
Abstract
Introduction:
Asexuality and aromanticism describe forms of sexual and relational diversity in which individuals experience little or no sexual or romantic attraction, encompassing a wide range of identities across the asexual and aromantic (ace/aro) spectrums. Despite being legitimate and well-established forms of sexual and relational diversity, asexual and aromantic identities remain largely absent from mental and physical healthcare education. This absence contributes to practitioner unawareness, clinical inaccuracies, and the pathologisation of non-normative experiences, reinforced by allonormative and amatonormative assumptions that frame sexual and romantic attraction as universal and necessary for well-being.
Summary of evidence:
Drawing on the existing qualitative literature, this paper offers a critical synthesis of asexual and aromantic people’s healthcare experiences. It identifies key sites of erasure and misunderstanding within clinical encounters, examines how normative assumptions about sex and romance shape care provision, and outlines the consequences of exclusion for patient trust, disclosure, and well-being. The paper then considers the implications of these findings for healthcare education and professional training.
Implications:
The systematic integration of asexual and aromantic perspectives into healthcare curricula is essential for ethical, patient-centred practice. To support translation into practice, the paper synthesises the reviewed evidence into applied educational guidance and illustrative scenarios relevant to clinical training and professional development.
Conclusion:
By outlining actionable priorities for education, training, and professional development, this paper contributes to efforts to advance equity, inclusion, and recognition of diverse sexual and relational experiences within healthcare practice.
Introduction
This paper examines asexuality and aromanticism as forms of sexual and relational diversity that remain largely absent from health professional education and training. While both identities are complex and encompass diverse experiences, for simplicity, this paper adopts broad definitions commonly used within the literature. Broadly, asexuality is commonly defined in relation to a partial or complete lack of sexual attraction (Bogaert, 2006), whereas aromanticism is commonly defined in relation to a partial or complete lack of romantic attraction (Aromantic Spectrum Union for Recognition, Education, and Advocacy [AUREA], 2021). While these two identities may co-occur within the same individual (i.e. ace-aro identity), they are generally understood as being conceptually distinct. This distinction is reflected within the “ace” and “aro” communities – for example, in a recent Australian survey of 1642 participants with asexual, aromantic, or ace-aro identities, 90.3% of participants reported that asexuality and aromanticism should be considered distinct (Fowler et al., 2024).
These two identities describe relationship-relevant patterns of attraction that challenge dominant assumptions about sexuality and intimacy in healthcare contexts. These patterns are often discussed in relation to allosexuality (i.e. the experience of sexual attraction) and alloromanticism (i.e. the experience of romantic attraction) – terms used to describe more socially normative experiences of attraction (Clark et al., 2023; Clark and Zimmerman, 2022; Piwek, 2024). Despite their legitimacy and diversity, asexual and aromantic identities are rarely addressed in healthcare curricula, limiting practitioners’ capacity to provide inclusive, competent, patient-centred care (Schneckenburger et al., 2024). Asexuality and aromanticism are umbrella terms encompassing multiple orientations across the asexuality spectrum and aromanticism spectrum, ranging from no sexual or romantic attraction to non-normative experiences of sex and relationships. Examples of identities across these spectra are shown in Table 1 (Asexual Visibility and Education Network [AVEN], 2021; AUREA, 2022; Bejda, 2023).
A (non-exhaustive) list of identities associated with asexuality and aromanticism.
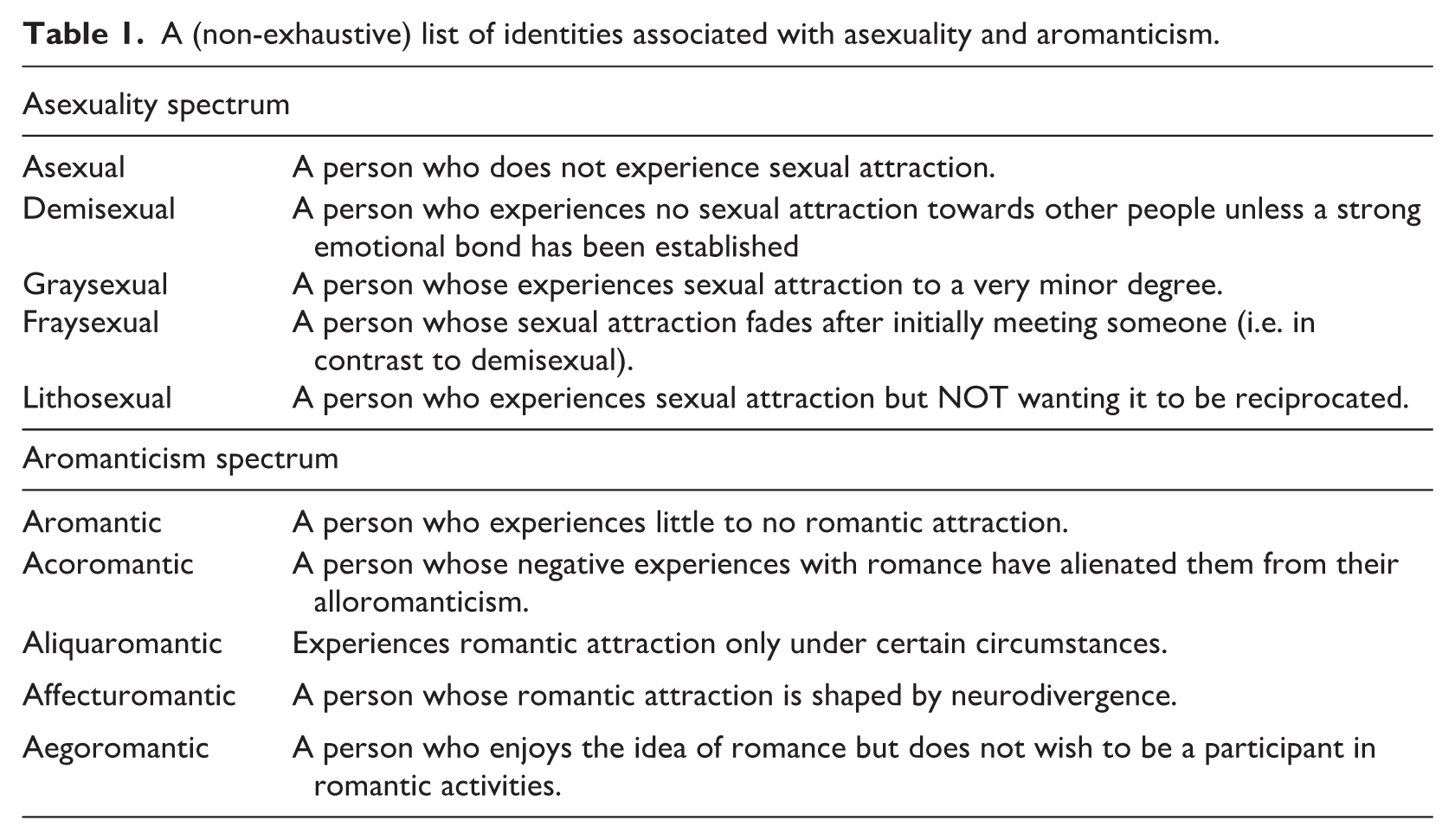
Asexuality is frequently conflated with hypoactive sexual desire disorder (HSDD), particularly in clinical and diagnostic settings where low or absent sexual desire may be pathologised, despite important conceptual and clinical distinctions between the two. Most notably, distress and impairment are central diagnostic features of HSDD but are not inherent to asexuality (Bogaert, 2006; Parish and Hahn, 2016). Failure to adequately distinguish these experiences within healthcare education and practice risks pathologising non-distressed asexual identities.
