
Abstract
The Centers for Disease Control and Prevention estimates that there were 719 000 knee replacement surgeries and 332 000 hip replacement surgeries in the United States during 2010. 1 In the United States, the lifetime risk for total knee replacement has been estimated to be 7% for males and 9.5% for females. 2 Epidemiological studies have demonstrated similar risks for total hip replacement.3,4 Historically, postoperative pain has been recognized as a significant complication with surgical procedures, and it is defined by the American Society of Anesthesiologists as any pain that is present in a surgical patient after a procedure.5-7 Current practice is to adopt a multimodal analgesic strategy during the perioperative period, which uses a combination of techniques and medications that target different components of the nociceptive pathway.8,9 Approaches to pain management include neuraxial anesthesia, peripheral nerve blockades, periarticular injections with local anesthetics, and use of analgesic medications including opioids, selective and nonselective nonsteroidal anti-inflammatory drugs (NSAID), acetaminophen, gabapentionoids, ketamine, and alpha-2 agonists. 10 Medications are a significant part of this strategy, and the combination of medications with differing mechanisms is thought to result in additive or synergistic analgesia with a lower incidence of overall adverse events. 9 Several studies have validated the benefits of a multimodal analgesic strategy in orthopedic procedures.11-14
Liposomal bupivacaine was approved by the US Food and Drug Administration (FDA) in 2011 for administration into surgical sites to produce postsurgical analgesia. 15 The product is formulated using multivesicular liposomes encapsulating bupivacaine, which allows for prolonged release of bupivacaine for up to 72 hours after injection. 16 Approval in the United States was based on 2 pivotal trials conducted in patients undergoing hemorrhoidectomy or bunionectomy.17,18 Published studies have been conducted in a variety of other patient populations undergoing surgical procedures including hernia repair, breast augmentation, and laparoscopic urology.19-21 Studies in patients undergoing joint arthroplasty have reported variable findings relative to the effect of liposomal bupivacaine on pain control and utilization of opioid pain medications.22-25 There are limited number of studies that have specifically assessed the use of liposomal bupivacaine by a single surgeon in patients undergoing orthopedic knee or hip procedures.26-32 Evaluation of patients having undergone procedures by a single surgeon minimizes potential confounding effects of variable surgical technique. Furthermore, prior studies of liposomal bupivacaine use in joint arthroplasty have been limited by small sample sizes, minimal community hospital sites, and lack of measurements related to physical therapy milestones such as ambulation.
The objective of this study was to retrospectively evaluate the use of liposomal bupivacaine in an ethnically diverse, large sample of patients undergoing orthopedic knee or hip procedures performed by a single surgeon in a community hospital setting. The study assessed the association between the use of liposomal bupivacaine and concurrent opioid analgesic medication use, postoperative pain scores, length of hospital stay, ambulation, and range of motion.
Methods
This study involved retrospective chart review of patients who underwent joint arthroplasty from August 1, 2012, to July 31, 2014, at a 450-bed community hospital in a large metropolitan city in the United States. The Pharmacy and Therapeutics (P&T) committee at this community hospital approved the inclusion of liposomal bupivacaine to the formulary but restricted its use to only one individual surgeon for orthopedic procedures related to the knee, hip, or shoulder over the period of time from August 2013 to July 2014. Prior to the addition of liposomal bupivacaine to the formulary, patients undergoing these orthopedic procedures received an intraoperative dose of bupivacaine hydrochloride 0.5% with epinephrine, morphine, and ketorolac. The study compared a cohort of patients who underwent orthopedic procedures of the knee or hip and received intraoperative liposomal bupivacaine 266 mg (20 mL) into the joint, with a historical cohort of patients seen by the same surgeon who did not receive liposomal bupivacaine. All patients in both groups were at least 18 years old and were undergoing an orthopedic knee or hip procedure. Patients who were concurrently enrolled in a sponsored pain study were excluded from participation. This study was approved by the hospital’s institutional review board.
A report was generated from the pharmacy that provided a list of all patients with a charge for liposomal bupivacaine who had an orthopedic knee or hip procedure during a 1-year time period from August 2013 to July 2014. This group was defined as the study group. A separate report was generated from hospital admission data that included all patients who were seen by the same surgeon and who had an orthopedic knee or hip procedure during the 1-year period prior to addition of liposomal bupivacaine to the formulary (August 2012 to July 2013). This second group of patients served as the historical control group. Results are presented comparing the study group with the control group for knee patients and hip patients, respectively.
