
Abstract
Health-system and community pharmacy practice in the United States is experiencing transformational change; however, this transformation is lagging in the international arena. As a result, efforts are being made to provide support and education to the international pharmacy leaders and practitioners. This article describes one effort, the Mandela Washington Fellows Program, and suggests areas where pharmacy leaders can be involved to help advance the practice of pharmacy on an international level. The Mandela Washington Fellows Program for young Africa leaders consists of a US-Africa pharmacy-mentoring program identified ranging from educational opportunities to collaboration for implementation of patient care programs. The specifics of the mentoring program include daily meetings, clinic and ward rounds, round table discussions with mentors, and visits to various hospital care systems. Lessons were learned and strategies for sustaining the program are discussed. These types of programs represent leadership opportunities that may not be apparent to most pharmacy directors, but expanding their view to helping international pharmacists expand their practice only strengthens the professional goal of providing patient-centered pharmacy services.
Introduction
Health-system and community pharmacy practice in the United States is experiencing transformational change; however, this transformation is lagging in the international arena. Contemporary pharmacy practice, such as pharmacists as decision makers in patient care and education, is slow to progress outside of the United States due to opposition from traditional pharmacy disciplines. In addition, this slow-paced growth results from opposition by members of basic sciences faculty and physicians. This resistance has also stalled the full implementation of the proposed Doctor of Pharmacy program in various countries, including Nigeria. In addition, global pharmacy education and a consistent vision for the profession of pharmacy have not been established. In the 2010 Donald E. Franke Lecture Henry Manasse, the American Society of Health-System Pharmacists Donald E. Franke Lecturer, stated “Pharmacy is made up of polyglot definitions, diverse philosophies and various viewpoints . . . however, the profession has and is on an evolutionary journey. 1 The lack of a universal definition for the profession, the lack of a global standard for the training of pharmacists, and the lack of a definition of the competencies required of a skilled pharmacist have all been mentioned as reasons for such vast inequities between nations.
The Mandela Washington Fellowship (MWF) for young African leaders was started by President Obama in honor of Nelson Mandela. Founded in 2014, the MWF seeks to empower young leaders from sub-Saharan Africa to create change and develop solutions to the continent’s most pressing challenges. 2 Young African leaders between the ages of 25 to 35 years apply to a 6-week leadership program held in numerous universities across the United States. Applicants must have proven track records of leadership in a public, private, or civic organization and demonstrate a strong commitment to contributing their skills and talents to building and serving their communities. The 2016 class included 1000 fellows who worked in nearly 40 Universities across the United States.
The Ohio State University (OSU) hosted 25 fellows, including 1 pharmacist from the Faculty of Pharmaceutical Sciences at the University of Nigeria. As part of the leadership program, each fellow is matched with a mentor who is asked to guide and support the fellows as they learn how to apply lessons and skills gained through their fellowship experience after their return to Africa. Fellows participate in daily leadership classes, site visits, and community service activities. Volunteer faculty mentors are asked to meet with their fellow before or after these planned activities.
The Mandela Fellows program is an example of international efforts to improve health care at the level of more developed countries such as the United States, Canada, and United Kingdom. These efforts are also opportunities for health-system pharmacy leaders to contribute to improving the practice of pharmacy in other countries. The goal of this article is to use the example of the MWF program as an example to increase awareness of the pharmacy director’s role in growing the contemporary role of pharmacists around the world. Specifically this article will discuss the MWF, areas of opportunity to impact pharmacy practice through this fellowship and others, and provide some guidance to pharmacy directors who are asked to participate in similar programs. These types of programs represent leadership opportunities that may not be apparent to most pharmacy directors, but expanding their view to helping international pharmacists expand their practice only strengthens the professional goal of providing patient-centered pharmacy services.
Mandela Washington Fellowship
The 2016 class included 1 fellow who is a pharmacist (C.U.) from Nigeria. The following steps were taken with C.U. to complete his fellowship. In addition, a faculty member from the college of pharmacy and a clinical infectious diseases (ID) pharmacist at the Ohio State University Wexner Medical center (D.G.) was chosen as the Mandela faculty member for C.U.
