Abstract
These medication errors have occurred in health care facilities at least once. They will happen again—perhaps where you work. Through education and alertness of personnel and procedural safeguards, they can be avoided. You should consider publishing accounts of errors in your newsletters and/or presenting them in your inservice training programs.
Your assistance is required to continue this feature. The reports described here were received through the USP Medication Errors Reporting Program (MERP), which is presented in cooperation with the Institute for Safe Medication Practices. If you have encountered medication errors and would like to report them, you may call USP toll-free, 24 hours a day, at 800-233-7767 (800-23-ERROR).
Any reports published by ISMP will be anonymous. Comments are also invited; the writers’ names will be published if desired. ISMP may be contacted at the address shown below.
Errors, close calls, or hazardous conditions may be reported through the ISMP (www.ismp.org) or USP (www.usp.org) Web sites or communicated directly to ISMP by calling 800-FAIL-SAFE or via E-mail at
Exubera: Risk of Dosing Errors
A new form of inhaled insulin, Exubera (insulin human [rDNA origin]), is about to become available or may even have been marketed by now. The drug has an onset of action similar to rapid-acting insulin analogs and must be inhaled about 10 minutes before a meal. It's duration of activity is comparable to subcutaneously administered regular human insulin. The drug will be available as a powder in 1 mg and 3 mg blisters, to be administered using an Exubera Inhaler.
We have already heard from pharmacists about the risk of serious errors with this high-alert drug. Exubera is dosed in mg (as it was during clinical trials), with a weight-based dosing chart for initial mg doses, and a conversion chart for equivalent doses in units. Confusion between doses ordered in mg and units seems inevitable, especially given the following. First, the drug will be used in conjunction with injectable insulin, dosed in units. Next, the 1 mg blister is equivalent to “3” units of insulin, thus the risk of confusion between the “3” mg blister and “3” units is heightened. Another potential source of error is that the equivalency of mg to units is not exactly incremental. For example, 1 mg of the drug is equal to 3 units of insulin, but a 3 mg dose is equal to 8 units, not 9 units, as may be expected. Likewise, consecutive inhalation of three 1 mg blisters results in significantly greater insulin exposure than inhalation of one 3 mg blister, due to differences in retention of blister contents. Thus, three 1 mg doses should NOT be substituted for one 3 mg dose.
While this less intrusive route of administration for insulin is welcomed, for safety reasons, current dosing instructions and labeling should not have been approved. We have alerted FDA and Pfizer to these problems. Meanwhile, please warn health care practitioners about this serious problem as soon as possible, before the drug reaches your inventory. By the way, the Exubera package insert includes the abbreviation “U” for units, and the dosing table refers to “unit” equivalents as “international units,” expressed as “IU.” Both are error-prone abbreviations included in the Joint Commission's, ISMP's, and FDA's lists of error-prone abbreviations.
Using Technician Errors as an Opportunity for Change
In an October 2005 article in the American Journal of Health-System Pharmacists, the results of a random nationwide survey of more than 800 pharmacy technicians’ views about their medication errors was published (Desselle SP. Certified pharmacy technicians’ views of their medication preparation errors and educational needs. Am J Health Syst Pharm Oct. 1, 2005; 62:1992–97). Most of the technicians worked in community pharmacies, but more than a quarter (27%) were employed in hospitals.
As one might expect in both settings, interruptions and inadequate staffing were among the most frequent factors perceived to contribute to technician medication preparation errors. Inadequate staffing was perceived as especially problematic in chain pharmacies, while inadequate supervision by pharmacists was cited as a factor more frequently by hospital technicians. It also may come as no surprise that the pharmacists’ most frequently cited response to an error that was caught during the checking process was to make the technician aware of the error and require him or her to correct it. However, only about 17% of the technicians reported that the pharmacist had used the error as an opportunity to provide instructions on how to avoid the same or similar errors in the future.
While many of these respondents attributed this responsibility to the organization as a whole, not necessarily the individual pharmacist who detects an error, it appears technicians may not be receiving guidance about system and process changes that can help avert errors. After an error is corrected, the checking pharmacist should find time that day (or the next day, if necessary) to review the error with the technician and suggest ways to avoid it, including safer behavioral choices if applicable. Later, during pharmacy staff meetings or other forms of intradepartmental communication, errors, their causes, and ways to prevent them should be shared with all staff in a way that does not embarrass those who were possibly involved in the errors.
Sodium Bicarbonate Extravasation
Repeated doses of undiluted IV sodium bicarbonate delivered to an elderly hospitalized man with statin-induced rhabdomyolysis resulted in a serious infiltration at the peripheral IV access site. On admission to the emergency department, the patient's potassium level was 8.2 mEq/L. He was treated for hyperkalemia with regular insulin, 50% glucose, and 50 mEq of sodium bicarbonate via slow IV push. Once in ICU, he received three additional doses of 50 mEq of sodium bicarbonate, each 2 hours apart, via slow IV push into an IV site through which normal saline had been infusing at 125 mL/ hour. Before the third and final repeat dose, the patient complained of pain at the IV site on his left hand, which was swollen and beginning to turn purple. However, the nurse continued to administer this dose into the existing IV site and, afterwards, changed the site to the right hand. Unfortunately, the patient's left hand continued to swell and became a dusky purple for 2 more days, after which healing was very slow.
Inadvertent extravasation of hypertonic solutions of sodium bicarbonate has reportedly caused chemical cellulitis due to its alkalinity, subsequently resulting in tissue necrosis, ulceration, and/or sloughing at the site of the injection. Although not recommended for routine use during cardiopulmonary resuscitation, sodium bicarbonate is sometimes given slow IV push if other efforts per advanced cardiovascular life support (ACLS) guidelines have been ineffective. For administration in non-emergent situations through peripheral lines, diluting the drug to a 1:1 concentration with sterile water for injection, and administering it via an infusion over a longer period of time (1 to 8 hours) can reduce the risk of serious harm in the event of extravasation. Review your current guidelines for IV administration of sodium bicarbonate and make any necessary changes to avoid the risk of extravasation.
