
Abstract
Each month, subscribers to The Formulary Monograph Service receive 5 to 6 well-documented monographs on drugs that are newly released or are in late phase 3 trials. The monographs are targeted to Pharmacy & Therapeutics Committees. Subscribers also receive monthly 1-page summary monographs on agents that are useful for agendas and pharmacy/nursing in-services. A comprehensive target drug utilization evaluation/medication use evaluation (DUE/MUE) is also provided each month. With a subscription, the monographs are available online to subscribers. Monographs can be customized to meet the needs of a facility. Through the cooperation of The Formulary, Hospital Pharmacy publishes selected reviews in this column. For more information about The Formulary Monograph Service, contact Wolters Kluwer customer service at 866-397-3433.
Pharmacy and Therapeutics Review
Indications
Meloxicam intravenous (IV) injection is approved by the Food and Drug Administration (FDA) for the management of moderate to severe pain in adults, for use alone or in combination with non-nonsteroidal anti-inflammatory drug (NSAID) analgesics. 1 Meloxicam IV is associated with a delayed onset of analgesia and is not recommended for use when rapid onset of analgesia is required. 1
See Table 1 for a comparison of the injectable formulations of the NSAIDs ketorolac and meloxicam.1,2
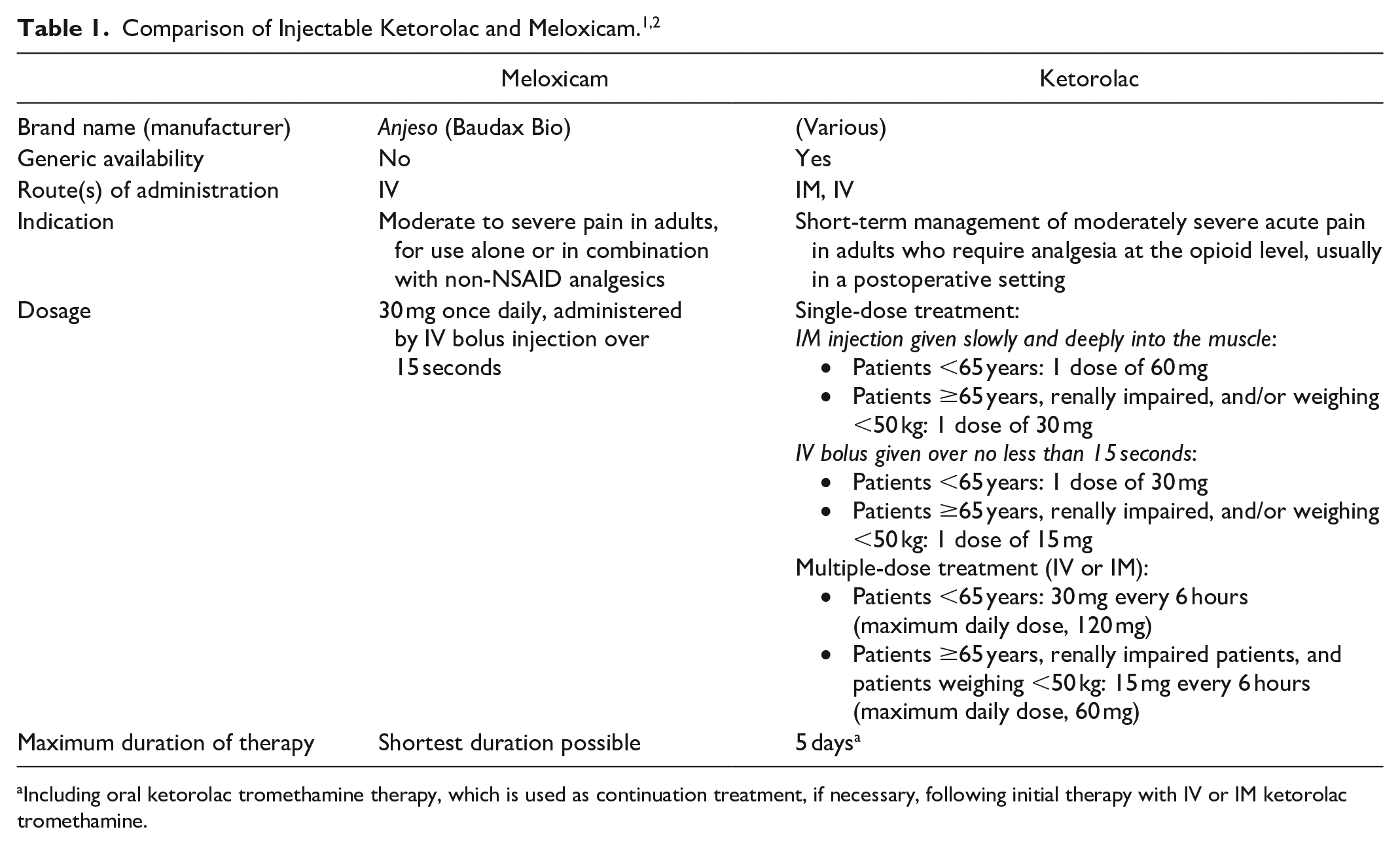
Including oral ketorolac tromethamine therapy, which is used as continuation treatment, if necessary, following initial therapy with IV or IM ketorolac tromethamine.
Clinical Pharmacology
Meloxicam IV is an NSAID with analgesic, anti-inflammatory, and antipyretic properties. Its mechanism of action is thought to involve the inhibition of cyclooxygenase (COX-1 and COX-2). 1
The effects of IV meloxicam and ketorolac on platelet function have been evaluated using various tests. The collagen with adenosine diphosphate test (sensitive to thrombocytopathies) showed no differences in closure time for meloxicam- or ketorolac-treated samples and untreated control. The collagen with epinephrine test (sensitive to aspirin-induced platelet abnormalities) showed no difference in closure time between any meloxicam concentration and untreated control, while ketorolac was associated with longer closure times versus untreated control and versus meloxicam at several concentrations. 3
Meloxicam IV has no clinically significant effect on the QTc interval. 1
Pharmacokinetics