Research exploring asexual and aromantic individuals’ experiences with healthcare providers suggests that this conflation remains common in clinical encounters. Participants have described frustration when healthcare professionals assume dysfunction without attending to the individual’s own experience or stated lack of distress (Meera, 2025; Pavanello Decaro et al., 2025). These findings highlight the importance of explicitly addressing distinctions between asexuality and clinical diagnoses within health professional education and diagnostic frameworks, including the central role of distress in ethical and appropriate care.
Taken together, this evidence suggests the need to examine how normative assumptions about sex, romance, and distress shape asexual and aromantic people’s healthcare experiences and what this means for health professional education. Accordingly, the aims of this paper are threefold: first, to synthesise existing qualitative evidence on the healthcare experiences of asexual and aromantic people; second, to identify how normative assumptions about sex and romance are embedded in clinical practice; and third, to identify implications for healthcare education and professional training aimed at improving the quality and inclusivity of care for asexual and aromantic patients.
Understanding asexuality and aromanticism
Asexuality and aromanticism are frequently misunderstood within both lay and clinical contexts. Asexuality is not synonymous with celibacy, sexual abstinence, sexual dysfunction, or lack of libido, nor does it necessarily imply distress, trauma, hormonal imbalance, or disinterest in intimacy. Many asexual individuals experience emotional closeness, desire for relationships, physical affection, or romantic attraction, and some engage in sexual activity for a variety of personal, relational, or contextual reasons. What distinguishes asexuality is the experience of little or no sexual attraction, rather than the presence or absence of sexual behaviour or desire (AVEN, 2021). Similarly, aromanticism is often misinterpreted as fear of intimacy, emotional detachment, or an inability to form meaningful relationships. However, aromantic individuals may form deep emotional bonds, long-term partnerships, or committed non-romantic relationships, including queerplatonic relationships. Importantly, aromanticism refers specifically to patterns of romantic attraction, not to relationship capacity, emotional well-being, or relational competence (AUREA, 2022).
The above distinctions are salient in healthcare contexts, where sexual and romantic attraction are often assumed to be universal and developmentally necessary for well-being. When such assumptions go unexamined, asexuality and aromanticism may be misclassified as symptoms of pathology or targets for intervention rather than recognised as valid forms of sexual and relational diversity.
Although emerging research has begun to document mental health disparities among asexual individuals relative to their allosexual counterparts, comparable evidence for aromantic populations is strikingly limited, with important implications for healthcare education and practice. Existing research shows that individuals who identify as asexual tend to experience higher levels of depressive symptoms, psychological distress and loneliness, and report lower levels of general health and psychological well-being compared to their allosexual counterparts (Lech et al., 2024; Maadal et al., 2025). In addition, research has compared romantic asexual individuals (who experience romantic but not sexual attraction) and aromantic asexual individuals (who neither experience romantic nor sexual attraction, respectively) on a series of sexuality and bonding factors (Carvalho and Rodrigues, 2022). It finds that aromantic asexual individuals to have higher odds of avoidant attachment style and higher concern over relationship commitment. In contrast, research has yet to compare aromantic and alloromantic individuals on social or psychological factors including their mental health.
Two concepts relevant to understanding asexual and aromantic experiences are amatonormativity and allonormativity. Amatonormativity refers to the cultural assumption that everyone seeks, values, and should prioritise a central romantic relationship, and treats romantic partnership as a normal and expected part of adult life (Brake, 2012). Allonormativity similarly refers to the assumption that all people experience sexual attractions, and that these experiences are universal, natural, and desirable (Mollet and Lackman, 2021).
These normative assumptions contribute to distinct forms of stigma and minority stress for asexual and aromantic people, including invalidation, pathologisation, and exclusion. However, the impacts of amatonormativity may extend beyond ace and aro communities. For example, individuals who are single, unmarried, childfree, non-partnered, or who prioritise other aspects of life over romantic relationships may also encounter social and healthcare assumptions that position romantic partnership as expected or necessary. In healthcare settings, such assumptions may shape discussions about relationships, fertility, family planning, and well-being, reinforcing the importance of addressing amatonormative biases within health education and practice.
