
Abstract
Background
Alcohol abuse is associated with up to 40% of all intensive care unit (ICU) admissions, and an estimated 0.5% of ICU patients exhibit alcohol withdrawal.1,2 Guidelines for the assessment and management of alcohol withdrawal are outdated. 3 Thus, many institutions generate their own protocols to assess and treat alcohol withdrawal syndrome, resulting in many practice variations that could influence patient care and outcomes.
Benzodiazepines are frequently used to prevent or treat alcohol withdrawal as their mechanism of action overlaps with alcohol and reestablishes the gamma-aminobutyric acid (GABA)–mediated neurogenic inhibition that occurs when alcohol is no longer present. These agents reduce mortality and decrease symptoms but are associated with adverse events, such as respiratory suppression and mechanical ventilation, secondary to oversedation. To reduce the likelihood of these adverse events, benzodiazepines should be administered using a protocol-guided, symptom-triggered dosage regimen that directs as-needed doses based on the severity of withdrawal as assessed with a validated scoring tool.4,5 Even with theguidance of a protocol, the dosing of benzodiazepines is challenging for the clinician as it is a delicate balance between controlling the manifestations of withdrawal without inducing benzodiazepine-associated excess sedation. Moreover, critically ill patients frequently require higher than normal doses of benzodiazepines to treat alcohol withdrawal, up to 100-fold in some patients but the amount is unpredictable. 2 These high doses increase the likelihood of respiratory failure, encephalopathy, and other benzodiazepine-related side effects, particularly in patients who frequently have underlying liver disease. Other GABA-modulating agents such as barbiturates and propofol have not been widely studied but are often used to treat symptoms refractory to benzodiazepines.5,6 Unfortunately, they possess similar adverse event profiles.
Other adjunctive therapies may be used to control symptoms while minimizing sedation and respiratory suppression. Neuroleptic agents may help control psychosis but have little benefit beyond this manifestation. Prospective studies have shown alpha-2 agonists (clonidine and dexmedetomidine) reduce benzodiazepine administration while maintaining similar symptoms and severity of withdrawal.7-10 Glutamate-activated N-methyl-
While these agents may be used to treat acute alcohol withdrawal, the manner in which they are used remains ambiguous. This is particularly concerning given the lack of data supporting their utilization. The goal of this survey was to describe the practices in both assessing and treating acute alcohol withdrawal, including the parameters that direct the use of these agents, at institutions across the United States.
Methods
Survey Design and Development
The structured questionnaire (see online appendix) was a cross-sectional survey created within Qualtrics software (Provo, Utah). The survey consisted of 6 components: participant consent, characterization of the institution and the responding pharmacist, the manner in which the severity of acute alcohol withdrawal is assessed, the initial management of acute alcohol withdrawal, adjunctive management of acute alcohol withdrawal, and the perceived barriers to use of these agents to manage acute alcohol withdrawal. The survey was designed to assess practice patterns and perceptions of specific therapies using categorical and 9-point Likert response scales. Participant or institution identifiers were not collected. Responses were anonymously compiled and stored electronically. The survey was pretested by 2 sets of 10 ICU pharmacists and was altered based on their responses. Each question was revised through an iterative process consisting of sequential testing of each revised question with the complementary set of ICU pharmacists. Reliability was ensured through a process of test-retest of the pretest groups until responses were consistent. The protocol was approved by the Colorado Multiple Institutional Review Board with consent implied when the survey was completed and submitted.
Participants
Approximately 1500 eligible participants were hand selected from the American College of Clinical Pharmacy Critical Care Practice and Research Network, the Society of Critical Care Medicine Clinical Pharmacy and Pharmacology Section, and the American Society of Health-System Pharmacists Critical Care Residency Directory. Only 1 pharmacist per institution was selected. Of the 1500 preselected pharmacists, 500 were randomly chosen to receive a standardized e-mail with the survey available as an embedded link. The original e-mail was distributed September 12, 2016, and a reminder e-mail was sent 6 weeks after the initial invitation.
Statistical Analyses
The survey was distributed to 500 participants in an effort to ensure 335 usable surveys which would provide a margin of error of 5% around a 95% confidence interval assuming a population size of 3000 possible pharmacists. Responses were not weighted, and missing data were not imputed. For questions utilizing a 9-point Likert scale, responses were rated so that scores of 7 to 9 represented agreement, 4 to 6 represented no consensus, and 1 to 3 represented disagreement. Frequency, mean, median, standard deviation, and interquartile ranges (IQRs) were determined for continuous data. Univariate analyses were performed using the chi-squared test for proportional data and Mann-Whitney U test for continuous data. The Wilcoxon signed rank test was used to compare medians for the level of agreement of respondents with various statements. Responses were transposed electronically into an Excel database. Data analyses were performed using JMP Pro statistical analysis software, v.10.0.2 (SAS Institute Inc, Cary, North Carolina). A 2-sided P value < .05 was considered significant.
Results
Survey Population
From the 500 preselected pharmacists, 29 were removed from the sample because the original e-mail was returned as nondeliverable. Of the 471 eligible recipients, 94 (20%) pharmacists completed the survey (Table 1), which provided an adjusted margin of error of 9.9%.