A single-dose of meloxicam 30 mg administered IV in healthy volunteers produced a peak plasma concentration of 5642.9 ng/mL, a time to peak concentration of 0.12 hours, an area under the curve (AUCinf) of 107 508.7 ng•hour/mL, and a half-life of 23.3 hours. Oral administration of meloxicam 15 mg produced values of 1221 ng/mL, 6.57 hours, 53 998.8 ng•hour/mL, and 26.4 hours, respectively. Following multiple dosing, meloxicam 30 mg IV resulted in predictable accumulation (slightly higher than 2-fold) without a change in terminal elimination half-life. 1
Following administration of meloxicam IV, apparent volume of distribution during the terminal elimination phase is 9.63 L. 1 Meloxicam protein binding is extensive (99.4%) and primarily to albumin.1,4
Meloxicam is extensively metabolized in the liver to inactive metabolites.1,4 The main metabolic enzyme is CYP2C9, and CYP3A4 plays a minor role. 1
Meloxicam is excreted predominantly as its metabolites. 4 Traces of the unchanged parent compound are excreted in urine (0.2%) and feces (1.6%). Administration of cholestyramine following a single IV meloxicam dose can decrease meloxicam’s AUC by 50%. 1
No meaningful changes in meloxicam IV pharmacokinetics were observed based on age, gender, or race. 1
The impact of hepatic impairment on meloxicam IV pharmacokinetics has not been fully evaluated. Following a single 15 mg oral dose of meloxicam in patients with mild (Child-Pugh class A) or moderate (Child-Pugh class B) hepatic impairment, no marked difference in plasma concentrations or protein binding were observed compared with healthy volunteers. Patients with severe hepatic impairment have not been adequately evaluated. 1
Mild renal impairment in elderly subjects resulted in a minor change in peak plasma concentrations and AUC of meloxicam IV; no dosage adjustments are necessary in patients with mild renal impairment. Use of meloxicam IV in patients with moderate to severe renal impairment has not been adequately studied and is not recommended. Use is contraindicated in patients with moderate to severe renal insufficiency who are at risk for renal failure due to volume depletion. 1
Comparative Efficacy
Indication: Management of Moderate to Severe Pain
Guidelines
Studies
Results
Primary End Point(s)
Estimated effect size for summed pain intensity difference at 48 hours (SPID48) was 1.15 (95% CI, 0.51-1.79) for meloxicam 30 mg and 1.01 for meloxicam 60 mg (P ≤ .01 for both vs placebo). Pain reduction was significantly greater with both doses of meloxicam IV compared to placebo (P ≤ .05) based on SPID at all specific time points (6 hours [SPID6], 12 hours [SPID12], 24 hours [SPID24], and for the intervals 12 to 24 hours [SPID12-24], 12-48 hours [SPID12-48], and 24-48 hours [SPID24-48]).
