
Abstract
Introduction
Dual antiplatelet therapy (DAPT) with aspirin and a P2Y12 inhibitor is standard of care for patients receiving intracoronary stents or after an acute coronary syndrome to prevent future cardiovascular events and stent thrombosis.1-3 A subset of these patients require additional therapy with anticoagulation, termed “triple-therapy,” most commonly for venous thromboembolism (VTE) or stroke prevention in atrial fibrillation (AF). Triple therapy can significantly increase patients’ risk of bleeding, reportedly up to 27%, compared to about 16% with dual antithrombotic therapy comprised of an anticoagulant and P2Y12 inhibitor.4-7 Determining the ideal antithrombotic therapy to balance risk of thrombosis and bleeding in patients requiring triple therapy can be challenging.
Current guideline recommendations support the use of ticagrelor or prasugrel over clopidogrel after stent placement or acute coronary syndrome (ACS)1,3,8 and direct-acting oral anticoagulants (DOACs) over warfarin for most patients with AF or VTE.9,10 However, clopidogrel is generally recommended in triple therapy because it is a lower potency antiplatelet agent, which may result in lower rates of bleeding in this high bleed risk population. 11 Ticagrelor or prasugrel may still be selected in practice for specific patients at high risk for stent thrombosis (eg, ACS), and the 2020 American College of Cardiology Expert Consensus Decision Pathway suggests ticagrelor may be selected in this scenario.
The DOACs have been compared to warfarin in randomized controlled trials assessing various triple therapy regimens, each of which have shown similar efficacy, but improved safety.4-7 Although these trials suggest that DOACs confer a lower risk of bleeding compared to warfarin in triple therapy regimens, direct application of these results to clinical practice is difficult due to inherent limitations in the studies. In one trial, many patients did not receive FDA approved doses of rivaroxaban for AF and 2 others did not contain a triple therapy arm receiving a DOAC.5-7 In each study, approximately 90% of patients were receiving clopidogrel as the P2Y12 agent, making extrapolation of results to prasugrel or ticagrelor treated patients challenging.4-7 Lastly, these studies only evaluated patients with AF and excluded other common indications for anticoagulation. Therefore, the objective of this study was to compare bleeding rates between warfarin, apixaban, or rivaroxaban treated patients receiving FDA approved dosages as part of a triple therapy regimens including aspirin and a P2Y12 inhibitor in a real-world cohort.
Methods
Study Design, Setting, and Patient Population
This study was a multi-site, retrospective cohort study of patients admitted to a Western New York hospital system from January 1, 2014 to September 1, 2017. This study was approved by the institutional review board (IRB) at the University at Buffalo.
Patients were identified using medication charge data for a combination of aspirin, a P2Y12 inhibitor, and an oral anticoagulant during a single admission for hospitalization or elective procedure based on a request through clinical decision support. Adult patients discharged on triple antithrombotic therapy after hospital or elective procedure admission were included. Patients were excluded if they were on a triple therapy regimen prior to admission, if triple therapy was discontinued or changed to dual therapy prior to discharge, or if dabigatran or edoxaban was the DOAC used (due to low utilization).
Data Collection
Patient demographic and clinical characteristics were recorded. Antithrombotic therapy use was documented including the planned duration for each therapy when applicable. The presence of past medical events or comorbidities associated with increased bleeding or thrombotic risk and non-steroidal anti-inflammatory drug (NSAID) use was collected for each patient. Hemoglobin, platelets, serum creatinine, bilirubin, aspartate aminotransferase, alanine aminotransferase, and albumin were collected on hospital admission.
