
Abstract
Introduction
In Saudi Arabia, it is mandatory that drugs be licensed by the Saudi Food and Drug Authority (SFDA). The reason for this is to guarantee that they are safe, efficacious, and of good quality. Most of the medications that are administered to children have licensed approval outlining the indications for which they may be used, the doses and the routes by which they should be administered. Nevertheless, some of the medications that are prescribed to children are unlicensed. Moreover, many licensed drugs are prescribed to children outside of their approved terms of use. 1 According to US Food & Drug Administration (FDA), off-label drug use applies when medications are used for indication, dosage, and route of administration or patient populations that are not listed among the license recommendations. 2
Off-label use in pediatric by physicians seems to be more common practice in Saudi Arabia if usual treatment routines are not available. 3 However, many concern about the medical decision to use off-label medications in the pediatric patients because of the lack of scientific evidence about safety and efficacy. 4 Some argued that the absence of pediatric-specific information on some medications may indicate that evidence for drug efficacy and safety in the pediatric population has not been submitted to FDA for review or has not met the regulatory standards of “substantial evidence” for FDA approval. 5 Moreover, drug companies might increase the promotion of the use of off-label medications in pediatric patient due to financial aspects. Therefore, it can be said that off-label medication can bring benefits for some patients while it can also lead to unknown health risks or ineffective medicine to other patients. 4 All these concerns heightened the reason to understand the perception and attitudes of general practitioners, pediatricians, and other specialists toward off-label pediatric prescribing.
Methods and Materials
This is a cross-sectional study which was conducted from January 2017 to May 2018 among 160 physicians who agreed to participate after the researchers explained the objectives and benefits of the study in verbal and written form attached to the questionnaires. After doing a comprehensive literature review, the questionnaire was developed from the used questionnaire which was used by Mukattash et al. 6 Our modified questionnaires consisted of 4 parts: the first part included items on sociodemographics (gender, age, education level, year of experience, and the specialty of each participant). The second part assessed the knowledge and the experience of participants regarding to off-label prescribing. The third section was focusing on whether guardians are informed about off-label drug use to their children. The fourth part was concerned with dosing issues related to such use of drugs. In an effort to increase response rate, each physician was approached by telephone after 2 weeks of primary contact to see whether the response has been returned. If not, a further questionnaire was sent out.