Statistically significant decreases in pain from baseline (ie, negative pain intensity difference [PID] values) were detected as early as 15 minutes after the first dose of meloxicam IV: mean PID was −1.5 with meloxicam 30 mg (P < .05 vs baseline) and −0.7 with meloxicam 60 mg (P < .05 vs baseline).
Mean change in pain intensity score from baseline at all assessments was less than zero (ie, pain level was lower than at baseline) with both doses of meloxicam IV; mean changes at the 48-hour assessment were −4.6 with meloxicam 30 mg and −4.3 with meloxicam 60 mg (both P < .001 vs baseline). In the placebo group, mean PID at 0.25 hours was −0.1; thereafter, pain intensity changes were above zero until the 20-hour assessment, with no significant difference from baseline detected until hour 28.
Secondary End Point(s)
Proportion of patients with 30% or higher overall reduction in pain from baseline within the first 24 hours after study drug administration was 50% with meloxicam 30 mg (P ≤ .05 vs placebo), 40% with meloxicam 60 mg (P ≤ .05 vs placebo), and 10.5% with placebo.
Proportion of patients with 50% or higher overall reduction in pain from baseline within the first 24 hours after study drug administration was 30% with meloxicam 30 mg (P ≤ .05 vs placebo), 20% with meloxicam 60 mg, and 0% with placebo.
Patient global assessment (PGA) of pain control at 24 and 48 hours after first dose of study drug (5-point scale; 0 = poor, 1 = fair, 2 = good, 3 = very good, 4 = excellent): No statistically significant differences were observed among the 3 treatment groups at either time point; however, more patients in the meloxicam groups reported “good” or better pain control.
Rescue medication was required by at least 90% of patients in all 3 groups within the first 24 hours of receiving the initial dose of study medication. The need for rescue medication was lower in all 3 groups during the second 24-hour period (hours 24-48): 55% in the meloxicam 30 mg group, 52.6% in the meloxicam 60 mg group, and 77.8% in the placebo group.
Median time to administration of the first dose of rescue analgesia was 3.1 hours in the meloxicam 60 mg group and 1.57 hours in the placebo group (P < .05); there was no significant difference between the meloxicam 30 mg group and the placebo group.
Mean number of rescue analgesia doses was 8.2 with meloxicam 30 mg, 6.9 with meloxicam 60 mg, and 11.1 with placebo.
Similar results were observed in another bunionectomy study comparing meloxicam IV 30 mg and placebo. 7
Results
Primary End Point(s)
Pain intensity reduction was significantly greater with meloxicam IV compared to placebo based on SPID24: Least squares (LS) mean reduction in SPID24 was -4262.1 with meloxicam IV and -3535.7 with placebo (P = .0145).
Secondary End Point(s)
A statistically significant effect on pain intensity reduction was observed with meloxicam IV versus placebo for SPID12 (−1763.8 with meloxicam IV vs 1471.1 with placebo; P = .0434), SPID48 (−10 600 with meloxicam IV vs −8828.2 with placebo; P = .004), and SPID24-48 (−6337.8 with meloxicam IV vs −5293.5 with placebo; P = .0028), but not for SPID6 (−607 with meloxicam IV vs −510.9 with placebo; P = .1841).