Together, these normative assumptions contribute to the multiple and intersecting forms of stigma experienced by asexual and aromantic individuals, in addition to identity-related stigma shaped by social, religious, and political beliefs (Iraklis, 2024). Asexual and aromantic people may encounter prejudice, including invalidation, ignorance, and misunderstanding from outside and within sexual and gender minority groups (Dillon et al., 2025; Fowler et al., 2024). These intersecting forms of marginalisation may have important implications for healthcare access and navigation, particularly given the role of connection to sexual and gender minority communities in facilitating affirming care and support.
A small body of empirical evidence exists which underscores the mental health implications of the aforementioned stressors. In an international study of 12,449 asexual individuals, nearly two-thirds of participants (64.8%) reported experiences of minority stress, and almost one-third (32.2%) reported suicidal ideation (Chan and Leung, 2023). Minority stress was significantly associated with impairments in daily functioning, social relationships, and physical health, with health impairment showing a particularly strong association with suicidality. These population-level patterns provide important context for understanding how stigma and minority stress may be reproduced or challenged within healthcare settings.
What asexual and aromantic lives and relationships can look like
Despite growing scholarly recognition of asexuality and aromanticism, these identities continue to be misunderstood in healthcare contexts, often through assumptions that frame them as deficits in sexuality, intimacy, or relational capacity. Such misunderstandings obscure the diversity of asexual and aromantic lives and may be reproduced in healthcare education and training, contributing to clinical assumptions that undermine patient-centred care. Clarifying how asexual and aromantic identities are lived and experienced across relational, sexual, and social contexts is therefore essential for healthcare education. To support this clarification, Table 2 presents a set of illustrative (hypothetical) examples designed as a teaching tool for health education contexts, offering illustrative scenarios that can support reflective discussion, case-based learning, and examination of normative clinical assumptions in training settings.
Examples of asexual and aromantic experiences relevant to healthcare education.
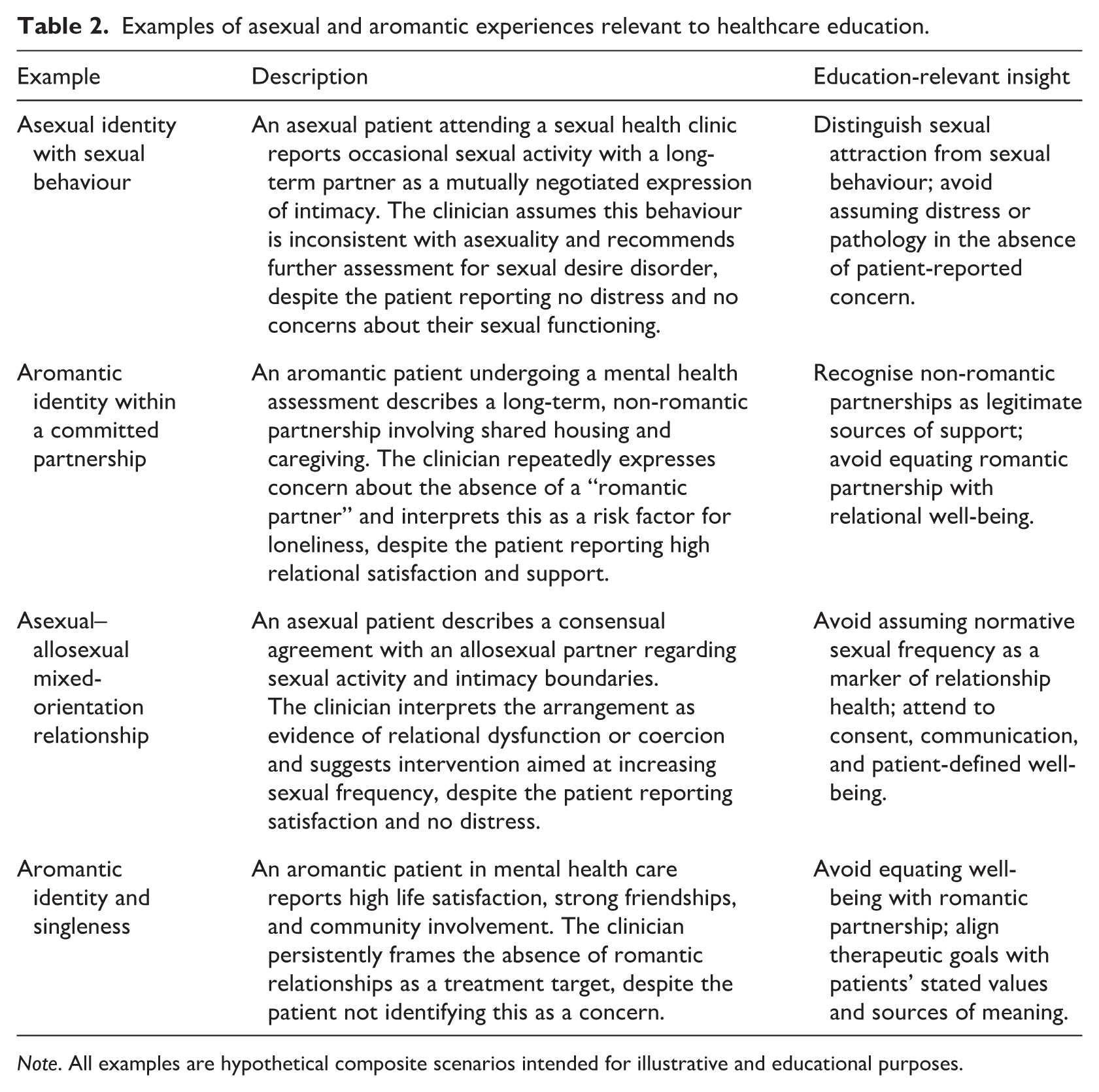
Note. All examples are hypothetical composite scenarios intended for illustrative and educational purposes.