Outcomes
The primary outcome compared bleeding rates between oral anticoagulant treatment groups within 90 days identified by chart review on initial presentation, or upon representation to a facility in the health system within 90 days of triple therapy regimen initiation. The secondary outcome was a comparison of bleeding rates between P2Y12 agents identified in the same manner as above. Bleeding was classified according to International Society on Thrombosis and Hemostasis (ISTH) criteria for major or clinically-relevant nonmajor bleeding. 12 Major bleeding was defined as bleeding resulting in a 2-unit (g/dL) or greater drop in hemoglobin from the patient’s baseline prior to bleed or greater than or equal to 2 units of red blood cells (RBC) transfused; bleeding into a critical organ (intracranial, intraspinal, intraocular, retroperitoneal, intra-articular, pericardial, or intramuscular with compartment syndrome); or a fatal bleed. Clinically-relevant nonmajor bleeding was defined as any sign or symptom of bleeding not fitting the definition of major bleeding but requiring an emergency department (ED) visit or hospital admission, or medical or surgical intervention for bleeding, or change in physician-directed antithrombotic therapy. Length of stay was defined as the hospitalization duration on initial presentation.
Statistical Analysis
Descriptive statistics were used to present demographic data and clinical characteristics. Categorical data were analyzed using χ2 or Fisher’s exact test as appropriate. Two-group continuous variables were analyzed with the Student’s t-test or Mann–Whitney U test and 3 group comparisons were analyzed using One-way ANOVA or Kruskal-Wallis test as appropriate. A P-value of less than .05 was considered statistically significant. Multivariable logistic regression was used to test the association between bleeding and antithrombotic use. Variables with a bivariate P-value of ≤.25 were evaluated for model inclusion, and collinearity was assessed with a variance inflation factor. Backward stepwise elimination was used to select factors significantly associated with bleeding. Confounding was tested by examining the effect of the individual factors on the parameter estimates in the final model. Model fit was assessed using the Hosmer-Lemeshow goodness-of-fit test. Data analyses were completed using SAS, version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
