
Abstract
Introduction
The publishing of “Will There Be a Pharmacy Leadership Crisis?” an ASHP Foundation Scholar-in-Residence report written by Sara White in 2005, brought to light a widening gap surrounding the future of pharmacy leadership. 1 White cited a significant lack of pharmacy managers and specifically a lack of available training programs for future pharmacy leaders. While many institutions have succeeded in filling this gap with successful and competitive postgraduate administration and management training, disparity remains between those large academic medical centers and their community hospital and health-system counterparts.1,2 According to the ASHP Residency Directory, there are currently only 41 programs that offer a PGY1/PGY2 in pharmacy administration combined with a master’s level degree. Of these programs, only four identify as community hospitals or provide significant administrative experiences as part of a network of community hospitals. In contrast, as of 2013, there were 5724 hospitals in the country and approximately 400 of those were academic medical centers. 3 This brings to light the fact that the majority of pharmacy leadership opportunities will be available in the community hospital setting.
Background
The profession of pharmacy requires transformation due to a combination of increasing complexity of medication regimens and financial constraints, all in an evolving health care landscape. These challenges increase the demand for advanced training and education of existing and future pharmacy management practitioners, specifically in health-system administration and management. 2 A health-system pharmacy administration (HSPA) residency incorporating a master of science (MS) with a specialization in health-system administration is a dependable option for molding the caliber of leaders necessary for long-term health-systems sustainability and viability. Numerous academic medical centers have successfully implemented HSPA programs that have produced qualified, capable, and experienced leaders. These leaders, however, can find their first employment in smaller, more rural hospitals and community health-systems as there is an increasing demand for these hospitals and systems to meet the ever-changing levels of performance efficiency. Data suggest that greater than 50% of all hospitals are now part of a health-system and even more have engaged in a collaborative health network to provide care more efficiently. This coupled with the initiatives to transition to quality-based reimbursement models rather than fee-for-service requires health care leaders who are well trained in the nuances of today’s care environment. 4 This exposes a significant opportunity to expand the scope of education and training programs for the development of pharmacy management practitioners and establish an internal pipeline of well-trained and experienced administrative residents.1,4
Mick Hunt, who served as president of ASHP in 2001, stated that a lack of leadership will hinder our professions’ ability to enhance patient safety, optimize care, and impact our patients. In addition, while the pharmacist shortage declined with a vacancy rate of 8.9% in 2000 to 5% in 2004, a severe shortage of pharmacy managers remained with a vacancy rate increasing from 27% in 2003 to 36% in 2004. 1 If sustainable training programs do not produce pharmacy administrators to fill this gap, these positions will be filled by other health care professionals such as nurses, physicians, or MBA graduates, leaving the administrative team without a pharmacist’s leadership expertise, training, and education.
Purpose
Cone Health is a large community teaching health-system located in Greensboro, North Carolina, supporting approximately 1273 beds across 6 community hospital sites, as well as 71 physician practices and 3 urgent cares. Cone Health, in partnership with academic affiliates, hosts a robust teaching program for student and training physicians, physician assistants, pharmacists, nurse practitioners, and other health care professionals. The pharmacy residency program at Cone Health was established in 1968 and is one of the oldest in the state of North Carolina. Cone Health currently trains 10 PGY1 residents, 5 PGY2 residents, and 2 Combined PGY1/PGY2 residents across its sites annually. Building off this long-established and well-respected legacy of training clinical leaders, Cone Health and its network leadership developed a strong partnership with the UNC Eshelman School of Pharmacy allowing for the establishment of a 2-year journey to implement a combined MS/PGY1/PGY2 HSPA residency.
The purpose and intent of the residency is to establish an educational training program in pharmacy administration that promotes the growth of pharmacists as future leaders of health-system pharmacy and enables the residency graduates to achieve their career goals through the development of necessary skills to best serve in advanced leadership positions throughout health care. Because it is based at a community teaching hospital, the ideal trainee will continue to work in this sector of pharmacy upon graduation, filling a desperate need.