Identifying Areas of Interest
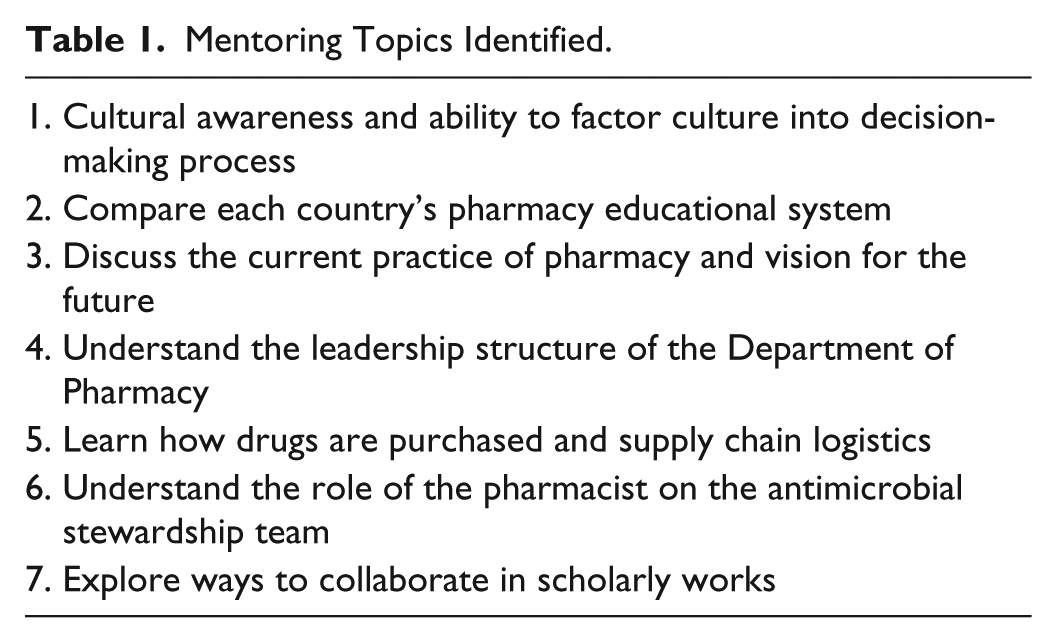
The first 2-hour mentoring session identified 7 areas of interest and value to C.U. (Table 1). D.G. invited a pharmacy master’s resident to also participate in the mentoring program acting as both a mentor to the MWF fellow and a mentee of the pharmacy faculty mentor. Time was spent getting to know each other both personally and professionally. In addition, we established a schedule, goals, and responsibilities for the mentee.
Mentoring Topics Identified.
Developing Cultural Awareness
Cultural integration in both social events and professional practice is important especially for first time visitors to a new country. C.U. attended a 4th of July celebration hosted by the mentor and the OSU fund-raising triathlon event that the mentor participated in. Both of these events were new cultural experiences for C.U. In addition, C.U. socialized with the pharmacy master’s resident to gain a student’s perspective of life on a college campus. During the cultural awareness discussions, we learned that the role of a hospital pharmacist, the process used to procure drugs both within the hospital setting and over the counter, and lack of multidisciplinary patient care teams in Nigerian hospitals were significantly different between our 2 countries. Without this cultural awareness, a mentor may recommend an idea that would be culturally insensitive or inappropriate.
Opportunities to Impact International Pharmacy Practice
The advent of the Mandela Fellowship and the connection to Ohio State developed opportunities for the department to learn about other pharmacy practices, but also work with C.U. to help him translate some of his learning from the United States to Nigeria. To accomplish this, C.U. provided a background to Ohio State on the pharmacy education systems, operational and administrative processes of Nigerian pharmacy. This led to developing a specific plan for C.U. to develop additional skills in health-system pharmacy management and leadership that C.U. could take back to Nigeria for implementation and evaluation.
Review of the Nigerian Pharmacy Education System
Pharmacy education in Nigeria dates back to the late 19th century and is known to have evolved mainly through 3 phases of development; first, dispensers were trained through informal apprenticeship style of the observe-learn-practice model. This typically lasted through the years of 1887 to 1923. The second phase introduced the use of formal schools of pharmacy for chemists and druggists between 1924 and 1961 and 2 schools of pharmacy either located on the Southern (School of Pharmacy, Yaba) and Northern (School of Pharmacy, Zaria) regions. Last, the training of “pharmacists” became standard after the 1960 Independence. 3 The Ahmadu Bello University started the formal training of pharmacists in 1968, and since then nearly 30 pharmacy schools are operational with 17 of them fully accredited and others are at some stage of obtaining full accreditation. The curriculum has largely been the same for a student to obtain the Bachelors of Pharmacy in Nigeria.