PID from baseline was numerically lower with meloxicam IV than with placebo at every time point after 30 minutes. The meloxicam IV group showed a statistically significant difference in time to perceptible pain relief compared to placebo (median of 0.76 hours with meloxicam IV and 1.28 hours with placebo; P = .005); however, there was no statistically significant difference between the 2 groups for time to meaningful pain relief, which was approximately 3 hours in both groups.
Proportion of patients with 30% or greater overall reduction in pain from baseline within the first 24 hours after study drug administration was 71.8% with meloxicam IV and 56.9% with placebo (P = .0178).
Proportion of patients with 50% or greater overall reduction in pain from baseline within the first 24 hours after study drug administration was 28.2% with meloxicam IV and 18.3% with placebo (P = .0788).
PGA of pain control: A statistically significant difference favoring meloxicam IV over placebo was observed at 48 hours (P = .0027) but not at 24 hours. The proportion of patients reporting “good” or better pain control on PGA was numerically better for those treated with meloxicam IV compared to placebo at hour 24 (84.3% vs 67.3%) and at hour 48 (88.8% vs 83.4%).
At least 1 dose of rescue medication was used within the first 24 hours by 88.2% of patients in the meloxicam IV group and 89.9% of those in the placebo group (P = .6559). There was also no significant difference between the time to first dose of rescue medication (2.6 vs 2.45 hours, respectively); however, during hours 24 to 48, fewer patients in the meloxicam IV group required rescue analgesia (55.6% vs 75.7%; P = .0014). The number of rescue doses per subject was also significantly lower in the meloxicam IV group than in the placebo group: 3.66 versus 4.38 during hours 0 to 24 (P = .0275), 1.75 versus 2.72 during hours 24 to 48 (P = .0009), and 5.38 versus 7.07 during hours 0 to 48 (P = .0027).