Value to Candidates and Health-Systems
There is significant demonstrable value of developing an HSPA program for both the candidate resident and the health-system. First is the value added through a 2-year residency experience combined with a MS, MPH, or MBA experience. Cone Health partnered with the UNC Eshelman School of Pharmacy to provide a MS in pharmaceutical sciences, making Cone Health the fifth member of the UNC master’s cohort, including administration residents from UNC Medical Center, Duke University Hospital, Wake Forest Baptist Medical Center, and Mission Hospital. 5 This master’s education supplements the residency’s clinical and on-site administrative experiences with in-class leadership and health-system management understanding.
A strong cohort of HSPA residents also allows significant networking opportunities through the master’s education and HSPA resident collaborations. This benefits both the resident, who gets exposure and experience from other institutions, and the health-system which gets visibility into other pharmacy programs and into issues shared by multiple organizations. Health-systems also benefit from HSPA programs as they establish a high-quality pipeline of pharmacy leaders, allowing opportunity to recruit talented pharmacists from around the country and for the development of mutually beneficial relationships between pharmacy residents and health-system leaders. 4
Tools for Implementation
There are multiple facets that require consideration when designing a HSPA program, including efficiently allocating resources. Using students from local pharmacy schools and students on rotation is a fruitful approach. Cone Health enlisted an interested group of third-year student pharmacists at the UNC Eshelman School of Pharmacy enrolled in a pharmacy practice management course to develop a business plan for the new residency program. Guided by Cone Health leadership, the students met with system leadership and outlined the initial building blocks for the development of the residency program, setting the framework to meet accreditation deadlines. A timeline was developed based on the needs of Cone Health and the student pharmacists worked closely with the leadership team throughout the entire semester and beyond to ensure the successful implementation of the project. Table 1 outlines each section addressed in the final business plan and can serve as a toolkit for developing an implementation plan.
HSPA Business Plan Sections.
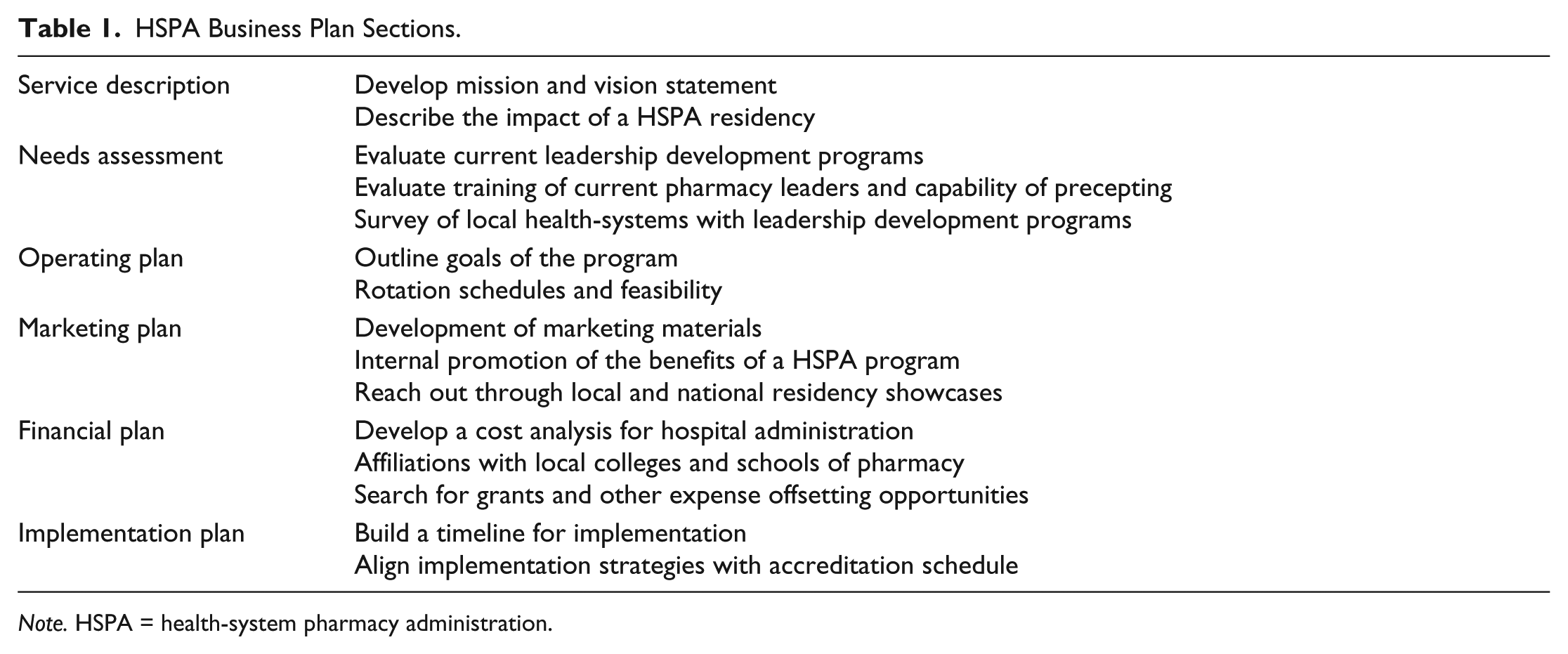
Note. HSPA = health-system pharmacy administration.
