
Abstract
In December 2025, the Australian Health Practitioner Regulation Agency introduced a new Code of Conduct for registered psychologists, replacing the Australian Psychological Society’s long-standing Code of Ethics. While regulatory reform is routine, this transition represents a significant shift in how ethical obligations are articulated, governed, and enforced, with implications for how psychologists are trained and supported to work ethically with LGBTQ+ clients. This paper examines how previous ethical guidance framed LGBTQ+ health and well-being, identifying conceptual omissions, dated assumptions, and uneven coverage across LGBTQ+ subpopulations. Drawing on this analysis, we consider how the new Code of Conduct might address – or risk reproducing – existing practice gaps, with a focus on competence, confidence, and accountability when working with marginalised subgroups. We discuss the implications for education, supervision, and continuing professional development, highlighting the need for explicit, contemporary, and inclusive ethical guidance to support culturally safe and affirming care.
Introduction
Australian health practitioners are regulated by national boards relevant to their specialism, as well as the Australian Health Practitioners Regulation Agency (AHPRA). The AHPRA is responsible for implementing national registration and accreditation schemes across regulated health professions. Regulatory agencies such as AHPRA (2025) play a central role in assuring the public that health professionals are suitably trained, qualified and safe to practice, including psychologists. In December 2025, AHPRA introduced a new Code of Conduct (CoC) for registered psychologists (AHPRA, 2025). This CoC now supersedes the earlier Australian Psychological Society’s (APS, 2007) Code of Ethics (CoE) as the primary regulatory framework for psychological practice in Australia (Psychology Board of Australia, 2024).
While updates to codes are important, necessary, and expected, this shift from the APS CoE to the AHPRA CoC represents a substantive shift in how ethical obligations are articulated and operationalised in practice. It also has specific implications for psychologists’ work with LGBTQ+ clients, particularly where guidance is ambiguous or uneven across subpopulations. This paper aims to critically appraise past APS ethical guidelines to identify how LGBTQ+ 1 health needs were framed, what was omitted, and how these gaps may persist in the new CoC.
Codes and guidelines
The APS CoE was introduced in 2007, with two relevant sets of Ethical Guidelines developed for Australian psychologists when working with lesbian, gay, bisexual, trans, queer or otherwise sexually or gender-diverse (LGBTQ+) clients. These are the Ethical Guidelines for Working with Lesbian, Gay and Bisexual clients – revised February 2010 (APS, 2014a), and the Ethical guidelines on working with Sex and/or Gender Diverse Clients – May 2013 (APS, 2014b). In 2025, AHPRA (2025) introduced a profession-wide CoC outlining expected standards and behaviours for registered psychologists. AHPRA (2025) has stated that the APS CoE was originally adopted as a suitable governance document but that this arrangement no longer holds.
While the APS’ CoE is no longer the guiding document for Australian psychologists, some of the APS’ Ethical Guidelines are referenced by AHPRA’s CoC in lieu of creating new guidelines for certain populations. One such case is related to LGBTQ+ clients where Australian psychologists will continue to be guided by the aforementioned ethical guidelines without any substantial changes being added to the CoC (AHPRA, 2025). Noting this adoption, the relevance of these guidelines – and whether they meet the needs of contemporary LGBTQ+ Australians – warrants review. Since the CoE documents were developed, significant legal and social changes have occurred, including many that caused varying levels of distress for LGBTQ+ people such as marriage equality and a rise in anti-trans discourse. These developments have had substantial impacts on LGBTQ+ people and have affected the mental well-being of trans and gender-diverse people more than most (Saxby et al., 2025). As shown in Table 1, while the AHPRA CoC introduces a more unified and enforceable framework, it largely retains a reliance on legacy APS guidelines, meaning that many identifiable limitations – particularly in relation to specificity, intersectionality, and trans-affirming care – remain unaddressed.
Comparison of APS ethical guidelines and AHPRA Code of Conduct in relation to LGBTQ+ practice.
