfaction with the intervention (20.1 out of 25), the attendance rates were also notable. Specifically, 88.6% of participants attended at least four out of the five sessions, which may indicate general satisfaction with the intervention. Potential explanations for the perceived satisfaction may include the group component and the inclusion of individual goal-setting and self-regulatory techniques, as these have been identified as preferred intervention characteristics among studies of office workers in recent research (Larisch et al., 2023; Olsen et al., 2018).
The office workers significantly increased their LTPA from pre- to post-test, which aligns with findings from earlier studies on the MoVo-work intervention (Krebs et al., 2015, 2019a). The present study identified a large effect size, while earlier findings demonstrated small-medium effect sizes (Krebs et al., 2015, 2019a). However, important considerations are the different study design (e.g. the absence of a control group in this study), study population, and the fact that the present intervention was a scaled-down version of the original MoVo-work intervention, as it did not include the practical exercise sessions.
Importantly, the current intervention targeted both intentional determinants (e.g. goal-setting of outcomes and the encouragement of autonomous, motivating, and realistic activities) and volitional determinants (i.e. action planning, problem-solving, and self-monitoring of behaviour). Evidence suggesting that successful behaviour change depends on both intention and volition (Fuchs, 2007; Schwarzer, 2008). Recent evidence also indicates a tendency towards the superiority of combining BCTs targeting motivation and self-regulation (i.e. volition), to promote PA among employees (Gawlik et al., 2023; Lock et al., 2021; Sun et al., 2022).
The notorious intention-behaviour gap identified in previous research shows that approximately 50% of individuals who intend to be physically active do not translate this intention into actual behaviour (Feil et al., 2023). It is possible that the current intervention helped bridge this gap through concrete action planning, as this may facilitate the enactment of a behaviour whenever the pre-identified situation is encountered. In addition, as the participants identified counter-strategies to address anticipated barriers, this may have also helped bridge the intention–behaviour gap. Furthermore, study participants were encouraged to self-monitor their LTPA, which may have strengthened participants’ behavioural control and self-awareness of their plans for LTPA. Previous research supports the use of self-regulation techniques to promote PA which have also been shown to reduce the intention-behaviour gap (Lock et al., 2021; Peng et al., 2022; Rhodes, 2024; Rhodes et al., 2021; Samdal et al., 2017).
The emphasis in this study on developing realistic action plans and collecting counter-strategies may have enhanced the participants’ self-efficacy—and their belief in their ability to engage in LTPA. This potential increase in self-efficacy could help explain the notable increases in LTPA observed in the t study, as self-efficacy is a significant predictor of PA (Rhodes et al., 2021). Further potential mechanisms contributing to the positive outcomes include the fact that participants were encouraged to plan social support for LTPA, with the group-based intervention being a source of social support. Social support and group-based interventions have respectively been associated with higher PA and have been shown to be impactful in promoting PA earlier research (Krebs et al., 2015; Madden et al., 2020; Rhodes et al., 2021; Samdal et al., 2017; Smith et al., 2023), and may be essential when it comes to promoting LTPA (Smith et al., 2017).
Exploratory moderation analyses suggested that higher age was associated with smaller increases in LTPA, although previous research on age as a moderator of PA interventions is inconclusive (Rhodes et al., 2019, 2021). No statistically significant moderation effects were observed for BPAS, education, or gender, suggesting that the intervention effects did not differ across these participant characteristics.
Strengths and limitations
Strengths of the present study are the fact that the intervention was theory-driven and delivered by the same instructor in a manner aligned with a standardised course instructor manual, enhancing intervention fidelity. Furthermore, a low dropout rate was observed, and a statistical power of 0.8 was achieved. The intervention was conducted across three municipalities and six workplaces. Participants were nested within their workplaces either on premises or working at a distance.
Major limitations of this study were the absence of a control group, which precludes causal inference, and thus the effect sizes observed in this study may be overestimates, as earlier research identified smaller effects on PA outcomes in RCT studies (To et al., 2013). Thus, it cannot be ruled out that the results of increased LTPA from pre- to post-test in this study may be attributed to factors other than the intervention. Convenience sampling method may have introduced selection bias, attracting health-conscious employees to a larger extent than another sampling method would have done. Furthermore, the majority of participants were already physically active to some degree at baseline (i.e. 37% were categorised as moderately active and 17% as active), indicating a potential ceiling effect.
In this study, LTPA was measured by self-report questionnaires, increasing the risk of social desirability effects. However, the instrument used had been validated (Godin and Shephard, 1985), and previous research suggests that measurement type does not moderate intervention effects on PA (Rhodes et al., 2021). In contrast, the questionnaire assessing intervention satisfaction was not validated and the results from it should be interpreted with caution. Furthermore, the outcomes of moderation analysis should also be interpreted cautiously, due to a small sample size and limited power. Given that long-term adherence is critical in PA interventions, the lack of longer follow-up limits the study’s utility, since short-term assessments may overestimate intervention effects. The limited fidelity of the study was a further weakness since the intervention was delivered in a different manner to that than originally planned (i.e. some participants participated digitally).
Conclusion
In conclusion, this brief coaching intervention was well received and acknowledged as effective in promoting LTPA. The percentage of participants classified as active increased from 17.1% to 45.7% between pre- and post-tests. LTPA also significantly increased from pre- to post-test, but higher age was associated with smaller increases. Findings concerning the moderation analyses should be interpreted with caution due to limited statistical power.
Due to study limitations (i.e. the absence of a control group, self-reported LTPA), causal relationships between intervention and changes in LTPA could not be determined. Randomised controlled studies with objective PA measures, as well as well-conducted field trials are warranted to examine the potential of this brief coaching intervention to promote office workers’ LTPA and to determine any potential moderating effects due to age, gender, location of training, and other factors.
Footnotes
Acknowledgements
The authors thank the contact persons at each company who supported recruitment to the study, as well as the participants who took part in the intervention and contributed valuable insights during the group sessions.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data are available upon reasonable request.
AI use
Assistive AI tools, Grammarly and ChatGPT were used for language editing and minor rephrasing, and the text generated with AI assistance was carefully reviewed by the author to ensure its validity. No generative AI was used to develop scientific content, and the authors take full responsibility for the accuracy, integrity and quality of the paper as published.