
Abstract
Background:
Racialised health professions students frequently experience overt and covert racism, which can erode confidence, provoke emotional distress, and hinder learning, academic performance, and wellness. Innovative, accessible resources to build critical thinking and equip learners with strategies to navigate racism are urgently needed. Virtual simulation offers a promising approach to build capacity to respond to racism in health professions education.
Objective:
The objective of this study was to evaluate feasibility and impact of a virtual simulation educational module on cultural humility and perceived competence to respond to racism.
Methods:
A quasi-experimental pretest-post-test multi-site design was implemented across six academic sites in Canada and the USA. Participants completed standardised prebriefing materials, three asynchronous virtual simulations, and a self or group debrief. Outcome measures included feasibility indicators, the Simulation Effectiveness Tool–Modified (SET-M), Foronda’s Cultural Humility Scale, and scenario-specific perceived competency rubrics.
Results:
Among 354 consenting participants, 139 completed both pre- and post-surveys. The module demonstrated strong feasibility and acceptability, with high ratings for prebriefing, simulation design, and debriefing (⩾96% agreement). Cultural humility scores increased significantly from pre- to post-intervention (p < .001), remaining within the “usually culturally humble” range. Perceived competence to respond to racism improved significantly across all scenarios (p < .001), with post-test scores approaching the “competent learner” category.
Conclusions:
This research improves understanding of the use of virtual simulations to prepare health professions students to address racism in classroom and clinical settings.
Keywords
Introduction
The racism experienced by racialised health professions students contributes to loss of confidence, feelings of sadness, and anger (Tilki et al., 2007). These experiences can affect students’ ability to learn, academic performance, and personal wellness. There is an urgent need for innovative, accessible resources to promote critical thinking to address overt and covert racism (Beavers et al., 2024; Cénat et al., 2024; Tilki et al., 2007). This need includes providing resources for racialised health professions students regarding how to navigate situations where racism occurs, and resources for non-racialised faculty and peers to recognise and support students experiencing racism.
Cultural humility is one approach that can be utilised to address racism (Foronda, 2020), which can be taught using interactive teaching approaches. For example, eLearning and simulations have successfully been used to provide education and encourage context-specific problem solving in healthcare when supporting groups deserving social justice (Killam et al., 2024; Luctkar-Flude et al., 2021b; Pittiglio and Lidtke, 2021). This project was developed to address gaps in the research literature related to health professions education on cultural humility and responding to racism using virtual simulation (Sawhney et al., 2025). We aimed to evaluate an eLearning module with virtual simulations about responding effectively to racism in health professions classrooms and clinical settings.
Background
Despite recent attention to equity, diversity, and inclusion in society and academia, racism remains prevalent on university campuses and in clinical settings, as reported by our own learners. Policies, curricula, admissions, grading, and faculty representation contribute to structural racism and inequities, and deeply embed racism in academic settings (Beagan et al., 2023; Cranston and Bennett, 2024). Racism can be explicit and intentional (overt) or indirect and understated (covert), and both have a significant impact on learners (Williams et al., 2022). All forms of racism can have harmful effects in academic settings, including heightened symptoms of distress, trauma, depression, and reduced belonging (Nepton et al., 2025a, 2025b). Covert racism, historically referred to as racial microaggressions, may be defined as the experience of “brief and commonplace daily verbal, behavioral, or environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative racial slights and insults toward people of color” (Sue et al., 2007: p. 1). Bystander intervention frameworks help learners move beyond silence by providing practical strategies to identify racism and intervene in ways that support the recipients of racism (Overland et al., 2019). By immersing learners in realistic scenarios, virtual simulation makes the experience of responding to racism more tangible and emotionally resonant, strengthening their confidence and competence in real-world encounters (Blodgett et al., 2022). Together, these approaches underscore the ongoing need for cultural humility and an ethic of lifelong learning, self-reflection, and accountability that equips learners to recognise their own biases and respond to racism in ways that promote equity and respect.
Cultural humility
Cultural humility is a process of openness, self-awareness, being egoless, and incorporating self-reflection and critique after interactions with diverse individuals which result in mutual empowerment, respect, partnerships, optimal care, and lifelong learning (Foronda et al., 2016). Providing health care professions students and faculty with a foundation in cultural humility can support the development of more inclusive learning and clinical environments that will enhance learning and patient care.
Virtual simulation
Virtual simulation is an interactive computer-based educational strategy in which learners are required to make decisions about an unfolding situation and see the results of their decisions (Cant et al., 2019; Jenson and Forsyth, 2012; Killam et al., 2024). Immediate feedback including the rationale for why responses are correct or incorrect may be provided, indicating the appropriateness, effectiveness, and accurateness of the chosen response. Virtual simulations offer the advantages of accessibility and repeatability and have been shown to increase student engagement and critical thinking abilities (Auman, 2011; Chiniara et al., 2013; Padilha et al., 2019). Research to support the use of virtual simulation to address racism in health professions education is however limited.
Study purpose
The purpose of the Responding to Racism study was to evaluate an online virtual simulation module for health professions students to address racism in the classroom and clinical settings. The specific objectives were:
To describe the feasibility, acceptability, and perceived effectiveness of the Responding to Racism virtual simulations.
To describe the impact of the Responding to Racism virtual simulations on learner outcomes: in relation to cultural humility and competence related to responding to racism.
Methods
The virtual simulation module was evaluated using a quasi-experimental pretest-post-test multi-site design. This study is reported in accordance with the Reporting Item Standards for Education (RISE2) guidelines for development and delivery of education interventions (Nisselle et al., 2021).
Setting and sample
We aimed to recruit a convenience sample of at least 20 participants per site across 6 universities and colleges in Western USA and Central and Eastern Canada, with diversity of size, geographic region, institutional mandate, and student population. Based on an anticipated moderate effect size (Cohen’s d = 0.49–0.5) consistent with prior simulation-based education research for knowledge and performance outcomes, a minimum sample size of 102 participants was required to achieve 80% power at a 5% significance level (two-sided) for between-group comparisons (Faul et al., 2007).