The primary clinical outcomes of interest were concurrent opioid analgesic medication use during the 72-hour postoperative time period and postoperative pain score. Additional clinical outcomes of interest included time to first rescue analgesic medication, length of hospitalization, ambulation distance in all patients, range of motion only for patients who underwent knee procedures, and opioid-induced adverse events. The total consumption of intravenous or oral opioids for the 72-hour postoperative period was converted to morphine equivalents using online conversion calculators.33,34 Time to first rescue pain medication was calculated by comparing the time of first opioid administration that was documented in the electronic medication administration record to the time noted for the end of the surgical procedure. As part of the regular standard of practice, nurses performed pain assessments at least every 4 hours during the postoperative period, and these values were documented on the electronic medical flowsheet. Patients were asked to rate their pain on a numeric rating scale where 0 indicated no pain and 10 indicated the worst pain possible. Average pain scores were calculated from these recorded pain scores immediately after surgery, the first 24-hour period (0-24 hours), second 24-hour period (25-48 hours), third 24-hour period (49-72 hours), and total postoperative period (0-72 hours). Length of hospital stay reported in days was calculated based on the difference between date of admission and date of discharge. Finally, average distance ambulated for knee and hip patients were calculated from data physical therapists recorded in the medical charts on the day of surgery and for the subsequent 3 postoperative days. Range of motion values (extension and flexion) were also reported by physical therapists for knee patients on postoperative days 1 to 3. Physician and nurse daily progress notes, along with daily vital signs, were reviewed for any documentation of adverse events including respiratory depression, hypotension, nausea, constipation, or itching.