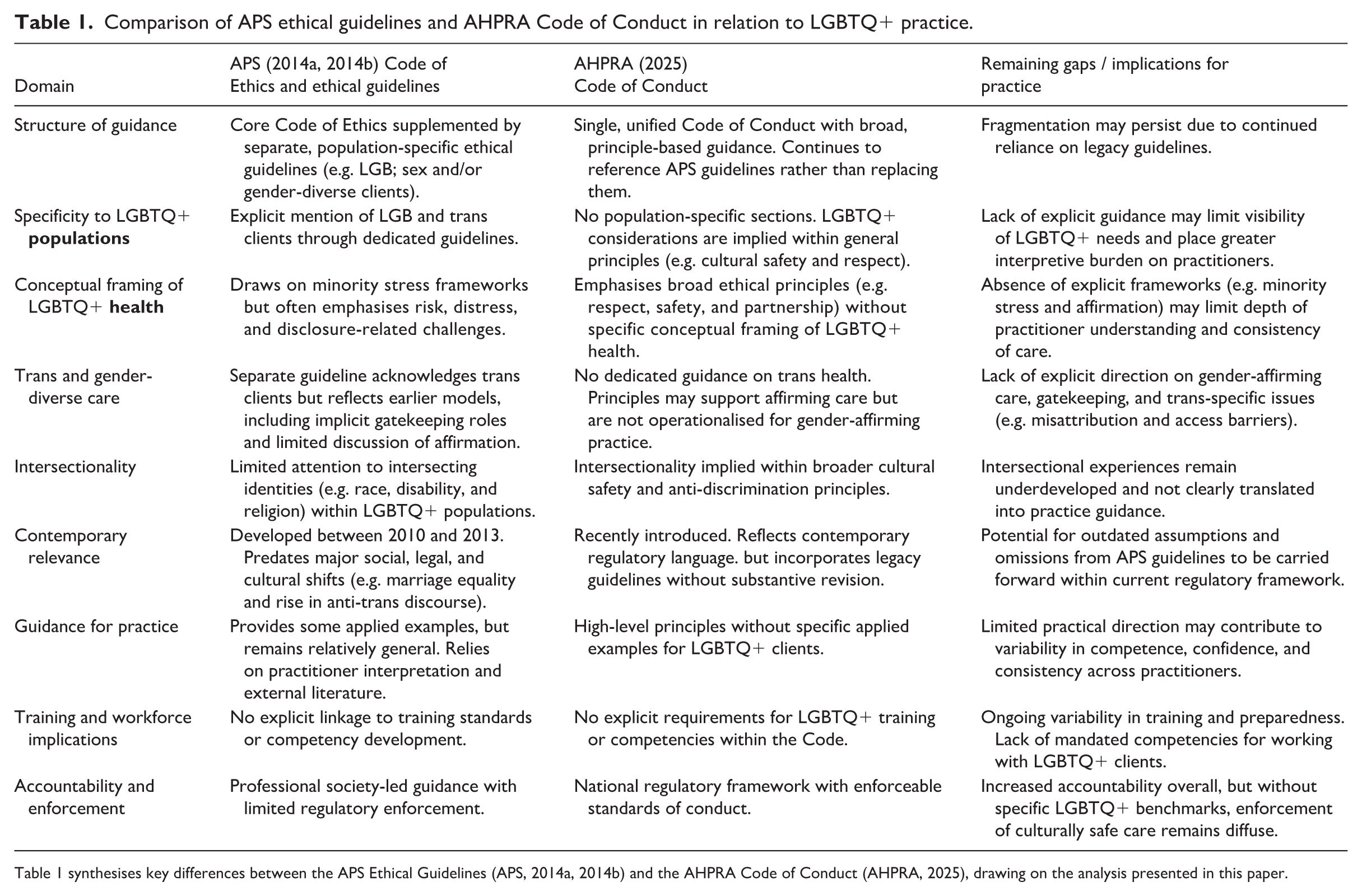
Table 1 synthesises key differences between the APS Ethical Guidelines (APS, 2014a, 2014b) and the AHPRA Code of Conduct (AHPRA, 2025), drawing on the analysis presented in this paper.
Although guidelines and codes are not intended to be explicitly practical, their specificity can shape practitioner confidence and consistency. This paper reviews the APS’ ethical guidelines and offers practical ways in which these can be utilised by psychologists working with LGBTQ+ people in Australia. While these APS guidelines may now be considered defunct, a workforce of psychologists was trained under them and there was little interrogation of the suitability of these guidelines for work with LGBTQ+ people during this period. Interrogating these guidelines for an up-and-coming workforce gives an opportunity to validate their effectiveness anew and to question how they can be adapted for work with contemporary LGBTQ+ individuals and communities. This is of particular importance given that the AHPRA CoC does not offer explicit guidance on supporting LGBTQ+ mental health and well-being, highlighting the deficits present in preparing a workforce for working with a diverse population.