The legal inclusion of the Doctor of Pharmacy degree into the training and practice of pharmacy in Nigeria has been met with severe opposition both from nonclinical pharmacy-based pharmacists and the allied health professions. A common ground for disagreement in the training of pharmacists in Nigeria has been on whether to follow a clinical-oriented or an industrial/research-oriented training model. No one wants either training model separated and existing as a self-entity. However, in July 2016, the National Universities Commission made an announcement of the legal backing of the Doctor of Pharmacy in Nigerian schools of pharmacy. That news was greeted with excitement but also with many questions on how prepared the schools of pharmacy are to switch to this new program.
Pharmacy education at the University of Nigeria (like other schools of pharmacy in Nigeria) commences with a prospective candidates’ successful completion of 3 entry examinations after the secondary school (an equivalent of high school in the United States). The average scores from the second and third (Joint Admission and Matriculation Board, [JAMB] and University) examinations form the basis for consideration for admission to study pharmacy at the University of Nigeria. With an estimated average of 3000 applicants qualifying to write the University entrance examination, only about 200 are admitted.
Another means of admission to study pharmacy is through the “Direct Entry Examination” which is also regulated by JAMB but administered through individual schools of pharmacy. Candidate would have possessed a related science-based university or technical degree to qualify for selection. An examination is written and only a maximum of 20 successful candidates are selected. This method of admission is less competitive (due to smaller numbers of competing candidates) and eventual accepted candidates are only about 5% to 10% of all candidates annually. For both methods of admissions, no face-to-face interviews or proposals are requested. Table 2 compares the admission requirements for OSU and University of Nigeria. A notable difference in the programs is Introductory Pharmacy Practice Experiences (IPPE) is not introduced in Nigeria’s curriculum until year 3 of pharmacy school.
Admission Requirements for Schools of Pharmacy at the University of Nigeria and The Ohio State University.
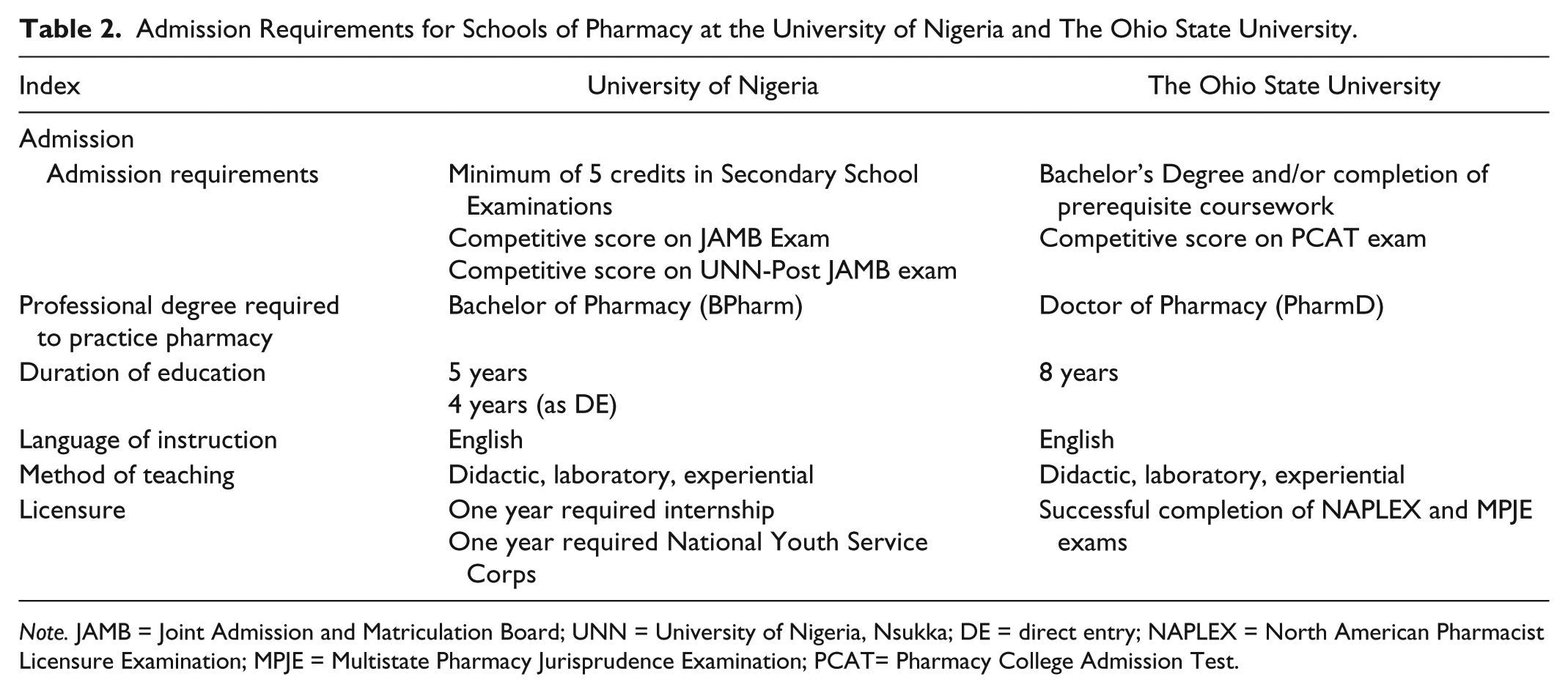
Note. JAMB = Joint Admission and Matriculation Board; UNN = University of Nigeria, Nsukka; DE = direct entry; NAPLEX = North American Pharmacist Licensure Examination; MPJE = Multistate Pharmacy Jurisprudence Examination; PCAT= Pharmacy College Admission Test.
At the University of Nigeria, the professional pharmacy degree currently is the Bachelor of Pharmacy (BPharm) and it is completed in 5 years (4 years for direct entry students). At the commencement of the program, pharmacy students take classes with students studying medicine, nursing, or physiotherapy, where they are taught advanced foundation courses. These courses include chemistry, biology, physics, and social sciences. This is the only point where interprofessional education is seen.