Respondent and Institutional Characteristics, N = 94.
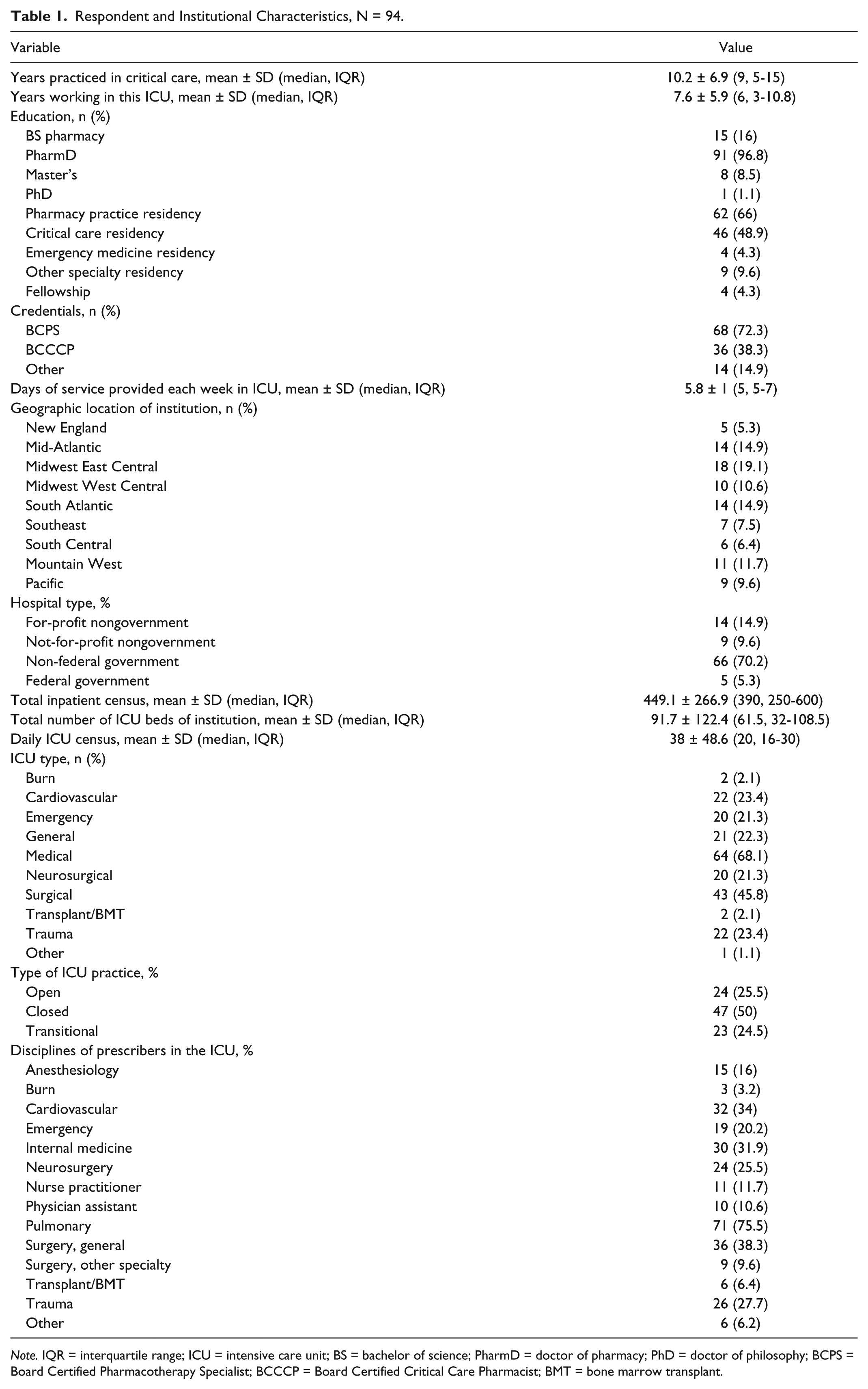
Note. IQR = interquartile range; ICU = intensive care unit; BS = bachelor of science; PharmD = doctor of pharmacy; PhD = doctor of philosophy; BCPS = Board Certified Pharmacotherapy Specialist; BCCCP = Board Certified Critical Care Pharmacist; BMT = bone marrow transplant.
Assessment of Severity of Alcohol Withdrawal
The Clinical Institute Withdrawal Assessment for Alcohol (CIWA) was the most commonly used assessment tool (Table 2). Only 43 (45.8%) respondents rated scoring tools as highly effective (score of ≥7 on a Likert scoring range of 1-9) for assessing the severity of acute alcohol withdrawal. An alcohol withdrawal protocol existed in 86 (90.5%) ICUs surveyed. Respondents indicated that protocols are used often or routinely 72.3% of the time for initial management but only 24.5% for adjunctive medications (P < .0001). In patients not requiring admission to the ICU, often or routine use of a protocol was 62.8%. Fifty-four respondents (57.5%) rated protocols as highly effective, with an average score of 6.7 ± 1.3 on a scale of 1 to 9. Greater than 98% of respondents agreed that inconsolable agitation; confusion with or without orientation to one of person, place, or date; hallucinations; seizures; and tachycardia were common manifestations of acute alcohol withdrawal (Table 3). Respondents indicated that severe manifestations of alcohol withdrawal were seizures; confusion without orientation to person, place, and date; delusions; diastolic blood pressure > 110 mm Hg; inconsolable agitation; and tachycardia (Table 3).