Rotation and Preceptor Development
A schedule must be developed for both the PGY1 and PGY2 years. Using the existing backbone of the institution’s PGY1 residency is a common approach and is one that Cone Health chose to follow. This is beneficial as it allows programs to leverage their existing resources and provides residents with a strong clinical background needed to be an effective manager within the pharmacy enterprise. There are many opportunities to enhance a first year administration resident’s experiences to meet their professional goals. Rotations that can be offered in their first year of residency, in addition to clinical acute care and ambulatory care experiences, include medication safety, formulary management, drug information, introductory clinical or operational management experiences, and antimicrobial stewardship. All of these rotation opportunities provide introductory administrative experiences to supplement the didactic master’s education.
Residents will also complete classes longitudinally throughout the first year of residency. Class selection will vary depending on affiliations health-systems have established with respective universities. Cone Health was fortunate to capitalize on a strong relationship with the UNC Eshelman School of Pharmacy to partner and provide a master’s education to their pharmacy administration residents. Classes included in UNC’s MS program cover topics including evaluation research, health-system leadership, overview to health-systems, advanced hospital operations, financial management, human resources, and data analytics. The master’s degree also includes a longitudinal master’s thesis substitute, where the resident completes a project providing demonstrable benefit to the health-system.
The second year of the MS/HSPA residency will involve continued classroom education, rotation experiences, clinical and operational staffing, and a focus on the resident’s master’s thesis substitute project. Cone Health’s HSPA residency is largely focused on a true health-system immersion providing administrative opportunities at all sites within the health-system ambulatory clinics, and accountable care organization.
It is important to maintain transparency and gather input from the pharmacy leadership team across the health-system early on in the development of the program. Cone Health incorporates its PGY2 administration resident in the manager on-call schedule and provides the resident with direct ownership of a health-system service line where he or she serves as a manager to departmental full-time equivalents. This provides real-world leadership experience under the supervision and mentoring of a well-seasoned pharmacy administrator.
Assessing and recruiting preceptors for the program is imperative when justifying a HSPA program and should be incorporated in the initial prescreening planning steps for the development of a HSPA residency. Outside of the clinical preceptors, an evaluation of the institution’s pharmacy leaders and their capacity to provide rotation experiences to HSPA residents is important when considering program accreditation. While having a previously trained manager in a HSPA program is beneficial, having a diverse leadership team with different experiences and educational backgrounds with the capacity to host an administrative resident is most essential to meet the needs of residents.
Marketing
During the 2016 American Society of Health-System Pharmacists (ASHP) Residency Matching Program, approximately 31% of potential applicants did not successfully match to a program of their choice across all residency programs. 6 There are currently 41 PGY1/PGY2 HSPA residency programs combined with a master’s degree nationwide with over 50 total positions available. This is in comparison to general PGY1 programs, which have greater than 1000 programs nationwide. 7 This leaves ample room for the addition of combined MS/PGY1/PGY2 HSPA residency programs as there is both a need for pharmacy leaders as well as an interest among potential applicants. The limited number of available HSPA residency programs provides incentive to capitalize on this unmet need and foster the growth of pharmacy leaders.
A vital component of the program’s success involves attracting competitive applicants with an interest in pharmacy administration and receiving support from within the organization. Verbal marketing is one of the primary ways in which programs can be promoted to future residents. An ideal place to begin this is with local schools of pharmacy and students that have rotation experiences within your health-system. Furthermore, digital marketing should be used via websites or social media to provide constant and easily accessible resources detailing the residency program. Positive promotion techniques highlighting the need to cultivate the next level of leadership in the community hospital setting and establishing an internal pipeline of administrative residents within the Cone health-system were crucial to the initial recruitment effort. For recruitment and marketing efforts, the Cone Health residency website was revamped to highlight the addition of the new program, as well as the success of existing residency programs within the health-system.