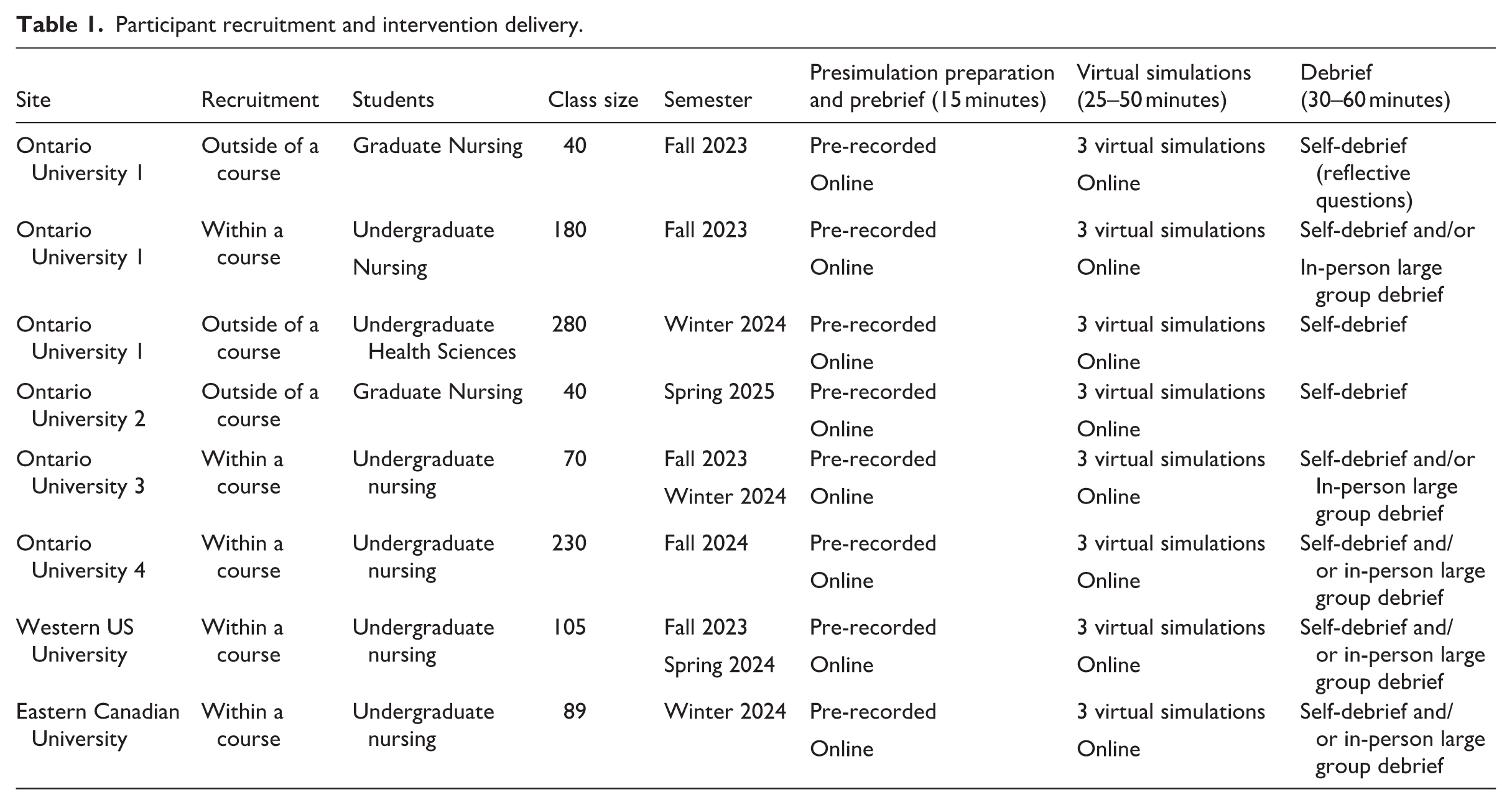
The range of institutional contexts represented in the study strengthened the ability to assess feasibility across varied educational environments. Although the virtual simulation targeted all health professions, the majority of recruitment sites were schools of nursing, thus, most participants were nursing students enrolled in undergraduate programmes (see Table 1). At half of the sites participants completed the virtual simulation module as a mandatory course component and were invited to participate in the research voluntarily. At the other three sites, learners had the option to complete the module independently outside of coursework. Participants were offered a $5.00 coffee shop gift card for completing each study survey.
Participant recruitment and intervention delivery.
Intervention: Responding to racism virtual simulations
A module on responding to racism in the classroom and clinical settings was developed using the Canadian Alliance of Nurse Educators using Simulation (CAN-Sim) virtual simulation design process (Tyerman et al., 2021). Learning outcomes focused on recognising overt and covert racism towards health professions students and applying models and strategies in response. The module features a series of three virtual simulations with embedded self-assessment as follows:
Differentiating overt and covert racism;
Allie’s Story: Bystander responding to racism in the classroom;
Clement’s Story: Health professional student responding to racism in the clinical setting.
Each virtual simulation consists of 5–10 decision points aligned with co-created learning outcomes, typically with 3 possible responses for each decision point, and the rationale for each response. Generally, one response is the best choice because it aligns with a given model for responding to racism; however, we emphasised that alternate responses are also appropriate depending on context, power relationships, and comfort when the individual experiencing racism feels psychologically unsafe to act.
The module was co-developed at Queen’s University in Kingston, Ontario, Canada by health professions faculty and students with lived experience and/or simulation design expertise. These contributors informed scenario priorities, reviewed scripts and decision points for authenticity, and provided feedback on the wording of responses options, rationales, and debriefing reflective questions (Luctkar-Flude et al., 2026). The virtual simulations were reviewed by equity, diversity, and inclusion experts prior to finalisation. A comprehensive description of the development process is reported elsewhere (Luctkar-Flude et al., 2026). Each virtual simulation underwent usability testing with a small group of faculty and learners to detect any technical or content issues prior to implementation and evaluation.