Descriptive statistics were used to characterize the study sample. Categorical variables were presented as number and percentages. Chi-square or Fishers exact test was utilized to determine any significant difference between groups. A P value of less than .05 was considered as statistically significant. Statistical analyses were performed using SPSS statistics 24.0.
Results
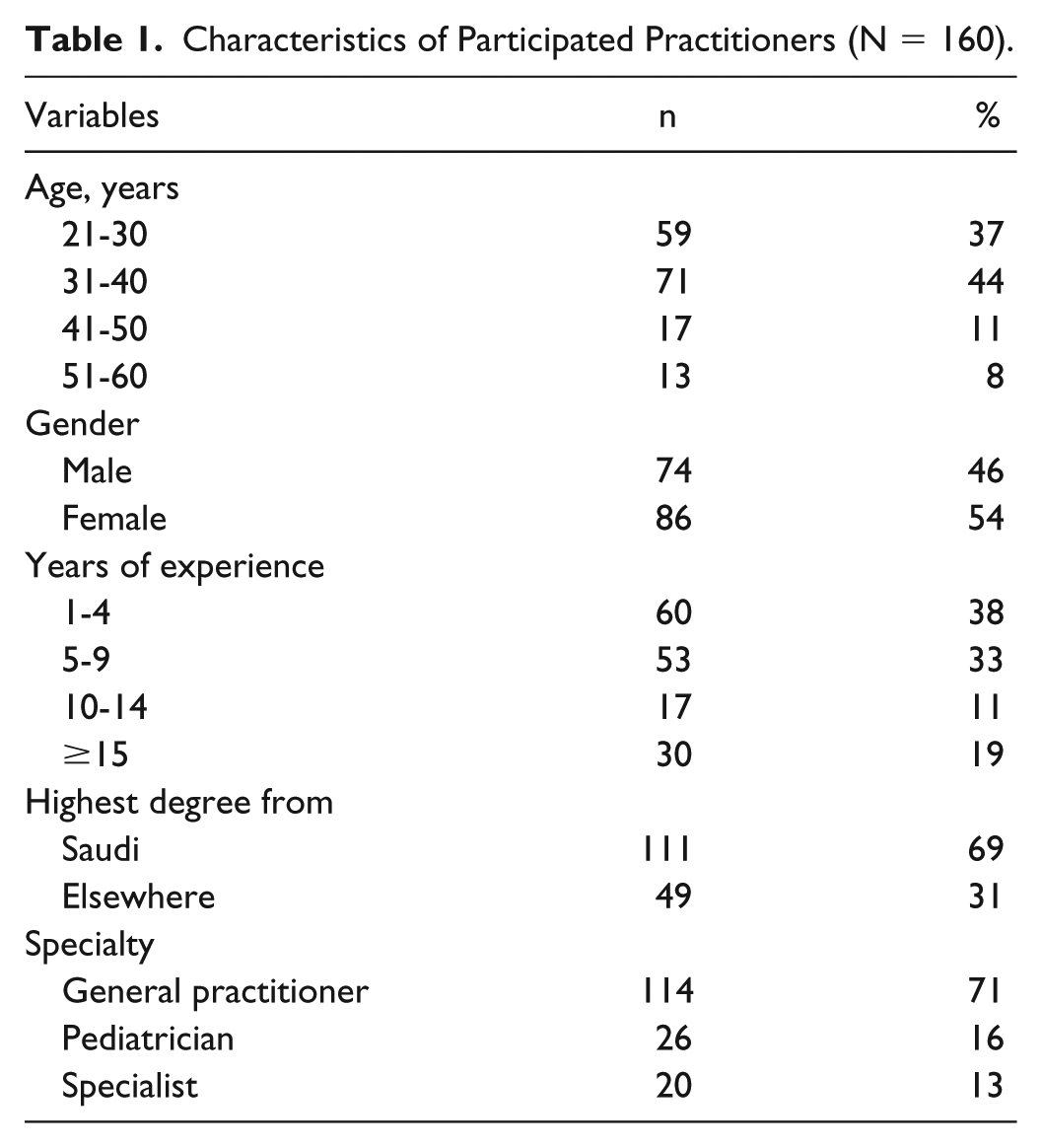
Table 1 presents the general characteristics of participants. Data were obtained from 3 hospitals, comprising a total of 160 practitioners. Among the participants, 80% (n = 130) were younger than 40 years and 54% (n = 86) were females. Regarding the practice and educational characteristics of the participants, a higher proportion of practitioners (n = 111; 69%) were trained from Saudi universities and 62% (n = 100) had 5 years or more experience. The sample comprised of 114 (71%) general practitioners, 26 (16%) pediatricians, and 20 (13%) other specialist practitioners.
Characteristics of Participated Practitioners (N = 160).
In overall, more than half of the participated practitioners (n = 86; 54%) were familiar with the definition of off-label prescribing (Figure 1). In specific, only 46% (n = 52) of general practitioners had the familiarity while three-quarters of pediatricians (n = 19) and specialist practitioners (n = 15) were familiar with off-label prescribing. The difference in proportions was statistically significant (P value = .005). Table 2 presents practitioners’ experience and views regarding off-label prescriptions for children. A total of 59 (37%) practitioners accepted that the terminology was new to them, and the proportion was significantly higher (P value = .006) among the general practitioners (n = 51; 45%) compared with that among pediatricians (n = 4; 15%) and specialist practitioners (n = 4; 20%). Critically, only 41% (n = 65) of practitioners were heard about off-label prescribing for the first time during their higher studies. Thirty percentage of participated practitioners (n = 48) agreed that more than 10% of their prescribed medicines to children were off-labeled; a higher percentage of pediatricians (n = 12; 46%) and general practitioners (n = 34; 30%) prescribed more than 10% off-labeled medications to children compared with specialist practitioners (P value = .020). A majority of participants expressed concerns over the efficacy (n = 133; 83%) and safety (n = 147; 92%) of off-label prescribing to children. The level of concerns over efficacy and safety has statistically differed between the type of practitioners (P value < .05). Importantly, a noticeable proportion of the responders (40 participants did not respond) claimed that they sometimes observed an adverse drug reaction (ADR; n = 23; 20%) or treatment failure (n = 43; 37%) following off-label prescribing medicines to children. Forty-three percent of participants (n = 68) agreed that children aged 2-11 years were more vulnerable to receiving off-label medications. However, a difference in the agreement was observed between general practitioners, pediatricians, and specialist practitioners (P value = .009).