A common source of clinical misunderstanding arises from the assumption that sexual attraction, sexual desire, and sexual behaviour necessarily align (Hagai and Zurbriggen, 2022: 56). Asexuality, however, is defined by patterns of sexual attraction rather than by sexual behaviour or capacity for intimacy. Consequently, asexual individuals may relate to sex in diverse ways. Some may be sex-averse or sex-indifferent, while others are sex-favourable and may engage in sexual activity for reasons including intimacy with partners, relational negotiation, curiosity, pleasure, or reproduction (Oliveira et al., 2021). Importantly, engagement in sexual activity does not invalidate an asexual identity, nor does lack of sexual activity necessarily indicate distress or dysfunction.
In healthcare settings – particularly sexual and reproductive health – failure to distinguish between attraction and behaviour can lead to inappropriate assumptions about risk, well-being, or pathology (Centers for Disease Control and Prevention, 2024; Thomas et al., 2026). Clinicians may assume that asexual patients who report sexual activity are misidentifying, or that those who are not sexually active require intervention. Such encounters exemplify how narrow definitions of sexuality can undermine ethical assessment and patient autonomy – an issue revisited below.
Aromanticism similarly challenges dominant assumptions about intimacy and relationships. Aromantic individuals experience little or no romantic attraction, yet may form meaningful, committed, and long-term relationships. These include close friendships, family-based bonds, community-centred lives, or non-romantic partnerships characterised by emotional intimacy, shared living arrangements, or caregiving. One relational form particularly relevant for healthcare contexts is the queerplatonic relationship: a committed, emotionally significant partnership that is not grounded in romantic attraction. Such relationships may involve cohabitation, shared finances, or mutual care, but are often rendered invisible by healthcare systems that prioritise romantic partnerships as the primary marker of social support. In mental health and psychosocial assessments, the inability to recognise non-romantic forms of commitment may result in inaccurate evaluations of patients’ support networks or relational well-being.
Asexual and aromantic individuals are likely to be in relationships with allosexual or alloromantic partners, which requires explicit communication and negotiation around intimacy, sexual activity, emotional expectations, and boundaries. Such negotiations may include decisions to engage in sex for relational reasons, to prioritise non-sexual forms of intimacy, or to explore alternative relationship structures such as consensual non-monogamy. In healthcare contexts, these relationships may be misinterpreted as inherently problematic or indicative of coercion, particularly when clinicians rely on normative assumptions about sexual and romantic compatibility. Such interpretations illustrate how normative clinical goals can conflict with patients’ self-defined relational well-being.
A further misconception relevant to healthcare education is the assumption that a fulfilling life necessarily involves an ongoing romantic partnership or sexual activity. Many asexual and aromantic individuals lead satisfying lives centred on careers, friendships, creative pursuits, community involvement, or chosen family. Others may move between periods of partnership and singleness without experiencing these transitions as deficits. Within mental health settings, however, singleness or lack of romantic involvement is often framed as a problem to be addressed. This can result in therapeutic focus on relationship acquisition rather than on patients’ stated goals, values, or sources of meaning. Recognising diverse life trajectories is therefore central to patient-centred care. When clinicians equate well-being with romantic or sexual norms, they risk overlooking resilience, satisfaction, and support structures that fall outside dominant frameworks.
Taken together, these examples underscore why healthcare education should move beyond abstract definitions of asexuality and aromanticism to engage with lived relational diversity. Without such understanding, clinicians may inadvertently pathologise non-normative experiences, misinterpret relationships, or pursue clinical goals misaligned with patients’ needs. These dynamics contribute directly to negative healthcare experiences, concealment, and disengagement from care. Integrating nuanced accounts of asexual and aromantic lives into healthcare education can support more accurate assessment, reduce normative bias, and equip health professionals to ask open-ended, non-assumptive questions about intimacy, relationships, and sources of support – all of which are key foundations for inclusive, ethical practice.
Healthcare experiences of asexual and aromantic people and implications for health education
Stigma and misconceptions surrounding asexuality and aromanticism are frequently reproduced within healthcare settings, where they shape patient–provider interactions and influence the quality of care given and received. Research examining asexual individuals’ healthcare experiences indicates that many encounters are characterised by limited provider knowledge, invalidation, or the use of offensive and pathologising language. For example, asexual individuals have reported low familiarity (e.g. “my practitioner did not seem to know asexuality exists and assumed I was making it up”; Flanagan and Peters, 2020: 1635), and offensive or harmful language (e.g. “I felt my therapist perceived me as weird, by saying ‘usually hormones make their way, but you are stuck’ . . . they labelled me as a lay nun or cloistered nun”; Pavanello Decaro et al., 2025: 105). Such responses can undermine trust and contribute to feelings of marginalisation within clinical environments.
Although the literature mainly points to the negativity override regarding the healthcare experiences of asexual and aromantic people, it also documents affirming healthcare experiences. Positive encounters are associated with providers who demonstrated familiarity with asexuality (e.g. “my practitioner seemed to be familiar with the concept and was able to listen effectively”: Flanagan and Peters, 2020: 1642), and showed positive reactions (e.g. “I was treated as if what I was saying was normal and understandable; in my world, to be treated like there’s not much different from me compared to others is the greatest dignity I can be given, so I was appreciative”: p.1642) and respectfulness (e.g. “they didn’t really understand what asexuality was, they were very respectful and listened well and made no assumptions or dismissive comments” Flanagan and Peters, 2020: 1642).
Research examining the healthcare experiences of aromantic individuals remains limited. Compared to the emerging literature on asexual healthcare experiences, only a small number of studies have specifically examined aromantic populations, and there remains little comparative or large-scale research focused on aromantic healthcare experiences. This very limited research (e.g. Pavanello Decaro et al., 2025) shows that aromantic people may face micro-aggressive responses from healthcare professionals regarding their aromanticism (e.g. “You only need to go out and have experiences to see what you like”). Areas in which aromantic people may face prejudices include the misinterpretation of aromanticism as fear of intimacy, depression, low self-esteem, medically induced loss of romantic attraction, etc. Therefore, both in physical and psychological healthcare settings, the prejudices that aromantic people may face should be addressed.