In the study period, 1606 admissions were identified as having inpatient charges for aspirin, a P2Y12 inhibitor, and an oral anticoagulant. Of those admissions, 1234 admissions were excluded, most (n = 902) due to triple therapy discontinuation prior to discharge. The remaining 372 unique patients comprised the study population with demographic and clinical characteristics depicted in Table 1. A majority of patients were on anticoagulation prior to admission and initiated on DAPT for percutaneous intervention (PCI) (n = 219, 58.9%). Of the patients that were on DAPT prior to admission, the most common indications for anticoagulation were new onset AF or VTE. There were 238 patients who received warfarin, 63 who received rivaroxaban, and 71 who received apixaban; and 321 who received clopidogrel, 39 who received ticagrelor, and 12 who received prasugrel. Almost all DOAC dosing were appropriate based on FDA labeled doses and renal adjustments (n = 121/134, 90.3%). The most common apixaban dosing was 5 mg twice daily (n = 58/71, 81.7%) and rivaroxaban was 20 mg daily (n = 44/63, 70.0%). Most baseline characteristics were not statistically significantly different between groups.
Baseline Characteristics.
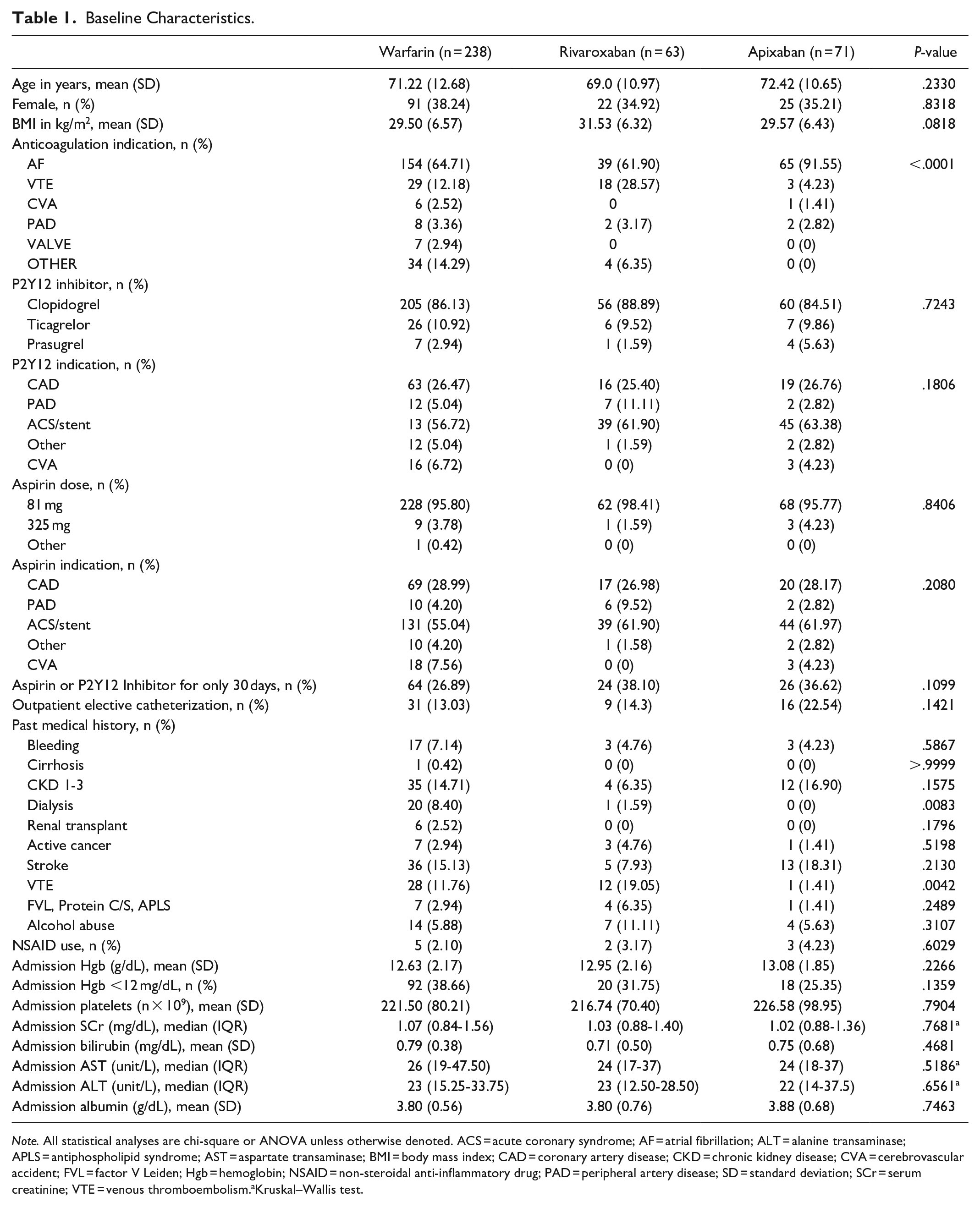
Note. All statistical analyses are chi-square or ANOVA unless otherwise denoted. ACS = acute coronary syndrome; AF = atrial fibrillation; ALT = alanine transaminase; APLS = antiphospholipid syndrome; AST = aspartate transaminase; BMI = body mass index; CAD = coronary artery disease; CKD = chronic kidney disease; CVA = cerebrovascular accident; FVL = factor V Leiden; Hgb = hemoglobin; NSAID = non-steroidal anti-inflammatory drug; PAD = peripheral artery disease; SD = standard deviation; SCr = serum creatinine; VTE = venous thromboembolism.aKruskal–Wallis test.