Scoring Rubrics/Tools Used to Assess the Severity of Acute Alcohol Withdrawal in the ICU, N = 94.

Note. ICU = intensive care unit; CIWA = Clinical Institute Withdrawal Assessment; MINDS = Minnesota Detoxification Scale; SEWS = Severity of Ethanol Withdrawal Scale.
Richmond Agitation Sedation Scale was most common “other” rubric and often used for patients if intubated.
Perceptions of Symptom Severity by Respondents, N = 94.
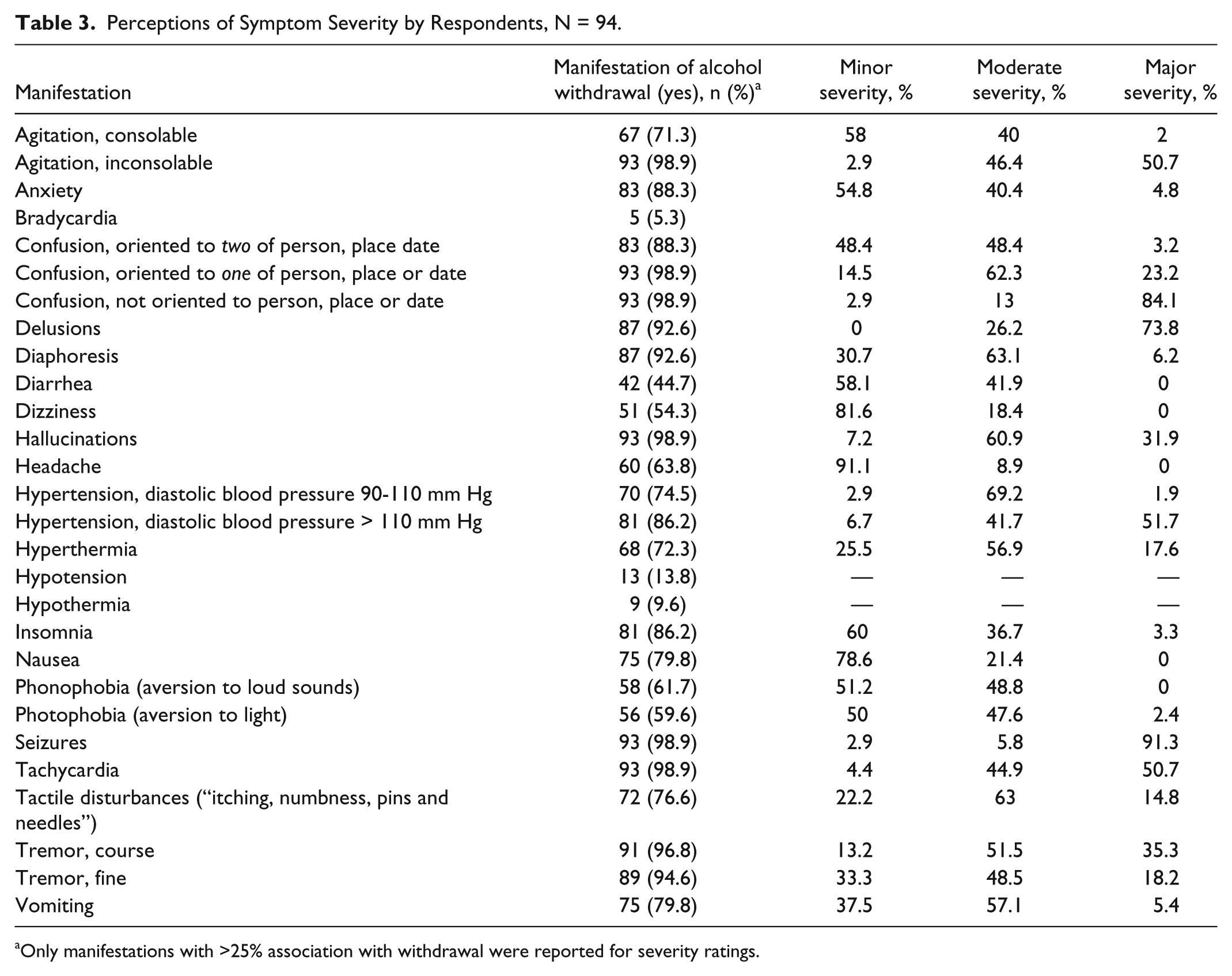
Only manifestations with >25% association with withdrawal were reported for severity ratings.