Together, these findings point to a clear need for healthcare education to more explicitly address asexual and aromantic identities. Expanding healthcare professionals’ knowledge and fostering reflective, non-assumptive practice – particularly within discipline-specific training – may substantially improve the healthcare experiences of asexual and aromantic patients.
Thematic structure of asexual and aromantic people’s healthcare experiences: Evidence from recent literature
Across the limited qualitative literature examining asexual and aromantic people’s healthcare experiences, a consistent theme emerges in which healthcare environments are frequently experienced as invalidating, exclusionary, and shaped by normative assumptions about sexuality and intimacy. This paper draws on two recent qualitative studies: Pavanello Decaro et al. (2025), which explored healthcare interactions reported by 284 asexual and aromantic individuals using codebook thematic analysis, and; Meera (2025), a phenomenological study based on semi-structured interviews with 43 asexual participants. Together, these studies provide converging insights into how interpersonal interactions and institutional practices shape asexual and aromantic people’s trust, disclosure, and engagement with healthcare.
Across these studies, seven recurring themes were identified, comprising five themes reflecting negative healthcare experiences and two themes reflecting positive or affirming encounters (Table 3). The synthesis below is organised around these themes, illustrating the mechanisms through which healthcare encounters may undermine or support inclusive, patient-centred care for asexual and aromantic individuals.
Asexual and aromantic people’s healthcare experiences identified in recent qualitative studies.
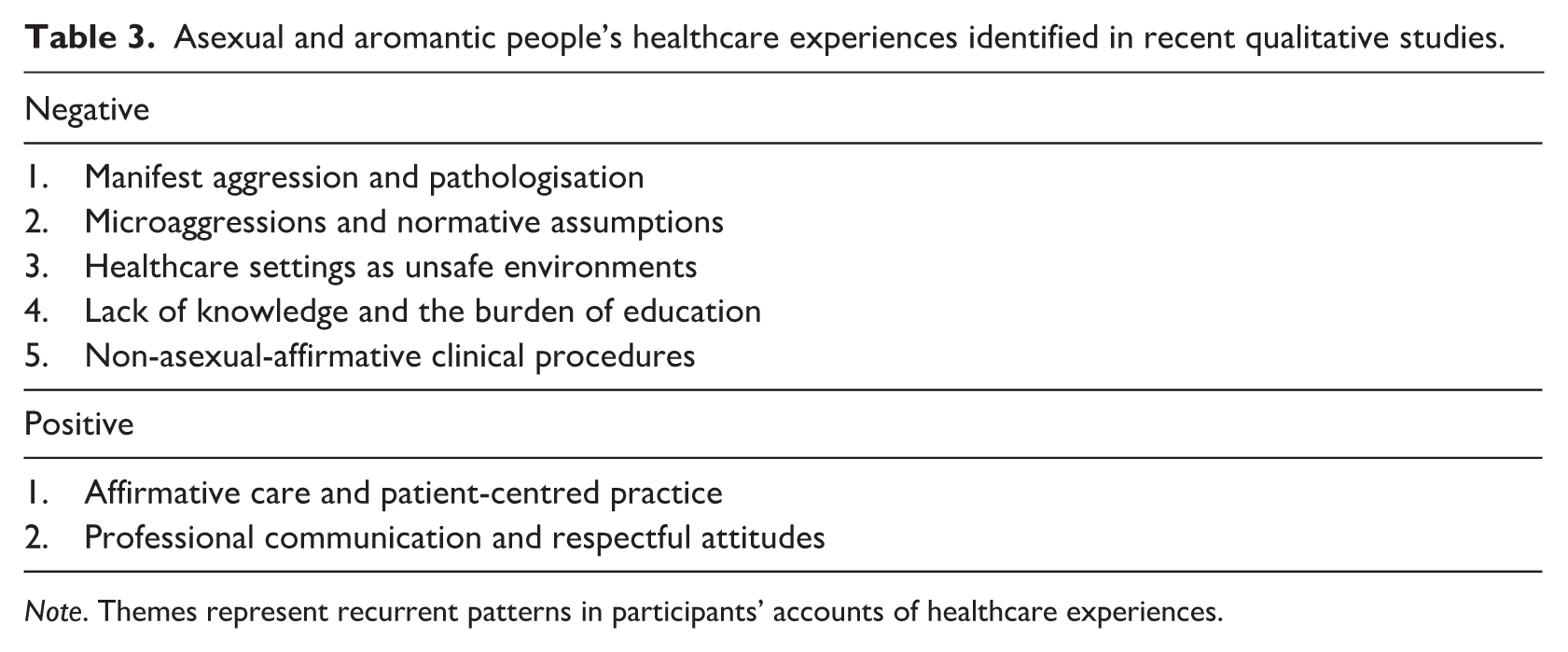
Note. Themes represent recurrent patterns in participants’ accounts of healthcare experiences.
Negative healthcare experiences
Manifest aggression and pathologisation
Participants in both studies reported experiences of overt hostility or explicit invalidation when disclosing asexual or aromantic identities. These encounters frequently involved offensive or harmful language, as well as attempts to pathologise asexuality by attributing it to trauma, hormonal dysfunction, psychological immaturity, or moral deficiency. Such responses reflect a biomedical and psychosexual framework in which sexual attraction is constructed as universal and developmentally necessary for well-being, rendering asexuality unintelligible except as pathology.
In some cases, participants recounted being told that asexual people “do not exist,” or that a lack of sexual attraction must be explained through childhood trauma or a psychological deficit. These responses positioned asexual individuals as inherently deficient and reinforced asymmetrical power relations within patient–provider interactions. Rather than recognising asexuality as a legitimate sexual orientation or identity, health providers framed it as a symptom requiring explanation or intervention, undermining patients’ self-understanding and trust in care.
Microaggressions and normative assumptions
More common than overt hostility, participants described subtle and pervasive microaggressions embedded within routine clinical encounters. These microaggressions were grounded in allonormative, heteronormative, and cisnormative assumptions, such as expectations that patients are sexually active, desire romantic relationships, or experience distress due to the absence of sexual intimacy. Even when not overtly hostile, such assumptions communicated that asexual and aromantic identities were abnormal, undesirable, or incomplete.