A pooled analysis of the safety of meloxicam IV for treatment of moderate to severe acute pain (conducted in 2018) consisted of 1426 adults with moderate to severe postoperative pain and treated with at least 1 dose of IV meloxicam (5-60 mg) or placebo in 4 phase 2 studies and 3 phase 3 studies. In trials monitoring opioid use, meloxicam IV was often associated with reduced postoperative rescue opioid use. According to the pooled data, treatment-emergent adverse events occurred in 47% of meloxicam IV-treated patients and 57% of placebo-treated subjects. The most common adverse events across treatment groups included nausea, headache, vomiting, and dizziness. 9
Several other studies evaluating meloxicam IV use are not described in the prescribing information but demonstrated adequate postoperative pain relief and decreased need for opioid analgesics in dental impaction surgery, open abdominal hysterectomy, major elective surgery, and orthopedic surgery.10-13
Contraindications, Warnings, and Precautions
Contraindications
Meloxicam IV is contraindicated in patients with known hypersensitivity reactions to meloxicam or to any component of the formulation (povidone, sodium deoxycholate [deoxycholic acid], sucrose, and water for injection); in patients with history of asthma, urticaria, or other allergic-type reactions after taking aspirin or other NSAIDs; in the setting of CABG surgery; and in patients with moderate to severe renal insufficiency who are at risk for renal failure due to volume depletion. 1
Warnings and Precautions
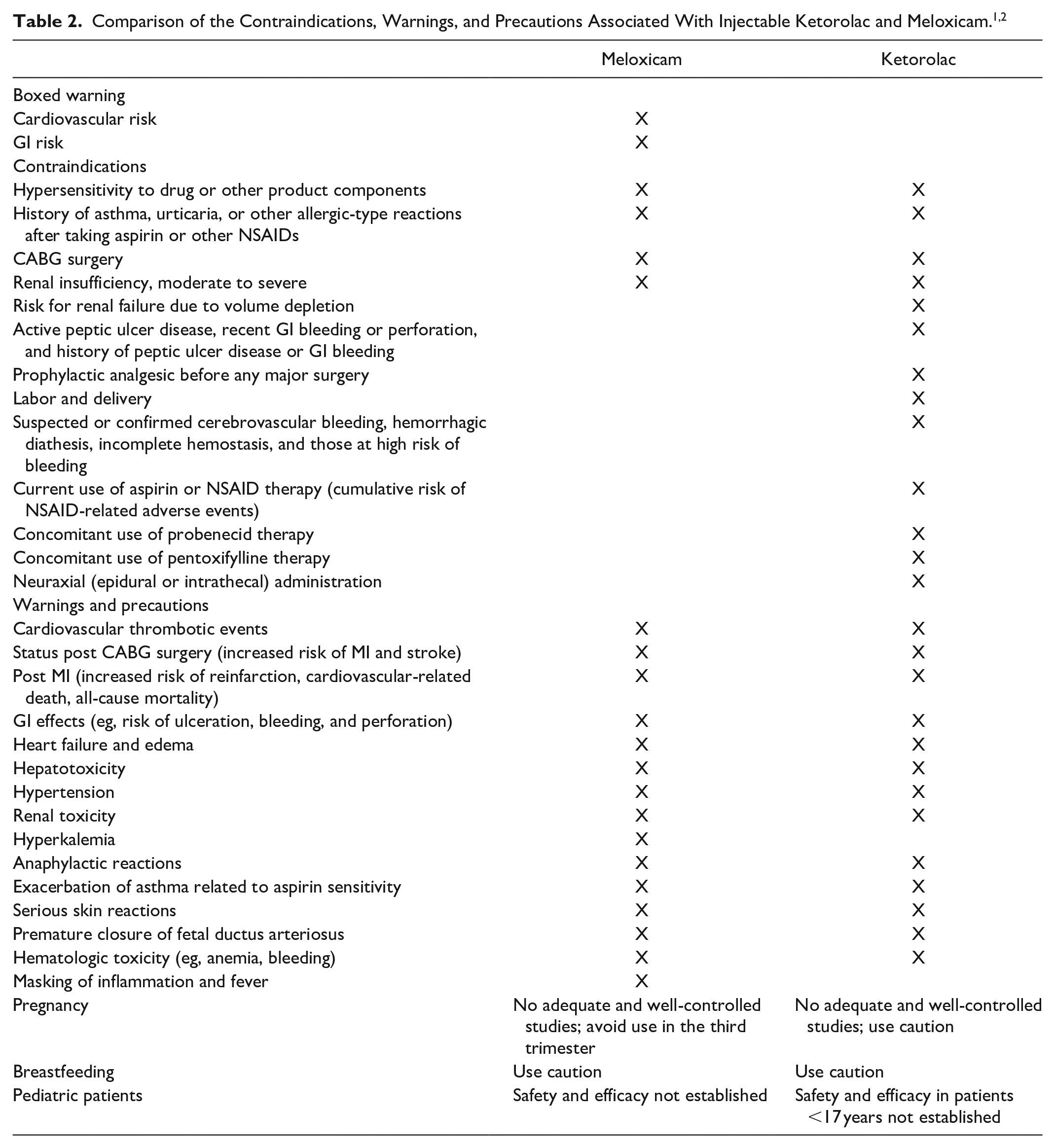
The warnings and precautions associated with meloxicam IV are similar to those of injectable ketorolac (see Table 2).