Intervention protocol
Participants completed online surveys before and after completing the eLearning module. All participants completed the same pre-simulation preparation, although delivery and debriefing methods varied (see Table 1).
Quantitative outcomes and instruments
Feasibility and Acceptability were measured by implementation, participation, and dropout rates.
Perceived Simulation effectiveness was measured by the Simulation Effectiveness Tool–Modified (SET-M) to evaluate learner perceptions of effectiveness of the simulation in meeting their learning needs (Leighton et al., 2015). The tool has been tested in nursing and medical education environments including virtual simulations. The validated 19-item survey has four subscales: prebriefing, learning, confidence, and debriefing and reliability ranges (Cronbach’s alpha varied from .833 to .908). Likert-type scores range from 1 (strongly disagree) to 3 (strongly agree); higher scores indicate greater perceived simulation effectiveness (Leighton et al., 2015).
Cultural humility was measured using Foronda’s Cultural Humility Scale, a 19-item scale (Foronda et al., 2021), based on Foronda’s theory of cultural humility (Foronda, 2020). The instrument demonstrated a high reliability (Cronbach’s alpha = .85) and a content validity index of 0.83 or higher on all items. Scores range from 1 (strongly disagree) to 5 (strongly agree); higher scores indicate greater cultural humility (Foronda et al., 2021).
Perceived competence in the ability to meet learning outcomes was assessed using the learning outcomes assessment rubrics accompanying the virtual simulations. Learning outcomes addressed cultural humility, response to racism, and interprofessional communication and teamwork. Similar assessment rubrics have demonstrated reliability and validity with higher scores indicating greater competence in meeting learning outcomes, and lower scores indicating developing or limited competence (Luctkar-Flude et al., 2020).
Data analysis