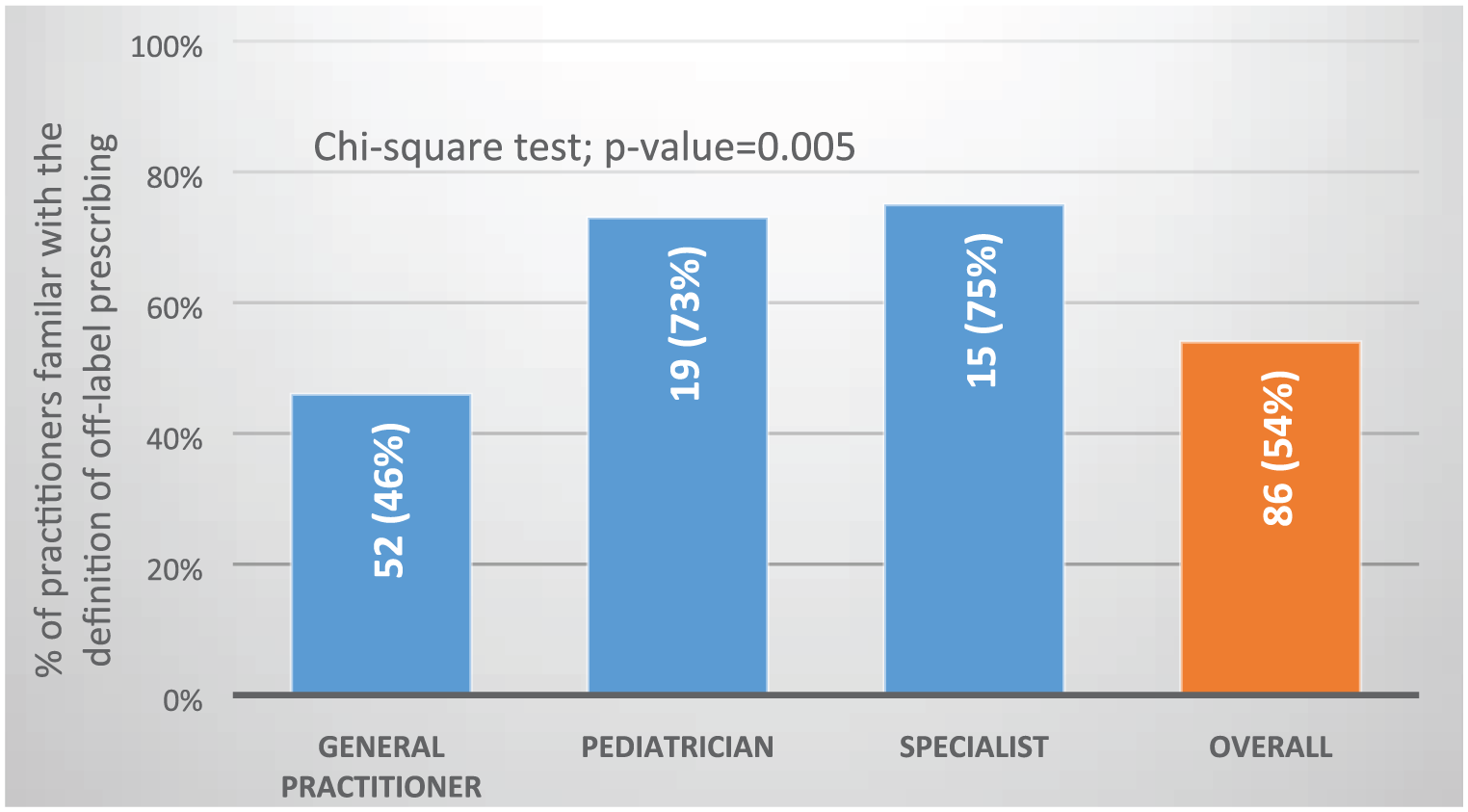
Proportion of practitioners familiar with the definition of off-label prescribing.
Off-label Prescribing by Practitioners: Experiences and Views Regarding Medicines for Children.