Meloxicam IV labeling includes a boxed warning regarding the risk of serious cardiovascular and GI events with use of NSAIDs. 1
Use of NSAIDs is associated with an increased risk of cardiovascular thrombotic events (eg, MI, stroke). Evidence regarding concurrent use of aspirin to mitigate this risk has been inconsistent; concurrent use of aspirin is associated with an increase in risk for serious GI events. 1
Two previous studies of another COX-2–selective NSAID for the treatment of pain following CABG surgery showed an increased incidence of MI and stroke. The use of NSAIDs in the setting of CABG is contraindicated for this reason. 1
Based on observational studies in the Danish National Registry, patients treated with NSAIDs in the post MI period may be an increased risk of reinfarction, cardiovascular-related death, and all-cause mortality beginning in the first week of NSAID treatment following MI. Therefore, meloxicam should be avoided in patients with a recent MI unless the benefits are expected to outweigh the risk of recurrent cardiovascular thrombotic events. If meloxicam is used in patients with a recent MI, monitor for signs of cardiac ischemia. 1
Treatment with NSAIDs, including meloxicam, can increase the risk of adverse GI effects (eg, inflammation; ulceration; bleeding; and perforation of the esophagus, stomach, or small or large intestine). These adverse events can occur at any time, with or without warning symptoms, in patients treated with meloxicam IV. The risk is increased in patients with a history of peptic ulcer disease and/or GI bleeding; other factors include longer duration of NSAID therapy; concomitant use of oral corticosteroids, aspirin, anticoagulants, or selective serotonin reuptake inhibitors (SSRIs); smoking; use of alcohol; older age; and poor general health status. The risk of GI bleeding is also increased in patients with advanced liver disease and/or coagulopathy. 1
Elevations in liver enzymes (eg, ALT, AST) have been reported in about 1% of patients treated with NSAIDs in clinical trials. Rare but sometimes fatal cases of severe hepatic injury, including fulminant hepatitis, liver necrosis, and hepatic failure, have been reported. Patients should be warned of this risk and informed of warning signs and symptoms (eg, nausea, fatigue, lethargy, diarrhea, pruritus, jaundice, right upper quadrant tenderness, and “flu-like” symptoms). 1
New or worsening hypertension can occur during NSAID therapy, including with meloxicam IV. Hypertensive patients taking ACE inhibitors, thiazides, or loop diuretics may have impaired response to these therapies while taking NSAIDs. 1
There is an increased risk of heart failure with NSAID use, based on meta-analysis results; a Danish National Registry study of patients with heart failure showed NSAID use increased the risk of MI, hospitalization for heart failure, and death. In addition, fluid retention and edema can occur with NSAID therapy. The therapeutic effects of treatments used to treat these medical conditions (eg, diuretics, ACE inhibitors, angiotensin receptor blockers) may be blunted by meloxicam use. Therefore, meloxicam should be avoided in patients with severe heart failure unless the benefits are expected to outweigh the risk of worsening heart failure. If meloxicam is used in patients with severe heart failure, monitor for signs of worsening heart failure. 1
Renal papillary necrosis, renal insufficiency, acute renal failure, and other renal injury can occur during NSAID therapy, especially during long-term administration. Renal toxicity has also occurred in patients in whom renal prostaglandins have a compensatory role in the maintenance of renal perfusion. In these patients, administration of an NSAID may cause a dose-dependent reduction in prostaglandin formation and, secondarily, in renal blood flow, which may precipitate overt renal decompensation. Patients at greatest risk of this reaction are those with impaired renal function, dehydration, hypovolemia, heart failure, or liver dysfunction, as well as those taking diuretics and ACE inhibitors or angiotensin receptor blockers and elderly patients. Volume status should be corrected in patients with dehydration or hypovolemia prior to initiation of meloxicam IV therapy. Discontinuation of NSAID therapy is usually followed by recovery to the pretreatment state. 1
Hyperkalemia may occur during NSAID therapy, including in patients without renal impairment. 1