Mucinex-Mucomyst Mix-Ups
A pharmacist received an order for Mucomyst (acetylcysteine) 600 mg PO every 12 hours. She found it unusual that there was no stop date or total number of doses specified. She also noted that the order was a transcription of a telephone order received by a nurse. After looking into the patient's medical record to identify an indication for the drug, the pharmacist found that the patient did not have an acetaminophen overdose and was not being prepped for renal protection prior to receiving IV contrast media for a radiological procedure. Instead, the patient had been admitted for acute bronchitis. The prescriber was called, and the order was clarified as Mucinex (guaifenesin) 600 mg PO every 12 hours.
If telephone orders must be used at all, immediate transcription on the chart and read back of the order is essential for patient safety. In this case, spelling the drug name during the process of reading back the order might have helped detect the misheard drug name, as would knowing the intended indication of the drug. For other prevention measures, see “What's in a name? Ways to prevent dispensing errors linked to name confusion” on our Web site at: www.ismp.org.
Incidentally, an additional complicating issue is that Mucomyst can in fact also be prescribed for long-term use (ie, no stop date) at 600 mg TID for interstitial lung disease. 1 Knowing the rationale for the medication and taking the time to be sure the medication and dose match the condition is a way to prevent this mix-up.
Mix-ups between Mucinex and Mucomyst have been reported previously2,3 and have happened with both drugs being confused with their counterparts. Considering the indication for acetylcysteine in acetaminophen toxicity, its continued use for renal protection, and more recently, for interstitial lung disease, errors of omission could lead to patient harm. We believe that Mucomyst and Mucinex present a common and potentially serious medication error situation that requires corrective action by FDA and the sponsor, Adams Laboratories. A risk management program with interventions up to and including a possible name change is warranted.
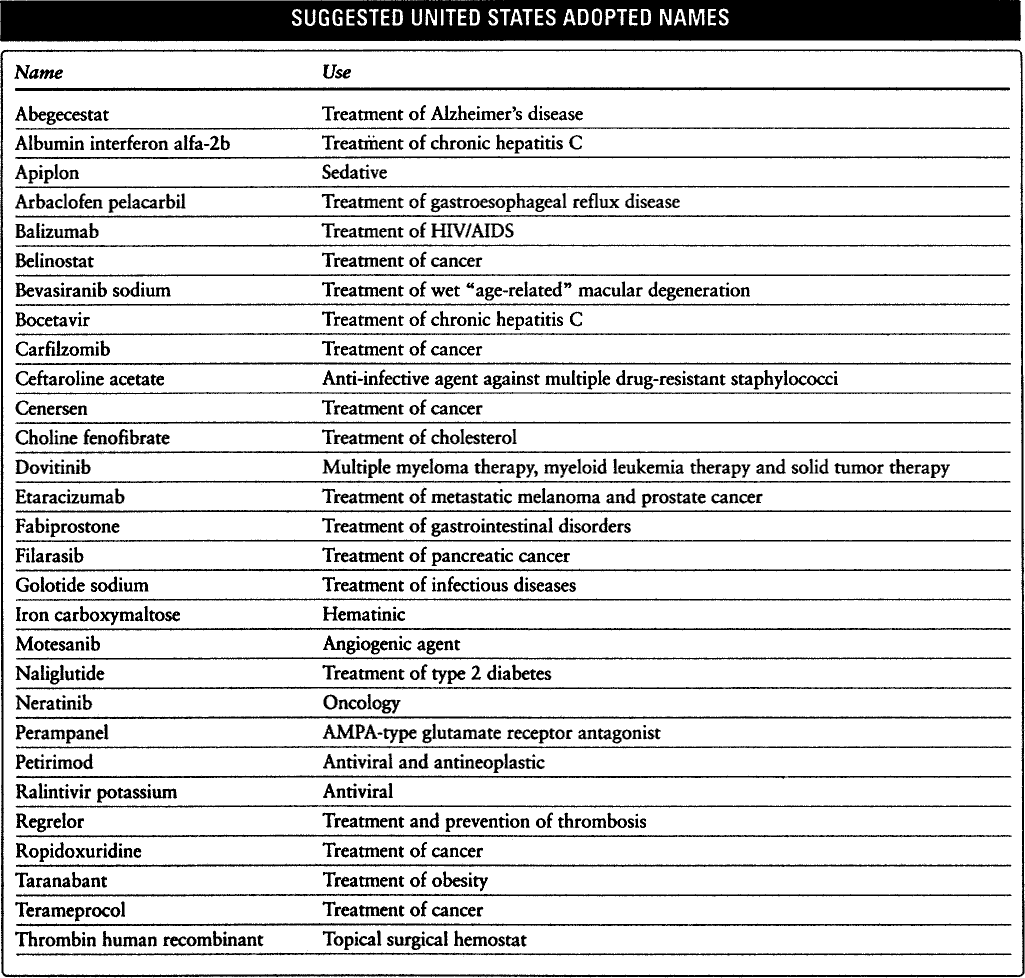
Suggested United States Adopted Names
The nonproprietary names for the drugs listed in the following table are under consideration by the United States Adopted Names (USAN) Council. All of the names listed are new suggestions. Any comments or protests should be addressed to Sandra Van Laan, American Medical Association, 515 North State Street, Chicago, IL 60610.
SUGGESTED UNITED STATES ADOPTED NAMES