Forty-five patients experienced a bleeding event, 25 of which (55.6%) experienced a major bleed, 4 being fatal (16.0%) (Table 2). Most bleeds (n = 29, 64.4%) occurred within 30 days of discharge, requiring readmission or a visit to the ED. The total rate of bleeding was 12.2% (n = 29) with warfarin, 14.3% (n = 9) with rivaroxaban, and 9.9% (n = 7) with apixaban, which was not different between groups (P = .7335). No patients in the apixaban or rivaroxaban group received a reversal agent for their bleed, while 5.0% (n = 12) in the warfarin group did. Five percent (n = 12) of warfarin users, 9.5% (n = 6) of rivaroxaban users, and 7.0% (n = 5) of apixaban treated patients required a transfusion of at least 2 units of PRBCs. In clopidogrel treated patients, the rate of bleeding was 11.2% (n = 36), ticagrelor was 12.8% (n = 5), and prasugrel was 33.3% (n = 4), P = .0691. Patients who bled were more likely to have a past medical history of bleeding compared to those without a bleed [13.3% (n = 6/45) vs. 5.2% (n = 17/327), P = .0336], and a lower mean ± SD index admission hemoglobin (12.21 ± 2.07 g/dl vs 12.85 ± 2.11 g/dl, P = .0591); respectively. Patients who bled had a significantly longer median [interquartile range (IQR)] index length of stay (LOS) [6 days (3-11.5) vs 4 days (2-7), P = .0057)], although when patients who bled during the index admission were removed from the comparison, the median (IQR) LOS between those with and without a bleeding event was no longer statistically significant [5 days (3-9) vs 4 days (2-7), P = .1388].
Clinical Outcomes.
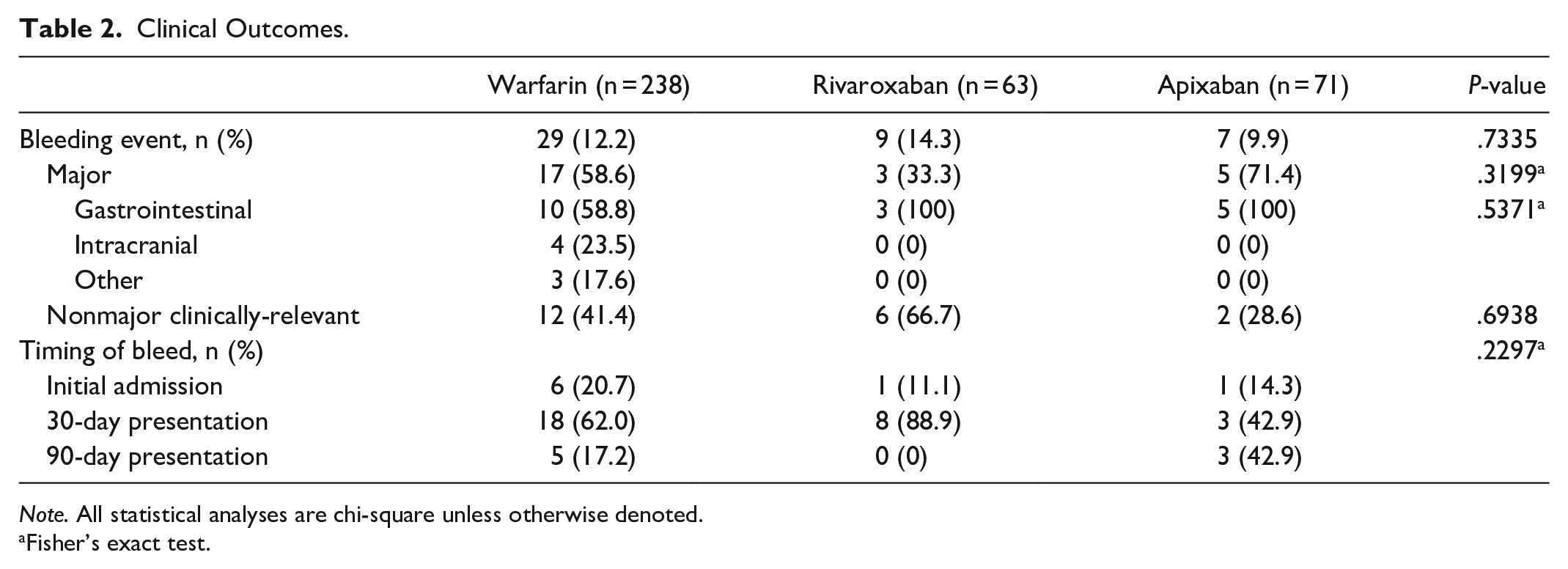
Note. All statistical analyses are chi-square unless otherwise denoted.
Fisher’s exact test.