In the second year of study, students are required to take supportive classes (anatomy, physiology, biochemistry, and statistics) and are combined with introductory pharmacy courses such as dispensing and pharmacognosy. It is in this study year that students begin to take courses at the school of pharmacy.
From the third until the final year of study, “professional” pharmacy courses range from subjects in the fields of pharmaceutical chemistry, pharmacognosy, pharmaceutics, pharmacology, pharmaceutical technology, and clinical pharmacy. In the final year at the University of Nigeria, the clinical pharmacy course incorporates a 12-week clinical clerkship program. Students make hospital rounds with pharmacist preceptors at the University of Nigeria Teaching Hospital and the Bishop Shanahan Hospital, a rural missionary hospital.
Pharmacy Leadership in Nigerian Administrative Structures
The Ministry of Health is in charge of the health sector in Nigeria and it regulates all heath-related concerns in the country. The Chief Medical Director of each federal owned government hospital is controlled by the Health Minister. The Chief Medical Director, a physician, supervises the activities of other departmental directors and administrative heads of which the Head of Pharmacy is one. At the University of Nigeria Teaching Hospital, a 500-bed tertiary hospital, an Assistant Director of Pharmacy heads the pharmacy department. The Assistant Director (the Director is at Ministry of Health) regulates and supervises all pharmacy activities in the hospital ranging from administrative, procurement, quality assurance, storage, pricing, and distribution of medicines in the hospital. The Deputy Directors of pharmacy who are under the auspices of the Assistant Director heads each of the units highlighted above. They also directly supervise other pharmacists in the hospital, which follows a hierarchical cadre decent from chief pharmacist to principal pharmacist to junior pharmacist to intern pharmacists.
At The Ohio State University Wexner Medical Center (OSUWMC), the Administrator of Pharmacy Services leads the administrative structure of the 1400-bed health-system’s Department of Pharmacy. Similar institutions may have varying titles such as Chief Pharmacy Officer or Director of Pharmacy, but the responsibilities include oversight of all legal liability, compliance, safety, operations, and finance of the medical center’s pharmacies. There is a tiered system of Associate and Assistant Directors who hold responsibility for the day-to-day functions over specific service lines within the department. Last, there are managers and team leads who are the change drivers for implementing new pharmacy services and facilitating transitions both internal and external to the department.