Management of Acute Alcohol Withdrawal
Protocol options: Initial and adjunctive agent use
Agents employed for initial and adjunctive management (Table 4) were benzodiazepines (92.6% and 61.7%, respectively, P < .0001), clonidine (29.8% and 34%, respectively), haloperidol (26.6% and 33%, respectively), and barbiturates (20.2% and 24.5%, respectively). Of GABA receptor modulators, intravenous lorazepam was preferred as initial therapy (Table 5). Forty-eight (51.1%) respondents indicated that GABA receptor modulators were front-loaded. Adjunctive agents were most commonly added to reduce dosage regimens of benzodiazepines (antipsychotics, barbiturates, alpha-2 agonists), prevent respiratory depression (alpha-2 agonists), prevent or treat autonomic symptoms (alpha-2 agonists), and prevent or treat agitation/delusions (antipsychotics, barbiturates, alpha-2 agonists). Overall, baclofen, intravenous ethanol, and enteral ethanol were the least likely to be used (<2% of respondents indicated these agents were highly frequently used).
Agents Included in the Protocol and Perceived Frequency of Use as Initial or Adjunctive Therapies, N = 94.
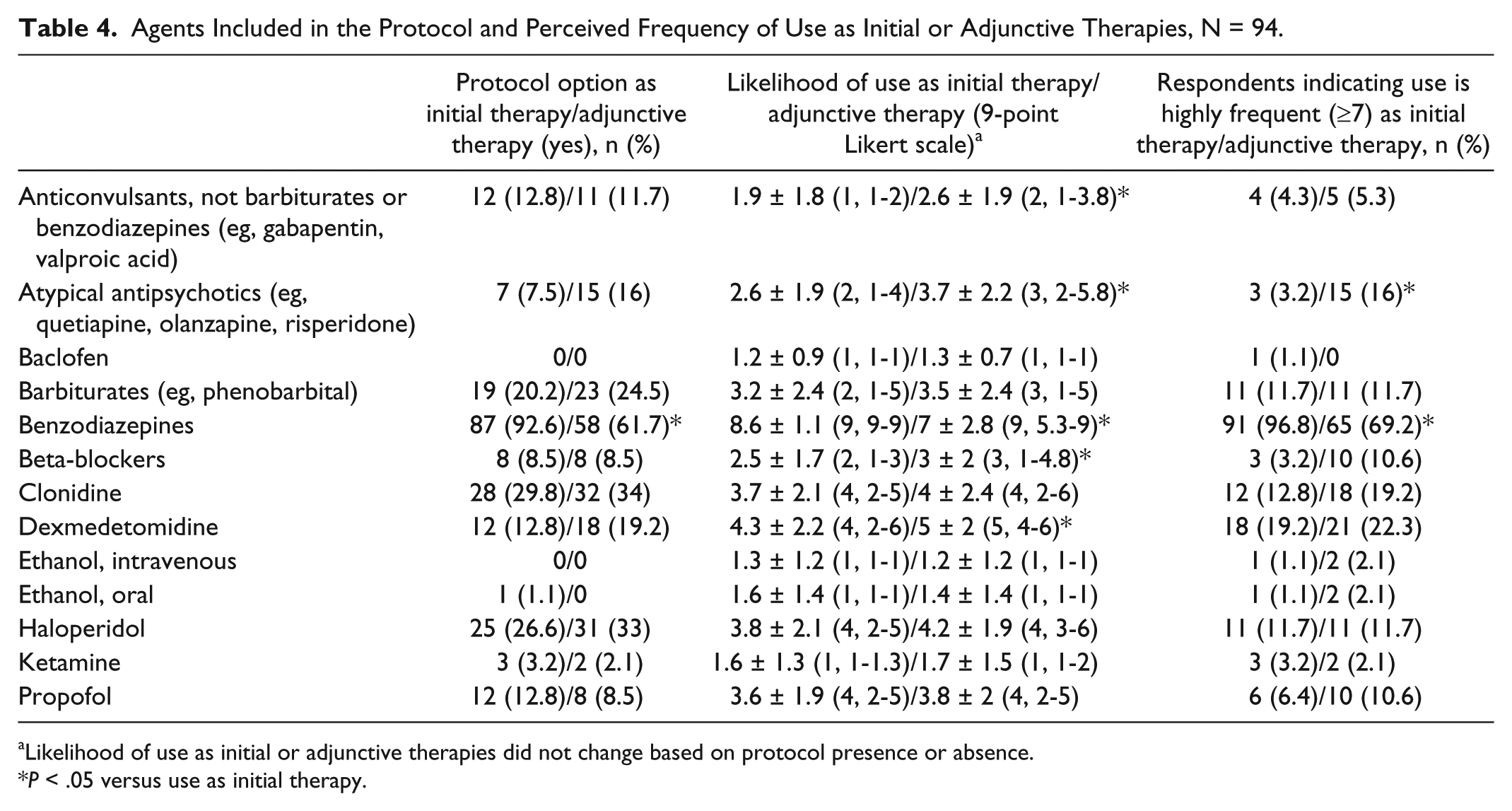
Likelihood of use as initial or adjunctive therapies did not change based on protocol presence or absence.
P < .05 versus use as initial therapy.
Gamma-Aminobutyric Acid Modulators for Initial Therapy of Alcohol Withdrawal, N = 94.