Chi-square test was used to compare study and control groups for categorical variables like gender and race. Student t test was used to compare study and control groups for differences in means for the following variables: total opioid consumption during the 72-hour postoperative time period, average pain scores, time to first opioid rescue pain medication, length of stay, distance ambulated, range of motion, and opioid-induced adverse events. For the nonparametric variables of length of stay and time to first rescue pain medication, median and interquartile range are reported and were analyzed using Mann-Whitney U test. Furthermore, multivariate regression was used to estimate the association between the use of liposomal bupivacaine and these variables while controlling for age, gender, or race. SAS software, version 9.3 (SAS Inc, Cary, North Carolina) was used for the analyses.
Results
Patient Characteristics
The study included a total of 357 patients over a 2-year period. A total of 201 patients received liposomal bupivacaine, including 133 patients who underwent knee procedures and 68 patients who underwent hip procedures. The historical control group comprised 156 patients; of these, 111 patients underwent knee procedures and 45 patients had hip procedures. The average age of participants was 63 ± 11 years. No statistically significant differences were noted between any of the groups with respect to age, gender, or race (Table 1).
Baseline Characteristics of Knee and Hip Arthroplasty Patients.
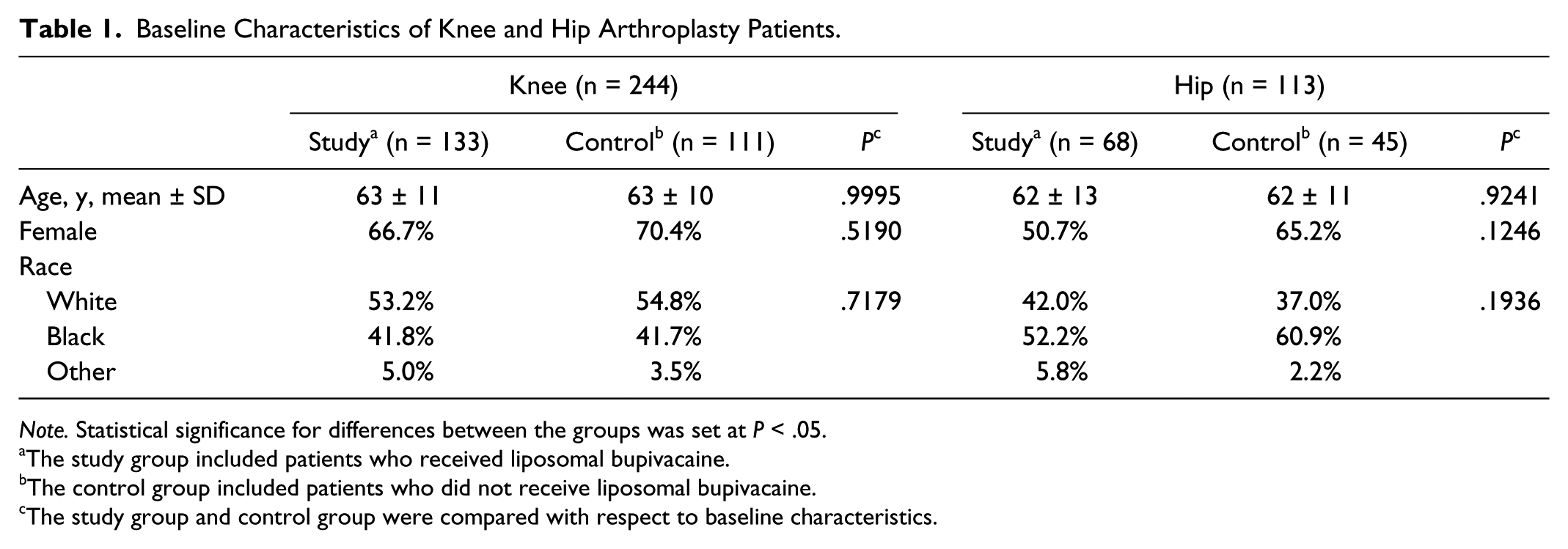
Note. Statistical significance for differences between the groups was set at P < .05.
The study group included patients who received liposomal bupivacaine.
The control group included patients who did not receive liposomal bupivacaine.
The study group and control group were compared with respect to baseline characteristics.
Knee Procedures
Patients in the knee study group, compared with those in the control group, received significantly lower amounts of opioid pain medication over the 72-hour postoperative period (209.4 ± 117.3 vs 247.8 ± 148.3 in milligrams of morphine equivalents; P < .05) (Table 2) and had a significantly delayed time to first rescue pain medication (4.0 [2.8-8.0] vs 3.0 [2.0-6.0] hours; P < .05) (Table 2). Average pain scores for the 72-hour postoperative period, however, were