Drug Purchasing and Supply Chain Logistics
The importation, manufacture, sale, and distribution of medicines in Nigeria are a very chaotic system that has been abused and severely exploited. The exploitation of the medicines supply chain has given nonpharmacists an opportunity to enter and control the drug market freely, and thus the system has been riddled with counterfeit, fake, and substandard medicines. 4 The morbidity or mortality consequences of these poisons have rarely been quantified, as there is a paucity of reliable data. One example includes the “MYPICKIN® saga” of 1990. This poorly constituted branded paracetamol killed 109 children before it was identified to contain poisonous ethylene glycol and withdrawn from the market. 5
There are laws that regulate the medicines supply chain in Nigeria and were summarized by a study attempting to evaluate the reasons for the preponderance of fake medicines in Nigeria. 6 These laws though old are still clear as regard the sacrosanct role of the pharmacist as the only custodian of medicines throughout the supply chain. Some of the laws such as the Poisons and Pharmacy Act, Cap 366 of 1990 regulates the compounding, sale, distribution, supply, and dispensing of drugs and also provides the level of control for different categories of drugs and poisons. The Counterfeit and Fake Drugs Act, Cap 73 of 1990 was also enacted into law to stem the rising tide of counterfeit, banned, or fake drugs. The act prohibits the sale of any drug in an open market without permission from the proper authority. There are also other laws that further expand the regulation of drug supply and use with the inclusion of food and food products. There are no indications yet that these laws would be reviewed or reenacted to address some “gray” areas, which have also allowed “charlatans” to exploit. Despite the availability of these laws, poor enforcement has been the bane of its effective implementation. In Nigeria today, physicians, medicine vendors, and even apprentice-trained persons can supply and distribute medicines with very little difficulty. It is widely believed in the pharmaceutical sector that the recent boost in indigenous production of medicines (especially essential medicines) could further foster a reduction in the volume of imported substandard and fake medicines.
The drug supply chain in the United States has remained relatively safe, though the complexity of the process has had its faults leading to patient harm. Threats similar to those in Nigeria have also made their way into the United States’ marketplace including counterfeiting, importation of substandard, counterfeit drugs, and gray markets. 7 These issues impact the authenticity and credibility of the supply chain, ultimately leading to ineffective or potentially harmful medications. The US government is confronting the issue of counterfeit and falsified medications by implementing the Drug Supply Chain Security Act (DSCSA). In 2013, President Obama signed into law the DSCSA, which ultimately implements a fully interoperable, electronic system for the tracking and tracing of products throughout the supply chain. To achieve this feat, the DSCSA addresses several major components including product tracking and tracing, serialization, verification, detection and response to a suspect product, and wholesaler licensing and reporting. 8
Nigerian Vision for the Future of Pharmacy Practice
Studies conducted in Nigeria, however, have shown good indices for further growth of clinical pharmacy and pharmaceutical care. There has been an evident improvement in attitudes toward pharmaceutical care provision by pharmacy students and pharmacists in Nigeria and increased preference for patient-oriented practice as career options for graduating pharmacy students.9,10
To be regarded as a clinical pharmacist in Nigeria, upon graduation or after some years of practice, one can either obtain a 2-year master’s degree in clinical pharmacy or become a fellow of the West Africa Postgraduate College of Pharmacists. The master’s degree in Clinical Pharmacy at University of Nigeria, Nsukka (UNN) focuses on therapeutics, pharmacy practice, pharmaceutical care, public health, pharmacoeconomics, and research methods. The Postgraduate College program lasts for 4 years (not within the hospital and is part-time) with the first 2 years largely focused on all disciplines in Pharmacy. Student fellows then opt to study clinical pharmacy courses for the last 2 years while completing a mandatory 6-month clinical round under the supervision of a clinical pharmacist preceptor. Both programs also incorporate research themes and projects as students complete a thesis in any of the areas mentioned above. There are still no specialist clinical pharmacists by formal training in Nigeria, but rather by experiential learning. With only a handful of US-trained PharmD specialists in Nigeria, the effective implementation of the PharmD program will be difficult.