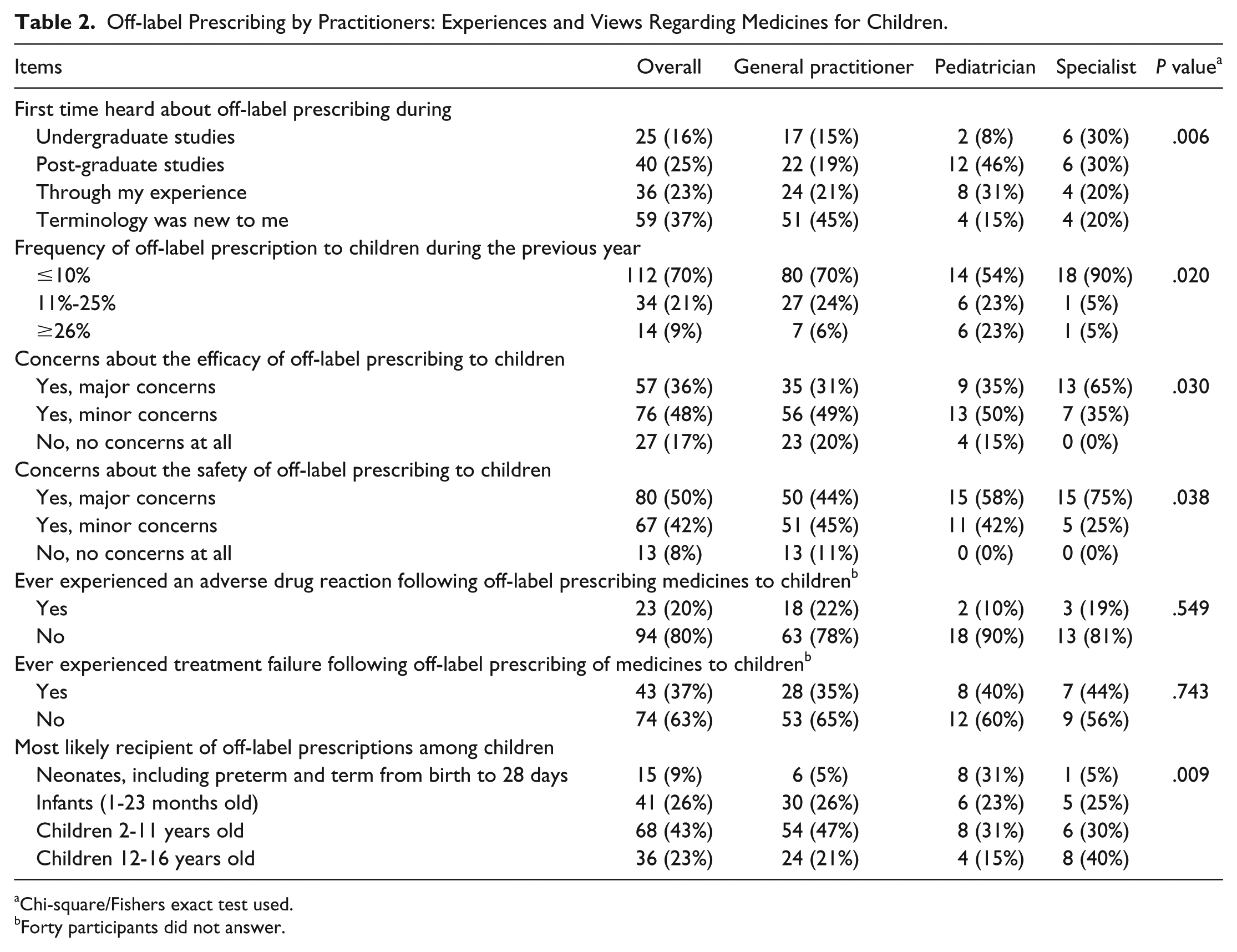
Chi-square/Fishers exact test used.
Forty participants did not answer.
Regarding the practice of informing parents or guardians about the off-label prescription of medications to children, it was found that majority of practitioners favored on the practice (n = 127, 79%; Figure 2). However, the numbers went down when it came to practicality where only 54 (46%; 40 participants did not respond) participants have always informed the parents or guardian (Figure 3). Importantly, pediatricians were more tend to follow the practice but the difference was not statistically significant.