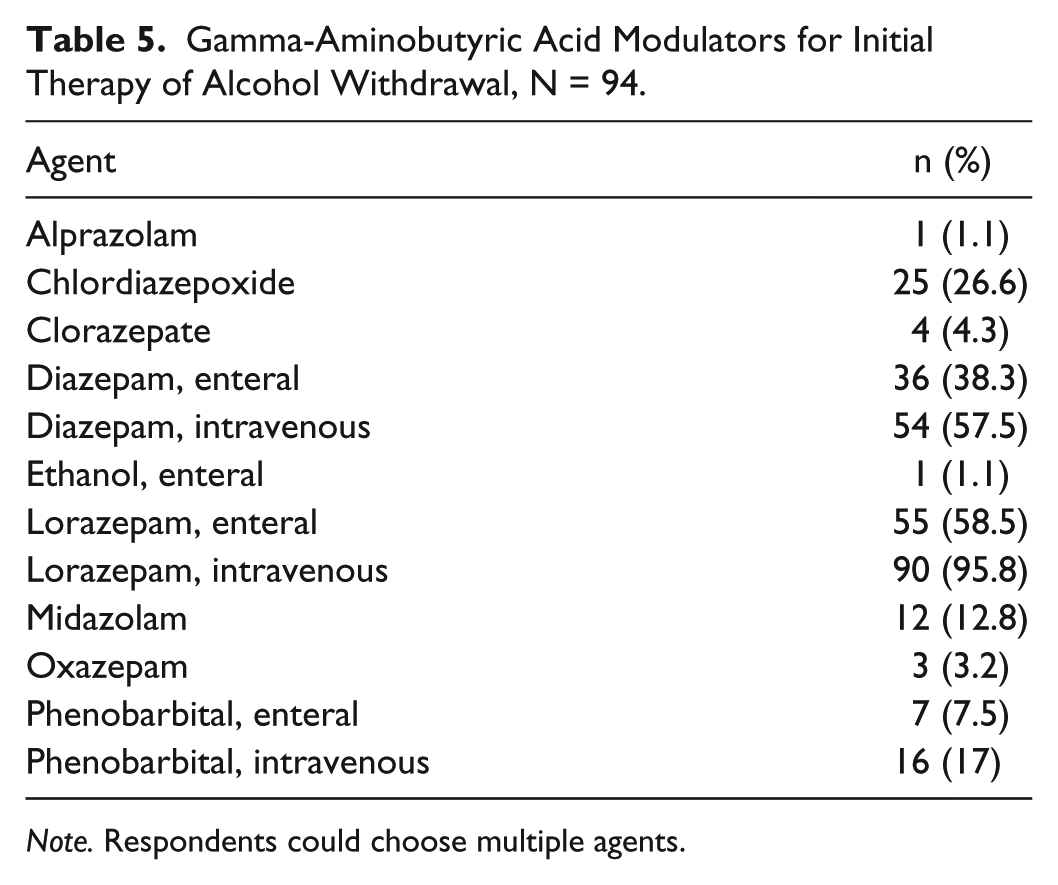
Note. Respondents could choose multiple agents.
Adjusting therapies
Respondents indicated that bedside nursing staff modified the initial regimen using a scoring tool (37.2%), or as instructed by prescribers based on their clinical judgment (29.8%). This is significantly different than modification of adjunctive regimens. Seventy respondents (74.5%) reported modification of adjunctive therapies by the prescriber based on their clinical judgment (P < .0001 vs initial therapy modification) and only 8.1% reported that bedside nursing staff modified adjunctive regimens (P < .0005 vs initial therapy modification).
Roles in therapy
Respondents were asked to agree or disagree with the statements presented in Table 6 for each agent. Numerically, it was more frequent for agents to be used for treatment of symptoms of alcohol withdrawal rather than prevention, but this did not reach statistical significance. Atypical antipsychotics, baclofen, beta-blockers, clonidine, dexmedetomidine, and haloperidol were all found to be significantly more likely to be utilized for prevention of central nervous system (CNS) depression related to GABA receptor modulator use over treatment once CNS depression occurred. Dexmedetomidine and anticonvulsants were both more likely to be used to reduce, rather than to prevent, the high or frequent doses of GABA receptor modulators. The only category not found to have significance between prevention or treatment were tremors. For both prevention and treatment of tremors, benzodiazepines were the agents of choice. Respondents agreed that atypical antipsychotics, clonidine, dexmedetomidine, haloperidol, ketamine, and propofol were more likely to be used to treat anxiety or agitation rather than for the prevention of these symptoms.
Respondents Agreeing With the Statement as Reason for Use of Each Agent, N = 94.
