
Abstract
Introduction
Cataracts are the leading cause of blindness and vision loss in the United States, with more than 20 million Americans over the age of 40 years affected with this condition. 1 Currently, approximately 60% of Medicare vision spending is due to cataract surgery. 1 It is estimated that the patient population needing cataract surgery will increase to 30 million by 2020, a near 50% increase.1,2 Cataract surgery is a significant risk factor for endophthalmitis, a serious ocular infection. Although rates of endophthalmitis are relatively low in the United States and Europe (0.40-2.65 per 1000 persons), this infection often leads to irreversible vision loss. 2
The use of intraoperative intracameral (IC), an injection into the eye cavity, moxifloxacin for the prevention of endophthalmitis after cataract surgery has been endorsed for over a decade. The European Society of Cataract & Refractive Surgeon’s (ESCRS) 2007 study on cataract antibiotic prophylaxis reported a 5-fold increased risk of postoperative endophthalmitis (POE) for those who did not receive IC cefuroxime. 3 There is ample evidence to support the safety and efficacy of IC moxifloxacin, but the literature lacks an adequate description of IC injection preparation.3-11 The widespread and increasing frequency of cataract surgery, in conjunction with the prevalent use of IC antibiotics for the avoidance of POE, has strengthened the importance for health care systems to identify the most appropriate and cost-effective preparation of IC antibiotics.
The Aurora Pharmacy Packaging Center (APPC) is a 503A compounding pharmacy within Aurora Health Care that repackages bulk pharmaceuticals into unit doses for distribution within the health care system. The sterile repackaging is done at Aurora St. Luke’s Medical Center of Aurora Health Care Metro, Inc. The APPC began the centralized compounding of IC moxifloxacin in February 2016 per the request of physicians, due to the