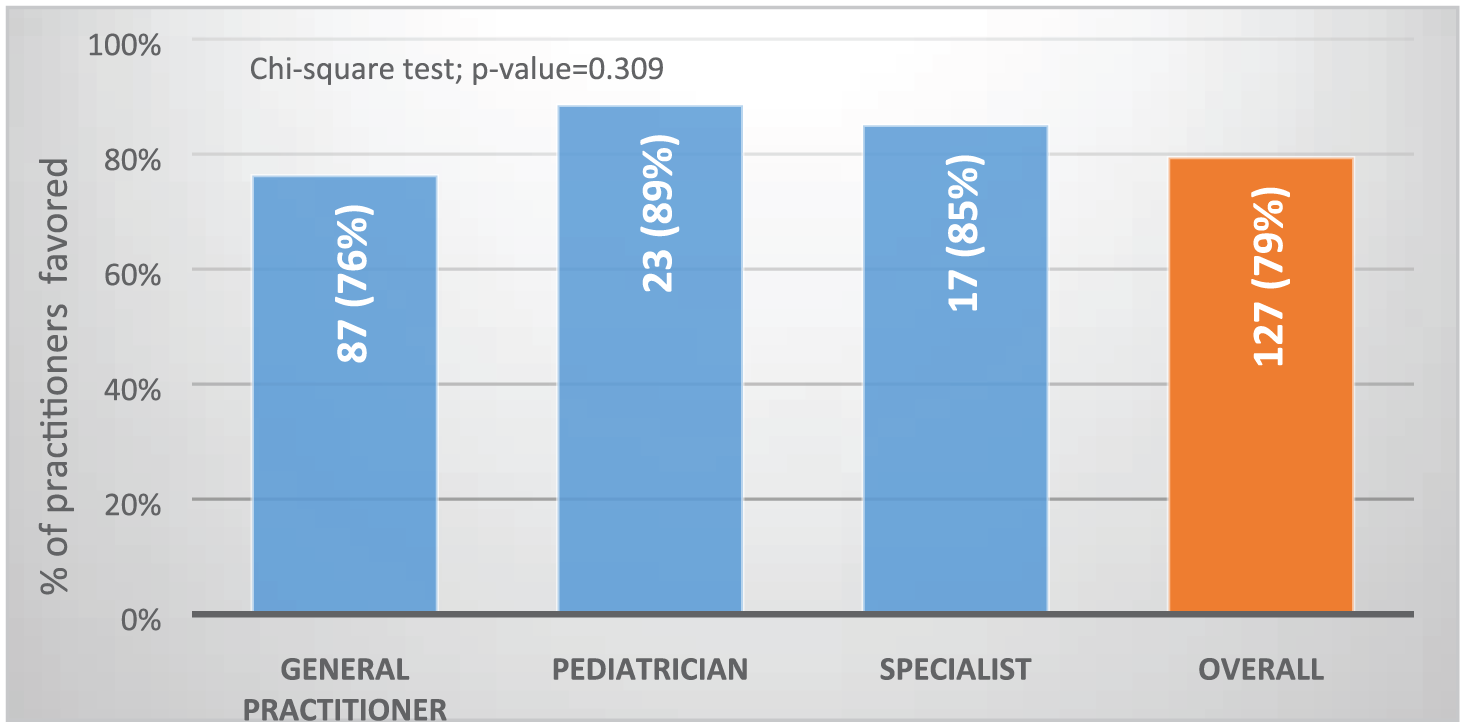
Should parents be informed about off-label prescription to children?
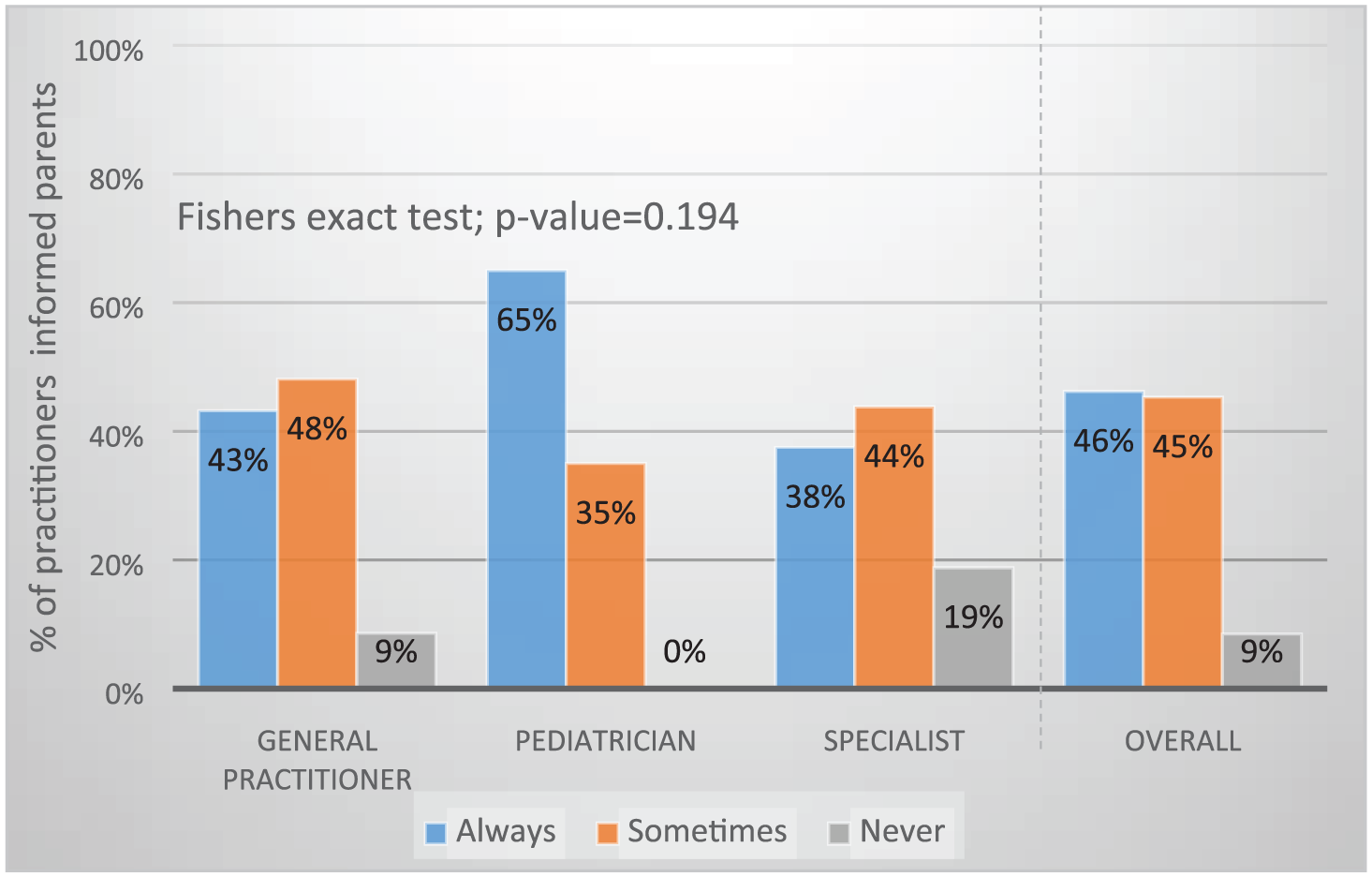
Did practitioner inform parents about off-label prescription?
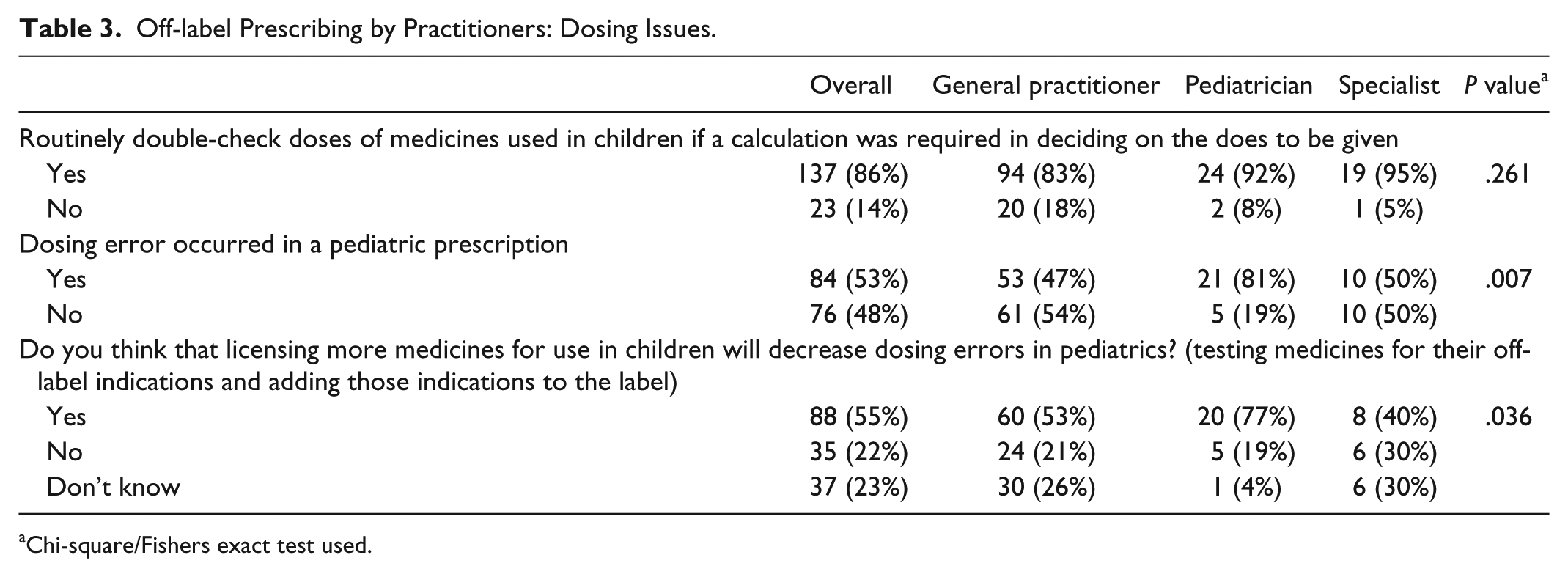
Table 3 presents concerns about overdosing issues with off-label prescriptions. Majority of participated practitioners (n = 137, 86%) claimed that they had routinely double-checked doses of medicines used in children if a calculation had been required in deciding on the dose to be given; no difference in this practice between practitioners (P value = .261). However, only 48% (n = 76) of practitioners were stated that they never came across a dosing error in a pediatric prescription. Critically, large proportion of pediatricians (n = 21; 81%) admitted occurrence of dosing error compared with general practitioners (n = 53; 47%) or specialist practitioners (n = 10; 50%); the difference was statistically significant (P value = .007). Majority of practitioners (n = 88; 55%) advocated testing more medicines for their off-label indications and adding those indications on the label would correlate with lowering such errors.
Off-label Prescribing by Practitioners: Dosing Issues.
Chi-square/Fishers exact test used.
Discussion
Off-label prescriptions are commonly practiced worldwide and are more frequent in the pediatric population. Off-label medicines are the medications that have been prescribed outside of their product license in terms of their recommended age, recommended dosage, a method of administering, or advised use. It is well reported that up to 80% of prescriptions to children were prescribed in an off-label manner. 7