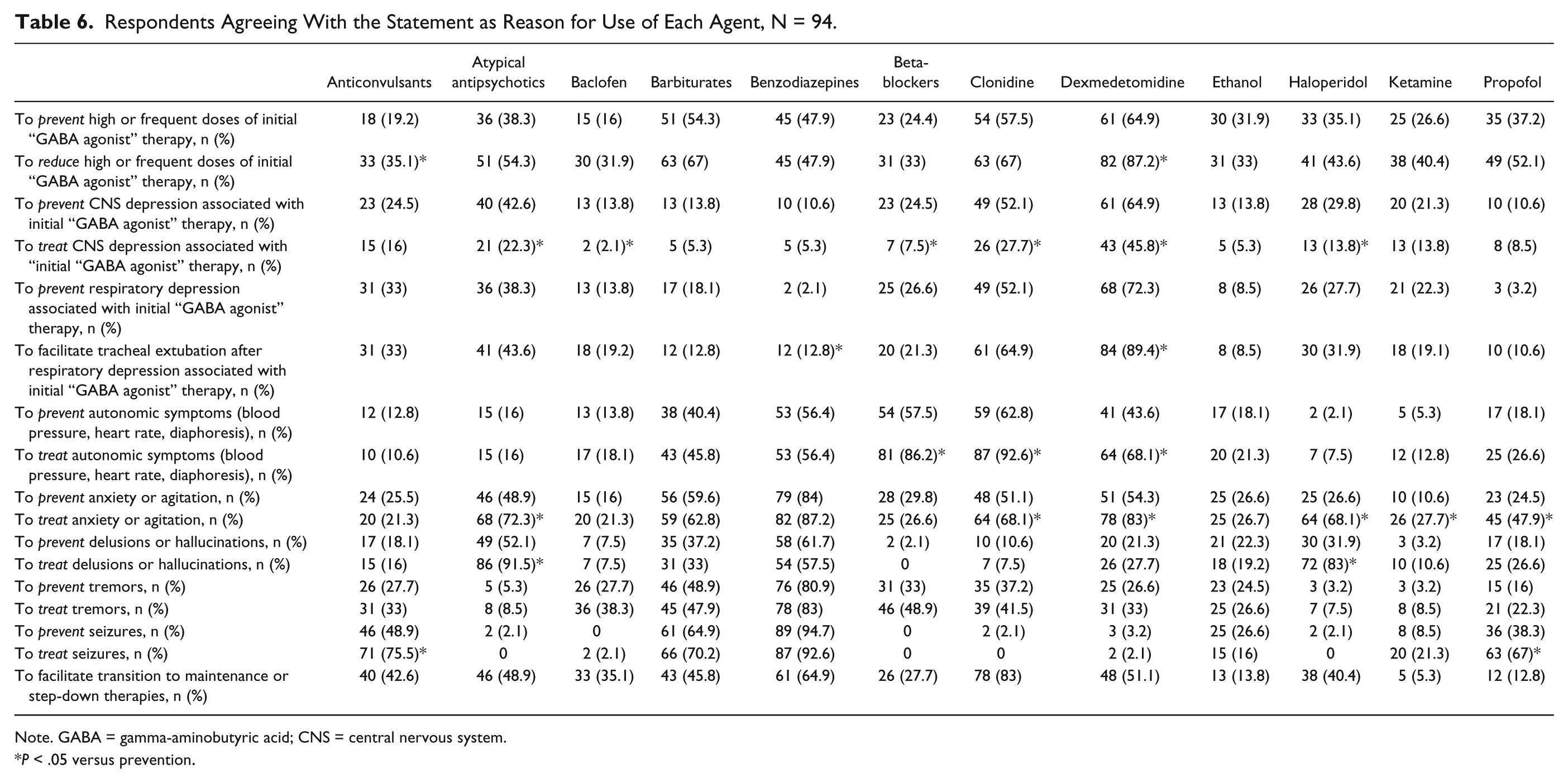
Note. GABA = gamma-aminobutyric acid; CNS = central nervous system.
P < .05 versus prevention.
Barriers to use
Respondents indicated the agents with the greatest barriers to use were dexmedetomidine, propofol, ethanol, ketamine, and baclofen (Table 7). Barriers to use of dexmedetomidine were increased drug cost (57.5%) and the side effects of bradycardia and hypotension. Respondents were most concerned for the need for mechanical ventilation with propofol. Perceived barriers for the use of ethanol included associated administration issues and the need for staff education. Increased education of staff was also evident for ketamine. Lack of beneficial effect was a perceived barrier for the use of baclofen.
Perceived Barriers to Use of Agents for Alcohol Withdrawal, N = 94.