Descriptive statistics were calculated for feasibility and usability survey data. Paired t-tests were conducted to compare pre-test and post-test data within groups. Independent samples t-tests or one-way analysis of variance (ANOVA) were conducted to compare means between groups. Data were tested for normality prior to the use of parametric analysis. Participants with incomplete data for a specific scale/subscale were not included in that analysis.
Ethical considerations
Ethics approval for the study was received from the Queen’s University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board (TRAQ # 6039489), followed by individual institutional ethics board approvals from all collaborating sites. Informed consent was obtained from participants prior to data collection and only anonymous data were collected.
Results
The module was delivered to a total of 674 students within a taught course and offered to an additional 360 students outside of the classroom.
A total of 354 study participants were recruited to the study across 6 participating sites with 311 participants completing the pre-survey, 174 completing the post-survey, and 139 completing both. Thus, 34% of students offered the intervention consented to participate and completed at least one of the study surveys; however, only 54% of participants completing the pre-survey also completed the post-survey.
Data from all participants (n = 354) were included in descriptive analyses, whereas repeated-measures analysis was only conducted on subsets of participants with both pre- and post-survey data. For the SET-M analysis, all available post-test data (n = 174) were included rather than restricted to the paired datasets, to avoid excluding relevant outcomes not linked to pre-test responses. Over 98% of data within surveys were complete.
Participants’ characteristics are shown in Table 2. Most participants were nursing students (85.6%), self-identified as female/women (82.2%), reported a white racial identity (48%), and ranged in age from 17 to 59 years (mean = 23 years). Although most (50.3%) had never played a video game, the majority (54.2%) reported previously completing over three educational virtual simulations.
Participants’ characteristics.
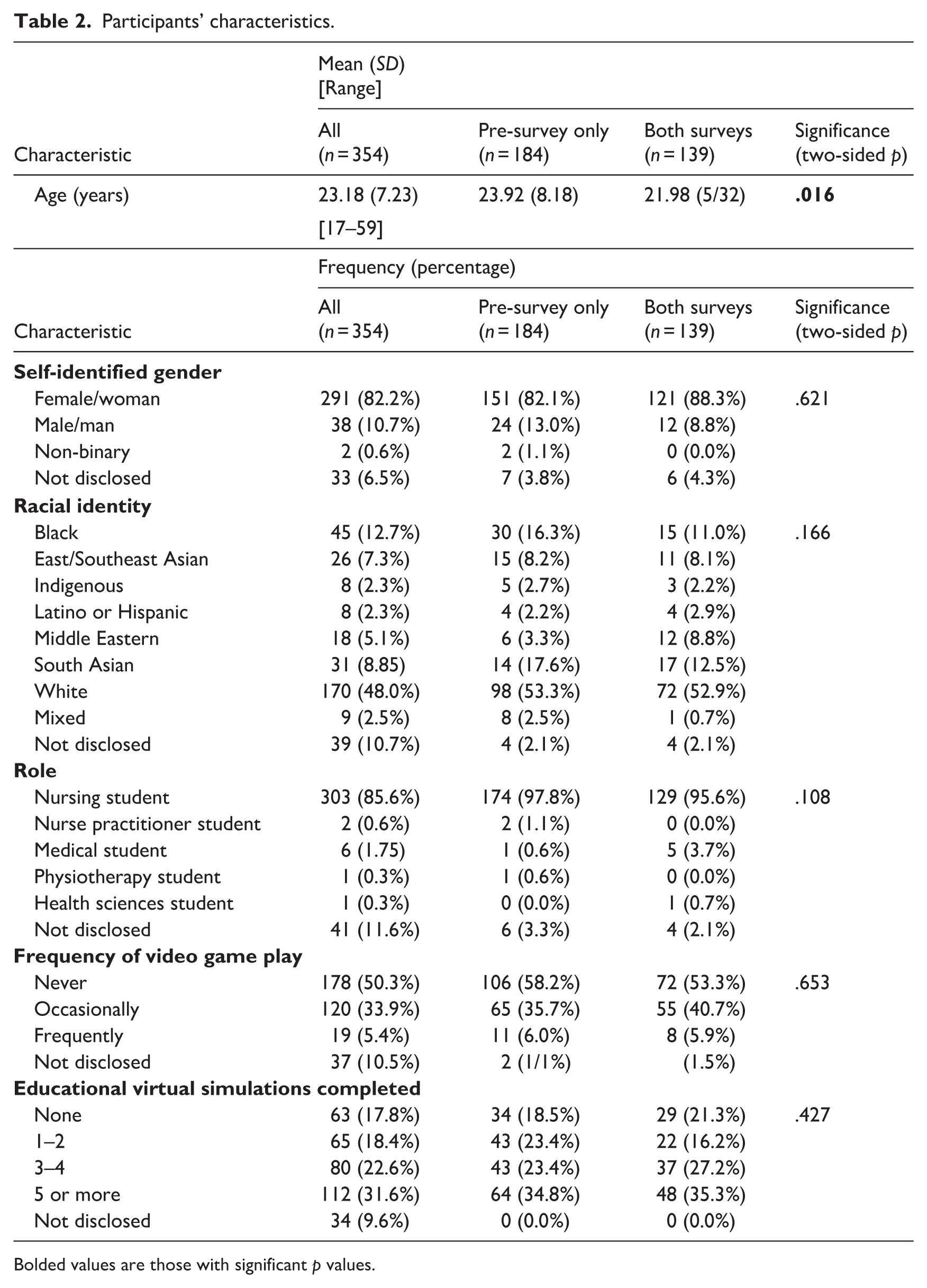
Bolded values are those with significant p values.