We compiled data from three hospitals, comprising a total of 160 practitioners. In our study, the substantial figure of practitioners was familiar with the definition of off-label prescribing (54%), which is in accordance with the study of Balan et al, who reviewed 11 studies, and concluded that the majority of doctors and community pharmacists to be familiar with the term off-label prescribing. 8 When compared this specifically with general practitioners, pediatrician, and specialist, a substantial proportion (45%) of our general practitioners reported that the terminology off-label prescribing is new to them, whereas pediatricians and specialist care doctors were more familiar with the term compared with their counterparts. A similar report was observed from the worldwide literature studies. 8 However, a study conducted in Italy reported that 74% of pediatricians declared not to have a good knowledge about this practice. 9 Using data from representative general practitioners, pediatricians, and other specialists, we found that 70% of them agreed that less than 10% of their prescribed medicines to children were off-labeled, which is in conformity with Petra Langerová et al, reporting 9.01% off-label prescriptions in children. 10 Whereas the highest percentage (31.7% and 78.1%) was reported from Brazil and Ethiopia.11,12 Although the majority of our practitioners irrespective of their status reported that 10% of their prescriptions to the children in the previous year were off-label, 23% of our pediatricians reported that more than 26% of their prescriptions in the previous year were off-label in nature. A similar trend was observed in other studies within the country, of which 29.7% (173/583) and 12.9% (75/583) were classified as off-label and unlicensed drugs respectively. 3 Hence, the off-label pediatric prescriptions range from 10% to 90% across the world, emphasizing the need for FDA-approved pediatric medications. 7