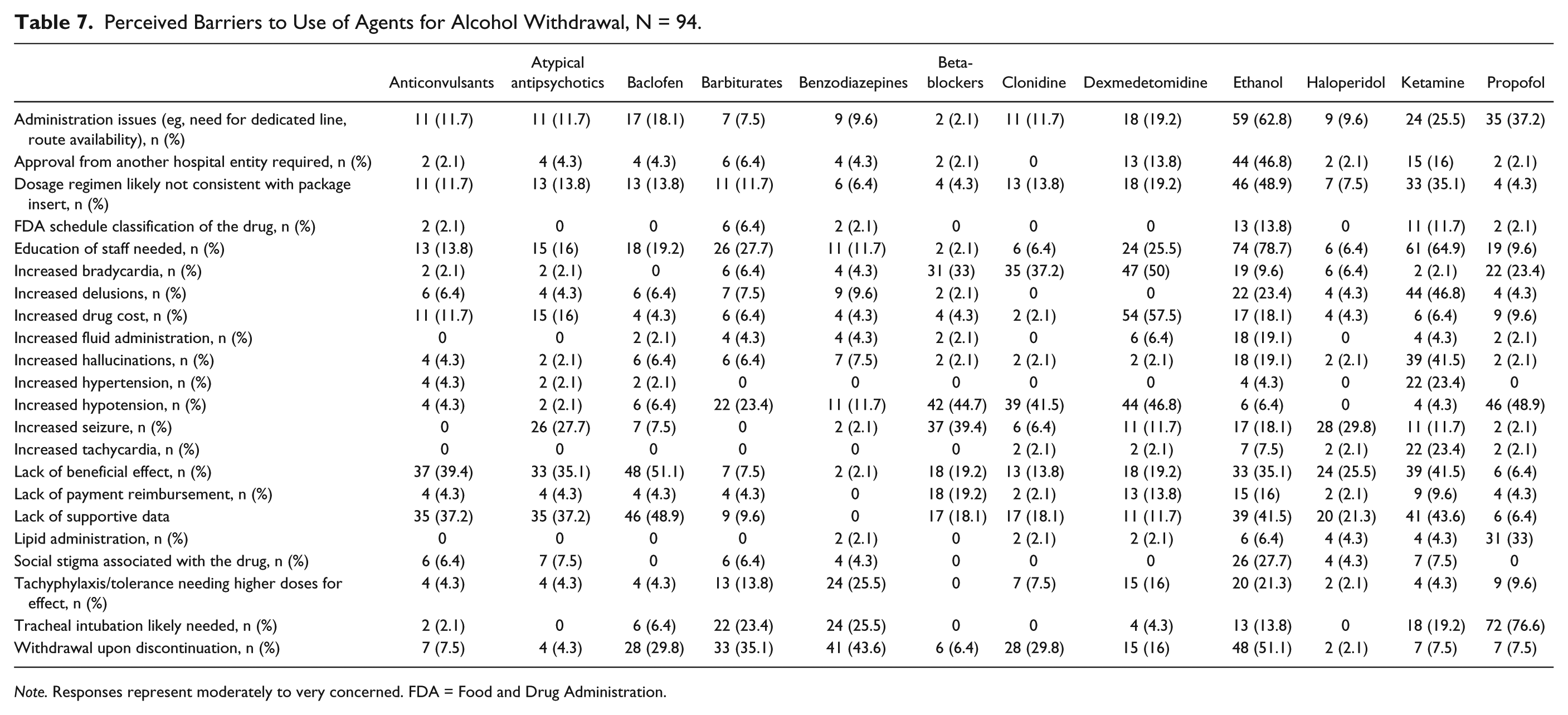
Note. Responses represent moderately to very concerned. FDA = Food and Drug Administration.
Discussion
The goal of this survey was to evaluate current assessment and treatment practices of acute alcohol withdrawal across the United States. To our knowledge, this is the first multicenter survey in the United States to assess current clinical practice patterns. The key findings indicate varying practices across institutions. The CIWA scale was the most commonly utilized assessment tool. Manifestations of alcohol withdrawal that were considered severe included seizures, not oriented to person/place/date, delusions, diastolic blood pressure greater than 110 mm Hg, inconsolable agitation, and tachycardia. Of agents included in the respective institutions, benzodiazepines were the preferred protocol option with high likelihood of use as initial and adjunctive therapies. The most common agent preferred for adjunctive therapy, following additional benzodiazepines, was dexmedetomidine. Several perceived barriers are evident for the use of many agents.
While most respondents indicated their institution utilizes a scoring tool, the most commonly applied scoring tool is the CIWA scale. However, only 45.8% of respondents rated scoring tools as highly effective. This lack of confidence in these tools emphasizes the need for formalized evaluation and validation of easy-to-use scoring tools to delineate the severity of withdrawal. Of note, similar rates of utilization existed for scoring tools and clinical judgment when adjusting therapies. This further highlights the lack of confidence in using scoring tools to aid in the management of therapies.
Respondents commonly agreed which manifestations represented alcohol withdrawal; however, few consistently were perceived as severe. Some manifestations such as bradycardia, hypotension, and hypothermia were rarely considered to represent withdrawal. This is noteworthy because autonomic instability manifested by extreme fluctuations in hemodynamic parameters is indicative of severe withdrawal.1,2 These patients frequently have intermittent bradycardia and hypotension necessitating therapeutic interventions. Other signs and symptoms were commonly rated as a manifestation of alcohol withdrawal, but they were viewed as less severe manifestations. Should a new scoring tool be devised, the perceptions of symptom severity found in this survey may form the basis of delineating which manifestations represent minor, moderate, or severe withdrawal.