In the multivariable model, 6 variables with P-values ≤.25 were evaluated for inclusion in addition to the primary outcome: P2Y12 inhibitor used, LOS, bleeding history, history of VTE, admission hemoglobin, and admission albumin. Many patients did not have an admission albumin level (n = 101, 27.2%), and therefore could not reliably be assessed in the model. Similarly, longer index admission LOS could have been the result of bleeding during admission and was removed from model consideration. The use of prasugrel versus clopidogrel and admission hemoglobin were identified as statistically significant risk factors associated with bleeding in the model (Table 3).
Multivariable Logistic Regression of Factors Associated with Bleeding.
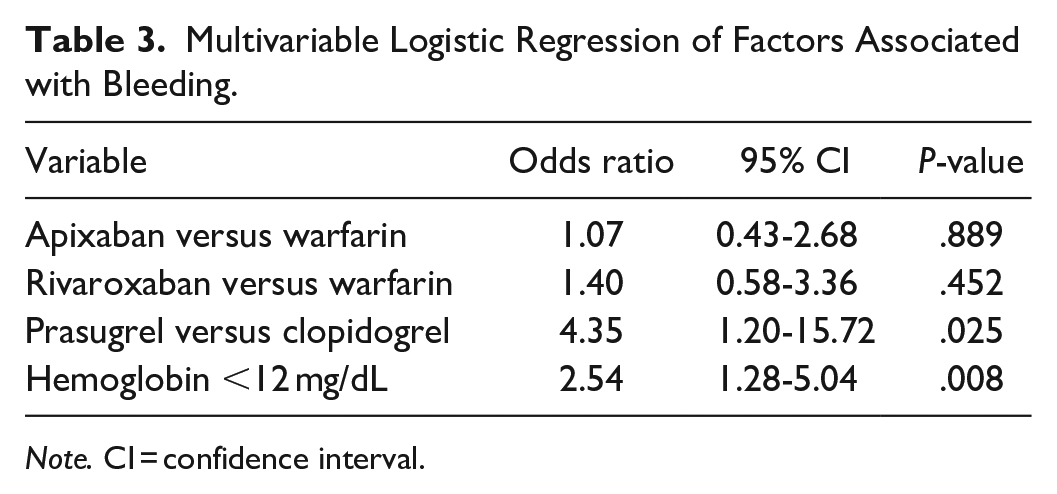
Note. CI = confidence interval.
Discussion
In this real-world retrospective cohort analysis of patients receiving triple therapy with an oral anticoagulant, P2Y12 inhibitor, and aspirin, bleeding rates did not differ significantly between patients treated with different oral anticoagulants. In the multivariable model, patients with a hemoglobin less than 12 had an over 2.5-fold increased risk of bleeding, and those receiving prasugrel had an over 4-fold increased risk of bleeding compared to patients receiving clopidogrel. Data in this study reflect patients who are continued on triple therapy for at least 30 days after admission. Though not recommended for most patients, this does occur in high risk patients and/or inadvertently due to the complexity of medication regimens and inaccurate accounting for aspirin since it does not require a prescription. As such, the investigators sought to evaluate bleed risk in patients prescribed triple therapy for at least 30 days to better quantify bleed risk and improve antithrombotic agent selection in this scenario. The timeline of bleeding events in our study support current guidance to stop aspirin therapy at the time of discharge as most events occurred within 30 days of discharge, during the timeframe that all 3 antithrombotic agents were continued in this study. In the 8 patients that experienced a bleeding event between days 31 and 90, all were instructed to continue triple therapy beyond 30 days.