Examples included therapists implicitly framing singleness or lack of romantic interest as a problem to be addressed in therapy, or assuming heterosexuality despite explicit clarification. Participants reported that these microaggressions were particularly damaging because they were often dismissed as benign or unintentional, making them difficult to challenge. Over time, repeated exposure to these assumptions contributed to feelings of alienation and erosion of trust in healthcare professionals.
Healthcare settings as unsafe environments
As a consequence of repeated invalidation, many participants described healthcare settings as unsafe environments for disclosure. Participants frequently reported intentionally concealing their asexual or aromantic identities to avoid misunderstanding, dismissal, or inappropriate questioning. In some cases, concealment occurred because providers did not create space for discussions of sexuality or relationships, particularly when sexual orientation was assumed to be irrelevant or uncomfortable to address.
Importantly, concealment was not indicative of disengagement or indifference, but rather a protective strategy shaped by prior negative experiences. Decisions about disclosure reflected calculated assessments of risk, where the potential harm of disclosure outweighed perceived benefits. These accounts highlight how healthcare environments can indirectly silence asexual and aromantic identities through normative expectations and limited provider responsiveness.
Lack of knowledge and the burden of education
A pervasive theme across both studies was the lack of professional knowledge regarding asexuality and the asexual spectrum. Participants frequently encountered providers who were unfamiliar with asexuality or held misconceptions about its meaning, leading to inaccurate interpretations of patients’ experiences. In many cases, providers relied on stereotypes or conflated asexuality with sexual dysfunction or psychological disorder.
A particularly salient consequence of this knowledge gap was the expectation that patients should educate their providers. Participants described feeling as though they were teaching rather than receiving care, a role reversal that disrupted therapeutic boundaries and placed an additional emotional burden on them. While some participants were willing to provide educational resources, this responsibility was often experienced as exhausting and inappropriate, particularly in therapeutic contexts where support rather than explanation had been sought.
Notably, ignorance alone was not necessarily experienced as harmful. Participants distinguished between providers who lacked knowledge but demonstrated openness, humility, and willingness to listen, and those who responded defensively or dismissively. Providers who acknowledged their limitations and engaged respectfully were often perceived positively, underscoring the importance of reflexivity and professional attitudes alongside factual knowledge.
Non-asexual-affirmative clinical procedures
Beyond interpersonal interactions, participants identified structural and procedural barriers that rendered healthcare systems non-affirmative of asexual identities, even when individual providers were supportive. Standardised assessment tools, routine screening practices, and mandatory testing often failed to account for asexuality, resulting in experiences of invalidation within otherwise affirming clinical relationships. For example, depression inventories that treat low sexual interest as an indicator of pathology were experienced as particularly problematic, as they failed to distinguish between distress-related changes in sexual desire and stable asexual orientations. Similarly, mandatory pregnancy testing and persistent pressure to undergo sexual or reproductive health procedures were described as dismissive of patients’ stated sexual histories and intentions. These practices illustrate how institutional norms and protocols, rather than individual provider intent alone, can perpetuate allonormativity within healthcare systems and reinforce marginalisation at a structural level.
Positive healthcare experiences
Affirmative care and patient-centred practice
Although less frequently reported, both studies identified affirming healthcare experiences that contrasted sharply with dominant narratives of marginalisation. Positive encounters were consistently associated with providers who adopted patient-centred approaches, recognised asexual identities as legitimate aspects of patients’ lives, and avoided reducing individuals to single defining features.
Participants valued providers who acknowledged how asexuality intersected with other aspects of identity, such as gender, disability, or mental health, while respecting these dimensions as distinct. This multifaceted approach allowed care to be tailored to individual needs and avoided reductive or essentialist interpretations of asexuality.
Professional communication and respectful attitudes
Professional communication practices played a central role in shaping positive healthcare experiences. Participants consistently emphasised the importance of being believed, listened to, and accepted without judgement. Providers who treated asexual identity as a factual aspect of the patient’s experience – rather than something to question, explain, or resolve – were perceived as particularly supportive.
Transparent communication further contributed to positive encounters. When providers clearly explained procedures, involved patients in decision-making, and invited questions, participants reported feeling more at ease and more trusting of the healthcare process. Respect for patient autonomy, particularly in sexual and reproductive health contexts, countered assumptions that sexual activity is inevitable or necessary for well-being and validated asexual individuals’ self-knowledge and boundaries.
Implications for health education and professional training
The reviewed literature underscores specific and actionable priorities for healthcare education and professional training aimed at improving care for asexual and aromantic patients. In the literature, both positive and negative healthcare experiences were shaped less by the clinical context itself than by health providers’ knowledge, communication, assumptions, and ability to offer patient-centred care. These findings indicate that shortcomings in healthcare encounters are not merely interpersonal but reflect broader gaps in education and training. The following sections synthesise key implications for health education and professional practice, with a focus on how curricula and training programmes can better equip healthcare professionals to provide inclusive, affirming care for asexual and aromantic people and populations.
Building foundational knowledge of asexual and aromantic identities
A consistent finding across the studies was the importance of healthcare providers having a basic understanding of asexuality and aromanticism. Participants frequently reported negative experiences when providers appeared unfamiliar with asexual and aromantic orientations or questioned their legitimacy, leading to confusion, frustration, or disengagement from care. Lack of knowledge sometimes resulted in providers assuming that asexuality or aromanticism did not exist, or that it must be explained by trauma, mental illness, or sexual dysfunction. This unfamiliarity may be attributed to providers reading more about disorders and diseases and less about individual differences in respect to sexuality and intimacy.