We conducted additional analyses to assess the risk of attrition bias by comparing baseline characteristics (e.g. demographic variables and pre-survey outcome scores) between participants who completed both surveys and those who completed only the pre-survey, which indicated that participant characteristics differed only for age, with no statistically significant differences for gender, racial identity, role, frequency of video game play, or number of educational virtual simulations completed. However, analyses revealed a statistically significant difference (p = .032) in baseline cultural humility scores between participants who completed both pre- and post-surveys (M = 74.78; SD = 11.19) and those who completed only the pre-survey (M = 77.37; SD = 9.52), with higher baseline scores observed among participants lost to follow-up.
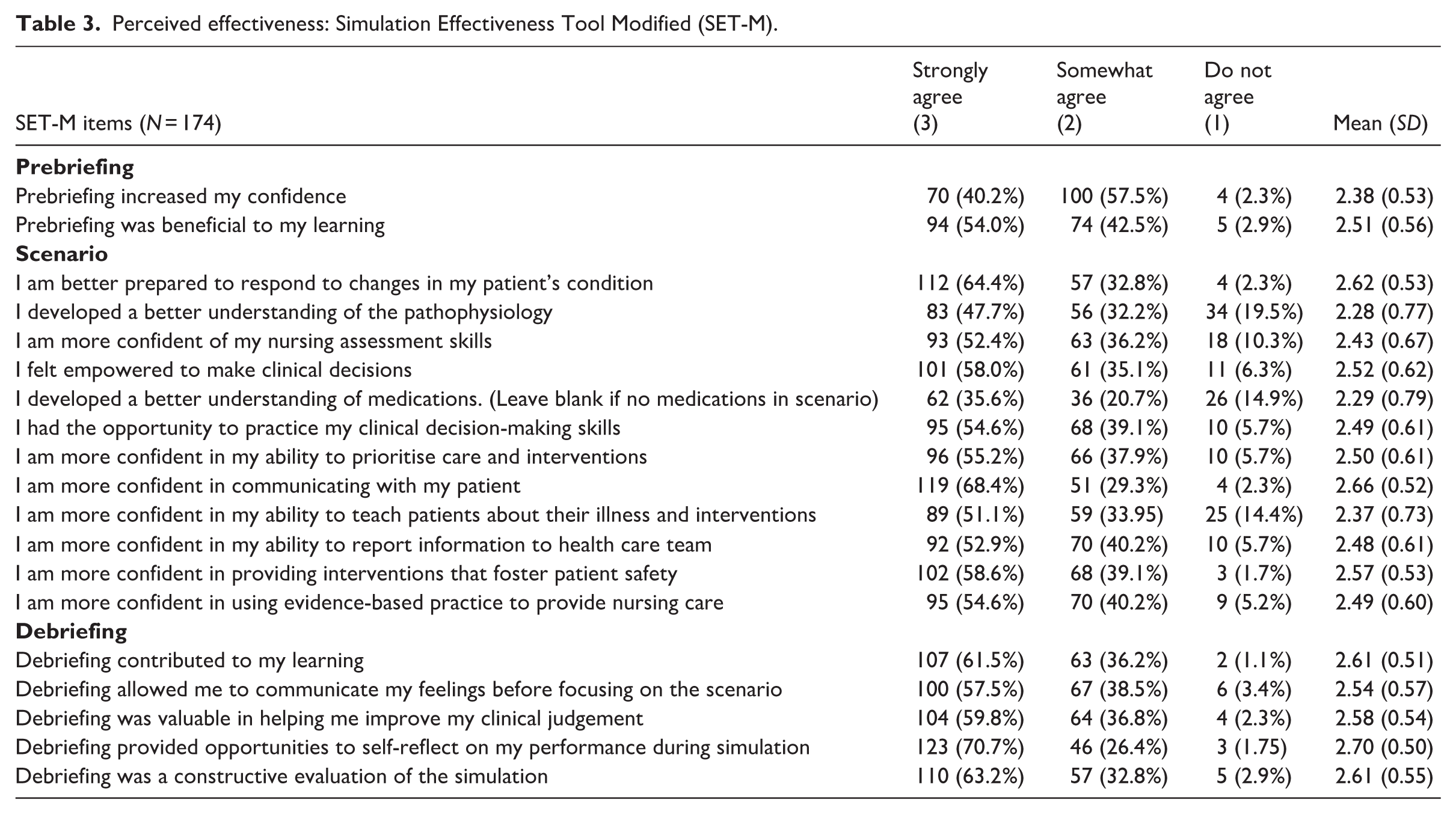
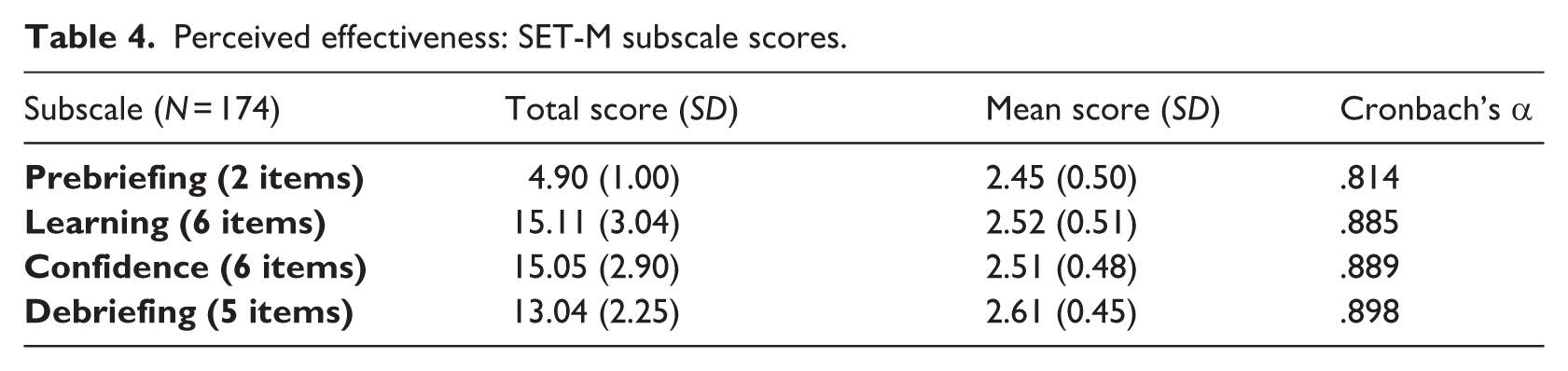
Participants’ SET-M ratings of perceived effectiveness of the virtual simulation components are shown in Table 3. Most participants somewhat agreed/strongly agreed the prebriefing was valuable (96.5%–97.7%), the scenario was valuable (80.5%–98.3%), and the debriefing was valuable (96.6%–98.9%). SET-M subscale scores (Table 4) were highest for debriefing (M = 2.61; SD = 0.45) and lowest for prebriefing (M = 2.45; SD = 0.50), with all four subscales demonstrating high internal consistency (Cronbach’s alpha .814–.898).
Perceived effectiveness: Simulation Effectiveness Tool Modified (SET-M).
Perceived effectiveness: SET-M subscale scores.
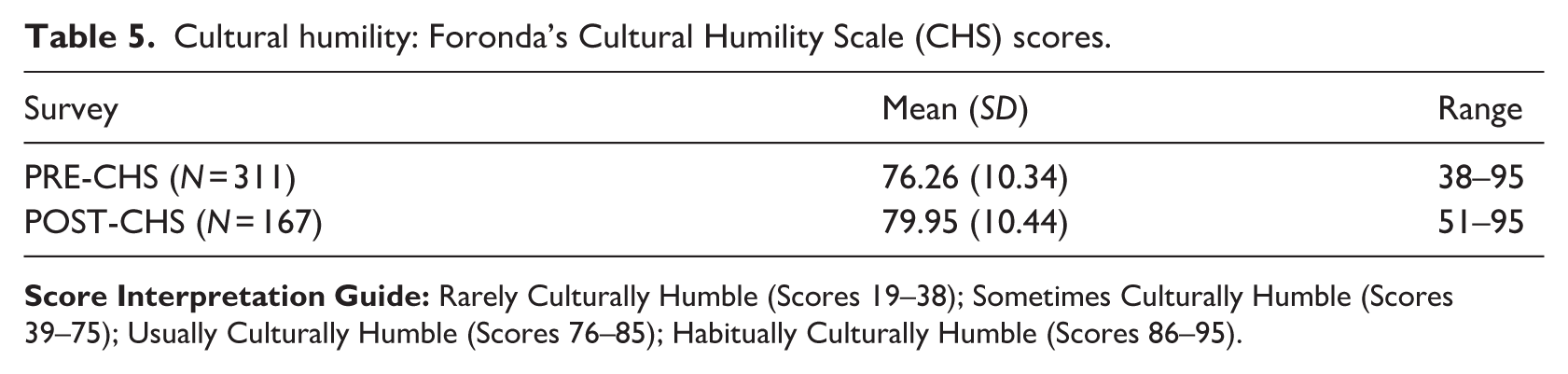
Cultural Humility Scale scores are presented in Table 5 for all study participants and Table 6 for participants who completed both the pre- and post-test surveys. Scores increased significantly from pre-test to post-test (p < .001); however, both sets of scores fell within the “usually culturally humble” range. Post hoc power analysis using the paired sample (N = 139) demonstrated the observed increase in cultural humility (Δ = 4.39) corresponded to a small-to-moderate effect size (Cohen’s d ≈ 0.41), with high statistical power (0.98–0.99, two-tailed α = .05).
Cultural humility: Foronda’s Cultural Humility Scale (CHS) scores.
Foronda’s CHS paired samples t-tests (N = 139).