Practitioners’ concerns about the safety and efficacy of off-label prescriptions were also assessed. Among the participants, overall 36% of them had major concerns with regard to the effectiveness of the off-label medicines. These concerns were raised mostly by the specialists (65%). Similarly, 50% of our practitioners considered the safety of off-label as the foremost concern. Likewise, a higher percentage of the specialist (75%) often had an abundant worry about the safety of off-label medication in children. Which obedience to other studies wherein a high proportion (77.8% and 87.9%) of practitioners expressing concerns about the safety and efficacy of off-label prescribing in children respectively.13,14 Concerns about how safe was the prescription of off-label medicine in children were again raised in a question that examined whether participants felt that the use of off-label medicines in children may increase the likelihood of ADRs or treatment failure. Interestingly, in our study, 80% of our responded practitioners never experienced an ADR with their off-label medication prescription in children. A similar trend was observed in another study also, wherein 83% had not perceived an adverse event in off-label prescriptions. 14 Moreover, 37% of our responded practitioners noticed treatment failure with their off-label prescriptions children. A similar report was obtained from McLay et al study wherein 45% of them had noticed a treatment failure with off-label prescriptions in children. 14
We also surveyed that which age group of the pediatric population is frequently prescribed with off-label drugs. It was observed that children at an age of 2-11 years old were routinely prescribed with off-label drugs (43%), which are in confirmation with previous studies from Ethiopia and Germany.12,15 Irrespective of the age group of the children, pediatricians use off-label medications broadly, while specialists and general practitioners have limited the number of their off-label prescription in neonates and preterm (5%).