Lesbian, gay, and bisexual clients
The APS Ethical Guidelines for Working with Lesbian, Gay and Bisexual Clients were approved by the APS board in 2010 and has since been used as a guiding document for any Australian psychologist who has, or intends to have, cisgender lesbian, gay and/or bisexual (LGB) clients within their practice (APS, 2014a). The guidelines were grounded in the outgoing APS (2014a, 2014b) CoE standards of Justice, Respect and Competence, and provide some guidance for psychologists to best engage with LGB clients. For the LGB Ethical Guidelines there is an attempt to identify some areas of distress that lesbian, gay and bisexual clients may present to psychologists. For instance, LGB clients may identify stressors associated with LGB well-being such as coming out, family of origin rejection, and workplace discrimination and career progression which have been well established in previous research (DeChants et al., 2022; Donaghy and Perales, 2022; Gray et al., 2016; Morgan et al., 2025; Osmetti and Allen, 2023). Consistent with minority stress frameworks, these difficulties are best understood as responses to stigma rather than anything inherent to LGB identities (APS, 2014a), and longitudinal and intervention evidence indicates that targeted support can reduce distress and improve well-being, which psychologists should consider when working with LGB clients (Nguyen et al., 2023). However, no other issues beyond rejection and career trajectory were articulated specifically within the Ethical Guidelines. This may lead psychologists to assume that LGB clients only seek support for issues of this kind and to not expand into other topics such as starting their own families, envisioning a positive future, or even general everyday stressors that may affect anyone regardless of their sexuality or gender.
Australian psychologists can of course support their own learning in these areas by consulting the available literature. However, a persistent limitation within this literature is a deficit framing that over-emphasises harm and under-specifies strengths and coping (Peel et al., 2022), which can create inadvertent knowledge barriers for psychologists and how they engage with and respond to LGBTQ+ clients (Cruciani et al., 2024). Strengths-based and affirmative approaches are associated with better client experiences and stronger therapeutic relationships (Lytle et al., 2014; Westcott et al., 2022), and can help shift practice away from ‘risk-only’ framings.
A key limitation of the APS’ guidelines is that they do not account for intersectional experiences within LGB communities. LGB clients may present with needs related to their intersecting forms of disadvantage, including sexual racism (Thai et al., 2025), racism in healthcare (Uink et al., 2024), ableism (Cull et al., 2025), ageism (Waling et al., 2021), being LGB and transgender or gender-diverse, and faith-based conflict (Mercieca and Anderson, 2025). These dynamics can compound barriers to care and well-being, including through microaggressions and structural disadvantage (Moagi et al., 2021). Minority stress models help explain how discrimination and internalised stigma can undermine well-being (Hendricks and Testa, 2012; Hunter et al., 2021; Lefevor et al., 2019) but psychologists should avoid homogenising LGBTQ+ mental health or relying on a singular deficit narrative (Hoy-Ellis, 2021). Instead, practice should combine an affirmative stance with attention to clients’ intersecting identities, resources, and protective factors to best support clients across the multitude of identities that each of them possess and not focus on singular LGBTQ+ identities while neglecting how experiences of minoritisation cannot be easily separated from one another (Pachankis et al., 2023). Some examples of intersectional practice are supporting LGB clients of colour, LGB First Nations clients, LGB clients with disabilities, and LGB clients who are also trans or gender-diverse.
While there is no singular approach to support LGB clients experiencing intersecting forms of oppression, adopting intersectional and affirmative approaches is worth considering (Astramovich and Scott, 2020; Dunlop and Lea, 2022). Affirmative practice involves integrating knowledge of the developmental and cultural contexts of LGBQ clients into ethically responsive care (Alessi et al., 2019). Adopting such an approach can also assist psychologists to consider protective factors – such as social support, community connection, and positive self-concept – that may buffer distress (Ibarra-Alexanderson, 2023; Wallace et al., 2024). Importantly, caring for LGB clients is not a niche speciality, but part of providing patient-centred, high-quality psychological care across practice settings (Pachankis et al., 2023).