Attendance at residency showcases sponsored by local and state pharmacy organizations as well as national meetings such as the ASHP Midyear Clinical Meeting and Exhibition are typically required for recruitment success. For potential applicants in the initial stages of researching residency programs, information regarding the combined MS/PGY1/PGY2 HSPA residency can be found on the ASHP Online Residency Directory. As a preliminary research tool, this directory provides basic information including contact information and special attributes of each residency program. By applying for precandidate status, the HSPA programs will automatically be included in the ASHP Directory.
Financial
Residents require a substantial yearly investment from the health-system including a stipend-based salary, benefits, educational fees, travel expenses, and research costs. Additional training expenses and accreditation fees must also be considered when implementing a new residency program. 8 The costs associated with implementing a HSPA residency will ideally be offset by the cost avoidance to the health-system by growing your residency program. 9
Several studies suggest that the cost savings from pharmacy residency programs effectively offsets the implementation cost with a return on investment (ROI) of up to 100% in some cases.8,9 HSPA residents may have potential for the highest ROI compared with other residents due to a guaranteed 2 years of employment as well as involvement in health-system-wide administrative projects. In addition to staffing, residents help offset their expenses through health-system improvement projects, involvement with the leadership team, and executing medication cost-saving programs and projects. Grants for adding a residency program, paying educational expenses, and supporting resident’s research can also be considered and help health-systems finance resident positions. The federal government plays an important role in offsetting implementation costs as well, as Medicare reimburses residency programs proportionally to the percentage of Medicare patients served by the health-system through Medicare pass-through funds in their PGY1 residency year. 8
During its infancy, programs require substantial funds to sustain the combined MS/PGY1/PGY2 HSPA residency program. It is estimated, for Cone Health’s program, that the investment for one resident per year is approximately $130 000 due to stipend, travel budget, master’s education, and preceptor time. This is in contrast to the cost avoidance which comes due to Medicare pass-through funding in the PGY1 year, staffing, cost reduction projects, and precepting to pharmacy students which estimates to approximately $170 000 cost savings per year. After 2 years, the projected ROI of Cone Health’s program is approximately $30 232, which is desirable of a residency program and attractive to the administrative personnel within the health-system.8,9 A breakdown of these figures is provided in Table 2.