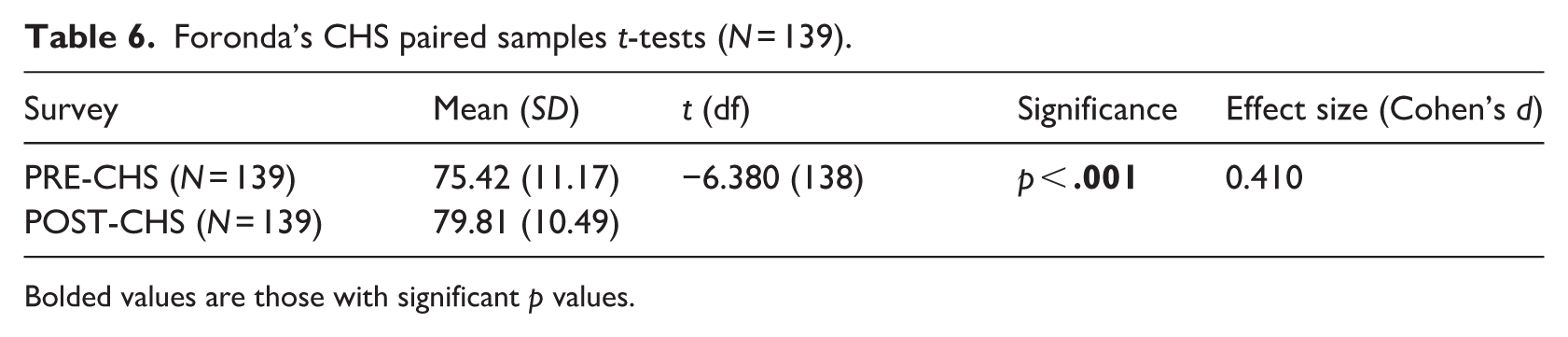
Bolded values are those with significant p values.
Although the Kolmogorov–Smirnov test conducted on the Cultural Humility Scale pre-test scores indicated a significant deviation from normality (p < .001), this test is highly sensitive in moderate to large sample sizes and may detect trivial deviations from normality (Ghasemi and Zahediasl, 2012). Examination of skewness (−0.686) and kurtosis (0.730) values suggested only mild deviation from normality. Therefore, the data were considered approximately normally distributed, and parametric analyses were deemed appropriate. In addition, visual inspection via a Q-Q plot confirmed that the data points fell along the diagonal line, justifying the use of a t-test. Similar results were obtained when testing for normality of the Cultural Humility post-test scores.
Perceived competence to respond to racism scores measured with the scenario-specific learning outcomes assessment rubrics are presented in Table 7. At pre-test, participants rated themselves significantly higher on the rubric for Clement’s story (a learner experiencing racism from a patient) than for Allie’s story (a learner witnessing racism towards another learner in a classroom) (p < .001). There were no significant differences between scenario rubric scores at post-test. Perceived competence scores increased significantly from pre-test to post-test for each scenario individually (p < .001) with all scores falling within the “intermediate learner” level of competence but approaching the “competent learner” level of competence at post-test. For Allie’s story, the increase in scores (Δ = 2.14) corresponded to a large effect size (Cohen’s d = 1.20), and for Clement’s story, the increase (Δ = 1.72) also reflected a large effect (Cohen’s d = 0.91). Post hoc power analyses indicated both analyses were highly powered (power > 0.99, two-tailed α = .05).
Perceived competence to respond to racism: Learning Outcomes Assessment Rubric scores.
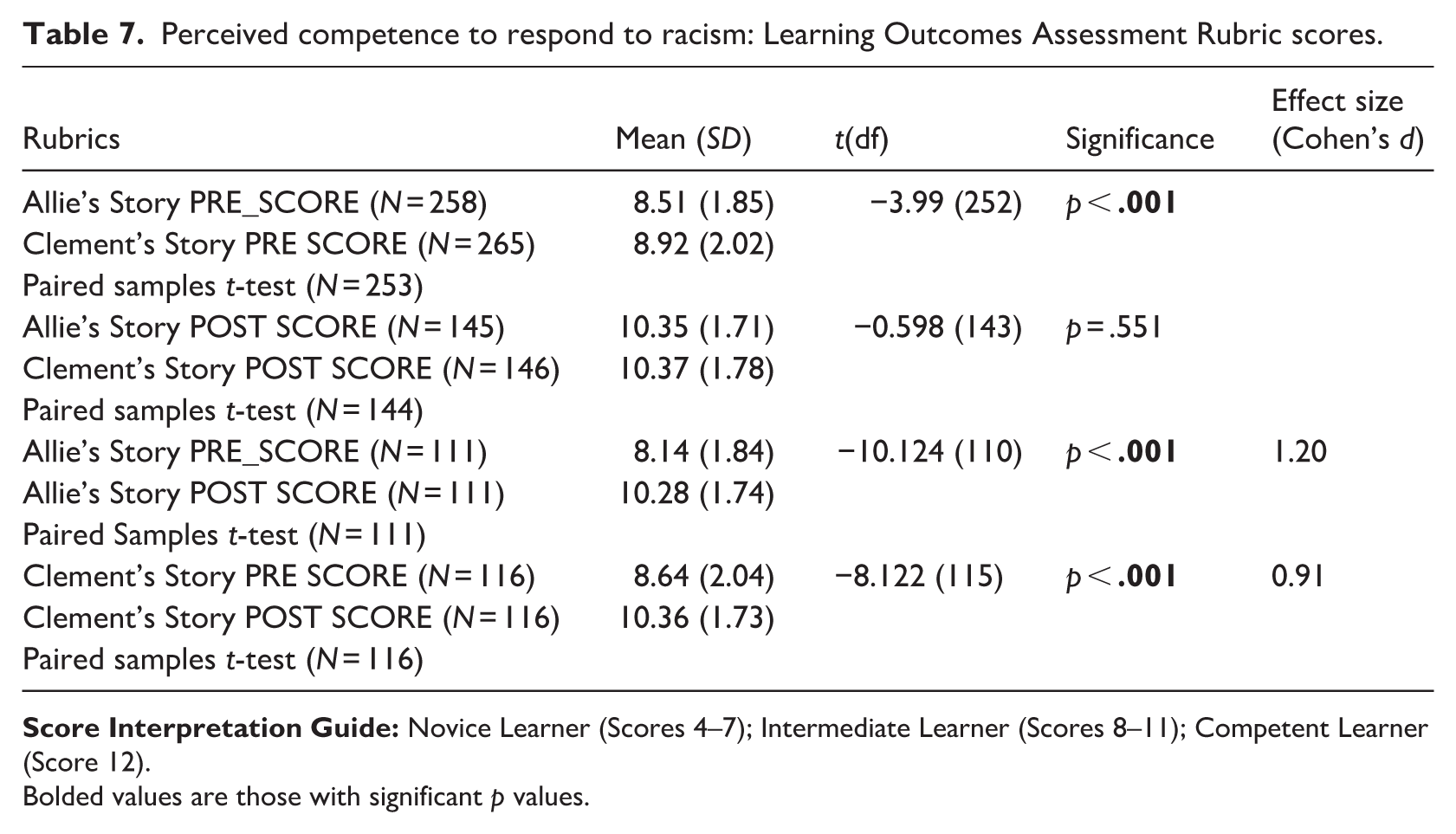
Bolded values are those with significant p values.