Transgender and gender-diverse clients
The APS Ethical Guidelines on Working with Sex and/or Gender Diverse Clients (APS, 2014b) provide the primary legacy guidance relevant to psychologists’ engagement with transgender and gender-diverse and nonbinary clients (hereafter, trans people). This section examines how that guidance aligns with contemporary models of gender-affirming care and identifies key gaps with implications for ethical practice under the new AHPRA CoC.
In supporting trans clients to understand their gender identity, psychologists can focus on gender-affirming care and recognise that experiences of questioning and affirming one’s gender are personal, unique, and a normal part of human experiences that are not inherently pathological (Coleman et al., 2022). Affirmation likely differs for each trans person, whether by choice or by limitation of accessible services (costs, geography, rights, parental supports, or all the above as examples). Affirmation can be social, legal, medical, a combination of these, or something else entirely. What is known is that gender-affirming care of all types alleviates distress and incongruence in trans people (Bhatt et al., 2022; Di Luigi et al., 2025; Kennis et al., 2022; Puckett et al., 2026). Importantly, affirmation is not inherently oriented towards ‘passing’ or conformity to cisnormative expectations, but may instead prioritise comfort, authenticity, safety, or self-definition (Anderson et al., 2025).
The Australian Professional Association for Trans Health (AusPATH, 2025), the national peak body supporting the health and well-being of all trans people, notes that psychologists can play an active role in supporting trans people in accessing gender-affirming care. However, psychologists and other mental health professionals can be viewed as gatekeeping care through their role in assessing trans people to access gender-affirming surgery (AusPATH, 2022). Many trans people report microaggressions during therapy, including during gender-affirming care pathways (Morris et al., 2020). Psychologists should therefore develop confidence (and competence) in providing affirming support and advocacy where appropriate, including when clients present with co-occurring mental health concerns which may or may not relate to their gender identity or affirmation (ACON, 2025; AusPATH, 2022).
Trans clients may also encounter ‘trans broken arm syndrome’, whereby health concerns are misattributed to their trans identity or to their (medical) gender-affirming care (Wall et al., 2023). This can lead to unaddressed pain, medical violence, distrust, and harm for trans clients who need to defend their identity to seek equitable and adequate care (Shane, 2023). Furthermore, incompetence that stems from this ‘syndrome’ can result in delays to accessing gender-affirming care (Anderson et al., 2025). Trans youth, in particular, report having to navigate multiple primary care providers before finding one who is capable of providing adequate support, often settling for a less knowledgeable practitioner simply to ascertain referrals to psychological pathways and gender-affirming services (Strauss et al., 2021). Some trans adults report seeking specialists over generalist providers as they view that as the only way their health needs will be addressed, despite this process resulting in longer wait times and higher costs (Zwickl et al., 2019).
Issues of stigma and transphobia are also present outside of medical and mental health spaces. While not all trans people experience transphobia in the same way, the pervasiveness of transphobia in society is high in Australia, with one in two trans people saying they had experienced transphobia online and in person within the last 12 months (Trans Justice Project and Victorian Pride Lobby, 2023). Although transphobia may be more expected outside of LGBTQ+ communities, it can also manifest from within them. This intragroup hostility can be more distressing for trans clients, especially when coming from romantic and/or sexual partners (Lombardi, 2024). It is important that psychologists consider the impact of stigma and transphobia, and be open to the multiple and complex ways this can affect their client over their lifetime. In particular, current guidelines offer limited direction on responding to the transphobia that occurs in online environments and within LGBTQ+ communities and intimate relationships, despite evidence that these forms of intragroup and relational hostility can be especially distressing.
Finally, supporting trans clients does not need to be treated as a specialist knowledge area for psychologists. While, historically, trans research has been problematic due to issues of pathologisation and consistent research gaps (Zwickl et al., 2019), there are pathways psychologists can take to support their clinical relationship with their trans clients. These can include supporting a client’s gender affirmation through social affirmation processes (e.g. name changes, using affirming pronouns) and providing a safer space for clients to talk through their gender journey (Orygen, 2021). Furthermore, avoiding singular narratives of resilience, which would require visibility and self-advocacy by the client themselves, can also assist trans clients. This removes an assumed role that trans clients must play in order to be considered valid enough to receive quality mental health care (Moreno Tucker and Degges-White, 2025). Psychologists may also wish to consider gaining membership to AusPATH, to learn from peers and access resources that can help guide their work with trans clients.