Hospital practice is one of the oldest areas of pharmacy practice in Nigeria. It has developed steadily but very slowly over the years and has continued to find it difficult to hold its unique “drug expert” identity. Some hospitals in Nigeria (especially privately owned hospitals) operate without the physical presence of a pharmacist or sometimes use nursing apprentice to “dispense” and “counsel” patients on their medications.
The hospital system in Nigeria is categorized into 3 tiers on the basis of their size, patient carrying capacity, and availability of specialized physicians. The first tier is the primary hospital, which serves a local community or village and has less than a 20-bed carrying capacity. They are sometimes referred to as primary health centers. The secondary hospitals form the second tier and serve a group of communities or local governments and have a bed capacity of between 50 and 100 beds. The highest tier, the tertiary hospitals are the main referral hospital for patient care in Nigeria. Bed spaces often range from 100 to 500 bed spaces and nearly all-available specialists are in these hospitals. Both privately and government-funded hospitals are classified same way. The distribution of hospital pharmacists in each tier or sector is still unknown, and a research grant was recently released to evaluate the geographic and sectoral distribution of pharmacists in Nigeria. 11
In contrast to Nigeria, the OSU practice of clinical pharmacy recently evolved to a higher level of practice through a collaborative practice model with OSU physicians. Clinical pharmacists are now authorized to prescribe medications under an agreement with physicians in the scope of their specialty. 12
Based on the structure of Nigerian pharmacy practice, a vision for enhancing the role of the pharmacist in Nigeria was established. The goal was to establish the pharmacist as a peer to physicians in the Nigerian health care system. This is accomplished by focusing in the area of antimicrobial stewardship and scholarly collaboration. A first step was taken to assist C.U. in understanding the importance of antimicrobial stewardship programs (ASP) in Nigeria. In addition, opportunities were identified to enhance the scholarly collaboration between OSUWMC and the Nigerian health care system.
Antimicrobial Stewardship Opportunities
Antimicrobial stewardship programs (ASP) improve patient outcomes, reduce adverse events, reduce readmission rates, and reduce antibiotic resistance,13,14 and thus a call for their implementation in all hospitals globally is recommended. The full impact of the effectiveness of ASPs can only be achieved if a global perspective is taken. No matter how many positive strides developed economies such as the United States achieve in reducing or controlling the emergence of resistant pathogens, their efforts would be in futility as every “superbug” is only a plane ride away. This was best demonstrated in the 2013-2015 Ebola epidemic. Nigeria was part of this epidemic but was also the one West African country to contain it rapidly.
A common barrier to successful implementation of ASP in resource-limited countries is lack of ID trained physicians and pharmacists. Similar to other resource-limited countries, Nigerian schools of pharmacy do not offer advance training in ID for pharmacists. However, with motivated pharmacists who have leadership skills and an effective mentor, this challenge can be overcome. For example, the OSUWMC ID PharmD serves as a mentor to South African pharmacists in both public and private hospitals across South Africa. The implementation of ASP by nonspecialized pharmacists across 45 South African hospitals led to a significant reduction in mean antibiotic defined daily doses per 100 patient-days. 15 The MWF mentee participated in multidisciplinary patient care rounds with a surgical intensive care unit (SICU) pharmacist and master’s resident in pharmacy to observe how specialized pharmacists contribute to the team and assure appropriate use of antimicrobials. Connecting the mentee with other health care providers who are willing to mentor is important. It helps the mentee build a wide network of trusted mentors who can provide different perspectives of pharmacy practice.
The use of Twitter was also recommended to C.U. as a way to maintain ongoing engagement, education, and global connection with health care providers. At the beginning of the mentoring program, the mentor registered the hashtag #MWF2016 at www.symplur.com to measure the engagement and reach (measured by impressions) of each tweet. Over 960 people who tweeted using the #MWF2016 engaged with each other and sent a total of 2731 tweets that made 19 034 901 impressions. 16 One of the most followed health care providers on Twitter is @bnwomeh an OSU-Nationswide Childrens Hospital surgeon with over 4900 followers. He is Nigerian and has a large Twitter following within Nigeria. The mentee was mentored by this surgeon and connected with him on Twitter to sustain the relationship.