significantly higher in the study group (6.38 ± 0.96 vs 6.06 ± 1.05; P < .05). There were no significant differences in average pain score by 24-hour intervals between the groups. In addition, the median length of hospitalization was shorter in the study group than in the control group (2.0 [2.0-3.0] vs 3.0 [2.0-3.0] days; P < .0001). The results of the multivariate regression analysis were consistent with the findings above showing liposomal bupivacaine associated with decreased opioid use, delayed time to first analgesic medication, decreased length of hospitalization, and increased average pain score (Table 3). In this analysis, as age increased, patients were found to have less total opioid consumed and took longer time to ask for the first analgesic medication. In addition, females stayed longer in the hospital prior to discharge than males.
Clinical Outcomes of Knee and Hip Arthroplasty Patients.
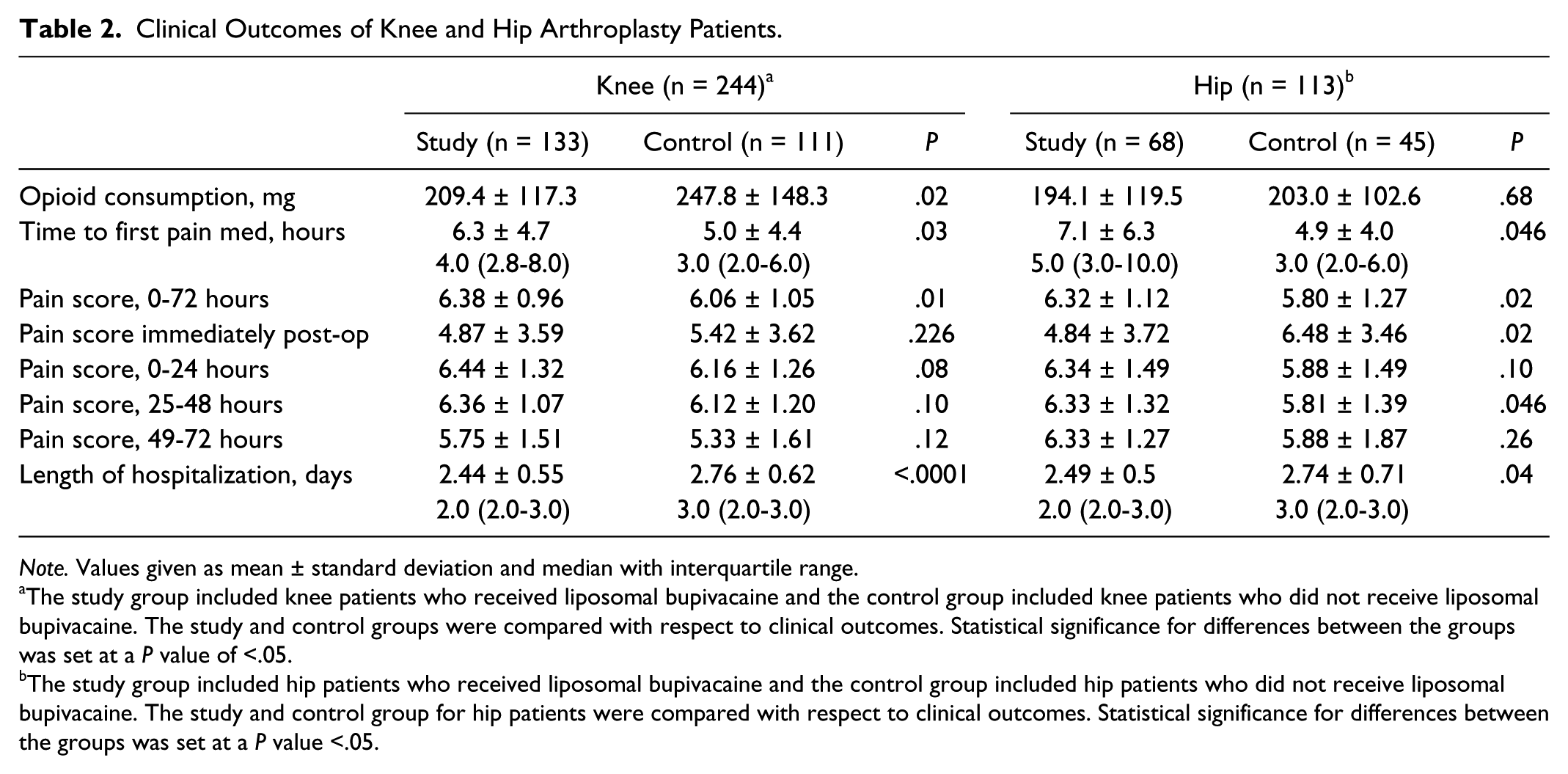
Note. Values given as mean ± standard deviation and median with interquartile range.
The study group included knee patients who received liposomal bupivacaine and the control group included knee patients who did not receive liposomal bupivacaine. The study and control groups were compared with respect to clinical outcomes. Statistical significance for differences between the groups was set at a P value of <.05.
The study group included hip patients who received liposomal bupivacaine and the control group included hip patients who did not receive liposomal bupivacaine. The study and control group for hip patients were compared with respect to clinical outcomes. Statistical significance for differences between the groups was set at a P value <.05.
Multivariate Analysis of Outcomes of Interest of Knee and Hip Arthroplasty Patients.
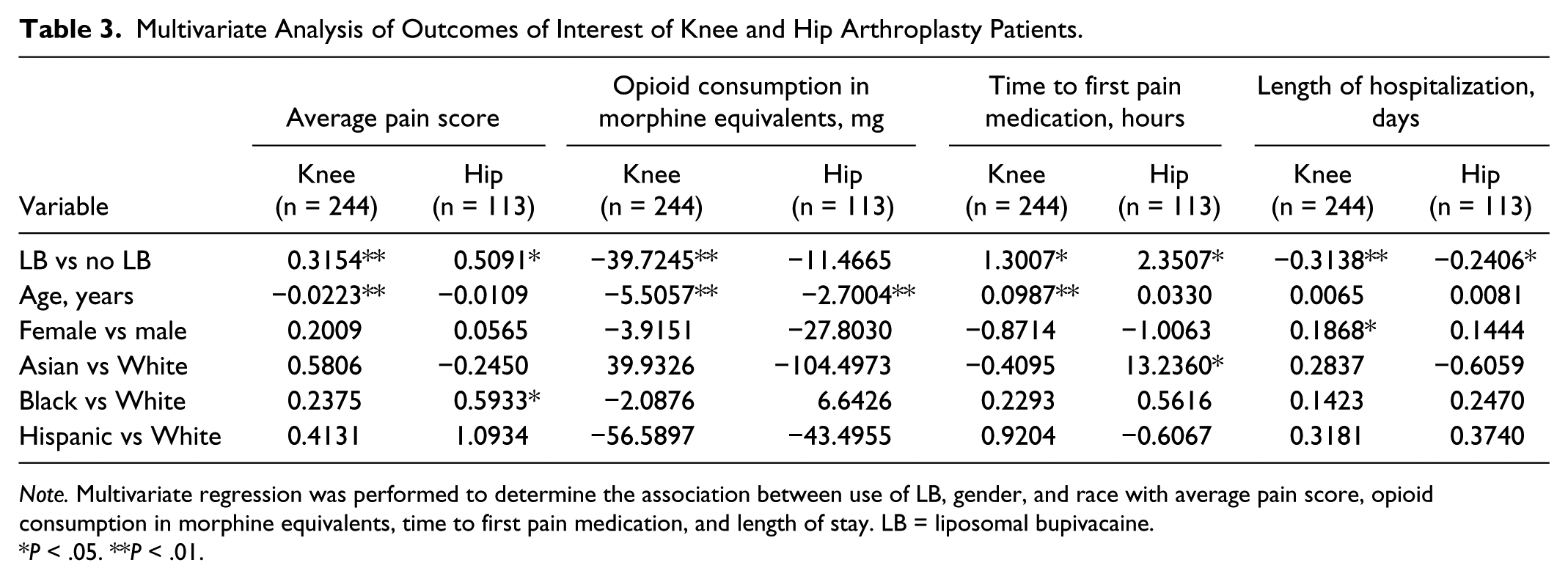
Note. Multivariate regression was performed to determine the association between use of LB, gender, and race with average pain score, opioid consumption in morphine equivalents, time to first pain medication, and length of stay. LB = liposomal bupivacaine.
P < .05. **P < .01.