Practical applications for health education
The new CoC, underpinned by the APS Ethical Guidelines on Working with Sex and/or Gender Diverse Clients and Ethical Guidelines for Working with Lesbian, Gay and Bisexual Clients, are not the only documents that inform competent practice with LGBTQ+ clients. However, variability in how LGBTQ+ content is taught and reinforced across training pathways means psychologists may enter practice with differing levels of preparedness. This section offers practical applications for already accredited Australian psychologists, all psychologists regardless of where they have been trained, and health educators working with people who wish to become accredited psychologists, all of whom wish to work competently with LGBTQ+ clients.
Australian psychologists
For currently registered Australian psychologists – who were trained prior to recent regulatory reforms – it is important to identify ways to support their ongoing learning about LGBTQ+ people’s needs. This is mainly due to inconsistencies in LGBTQ+ content being taught across different Australian institutions, noting that LGBTQ+ people have not been a named priority population in guiding documents such as the Australian Psychology Accreditation Council’s (APAC, 2019, 2025) Accreditations Standards which health educators will use when designing curriculum for psychology students.
Typically, training is available through Royal Colleges, Societies, and other expert bodies and academic groups (Trans Health Research, 2025). While some forms of training qualify for continued professional development (CPD), others may not. For non-CPD training psychologists, programmes such as Rainbow Health Australia can provide upskilling for individuals and accreditation for health organisations (Rainbow Health Australia, 2024). However, for CPD training, opportunities are more likely limited to recorded materials online and may be limited in what topics are offered (APS, 2024).
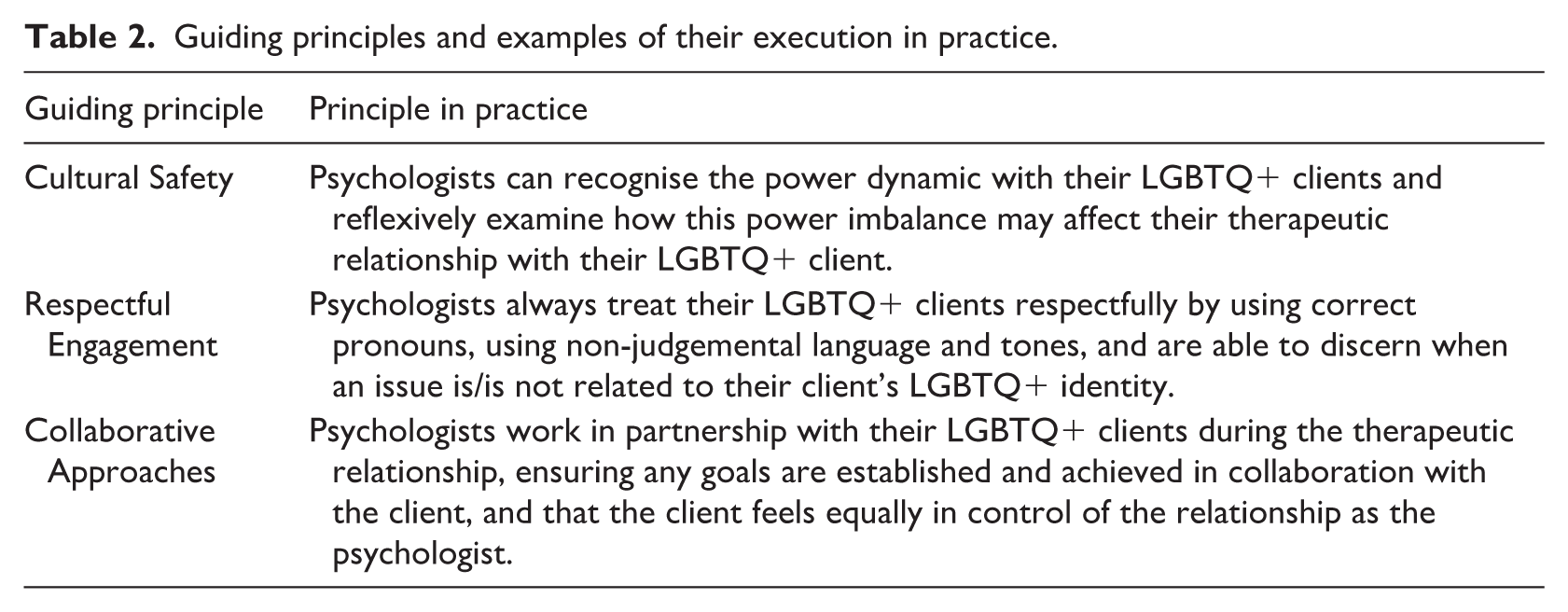
For practising Australian psychologists, the AHPRA CoC, Principles 1–4 offer guidance on how to practise cultural safety, respectful engagement, and collaborative approaches with clients. Although these are not specifically dedicated to LGBTQ+ clients, the codes provide a guiding framework to complement practice (AHPRA, 2025). These principles can be operationalised through concrete, affirming behaviours in work with LGBTQ+ clients. Examples of how to apply these principles are in Table 2.