Sample Financial Itemization of MS/PGY1/PGY2 HSPA Residency.
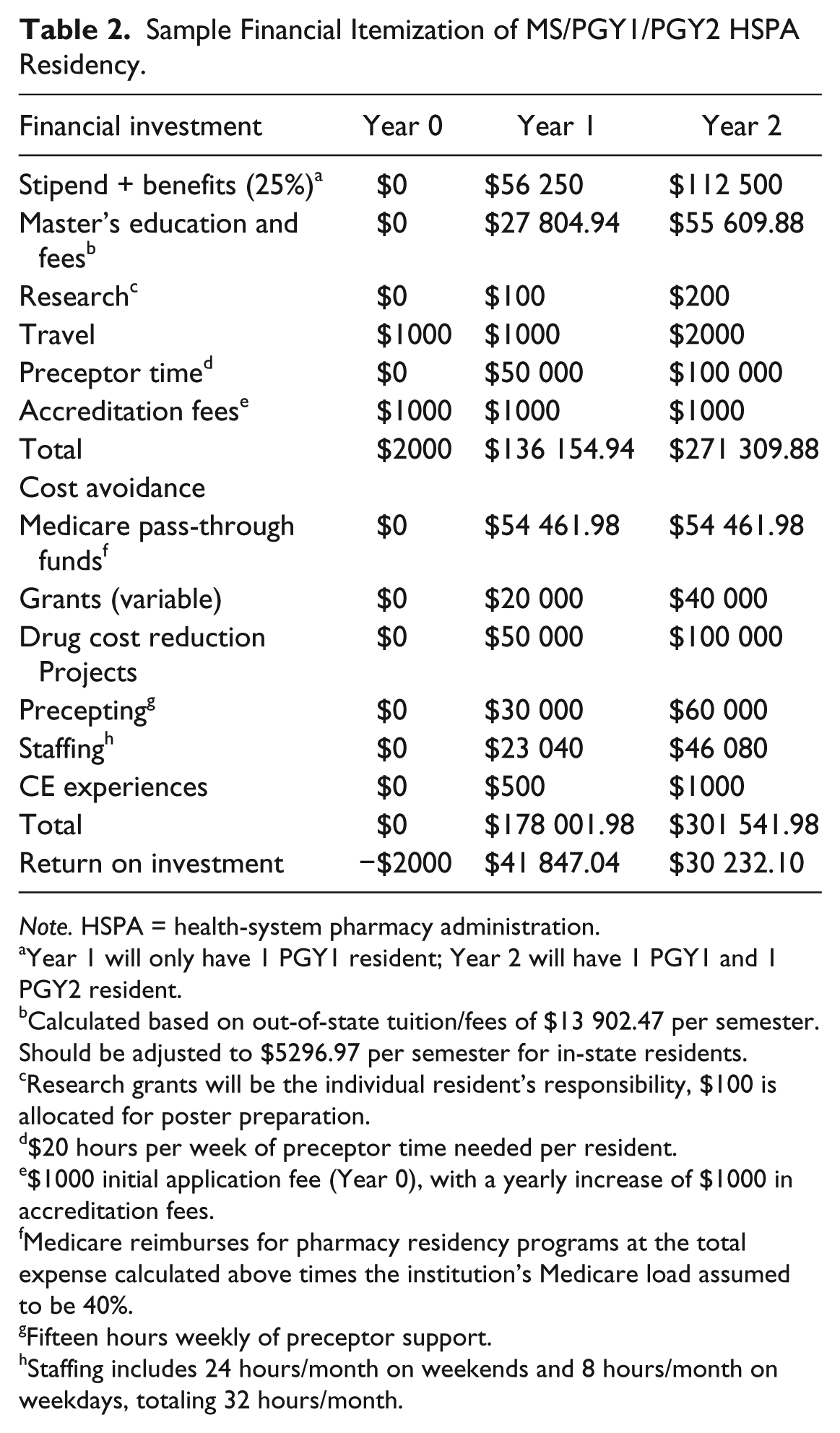
Note. HSPA = health-system pharmacy administration.
Year 1 will only have 1 PGY1 resident; Year 2 will have 1 PGY1 and 1 PGY2 resident.
Calculated based on out-of-state tuition/fees of $13 902.47 per semester. Should be adjusted to $5296.97 per semester for in-state residents.
Research grants will be the individual resident’s responsibility, $100 is allocated for poster preparation.
$20 hours per week of preceptor time needed per resident.
$1000 initial application fee (Year 0), with a yearly increase of $1000 in accreditation fees.
Medicare reimburses for pharmacy residency programs at the total expense calculated above times the institution’s Medicare load assumed to be 40%.
Fifteen hours weekly of preceptor support.
Staffing includes 24 hours/month on weekends and 8 hours/month on weekdays, totaling 32 hours/month.
Accreditation
After the commitment of the first resident to a newly established MS/PGY1/PGY2 HSPA residency, programs will need to receive accreditation from the ASHP Commission on Credentialing. The ASHP Commission on Credentialing is the sole nationally recognized nongovernmental, nonprofit pharmacy residency accrediting board in the United States. Since 1962, ASHP has set the standards that each residency program must attain and uphold.10,11
It is critical to review accreditation resources provided by ASHP, including their accreditation “Frequently Asked Questions” document, as well as the goals and competencies outlined for a PGY2 in Health-System Administration. These goals and competencies should be reviewed well before the first HSPA candidate begins the program and instilled in the development of rotations, longitudinal requirements, and marketing.10,11
Conclusion
A HSPA/MS residency has become a vital program in health-systems to create a sustainable pipeline of innovative leaders, as well as to progress pharmacy practice at the respective educational sites. While HSPA programs have been well established at academic medical centers, there is demonstrable benefit of these programs at large community health-systems. HSPA residents provide the opportunity to build a pipeline of high-quality leaders, provide high-level project involvement, and produce a positive ROI to benefit the health-system and its patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.