increased demand of IC injections and the need for sterile preparation of the product. Reasons to support this practice included limiting the on-site preparation of IC injections and prohibiting between-room transfer of stock antibiotic eye drops for infection control purposes. The APPC procedure involves simple manipulation of the commercially available product into 1-mL syringes, documentation of equipment/products used, and appropriate labeling and storage. The APPC has implemented a compounding procedure outlining their process (Figures 1-3).
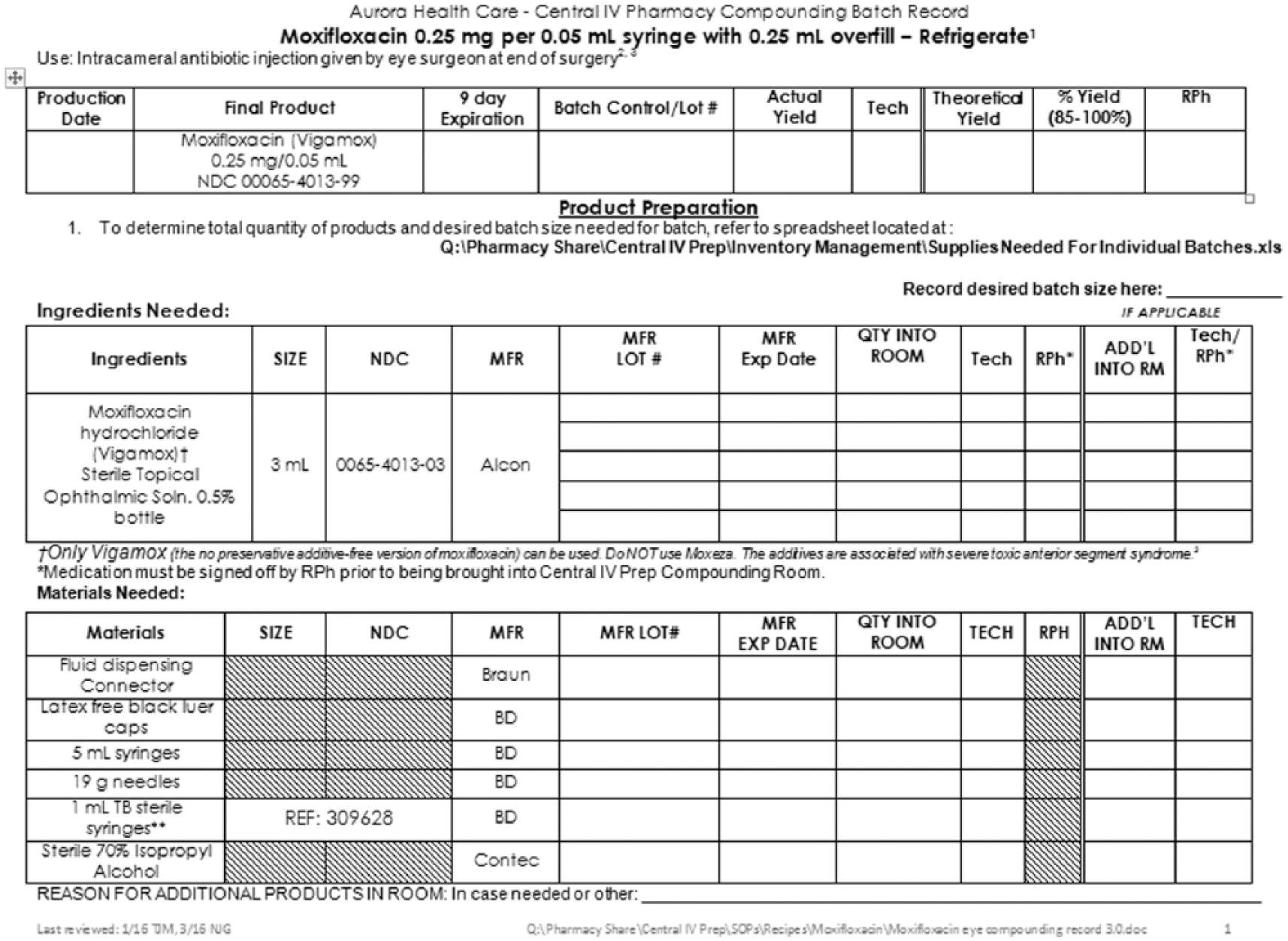
Aurora Pharmacy Packaging Center compounding procedure for intracameral moxifloxacin preparation.
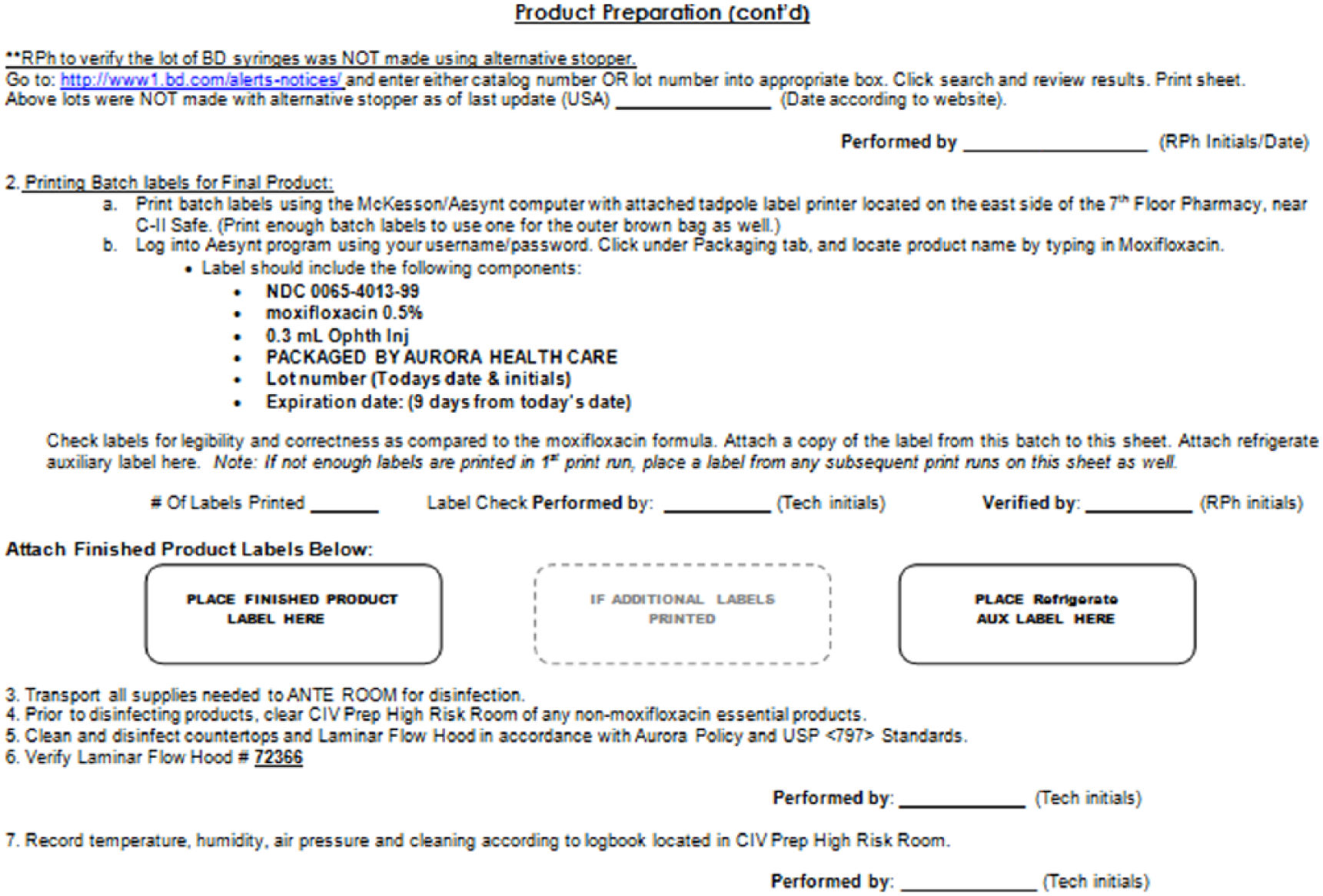
Aurora Pharmacy Packaging Center compounding procedure for intracameral moxifloxacin preparation continued.
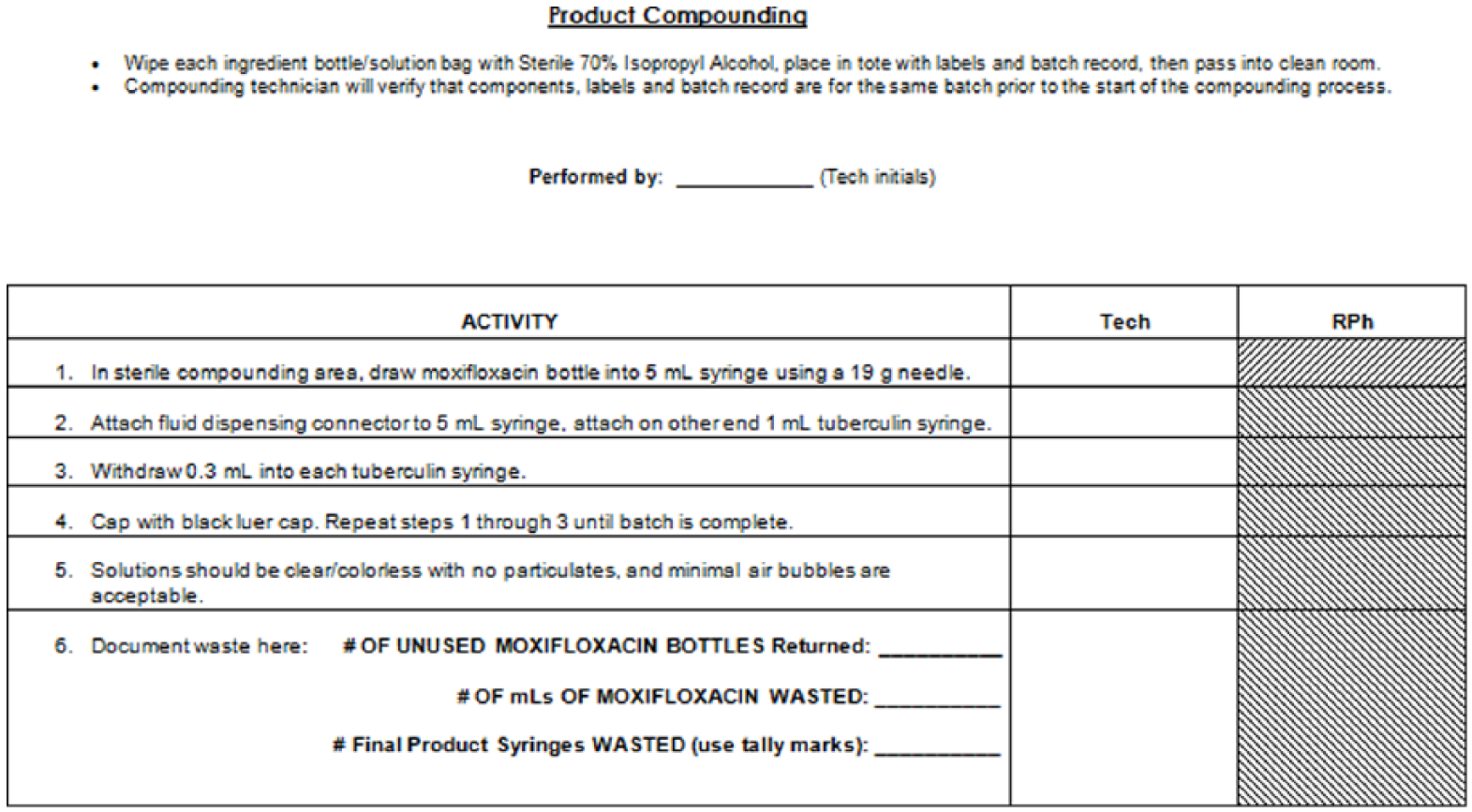
Aurora Pharmacy Packaging Center compounding procedure for intracameral moxifloxacin preparation continued.