Guiding principles and examples of their execution in practice.
All psychologists
Beyond the Australian context, where accredited training may be unavailable or inaccessible, psychologists may build LGBTQ+ competence through engagement with contemporary evidence. While evidence bases are not explicitly offered within the APS Ethical Guidelines of the AHPRA CoC, psychologists should feel empowered to consider where their own knowledge gaps may be, and what areas of LGBTQ+ experiences they need to deepen. Australian psychologists can build their competence of LGBTQ+ people by engaging with LGBTQ+ led peer-reviewed writing, as well as engaging in open forums and webinars offered by LGBTQ+ controlled health organisations and advocacy organisations. Training is associated with increased clinician confidence and improved client perceptions (Boekeloo et al., 2023; Mizock and Lundquist, 2016). Competent practice requires ongoing development and attention to intersecting identities beyond individual-level factors alone (Wing Sue, 2001). Cultural humility – characterised by lifelong learning, reflexivity, and attention to power – has also been associated with more positive LGBTQ+ client experiences (Dulyk and Young, 2025; Schmidt et al., 2024). Importantly, affirming practice appears more salient than identity salience alone in shaping clients’ perceptions of competence (Dulyk and Young, 2025).
To complement components of the AHPRA CoC such as cultural competence and humility, psychologists may consider using a reflexivity journal to ensure their thoughts are captured (Fischer et al., 2025). Prompts can be utilised to help support the process, as can speaking these through with a professional supervisor. Examples of possible prompts include the following:
Do I feel uncertainty or reluctance about taking on an LGBTQ+ client, and what may be driving this (e.g. competence concerns, values conflict, and countertransference)?
What assumptions do I hold about gender, sexuality, relationships, or life trajectories, and how might these shape my practice?
When do I refer LGBTQ+ clients on, and is this clinically indicated or driven by perceived lack of competence or discomfort?
How can I increase my proximity to LGBTQ+ knowledge and communities (e.g. training, supervision focus, and contemporary media)?
Do my language and attitudes towards LGBTQ+ people shift across contexts or audiences?
What belief about LGBTQ+ people have I revised recently, and what prompted that change?
Health educators
In Australia, university-level psychology curricula are guided by the Australian Psychological Accreditation Council (APAC), the independent accreditation authority responsible for ensuring the graduates of accredited programmes receive high-quality education and are equipped for professional practice (APAC, 2025). The APAC Accreditation Standards for Psychology Programmes was updated in December 2025 to coincide with AHPRA’s CoC and are used here to illustrate curriculum implications.
APAC’s 2025 iteration of their Accreditation Standards currently does not require LGBTQ+ content to be part of core competencies or training in any Australian undergraduate, honours, postgraduate, or standalone areas of practice (APAC, 2025). While sex, gender, and sexual orientation were noted in the 2019 version of the Accreditation Standards, these are not visible in the 2025 version (APAC, 2019, 2025). As a result, universities may include LGBTQ+ content inconsistently, and thresholds for competence remain unclear. International evidence suggests that LGBTQ+ health training is often minimal unless explicitly mandated and is most effective when introduced early and reinforced over time (Boroughs et al., 2015; Nowaskie et al., 2020).