Scholarly Collaboration Opportunities
To have change occur in the profession of pharmacy in Nigeria, the change must come from the thought leaders within the hospitals and Colleges of Pharmacy. Publishing scholarly works is one way to make a global impact on the profession of pharmacy. Creating a culture of cross collaboration between OSU-UNN Faculty of Pharmaceutical Sciences and the Department of Pharmacy extends the mentoring concept beyond the walls of our department. Although a 6-week time line to co-author a paper is challenging, the co-authors of this paper agreed it was important. In addition to this article, the mentee made a 6-minute podcast with photos describing his perspective of the pharmacy-mentoring program. The podcast is posted to the OSU-ASP website that can be viewed at http://rx.osumc.edu/asp2/podcasts/episode8.php.
Lessons Learned
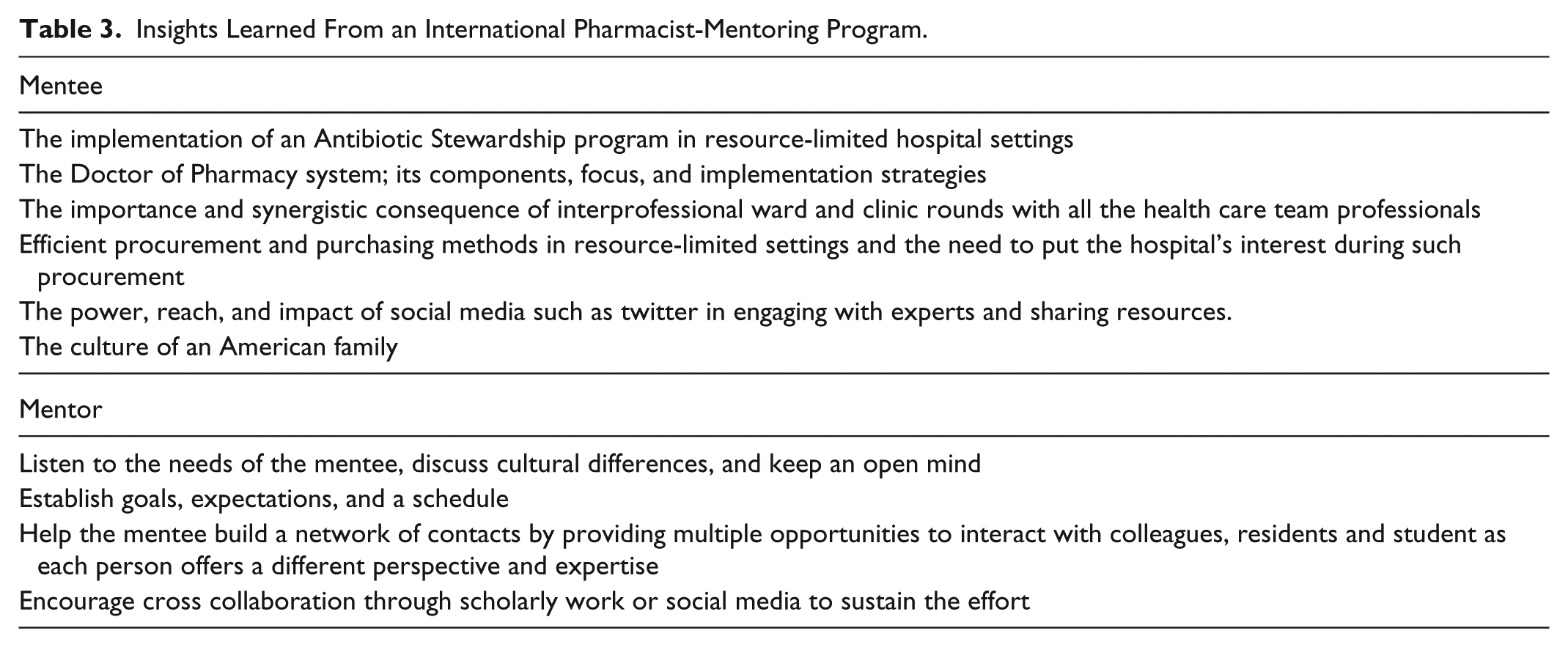
C.U., D.G., and the pharmacy leadership team learned a great deal from participating in the Mandela Fellowship. Table 3 lists the lessons learned from both the perspectives of all participants. As an example, C.U. learned that the training of pharmacists in the United States is done to serve the needs of the patient. There is so much effort toward excellent service provision in areas of patient care and appropriate use of medicines. With the just announced approval of the Doctor of Pharmacy program in Nigeria, the Faculty of Pharmaceutical Sciences at the UNN can be at the forefront of implementing qualitative and deeply thought curriculum which serves that common purpose, the patients. However, to achieve and sustain these newly developing ideas, cross-pollination between faculty members from schools of pharmacy in both countries needs to be fostered.