Bleeding rates did not differ based on oral anticoagulant use in this investigation, in contrast with previously published randomized controlled trials.4,6 The PIONEER AF-PCI trial studied patients with AF undergoing PCI requiring a combination of antithrombotic therapies. 6 Of the 3 groups studied: rivaroxaban 15 mg daily plus a P2Y12 inhibitor, rivaroxaban 2.5 mg daily plus DAPT, and warfarin plus DAPT; rates of clinically significant Thrombolysis in Myocardial Infarction (TIMI) bleeding were 16.8% (n = 109), 18.0% (n = 117), and 26.7% (n = 167); respectively (all comparison P-values < .001). The two-by-two factorial design of the AUGUSTUS trial investigated patients with AF who had an acute coronary syndrome and compared apixaban plus DAPT, warfarin plus DAPT, apixaban plus a P2Y12 inhibitor, and warfarin plus a P2Y12 inhibitor. 4 Patients receiving apixaban had lower rates of major or clinically relevant nonmajor ISTH bleeding compared to those receiving warfarin [10.5% (n = 241) vs 14.7% (n = 332); P < .001]. In patients who received DAPT, the bleeding rate with apixaban was 13.8% (n = 158/1145) and 18.7% (n = 210/1123) with warfarin. Both PIONEER AF-PCI and AUGUSTUS determined that triple or dual antithrombotic therapy utilizing warfarin led to higher rates of bleeding compared to apixaban or rivaroxaban.4,6 Importantly, the doses of rivaroxaban used with DAPT in the PIONEER-AF PCI trial are lower than the approved doses for VTE or AF which may underestimate the risk of bleeding using rivaroxaban in triple therapy regimens. 6 Additionally, different definitions of bleeding were used, including minor bleeding, which is not directly comparable with our study. In the AUGUSTUS trial, outcomes were assessed at 6 months, in contrast to our study where outcomes were assessed for only 90 days. 4 This could account for a lower incidence of bleeding in our study compared to AUGUSTUS. A higher rate of bleeding was seen in warfarin treated patients compared to apixaban; however, the difference was not significant in our investigation as it was in AUGUSTUS, likely due to the small sample size.
It is recognized that without anticoagulation, both ticagrelor and prasugrel have an increased risk of bleeding compared to clopidogrel.13-15 Unfortunately, landmark trials assessing antithrombotic regimens in patients with AF who undergo a PCI or experience ACS have largely used clopidogrel as the P2Y12 agent of choice (>90%) making direct comparisons between clopidogrel and non-clopidogrel containing triple therapy regimens difficult.4-7 In one observational trial assessing clopidogrel (n = 526) compared to prasugrel (n = 91) in triple therapy, patients receiving prasugrel had a higher rate of patient-reported bleeding compared to clopidogrel (39% vs 24.4%; adjusted RR 2.37; 95% CI 1.36-4.15; P = .003). 16 This aligns with the higher bleed risk seen with prasugrel containing regimens in our study. Ticagrelor or prasugrel (n = 42) were retrospectively compared to clopidogrel (n = 126) in patients receiving triple antithrombotic therapy. Receipt of ticagrelor or prasugrel increased risk of any bleeding event compared to clopidogrel (28.6% vs 12.7%; OR 3.3; 95% CI 1.38-8.34), though results were not further broken into ticagrelor versus prasugrel groups, likely due to the small number of patients. 17 Our study did not find a difference in patients receiving ticagrelor as a component of triple therapy, which supports the current guidance that ticagrelor may be used in triple antithrombotic regimens in patients at high risk of stent thrombosis, however the relatively small number of ticagrelor treated patients in our investigation should be noted. 11
Baseline hemoglobin was an additional factor associated with an increased risk of bleeding. Over half of the patients who experienced a bleeding event had anemia (hemoglobin < 12 g/dL) at baseline and this was confirmed to be an associated risk factor for bleeding in the multivariable regression model. Interestingly, hemoglobin is not included in the HAS-BLED score when assessing patients baseline risk for bleeding before initiation of anticoagulation. 18 Moreover, neither the PIONEER-AF PCI or the AUGUSTUS trial report baseline hemoglobin to determine if there was an association with bleeding events.4,6 A pooled analysis of 3 trials assessing patients undergoing PCI grouped patients into 4 different hemoglobin categories (high-normal, low-normal, mild anemia, and moderate/severe anemia): ≥14 g/dL in men and women (high-normal); 13-13.9 g/dL in men and 12-13.9 g/dL in women (low-normal); 11-12.9 g/dL in men and 11-11.9 g/dL in women (mild anemia); and <11 g/dL in women and men (moderate/severe anemia). 