Although the Kolmogorov–Smirnov test conducted on the learning outcomes assessment rubric scores (perceived competence) indicated a significant deviation from normality (p < .001), skewness (range = −.091 to −.770) and kurtosis (−.249 to −.958) values fell within a range that is considered acceptable for approximate normality, which with an n = 139 supports the use of parametric tests (Ghasemi and Zahediasl, 2012). In addition, visual inspection via a Q-Q plot confirmed that the data points fell along the diagonal line, justifying the use of a t-test.
A one-way ANOVA was conducted to evaluate differences in post-test outcomes across three debriefing approaches (self-debrief only; self plus in-person group debrief; self plus synchronous virtual group debrief). There were no significant differences between debriefing groups for perceived simulation effectiveness as measured by the SET-M scores for prebriefing (p = .479), scenario (p = .914), and debriefing (p = .893), and no significant differences for cultural humility (p = .612), perceived competence for Allie’s story (p = .943), or perceived competence for Clement’s story (.780) between the three debriefing types.
Discussion
The purpose of the study was to evaluate the impact of the Responding to Racism online virtual simulation module on learners’ cultural humility, perceived competence to respond to racism, and perceived effectiveness. The study also assessed the feasibility and acceptability of the teaching tool. Evaluation of the module, conducted with mostly nursing students, elicited positive outcomes.
Study findings support the premise that simulation-based experiences offer a viable tool to address topics related to health equity (Vora et al., 2024). The novel virtual simulation module has potential to prepare health professions students to recognise and respond to racism directed at themselves, peers, and clients encountered in the classroom and clinical settings. The responding to racism module provides the learner with a framework, tools, and practice to address racism as a bystander and as a recipient for which there is limited evidence in the literature. The module encompasses a comprehensive virtual simulation design that implements principles of psychological safety during the prebrief and debriefing methods, active learning, and cultural humility.
Participants included a diverse sample, with more than half identifying as racialised. This was a multi-site, international study making results more generalisable to the larger target population. The Cultural Humility Scale, Perceived Effectiveness, and the Perceived Competence scales were reliable and validated measurement tools (Foronda et al., 2021; Leighton et al., 2015; Luctkar-Flude et al., 2020). The virtual simulation design used standardised prebrief and debriefing guidelines and followed Healthcare Simulation Standards of Best Practice (HSSOBP®) (Watts et al., 2021). The intervention provided educators flexibility and adaptability to implement within existing curricula with multiple debriefing modalities, allowing for tailored approaches to unique needs of diverse educational programmes and settings.
Successful implementation of the Responding to Racism virtual simulation module across diverse academic sites in Canada and the USA, as a complement to existing curricula or as a voluntary learning opportunity, demonstrates its feasibility. In all six settings, the module was delivered without major technical issues. Recruitment, data collection, and standard protocol delivery were similar across sites. Participation of over 350 learners demonstrated strong feasibility; however, attrition in survey completion highlights logistical challenges in maintaining participant engagement in research over time, especially with online surveys. Planned variation in debriefing formats, including in-person or online synchronous options, supported feasibility of delivery within different academic contexts.
Most learners completed the three-part module and associated prebrief, indicating sustained engagement with the content. High ratings of satisfaction across prebriefing, simulation, and debriefing suggest participants found the virtual simulations engaging and relevant to their learning. Participant feedback on the prebriefing process was overwhelmingly positive, with over 96% agreeing it was valuable in preparing them for the simulation experience. In addition, the diversity of learners and settings in which the simulation was implemented suggests broad relevance and resonance of the content.
Participants reported high levels of perceived impact across key domains of the simulation experience, as measured by the SET-M which is commonly used to identify items or subscales with consistently low ratings as these highlight areas where learner needs were not being met and prioritise these for improvement in future simulations. Participants agreed the virtual simulations enhanced their learning, confidence, and preparedness to address racism in the classroom and clinical settings. Ratings were strong in the prebriefing and learning subscales, affirming the simulation’s educational value. The virtual simulation module was developed in accordance with the HSSOBP® (INACSL Standards Committee et al., 2021). These best practices were intentionally incorporated into the module delivery to optimise learner engagement and outcomes.