Importantly, positive healthcare experiences were not limited to encounters with providers who had extensive prior knowledge of asexuality or aromanticism. Several participants described affirming experiences with health providers who openly acknowledged their limited knowledge but demonstrated curiosity, humility, and a willingness to listen. This suggests that health professional education should not only provide foundational knowledge about asexual and aromantic identities, but also cultivate cultural humility, reflective practice, and skills in respectful inquiry. In this context, “knowing enough to ask respectfully” means recognising that attraction, identity, behaviour, intimacy, relationship structure, and distress are distinct, and avoiding assumptions about what this means for a patient’s health, well-being, or care needs. Training should therefore support providers to ask open, non-pathologising questions, respond affirmingly to disclosure, and recognise asexual and aromantic identities as valid rather than as problems to be explained or corrected. Consistent with this, Lu and Chui (2025) emphasised the importance of respect and humility in clinical encounters with asexual patients, positioning these qualities as central to affirming and supportive mental healthcare.
Affirmation and avoidance of pathologisation
Across studies, asexual and aromantic patients emphasised the importance of having their sexual and romantic orientations respected, accepted, and validated. Affirming care was characterised by providers treating asexual and aromantic orientations as valid approaches to sex and/or relationships rather than as problems to be solved. On the other hand, negative experiences involved the pathologisation of asexuality and aromanticism, including attempts to identify a cause, frame the identity as a symptom, or suggest it required treatment. Therefore, healthcare providers are advised to validate and accept the experiences and orientations of asexual and aromantic individuals, and not to view asexuality or aromanticism as pathologies.
Communication, attitudes, and relational safety
Consistent with themes relating to microaggressions and unsafe healthcare environments, participants emphasised the importance of respectful and non-assumptive communication. How providers communicate with asexual and aromantic patients strongly influences how healthcare encounters were experienced. Positive interactions were marked by respectful language, calm and supportive reactions to disclosure, and a non-judgemental attitude. Participants valued providers who responded to disclosures of asexual and aromantic identity without surprise, dismissal, or attempts to normalise the identity through statements such as “You’ll find the right person.”
Conversely, negative experiences often involved dismissive or inappropriate reactions, including offensive language, intrusive questioning, or overtly unprofessional behaviour. Such responses undermined trust and contributed to feelings of being unsafe or misunderstood in clinical settings. These findings highlight the importance of communication skills training that emphasises respect, professionalism, and emotional awareness, particularly when working with marginalised sexual and romantic minorities. While training on professional ethics has been incorporated into some healthcare curricula (e.g. Melhem et al., 2025), research suggests there is variability in the depth and consistency of ethics and professionalism training across educational contexts (e.g. Noor et al., 2024).
Patient-centred and collaborative care
Patient-centred care emerged as a key determinant of positive healthcare experiences for asexual and aromantic individuals. Participants described feeling supported when providers prioritised their stated needs, preferences, and goals, rather than making assumptions based on sexual or romantic norms. Collaborative approaches, in which patients are actively involved in decision-making and felt their autonomy was respected, were particularly valued. While collaboration is strongly emphasised in certain treatment approaches, such as cognitive behavioural therapy (Beck, 2020), research suggests that patient-centred collaborative principles are not always implemented consistently in practice. These findings reinforce the importance of strengthening these approaches within professional education and ongoing training.
Transparency in communication is also important. Providers who clearly explained procedures, discussed options openly, and ensured that patients understood and consented to care fostered greater trust and comfort. In contrast, experiences in which providers imposed unwanted procedures or dismissed patients’ concerns contributed to feelings of disempowerment. A review study by (Chryssofos et al., 2025) found that across different surgical and medical training levels and specialties, education on informed consent needs to be more robust. These findings reinforce the importance of teaching patient-centred and shared decision-making approaches in healthcare education, which in turn can improve comfort, trust and the overall experiences of patients.
Avoiding assumptions, microaggressions, and structural harm
Findings relating to normative assumptions and non-affirmative clinical procedures highlight the importance of addressing structural and interpersonal bias within healthcare education. A recurring theme across studies was the harm caused by assumptions embedded in both interpersonal interactions and institutional practices. Participants described microaggressions rooted in allonormative, heteronormative, or cisnormative assumptions, such as being presumed to be sexually active or interested in romantic relationships. These assumptions often resulted in repeated invalidation of patients’ self-reports.
Structural practices also posed challenges for asexual and aromantic patients. Standardised screening tools, mandatory pregnancy tests, and routine sexual health procedures were frequently experienced as inappropriate or distressing when applied without consideration of an individual’s sexual history or identity. While such practices are often well-intentioned, they can unintentionally create unsafe environments and discourage disclosure. Health professions education should therefore encourage critical reflection on how standard clinical practices may affect diverse patient populations and how care can be adapted accordingly.
Conclusion
Overall, the reviewed literature indicates that affirming healthcare for asexual and aromantic individuals depends on a constellation of interrelated factors rather than any single provider attribute or clinical skill. Key elements include foundational knowledge of asexuality and aromanticism, respectful and non-judgemental communication, and the consistent application of patient-centred care that recognises the intersection of sexual and romantic identities with other aspects of patients’ lives, such as gender, mental health, and disability. Conversely, negative healthcare experiences were most commonly associated with pathologisation, normative assumptions about sex and romance, microaggressions, and non-affirmative clinical procedures. Collectively, these findings underscore the need for healthcare education and professional training that explicitly includes asexual and aromantic identities, promotes reflexivity and respectful engagement, and equips providers to deliver inclusive, ethically sound care across diverse sexual and romantic experiences.
Importantly, this paper moves beyond documenting the marginalisation of asexual and aromantic individuals within healthcare settings to translating qualitative evidence into concrete educational and professional education and training priorities. By synthesising recurring themes across the reviewed literature and mapping these onto actionable recommendations, illustrative teaching scenarios, and a practical training checklist, the paper provides a framework for integrating asexual and aromantic perspectives into healthcare curricula and professional development.
To support translation of these insights into educational practice, Table 4 presents a checklist that synthesises the reviewed qualitative evidence into actionable priorities for healthcare education and professional training. This checklist is intended as a practical tool for educators, curriculum designers, and educators and trainers seeking to integrate asexual and aromantic perspectives into foundational curricula, clinical skills training, and continuing professional development.