19 Patients with low-normal hemoglobin, mild anemia, and moderate/severe anemia were each associated with Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Arteries Trial (GUSTO) moderate/severe bleeding with an adjusted hazard ratio (HR) of 1.22 (95% CI, 1.04-1.44), 1.73 (95% CI, 1.47-2.04), and 2.31 (95% CI, 1.92-2.78); respectively. Further, a post-hoc analysis of the Apixaban for Reduction in Stroke and Other Thromboembolic Events in AF (ARISTOTLE) trial assessed the presence of anemia to determine if anemia was associated with bleeding events in patients receiving apixaban. 20 The presence of anemia led to a 1.9-fold higher incidence of ISTH major bleeding events, and each 1 mg/dL lowering of hemoglobin increased the risk of ISTH major bleeding by 29%. Lastly, the European Society of Cardiology recently published a new guideline for the treatment of AF and include hemoglobin < 10 mg/dL as a risk factor for the bleeding. 21
The real-world nature of this study with triple therapy durations similar to the large scale, landmark, randomized controlled trials evaluating patients with AF and ACS/PCI is a strength of this investigation.4-7 Our data can be more directly applied and compared to these large trials which would be difficult if our study patients had discontinued aspirin therapy at discharge. 11 Further, our data adds to the triple therapy literature in that we included patients with all indications for anticoagulation including a large percentage (30.6%) of patients with non-AF indications.
There are several limitations to consider for this study. In regards to differences in baseline characteristics, almost all patients on dialysis were treated with warfarin. This is likely due to the drug labeling for patients with ESRD at the time of the study. ESRD was not associated with bleeding in this analysis, likely due to the small numbers of patients with this comorbidity. Indications for anticoagulation were also slightly different between treatment groups. Factors such as time within therapeutic range and proton pump inhibitor use were not collected, which may have ultimately impacted bleeding outcomes. Notably, patients who experienced a bleeding event and presented to their primary care physician, urgent care, or outside of the health system were not captured. It is also possible that patients could have expired in the 90-day post discharge time frame and were incorrectly labeled as not readmitted, since mortality data after discharge was not readily available. Due to the overall low number of included patients in our study compared to the large-scale, randomized controlled trials, it is also possible that there was no observed difference in bleeding between treatment groups. Although this study did show a higher rate of bleeding in patients receiving prasugrel, the relative number of patients receiving prasugrel was low (n = 12), which requires validation in a larger population.
Conclusion and Relevance
Differences between bleeding rates among patients on varying oral anticoagulants were not significant in this multisite, single-health system cohort of patients on triple antithrombotic therapy. Higher bleeding rates were observed in prasugrel treated patients and patients with a hemoglobin less than 12 mg/dL in a multi-variable model; however, the number of prasugrel treated patients was low requiring additional larger studies to determine optimal triple antithrombotic therapy.
Research Data
sj-xlsx-1-hpx-10.1177_00185787211024602 – for Comparison of Bleeding Rates between Oral Anticoagulants in Combination with Dual Antiplatelet Therapy (Triple Therapy) in a Real-World Cohort
sj-xlsx-1-hpx-10.1177_00185787211024602 for Comparison of Bleeding Rates between Oral Anticoagulants in Combination with Dual Antiplatelet Therapy (Triple Therapy) in a Real-World Cohort by Maya R. Chilbert, Sarah E. Reidy, Collin M. Clark, Marissa Guszkowski, Emma Gargala and Ashley E. Woodruff in Hospital Pharmacy
Footnotes
Authors’ Note
Previous presentation of this work occurred virtually at the American College of Clinical Pharmacy Annual Meeting 2020.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Sarah E Reidy, Collin M Clark, Marissa Guszkowski, Emma Gargala, Ashley E Woodruff. The first draft of the manuscript was written by Maya Chilbert, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Approved by the Institutional Review Board at the University at Buffalo.
Availability of data and material
Uploaded with manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.