Anaphylactic reactions have occurred with meloxicam therapy in patients with and without known hypersensitivity to meloxicam and in patients with aspirin-sensitive asthma. 1
Patients with asthma may have aspirin-sensitive asthma, which may include chronic rhinosinusitis complicated by nasal polyps; severe, potentially fatal bronchospasm; and/or intolerance to aspirin and other NSAIDs. Because cross-reactivity between aspirin and other NSAIDs has been reported in patients with aspirin-sensitive asthma, meloxicam IV is contraindicated in patients with this type of aspirin sensitivity. If meloxicam is used in a patient with preexisting asthma (without known aspirin sensitivity), monitor for changes in the signs and symptoms of asthma. 1
NSAIDs, including meloxicam IV, can cause serious skin reactions (eg, exfoliative dermatitis, Stevens-Johnson Syndrome, toxic epidermal necrolysis). Meloxicam should be discontinued at the first appearance of skin rash or any other sign of hypersensitivity. 1
Meloxicam can cause premature closure of fetal ductus arteriosus. Use during pregnancy should be avoided starting at 30 weeks’ gestation (third trimester). 1
Anemia can occur with NSAID therapy, possibly due to occult or gross blood loss, fluid retention, or an incompletely described effect on erythropoiesis. In the case of signs or symptoms of anemia, monitor hemoglobin or hematocrit. 1
The risk of bleeding events may be increased in with use of NSAIDs, including meloxicam IV. Comorbid conditions (eg, coagulation disorders) or concomitant use of warfarin, other anticoagulants, antiplatelet agents (eg, aspirin), SSRIs, or serotonin norepinephrine reuptake inhibitors (SNRIs) may increase bleeding risk. 1
The pharmacologic activity of meloxicam IV can mask signs of infection (eg, inflammation and/or fever). 1
Use of NSAIDs, including meloxicam IV, in pregnant women during the third trimester increases the risk of premature closure of the fetal ductus arteriosus. Meloxicam IV should be avoided during pregnancy starting at 30 weeks’ gestation. There are no adequate and well-controlled studies of meloxicam in pregnant women; data from observational studies regarding potential embryo-fetal risks of NSAID use during the first 2 trimesters are inconclusive. 1
There are no studies on the effects of meloxicam during labor or delivery. In animal studies, NSAIDs, including meloxicam, inhibited prostaglandin synthesis, caused delayed parturition, and increased the incidence of stillbirth. 1
There are no data regarding the presence of meloxicam IV or its metabolites in human milk or its effects on breastfeeding infants or milk production. Caution is advised. 1
Safety and efficacy of meloxicam IV have not been established in pediatric patients. 1
Use in elderly patients may be associated with an increased risk of NSAID-related serious cardiovascular, GI, and/or renal adverse reactions. 1
See Table 2 for a comparison of the contraindications, warnings, and precautions associated with the injectable formulations of ketorolac and meloxicam.1,2
Adverse Reactions
The most common adverse reactions associated with meloxicam (incidence at least 2% and occurring at a greater frequency than with placebo) in controlled clinical trials included constipation (7.6% vs 6.1% with placebo), gamma-glutamyltransferase increased (2.8% vs 1.5% with placebo), and anemia (2.4% vs 1% with placebo). 1
Other adverse reactions (incidence less than 2%) reported with meloxicam in clinical trials included asthenia, back pain, edema, fatigue, hyperthermia, infusion-site reactions (including pain, pruritus, phlebitis, and thrombosis), muscle spasms, noncardiac chest pain, pyrexia, vaginal discharge, weight decrease, disturbance in attention, migraine, presyncope, somnolence, syncope, abdominal discomfort, abdominal distension, abdominal pain, diarrhea, dry mouth, epigastric discomfort, flatulence, frequent bowel movements, gastritis, gastroesophageal reflux, GI pain, rectal hemorrhage, tachycardia, increased bleeding time, neutropenia, thrombocytosis, cellulitis, gastroenteritis, urinary tract infection, vulval abscess, abnormal liver function test, hypokalemia, hypomagnesemia, incision-site hemorrhage, incision-site rash, wound dehiscence, wound hematoma, confusion, hallucination, insomnia, dyspnea, epistaxis, hypoxia, oropharyngeal pain, contact dermatitis, ecchymosis, rash, pollakiuria, and urinary retention. 1
Drug Interactions
Drug interactions with meloxicam are similar to those reported with other NSAIDs.