Insights Learned From an International Pharmacist-Mentoring Program.
While the Federation of International Pharmacy (FIP) at the 2013 congress strived to raise the bar of pharmacy practice across the globe equitably, a realization made during the mentoring program is that the most effective efforts should be geared toward pharmacists themselves first, before an attempt to change the system. Educate, improve, and equip pharmacists from nations with poorer health systems and mentoring them will turn the wheels. C.U. learned this from the collaborative interprofessional hospital rounds at the OSU hospital. The pharmacists were specialists in that field; they were prepared and very much able to contribute meaningfully to patient care. It is one thing to be called a specialist clinical pharmacist and it’s another to make one’s impact felt. The hospital “rounds” was a team of physicians (from attending to residents), pharmacists (specialists to residents), nurses (nurse practitioners to ward nurses), and other health professionals whose expertise was also important. The synergy could be felt and the greater importance of serving the patient first remained paramount all through. They all worked as equals.
In a meeting with the head of pharmacy purchasing and pricing at the OSUWMC, 2 major lesson points stand out. First, “in whose interest are you purchasing medicines, the hospitals’ interest or the manufacturer’s interest?” Purchasing of medicines at OSU is devoid of bias and acceptance of “kickbacks,” and the procurement system is driven by cost-saving effectiveness. As hospitals in the United States are self-funded unlike in Nigeria, which is primarily government funded, there is always a drive to increase savings from drug procurement, which could be redistributed to other sectors of the hospital. This is one key way pharmacists can show their impact in the overall financial operations of a hospital and gain respect from the hospital’s administration. Second, in the drug supply chain of every hospital, someone or some identifiable persons must be accountable for the type, quality, volume, and distributive efficiency of medicines being procured, and efficient systems must be put in place to ensure this accountability. This has helped reduce cases of understocking and overstocking, and the overuse of nonformulary drugs that is evident in tertiary level hospitals in Nigeria. Pharmacists need to take charge in revitalizing the weak efforts of the Pharmacy and Therapeutics Committees in their hospitals and meet regularly (at least once in 2 months) to review new and outdated/ineffective medicines within the hospital’s supply chain. C.U. observed the stages of implementation of the antibiotic stewardship program at the OSU, and thus he can adopt such a mechanism back in hospitals in Nigeria, even though there is paucity of ID-trained specialists or pharmacists. The OSU mentor took C.U. through the different components of the ASP and discussed valid ways of implementing them in view of a system with limited resources. C.U.’s experience with Twitter and its ability to achieve a global impact has connected him with pharmacist specialists, ID physicians, and other health practitioners. Resources and discussions on implementing current guidelines on ID have been mutually shared and have benefited all.
The pharmacy leadership team benefitted greatly from the Mandela Fellowship. First the fellowship provided an in-depth look at health care in an African country—something that none of the leadership team had experience. In addition, it was surprising to see that pharmacy was a very close-knit community—all experiencing the same problems, aspirations, and goals for growth and excellence. Finally, the administrative time spent with the program was minimal—and truly counted on the organizational skills of a few people who helped to coordinate meetings, and schedule project time and observational experiences for C.U.
Conclusions
Major global challenges exist in the profession of pharmacy and pharmacy practice. A possible root cause could be that the current educational structure may not be meeting the needs of a nation’s health care. It is important for pharmacy leaders and schools of pharmacy in the United States to collaborate with the international community to influence and accelerate the growth of their practice model. The experience with Nigeria through the MWF program is one example of how pharmacy leaders can collaborate and establish international ties within health-system pharmacy. As a component of the MWF program, the pharmacy-mentoring program allowed C.U. to experience firsthand the impact pharmacists make on patient care. Many insights were gained from the cross collaboration between C.U. and D.G., and a lifelong professional and personal relationship has also been forged. These types of programs represent leadership opportunities that may not be apparent to most pharmacy directors, but expanding their view to helping international pharmacists expand their practice only strengthens the professional goal of providing patient-centered pharmacy services.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.