There were no significant differences in ambulation distance between study and control group patients (Table 4). The degrees of knee flexion range of motion for the control group were significantly higher than the study group on day 2 after surgery (96 vs 92; P < .05) and day 3 after surgery (97 vs 93; P < .05). There were no other significant differences in range of motion observed between groups. Patients receiving liposomal bupivacaine were significantly less likely to complain of nausea (31.2% vs 45.2%; P < .001). No other statistically significant differences between groups were noted in other adverse events.
Ambulation (Feet) and Range of Motion (Degrees) in Knee Patients (n = 244).
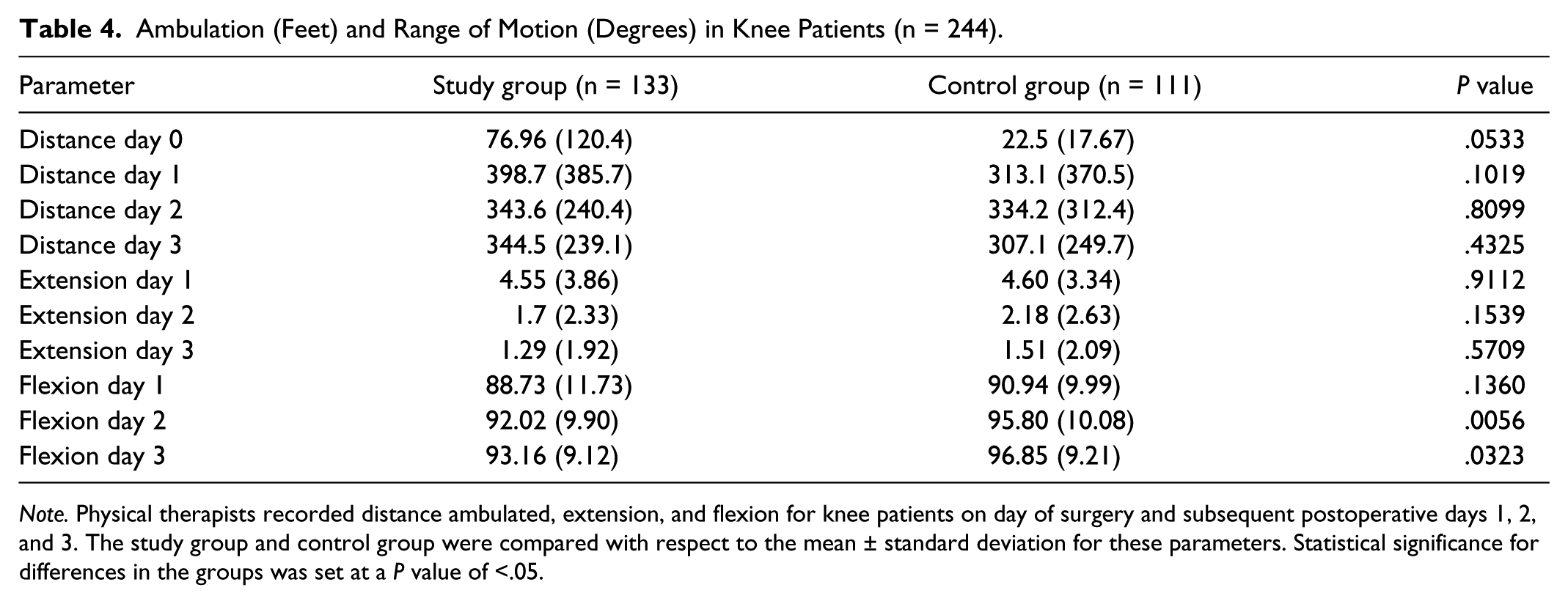
Note. Physical therapists recorded distance ambulated, extension, and flexion for knee patients on day of surgery and subsequent postoperative days 1, 2, and 3. The study group and control group were compared with respect to the mean ± standard deviation for these parameters. Statistical significance for differences in the groups was set at a P value of <.05.
Hip Procedures
Unlike the knee study group patients, there were no significant differences in opioid consumption during the postoperative phase noted between study and control groups; however, there was a statistically significant delay in time to first rescue pain medication for those patients receiving liposomal bupivacaine (5.0 [3.0-10.0] vs 3.0 [2.0-6.0] hours; P < .05) (Table 2). Similar to knee patients, there was also a higher average pain score during the 72-hour postoperative time period for patients receiving liposomal bupivacaine compared with the control group (6.32 ± 1.12 vs 5.80 ± 1.27; P < .05). Furthermore, the average pain score during postoperative day 2 (25-48 hours post-op) was significantly higher in the study group (6.33 ± 1.32 vs 5.81 ± 1.39; P < .05). The median length of hospitalization was lower in the study group (2.0 [2.0-3.0] vs 3.0 [2.0-3.0]; P < .05). Findings from multivariate regression analysis were consistent with the results above showing delayed time to first rescue analgesic medication, reduced length of hospitalization, and higher pain scores. Age was associated with a marginally lower total opioid consumption. In addition, Asian race was associated with a delayed time to first pain