Concomitant use of meloxicam with anticoagulants (eg, warfarin), antiplatelet agents (eg, aspirin), SSRIs, or SNRIs may increase the risk of bleeding. 1
Analgesic doses of aspirin and low-dose aspirin for cardiac prophylaxis may increase the risk of bleeding when used with meloxicam. Meloxicam is also not a substitute for low-dose aspirin for cardiovascular protection. 1
Concomitant use with other NSAIDs or salicylates (eg, diflunisal, salsalate) may increase the risk of GI toxicity. 1
NSAIDs may diminish the antihypertensive effect of ACE inhibitors, angiotensin receptor blockers, or beta-blockers (including propranolol). In addition, the combination of NSAIDS and these drugs may cause deterioration of renal function in patients who are elderly, volume depleted, or have preexisting renal impairment. 1
Use of NSAIDS with loop diuretics (eg, furosemide) or thiazide diuretics may reduce the natriuretic effect of the diuretic. While this effect has not been observed in studies with furosemide agents and meloxicam, patients should still be monitored for a decreased diuretic effect. 1
Use with lithium may result in elevated lithium plasma levels due to decreased lithium clearance. 1
Concomitant use of NSAIDs and methotrexate may increase the risk of methotrexate toxicity (eg, neutropenia, thrombocytopenia, renal dysfunction).
Concomitant use of meloxicam IV may increase the risk of pemetrexed-related toxicities (eg, myelosuppression, renal and GI toxicity). 1
Concomitant use of meloxicam and cyclosporine may increase cyclosporine’s nephrotoxicity. 1
Concomitant use of CYP2C9 inhibitors (eg, amiodarone, fluconazole, sulphaphenazole) may increase the plasma levels of meloxicam due to reduced metabolic clearance. 1
Recommended Monitoring
Complete blood cell count and chemistry profile; occult blood loss; periodic liver function tests; renal function (urine output, serum urea nitrogen and creatinine); signs or symptoms of GI bleeding; blood pressure (baseline and periodically during therapy); and periodic ophthalmologic exam with long-term therapy. 1
Monitoring of renal function is recommended in patients with preexisting renal or hepatic impairment, heart failure, dehydration, or hypovolemia. 1
If anemia is suspected, monitor hemoglobin and/or hematocrit. 1
All patients should be monitored for signs of bleeding. 1
Dosing
The recommended meloxicam IV dose is 30 mg once daily. The injection should be given as an IV bolus over 15 seconds. Duration of treatment should be for the shortest period consistent with individual patient treatment goals. When initiating meloxicam IV, monitor patient analgesic response. If pain control is not adequate for the entire 24-hour dosing interval, a short-acting, non-NSAID, immediate-release analgesic should be used. 1
To reduce the risk of renal toxicity, it is important that the patient be well hydrated before the administration of meloxicam IV. 1
Meloxicam IV has not been studied in patients with hepatic impairment; no dosage adjustment is necessary in patients with mild to moderate hepatic impairment. 1
The pharmacokinetics of meloxicam IV were similar in patients with mild renal impairment and in healthy young subjects. Patients with moderate or severe renal impairment were not evaluated; meloxicam IV is not recommended for this population. Meloxicam IV is contraindicated in patients with moderate to severe renal insufficiency who are at risk for renal failure due to volume depletion. 1
Poor metabolizers of CYP2C9 substrates may have higher than anticipated meloxicam plasma concentrations. A lower dose of meloxicam may be necessary to decrease the risk of dose-related adverse effects. 1
Product Availability and Storage
Meloxicam IV was approved by the FDA on February 20, 2020. Meloxicam IV is available as a 1 mL fill (30 mg/mL) in a single-dose 2 mL vial. 1
Store meloxicam IV vials at 15°C to 25°C (59°F-77°F), with excursions permitted between 4°C to 30°C (40°F-86°F). The vials should not be frozen and should be protected from light. 1
Drug Safety/REMS
No REMS is required for meloxicam IV. 1
Conclusion
Meloxicam IV is approved for the management of moderate to severe pain in adults, for use alone or in combination with non-NSAID analgesics. The time to meaningful pain relief after IV bolus administration is 2 to 3 hours; therefore, non-NSAID analgesics with rapid onset of effect may be needed, for example, upon anesthetic emergence or resolution of local or regional anesthetic blocks. In addition, some patients may not experience adequate analgesia for the entire 24-hour dosing interval and may require administration of a short-acting, non-NSAID, immediate-release analgesic. There are no head-to-head comparison studies with injectable ketorolac.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.