Checklist for inclusive healthcare education and training on asexual and aromantic people.
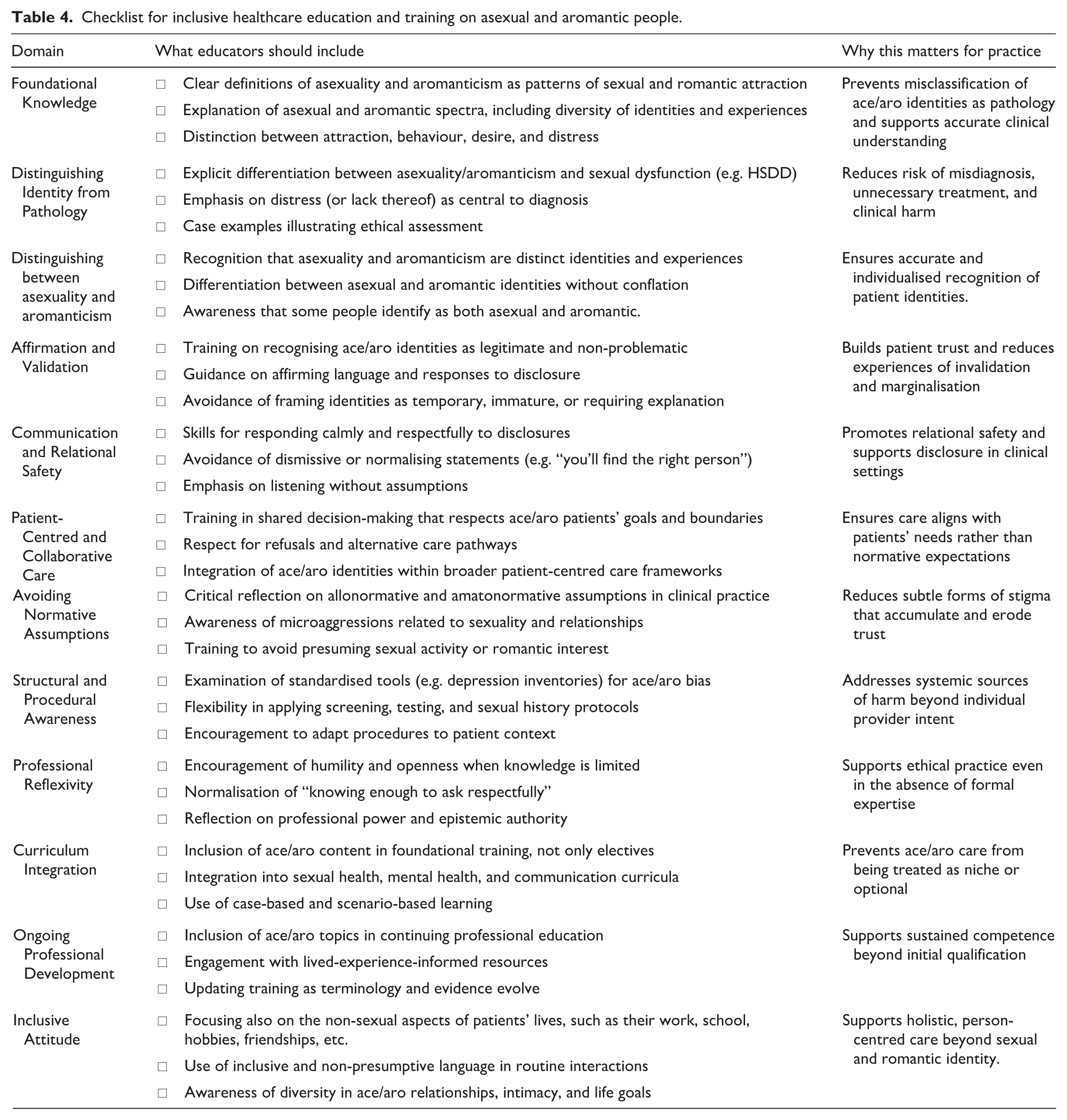
The reviewed literature demonstrates that affirming healthcare requires more than provider goodwill alone. It also requires awareness of normative assumptions surrounding sex and romance, alongside healthcare systems and educational frameworks capable of recognising diverse forms of intimacy, identity, and well-being. Without such changes, healthcare systems risk continuing to pathologise or marginalise experiences that fall outside dominant sexual and relational norms. Integrating asexual and aromantic perspectives into healthcare education is therefore not a niche or optional addition, but an important component of ethical, inclusive, and evidence-informed healthcare practice.
Future research
While this review has focused on healthcare experiences from the perspectives of asexual and aromantic individuals, future research would benefit from examining the perspectives of healthcare professionals and educators themselves. Investigating clinicians’ understandings, assumptions, and training experiences related to asexuality and aromanticism may provide insight into how stigma and misunderstanding are reproduced – or interrupted – within healthcare settings. Such work could inform more targeted educational programme and interventions, and support the development of training that addresses both knowledge gaps and normative professional cultures.
Finally, although research on asexual individuals’ healthcare experiences remains limited, research focusing specifically on aromantic individuals is even more sparse. Given the likelihood that aromanticism is frequently misinterpreted within clinical contexts – as a symptom of depression, low self-esteem, avoidant personality traits, or medical dysfunction – future research should prioritise the systematic examination of aromantic people’s healthcare experiences in their own right. Expanding this evidence base is essential for ensuring that healthcare education and practice adequately reflects the full diversity of sexual and romantic experiences.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A.M. was supported by an Australian Government Research Training Programme (RTP) Scholarship. J.A. was supported by the Australian Research Council [DE230101636].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
There are no data associated with the publication of this article.
AI declaration
Generative AI tools were lightly used to support proofreading, clarity, and English-language expression. All AI-assisted suggestions were reviewed and revised by the authors, who take full responsibility for the final content of the manuscript.