Although 90.5% of respondents indicated that an alcohol withdrawal protocol existed at their ICU, they were used routinely 72.3% of the time for initial management and only 24.5% of the time for adjunctive treatment. Almost all (96.8%) respondents agreed that benzodiazepines were the preferred agents for the initial therapy of alcohol withdrawal. No other agent reached 50% agreement in terms of preference for use as an initial therapy. Benzodiazepines possess the most data in alcohol withdrawal and are considered the standard of care, with which to compare other therapies.1-5 In 2010, a systematic review found benzodiazepines to have a protective effect for alcohol withdrawal–induced seizures; however, more adverse events existed when compared with placebo, highlighting the need for optimization and minimization of benzodiazepine use. 13 Intravenous lorazepam was the preferred benzodiazepine. Respondents indicated that α2-adrenoceptor agonists (dexmedetomidine and clonidine) were the second most likely class of agents to be used as initial therapy, although fewer than 20% of respondents indicated either agent is used highly frequently as initial therapy. It is important to note that α2-adrenoceptor agonists only alleviate the autonomic symptoms of alcohol-withdrawal syndrome. Unlike benzodiazepines, which modulate the GABAA receptor to inhibit neuronal excitation, α2-adrenoceptor agonists will not prevent central manifestations from occurring. If dexmedetomidine or clonidine is used as initial therapy without a GABA modulator, patients may be at risk for seizures, agitation, and delirium tremens.
For adjunctive therapy, respondents indicated that benzodiazepines were also the preferred agents. The drivers of use for benzodiazepines were the prevention and treatment of autonomic symptoms, anxiety or agitation, delusion or hallucinations, tremors, seizures, or to facilitate transition to maintenance of step-down therapies. Respondents indicated that α2-adrenoceptor agonists and antipsychotics agents were used frequently for adjunctive therapy at rates of 10% to 25%. α2-adrenoceptor agonists were used for many indications including preventing or reducing GABA-modulating therapies, preventing or treating neurologic depression or respiratory depression associated with GABA-modulating therapies, preventing or treating autonomic symptoms of withdrawal, and preventing or treating anxiety or agitation. Despite only being available as intravenous administration, respondents also suggested dexmedetomidine could aid in the transition to maintenance therapies. The numerous indications for dexmedetomidine are somewhat surprising because the results of small studies only suggest adjunctive dexmedetomidine decreases benzodiazepine requirements in the short term.7-9 It may be that beneficial data from numerous studies with clonidine are being applied to dexmedetomidine. 10 α2-adrenoceptor agonists, however, do not provide protection from alcohol withdrawal–induced seizures so it is not surprising that these agents were rarely used for this indication. Little data support the use of antipsychotic agents for alcohol withdrawal, yet respondents indicated it was an option for reducing GABA-modulating therapies, treating anxiety or agitation, treating delusions or hallucinations, and facilitating transition to maintenance therapies. 14 Of note, few respondents indicated a high likelihood of use of barbiturates, with driving factors including the treatment and prevention of seizures, treatment and prevention of anxiety and agitation, and to reduce or prevent the use of high doses of benzodiazepines. Based on the similar mechanisms of action, there has been interest in utilizing barbiturates, particularly in patients considered refractory to benzodiazepines. Phenobarbital has been shown to potentially reduce the dose of benzodiazepines needed, prevent mechanical ventilation, and prevent admission into the ICU.15-18
Perceived barriers to use were numerous across all agents, although few were frequent. Withdrawal upon discontinuation of benzodiazepines was reported by more than 45% of respondents. The barriers to using dexmedetomidine included bradycardia (50%), hypotension (49%), and cost (58%). Over one-third of respondents regarded lack of beneficial effect or lack of supportive data to be a barrier to the use of anticonvulsants, atypical antipsychotics, baclofen, ethanol, and ketamine.
Limitations
This survey has several limitations. The largest limitation is the response rate of 20%. Of 500 e-mails sent, 94 valid surveys were collected, underpowering the study and potentially not representing the original population of 1500 potential participants. The study was pretested by local practitioners; however, question structure or interpretation could have introduced content validity issues. Responses were not stratified based on size or category of hospital as the number of respondents were too few. Of respondents, 67 (71.3%) practiced in a non-federal government hospital, with a mean number of ICU beds of 92 beds. The majority of respondents appeared to be well trained as many had completed a pharmacy practice residency and 72.3% were Board Certified Pharmacotherapy Specialists. These features may alter the applicability to smaller hospitals or areas of practice with fewer ICU beds or to centers lacking clinical specialists.
Conclusion
This is the first multicenter survey in the United States to assess current clinical practice patterns in assessment and treatment of acute alcohol withdrawal. This survey found that practices vary considerably across the United States for assessment, initial treatment, and adjunctive therapy use. These results justify the need for further study on how best to assess and treat alcohol withdrawal.
Supplemental Material
HospitalPharmacy_AppendixI – Supplemental material for The Assessment and Management Practices of Acute Alcohol Withdrawal: Results of a Nationwide Survey of Critical Care Pharmacists
Supplemental material, HospitalPharmacy_AppendixI for The Assessment and Management Practices of Acute Alcohol Withdrawal: Results of a Nationwide Survey of Critical Care Pharmacists by Susanne Dyal and Robert MacLaren in Hospital Pharmacy
Footnotes
Authors’ Note
A poster was presented at the American College of Clinical Pharmacy Annual Meeting on October 9, 2017 in Phoenix, AZ.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.