The FDA policy undeniably declares the use of a pharmaceutical product once approved, for indications, dosages, routes, or age groups other than the approved on the label. However, as reported, the off-label drugs are not always safe and efficacious and might expose children to unnecessary and unpredictable risks. It is quite sensible to inform parents about off-label use of drugs in their children and/or to obtain informed consent. 16 Off-label use becomes not an illegal, but an ethical issue when the principle of informed consent is introduced. Unfortunately, although prescribers (79%) insisted on informing guardians regarding off-label prescribing, in reality the numbers went down (46%). Bang et al reported unawareness of parents (70%) in regard to off-label prescribing of drugs to their children, while 93% of them emphasized to be informed about such use. 17 McLay et al reported attitude of Scottish pediatricians not to inform parents (69%) and family’s general practitioner (67%) about off-label drug prescribing and neither secure informed consent. 14 A survey conducted by Radley et al scrutinized 150 million prescriptions in the United States for off-label use and concluded 73% had little or none scientific backing. Furthermore, the study evidenced that most of off-label drugs were prescribed to outpatients and that without scientific support. 18 The lack of scientific support endangers life, such as the case of fenfluramine prescribed as off-label drug for weight-loss (18 million prescriptions) prior to the conclusion that it caused heart valve damage in thousands of people. The lack of evidence of efficacy and safety of a drug to be used in some other indications puts patients on risk, hence legal standards that require informed consent from a person before being exposed to risk should be followed by physicians. 16
The pediatric patient population is deadlocked in studies accessing clinical efficacy and safety of drugs; it is well established that pharmacokinetic and pharmacodynamic properties of drugs are affected by developmental changes in infants and children, thus their remains need for dose adjustments.19,20 A majority (86%) of participants whispered that they had routinely rechecked the doses of the medicines being prescribed to the pediatric patients when a calculation was required in determining the required dosage. Interestingly, 53% of the participants had encountered an error in the dosage of prescription. Especially, the pediatricians (81%) reported that dosing errors occurred in their off-label prescriptions. A comparable result was obtained from a recently published study from Jordan wherein 48% of the pharmacists had encountered an error in the dosage of a pediatric prescription. 21 Even if the physician considers dose adjustment, there are limitations of the dosage forms available for children. In case of oral solids, the risk of choking with small dose is a significant risk factor. Moreover, flexibility, dose uniformity, palatability, and stability (chemical, physical, or microbiological) may be challenging for liquid preparations. 22 Goncalves and Heinneck reported that overdose (93.3%) of off-label drugs was more frequent than underdose (6.7%) in said prescriptions, unlike as reported by studies from Ekins-Daukes et al and ’t Jong et al.23-25 Gabapentin was used as an antiepileptic off-label drug in children, and studies demonstrated that children less than 5 years of age needed higher doses per kg for effective seizure control, while children less than 12 years of age presented newer adverse effects such as aggression and hostility. Hence, the dosing and safety label for Gabapentin was changed. 26 Thus, measures taken in case of Gabapentin need to be instituted in case of other drugs also.
Conclusion
This is the first study performed to examine the current knowledge and views of general practitioners, pediatricians, and specialists toward off-label pediatric prescribing in the Eastern province in Saudi Arabia. The majority of participants were familiar with the definition of off-label prescribing. More specifically pediatricians and specialist care doctors were more familiar with the term. Thirty percentage of participated practitioners consented that more than 10% of their prescribed medicines to children were off-labeled. This practice has more commonly seen with pediatricians and general practitioners than other specialists. Children at an age of 2-11 years old were routinely prescribed with off-label medications. Participants showed more concerns about the safety and efficacy of off-label prescriptions, and more work toward assessing the efficacy and safety is required as off-label medications might expose children to unnecessary and unpredictable risks.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.