To our knowledge, there are few published descriptions detailing the preparation of IC moxifloxacin.4,6 Articles reviewed by this evaluation do not correlate the direct financial benefit of such practice.4-11 This financial evaluation was developed to describe the centralized repackaging of IC moxifloxacin in compliance with the United States Pharmacopeia (USP) 797 standards, 12 and to identify the impact on product cost savings.
Methods
Evaluation of Production Quality
The APPC’s centralized compounding procedure of IC moxifloxacin was evaluated using USP 797 standards and compared with evidence-based literature. A systematic literature search using OvidSP and Ovid Medline platforms was used to identify evidence-based literature (limited to publications in English from after the year 2000, with the following primary search terms: intracameral, moxifloxacin, antibiotics, endophthalmitis, safety, efficacy, and cataract). Articles were chosen based on relevance, date of publication, and outcomes. USP 797 criteria were also reviewed and summarized. The final criteria for evaluation are described in Table 1. Pharmacy leadership within the hospital and APPC reviewed the evaluation criteria with respect to the centralized compounding practice, and the procedure was deemed compliant with USP 797 standards per expert consensus.
Evaluation of Aurora Pharmacy Packaging Center Compounding Procedure With USP 797 Standard Criteria. 12
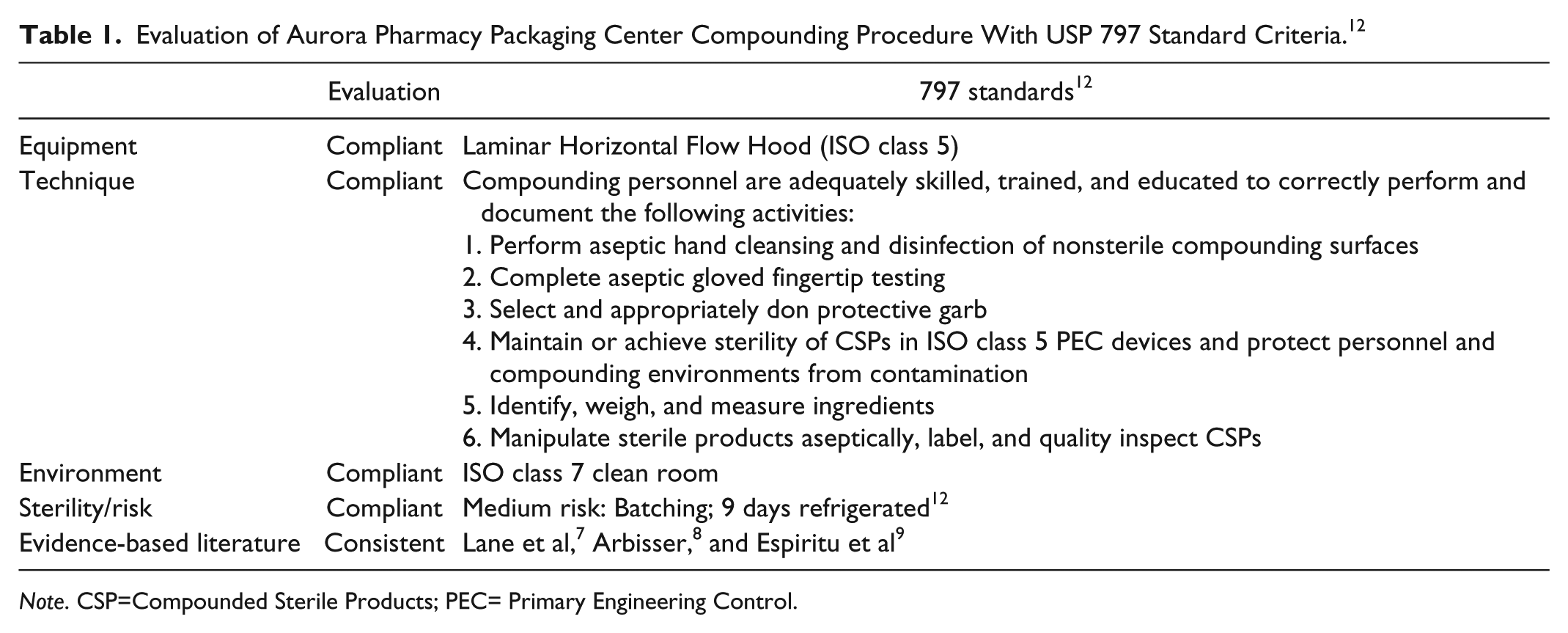
Note. CSP=Compounded Sterile Products; PEC= Primary Engineering Control.