For health educators, ambitious opportunities exist to support pre-practice psychologists by embedding LGBTQ+ experiences across curricula, even if these additions do not align explicitly with the APS Ethical Guidelines, AHPRA CoC and APAC graduate outcomes. While LGBTQ+ content may not be explicitly mandated in the APAC graduate outcomes, health educators should not feel that they are prevented from including LGBTQ+ content across all areas of psychology training. This inclusion can be achieved by mapping required competencies against ethical guidance and integrating LGBTQ+ content into foundational units. While being evidence-based, educators may also consider creative, intersectional, and strength-based approaches within workshops and assessments to prepare graduates for culturally humble practice. Furthermore, should LGBTQ+ content remain confined to elective units and not be embedded throughout curricula, it risks reinforcing the perception that LGBTQ+ clients constitute a specialist cohort rather than a routine part of psychological practice.
Limitations
More work is needed across undergraduate, honours, Masters, DPhil, and PhD psychology programmes to meaningfully integrate positive approaches to LGBTQ+ experiences into education and training, both within and beyond Australia. Governing bodies such as APAC should consider making LGBTQ+ peoples’ needs and care a priority in future iterations of their accreditation guidelines ensuring that all psychology students establish a base level of understanding LGBTQ+ clients before they begin supervised practice. Beyond this, new ethical guidelines that are contemporary and evidence-based should be developed to sit under AHPRA’s CoC, and should be updated routinely as evolving needs for LGBTQ+ people arise.
Pre-practice psychologists deserve early and sustained exposure to LGBTQ+ knowledge to build competence before entering supervised or independent work. It is the responsibility of accrediting bodies to lead on this so an informed and competent workforce of psychologists await any LGBTQ+ client, regardless of location or identity. Truly, it is an ethical choice to do so. To not do so would be antithetical to the ethics which psychology as a discipline and profession is bound by. LGBTQ+ people and communities are normal expressions of human diversity and deserve equitable, affirming and safe psychological care.
Conclusion
This paper has considered how the APS Ethical Guidelines can be applied for contemporary psychologists who work with LGBTQ+ clients. While multiple gaps exist in the guidelines, the paper has offered a starting point for psychologists to consider when working with or considering working with LGBTQ+ clients.
LGBTQ+ experiences and people are not a niche or specialist area of knowledge reserved to a select few psychologists, nor to LGBTQ+ psychologists themselves. Health educators have opportunities to create engaging ways to incorporate LGBTQ+ experiences into curriculum in meaningful and practical measures. This opportunity can also provide ways for pre-practising psychologists, as well as any student interested in tertiary level psychology, to consider how cultural competence and humility can be practised within their early learning. Psychologists deserve to graduate feeling confident, affirmed and competent to provide patient-centred care to LGBTQ+ clients they may see when entering their practice. The paper has also offered practising psychologists opportunities to ensure they are informed of the psychological needs of LGBTQ+ people as well as the ways they, as practising psychologists, can better connect and work with LGBTQ+ clients.
While this paper has offered a significant evidence base for psychologists and health educators alike to call on, it is limited in how deep the content can be considered. Evidence moves quickly, and community needs even quicker. Many more papers and guidelines can be developed beyond this paper. Considering the ever-changing landscape of LGBTQ+ health, and changes in LGBTQ+ rights the world over, so they should.
Ethical standards will also continue to change, whether they sit within bodies such as the APS or if they sit within regulatory agencies such as AHPRA and the national boards. Future recommendations for such bodies are to be explicit in their inclusion of LGBTQ+ clients, including how training bodies can help prepare psychologists for working with LGBTQ+ prior to entering practice. Clearer links can also be formed between how psychologists apply codes and guidelines, and how they relate to LGBTQ+ clients to ensure culturally safe and high-quality care is achieved. Finally, LGBTQ+ people should be treated with as much competence as any other client when accessing psychological care – including children and adolescents – in line with the ongoing codes of ethics, justice, and dignity, unwaveringly and steadfastly.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jacob Thomas was supported by an Australian Government Research Training Programme (RTP) Scholarship. Joel Anderson was supported by the Australian Research Council (DE230101636).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
There are no data associated with the publication of this article.
AI use
No assistive or generative AI was used throughout the development of this paper