medication and higher average pain scores. Like the knee patients, there were only minimal differences between groups with respect to distance ambulated (Table 5). Study hip patients had a higher distance ambulated on day 2 after surgery compared with controls (335 ft vs 238 ft; P = .04); however, no other differences in ambulation were noted between groups. Similar to the knee patients, significantly fewer study group patients experienced nausea compared with the control group (24.6% vs 37.0%; P < .001).
Ambulation (Feet) in Hip Patients (n = 113).

Note. Physical therapists recorded ambulation distance for hip patients on day of surgery and subsequent postoperative days 1, 2, and 3. The study group and control group were compared with respect to the mean ± standard deviation for distance ambulated. Statistical significance for differences in the groups was set at a P value of <.05.
Discussion
We evaluated a large ethnically diverse patient population undergoing knee or hip arthroplasty performed by a single surgeon in a community hospital setting. Among patients undergoing orthopedic knee procedures, liposomal bupivacaine use was associated with a significant decrease in use of postoperative opioid analgesic medication of approximately 40 mg in morphine equivalents and delayed time to first opioid analgesic. Patients undergoing orthopedic hip procedures who received liposomal bupivacaine had similar outcomes with respect to delayed time to first opioid analgesic; however, no significant benefits were achieved in terms of reducing concurrent opioid analgesic medication use. Average pain scores for the 72-hour postoperative period were actually higher among knee and hip patients who received liposomal bupivacaine. These findings suggest that while liposomal bupivacaine may reduce the need for postoperative opioid analgesic medications, there appears to be no benefit in improving overall pain control. The decreased length of stay associated with liposomal bupivacaine of one-third of a day suggests limited potential for significantly decreasing overall health care costs related to hospitalization; however, future studies may be warranted to better characterize the potential cost implications.