Cost Savings
Patients who received IC moxifloxacin intraoperatively from one of 3 ophthalmologists during cataract surgery between February 15, 2016, and August 15, 2016, were identified using data from the APPC. Standard procedure involved running weekly reports through EPIC health care software to determine the anticipated number of cataract surgery cases per week and then compounding the corresponding number of syringes. The number of cases per physician and number of syringes dispensed weekly were recorded in a production log. After the study period, cost savings were calculated by reviewing costs associated with drug supplies. Descriptive statistics were calculated.
Results
Evaluation of Production Quality
The APPC’s current process was validated as compliant with USP 797’s sterile compounding standards. USP 797 validation criteria included proper sterile technique, equipment, room sterility and pressure, beyond use dating, and storage. 12 Sterile technique by technicians was supported by aseptic technique training, media fill testing, and gloved fingertip testing. These results are documented and stored via templated production logs (Figures 1-3). The potency and purity of the product under refrigerated conditions over the specified time frame (9 days) were determined by high-performance liquid chromatography (HPLC) by an independent laboratory. All samples were within the USP-specified range for moxifloxacin ophthalmic solution.
Cost Savings
Prior to centralized production, a vial of moxifloxacin was dispensed for each surgery at a direct cost of $140/surgery. After implementing centralized production, a vial of moxifloxacin produced 9 IC injections and therefore reduced the direct cost to $20/surgery. Direct cost savings to the organization was $120/surgery. There were 459 surgeries during the study period, resulting in a savings of over $55 000 over 6 months and a projected annual savings of over $100 000 for the health system.
Discussion
Implications
This study described the magnitude of a small operational change, and how it can save an organization a substantial amount of money while maintaining quality. The implementation of the usage of centralized IC moxifloxacin syringes during cataract surgery will save this organization over $100 000 dollars over its first year. As more ophthalmologists accept this practice, there will be a greater demand for its production, and further savings. This study will help support the transition to the centralized production of IC moxifloxacin by providing evidence on continued quality and adherence to best practices through centralized production, with an added cost savings advantage.
Future research could evaluate the financial benefit of the centralized production of additional IC antibiotics for ocular surgery. Moxifloxacin was an appropriate first choice for investigation as it has clinical advantages which may outweigh the cost savings with using alternative antibiotics. These advantages include a broader spectrum of antibacterial activity against common ocular pathogens, compatibility with intraocular tissues, its preservative-free formulation, and commercially available status reducing the complexity of compounding.6,7,13
Limitations
This study was limited by its short duration of 6 months. With a longer study duration, there would have been no need to estimate potential cost savings. Despite this limitation, the consistency of the production and documentation practices supports the extrapolation of reported data. In addition, the cost savings were calculated based solely on direct costs, not considering production time and labor costs. Finally, although the use of IC moxifloxacin has been established and supported in the evidence-based literature, it should be noted that the use of moxifloxacin as an IC injection is off-label.
Footnotes
Acknowledgements
The authors acknowledge the practitioners who developed the process and made substantial contributions to this project, including Tracy Mathia, PharmD, BCPS; Stacy Wucherer, RPh; and Amber Johnson.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.