Cultural Humility Scale scores increased significantly with a small to moderate effect size. In the paired sample, pre-test scores were near the upper boundary of the “sometimes culturally humble” range, whereas post-test scores approached the middle of the “usually culturally humble range,” supporting the potential for virtual simulation as an educational tool for fostering self-awareness and reflective practice related to racism and bias. The results are similar to those in previous studies that used virtual simulation to promote cultural humility in learners. In Tschannen et al.’s (2025) study, four 360-degree video virtual simulations were used to improve nursing students’ cultural humility, empathy, and reduction of implicit bias. The 360-degree videos were 3- to 6-minute scenarios of cases focused on social determinants of health and followed the HSSOBP®. One key finding was participants identifying the importance of cultural humility in reducing implicit biases in nursing care (Tschannen et al., 2025). A mixed-methods study by Luctkar-Flude et al. (2021b) evaluated a virtual simulation game module to teach cultural awareness and inclusivity for the LGBTQI2S community in nursing students; quantitative and qualitative results were positive for improving cultural humility and personal bias.
The significant improvements in perceived competence for Allie’s and Clement’s stories with large effect size suggest the simulations successfully enhanced learners’ confidence and preparedness to respond to racist incidents. The finding that participants initially rated themselves more competent responding to patient-initiated racism than peer racism may reflect differing perceived power dynamics and psychological safety levels in classroom versus clinical settings. Convergence of competence scores between the two scenarios indicates learners gained a more consistent framework for identifying and addressing racism across contexts. However, both pre and post mean scores fell within the category of intermediate learners. This is not unexpected within the short intervention time frame, suggesting that while learners gained insight and awareness, stronger feelings of competence may require repeated practice opportunities.
The results align with previous research evaluating simulation as a strategy to teach healthcare professionals how to respond to bias from clients. Carter and McMillian-Bohler (2021) created and evaluated a workshop to enhance learners’ ability to recognise and respond to microaggressions including racism. Durosier et al. (2024) developed and evaluated a 2-hour virtual course that included simulated patient scenarios to educate providers on how to respond to bias. Both studies reported positive outcomes including increased self-confidence to address patient bias.
Despite planned variability in debrief delivery, learner outcomes were consistent across modalities. This may reflect the standardised nature of the virtual simulation experience and the use of structured debriefing prompts aligned with the same learning objectives across sites. Thus, the virtual simulation intervention can be reasonably interpreted as a cohesive educational approach, with flexibility in debrief modality that did not appear to meaningfully influence outcomes. These findings align with results of a systematic review in which all debriefing methods for virtual simulations demonstrated some benefits in terms of learner outcomes (Luctkar-Flude et al., 2021a).
Limitations
A number of limitations should be considered when interpreting the findings of this study. First, there was substantial attrition between pre- and post-survey completion, with only 139 of 311 participants (44.7%) completing both surveys. This level of attrition introduces a risk of attrition bias, as participants who completed both surveys may differ systematically from those who did not. Specifically, non-completers were older and reported higher baseline cultural humility scores, suggesting that attrition was not random and may reflect differences in engagement or perceived relevance of the intervention. As a result, the analytic sample may overrepresent individuals with greater potential for improvement, potentially inflating estimates of intervention effectiveness. Although statistically significant, the magnitude of this difference was small, suggesting limited practical impact; however, its potential influence on estimates of change over time is acknowledged. In addition, repeated-measures analyses were conducted using complete-case data, which may bias estimates if data are not missing at random. Thus, findings related to changes over time should be interpreted with caution; however, small to large effect sizes to learner outcomes were noted despite attrition. The observed attrition may be attributable to factors such as survey fatigue, competing academic demands, and limited follow-up reminders, consistent with prior research involving student survey participation (Porter and Whitcomb, 2005; Saleh and Bista, 2017).
Second, the use of self-report measures introduces the potential for response bias. Given the module’s focus on racism and equity and its integration as a mandatory course component at most sites, participants may have been motivated to respond in socially desirable ways, potentially inflating perceived improvements in outcomes. Third, the planned variability in debriefing approaches and facilitators across sites may have introduced inconsistency in the learning experience; however, analyses indicted no significant differences in outcomes by debriefing method. Fourth, the intervention’s reliance on access to an online learning module may have influenced participation. In addition, the sample was predominantly composed of nursing students (85%) and individuals identifying as female/women (82%), which, while reflective of the nursing profession, may limit generalisability to other health professions student populations. Finally, the quasi-experimental pretest–post-test design without a control group limits causal inference, as observed changes may reflect maturation, testing effects, concurrent learning experiences, or attrition bias rather than the intervention alone (Bierer et al., 2025).
Conclusion
Findings from this multi-site evaluation demonstrate that the Responding to Racism virtual simulation module offers a feasible and scalable approach to integrating anti-racism pedagogy into health professions education. Grounded in cultural humility and psychological safety, it equipped learners with practical skills to recognise and respond to racism across academic and clinical contexts. Its asynchronous, online design enhances accessibility and allows flexible integration across traditional, hybrid, and online curricula, supporting the development of core equity, diversity, and inclusion competencies (Pacquiao et al., 2025). Health professions programme leaders and educators may consider adopting this module as a standardised component of anti-racism education, while policymakers can leverage these findings to support institutional mandates and resource scalable simulation-based learning. Future research should examine long-term learning outcomes and expand to interprofessional populations to inform best practices and policy aimed at reducing health inequities.
Footnotes
Acknowledgements
We acknowledge the study participants and participating sites for their support for this research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this project was funded by a Queen’s University Reznick Scholar Award in Health Professions Education and a Canadian Alliance of Nurse Educators using Simulation (CAN-Sim) Research and Innovation Grant.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Marian Luctkar-Flude and Jane Tyerman are co-presidents of the Canadian Alliance of Nurse Educators using Simulation (CAN-Sim), a non-profit organisation that supports nursing simulation education and research, and instructors in the Canadian Association of Schools of Nursing (CASN) Canadian Simulation Nurse Educator programme. Laura Killam undertakes freelance work for CAN-Sim.
Data availability statement
Data to support the findings of this study may be made available by the corresponding author upon reasonable request.
AI use
The authors declare that no assistive or generative artificial intelligence tools were used in the manuscript’s production.