The results of this study, in a larger number of patients, are similar to prior retrospective studies of total knee replacement patients that demonstrated the potential for lower concurrent opioid use.31,32 However, prospective, randomized studies have demonstrated no benefit of liposomal bupivacaine with respect to concurrent opioid use.28-30 With respect to pain scores, a larger retrospective evaluation of greater than 1000 joint arthroplasty patients receiving liposomal bupivacaine found significantly lower average pain scores in total knee replacement patients who received liposomal bupivacaine. 25 However, our study results are similar to what prior prospective, randomized studies have shown in demonstrating no clinically relevant improvement in pain control. The lack of analgesic benefit seen in overall average pain scores may be explained by the higher concurrent use of opioids in the control group and the subjective nature of pain assessments. Another unique aspect of this study is that patients receiving liposomal bupivacaine were found to have a significant delay of approximately 1.5 hours in requesting a rescue pain medication. It is possible that a delay in the first rescue pain medication can indicate some level of improved pain control during the period of time immediately after the surgery; however, the clinical significance of this is questionable given the fact that average pain scores were not different between groups during the first 24 hours after the procedure. This study is important for the literature in that it adds to the limited data regarding the effect of liposomal bupivacaine on pain management in community hospital settings, as opposed to larger tertiary academic institutions. Furthermore, the study included evaluation of physical therapy milestones such as ambulation and knee range of motion.
Ambulation as soon as possible after a surgery is an important goal in physical therapy to minimize the hazards of immobility that can include development of joint stiffness with pain, deep vein thrombosis, disuse muscle atrophy, and cardiopulmonary compromise. In a prospective, randomized trial, Surdam and colleagues reported findings suggesting that liposomal bupivacaine may be associated with improved ambulation on the day immediately after total knee replacement. 30 Results from this study indicate no significant differences in ambulation or range of motion during the entire 72-hour postoperative period among knee patients; however, there was a significant association between use of liposomal bupivacaine and a reduction in overall length of hospital stay indicating that patients receiving liposomal bupivacaine may achieve functional mobility that supports an earlier discharge.
This study contradicts results from the very limited number of published studies examining use of liposomal bupivacaine during orthopedic hip procedures, which have reported a statistically significant association with reduced opioid analgesic use.26,27 Furthermore, in this study liposomal bupivacaine was not associated with any benefit with respect to improved postoperative pain control. The difference in findings may be attributable to a larger sample size in this study compared with previous evaluations. There is significant variability in the surgical approaches and techniques used in hip procedures compared with knee procedures; therefore, benefits in one type of procedure may not predict success in other patients. This study adds to the knowledge regarding the value of liposomal bupivacaine use for orthopedic hip procedures from a rehabilitation perspective by examining the effect on distance ambulation. There were no significant improvements in distance of ambulation on most days; however, there was an unexplained significant increase on day 2. Previous studies have not examined physical therapy milestones so further studies in randomized controlled designs are warranted on any potential benefits.
No significant differences in either knee or hip patients were noted with respect to adverse events, except as related to nausea. The validity of these findings may be limited, because documentation of adverse events in the electronic medical chart had significant missing data. The decreased need for opioid medications is beneficial in improving participation in physical therapy as patients can focus on advanced skills, such as stair climbing, needed for discharge. Increased opioid use can contribute to decreased safety awareness and unnecessary falls. 35 While the shorter length of hospitalization may have minimal direct economic implications, there is a potential benefit in decreasing the risk of infection and thromboembolism from the hospital environment. Further studies are warranted to quantify the potential health economic benefits in this setting.
There are a number of limitations for this study including the retrospective study design, comparison to a historical cohort group, and significant missing data for adverse events. Having all patients seen by a single surgeon would theoretically limit any bias or confounding related to surgical technique. Multivariate regression analysis to minimize any effects of confounding variables adds rigor to the analysis.
Conclusion
The use of intraoperative liposomal bupivacaine was beneficial during orthopedic knee procedures in producing a relatively modest reduction in concurrent postoperative opioid analgesic medication; however, similar results were not seen in patients having orthopedic hip procedures. Both groups of patients experienced a delay in first opioid rescue pain medication but no clinically significant improvement in overall pain management during the 72-hour postoperative period. Differences in ambulation between groups were limited. These findings suggest a limited role for liposomal bupivacaine in achieving positive health outcomes for patients undergoing orthopedic knee or hip procedures.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.