
Abstract
A 38-years-old female with an aortic valve replacement presented to an outside hospital (OSH) with fevers and malaise. Blood cultures revealed VRE which was resistant to linezolid, resistant to ampicillin, non-susceptible to daptomycin (MIC of 8 mcg/mL), and exhibited susceptibility to gentamicin. The patient was therefore initiated on intravenous (IV) daptomycin 6 mg/kg q24h and gentamicin IV 1 mg/kg q8h. However, after 14 days of therapy with daptomycin and gentamicin, the patient was transferred to our institution for the management of cardiogenic shock and hypoxemic respiratory failure. Given the concern for treatment failure, her antimicrobial regimen was changed to IV chloramphenicol 12.5 mg/kg every 6 hours with IV daptomycin 10 mg/kg every 48 hours given an estimated creatinine clearance of 30 mL/minutes. In vitro susceptibilities for chloramphenicol were performed which confirmed susceptibility. A transesophageal echocardiogram revealed a possible abscess at the left coronary cusp and aortic valve dehiscence. The patient underwent aortic valve replacement with aortic root reconstruction. The aortic valve culture grew VRE susceptible to linezolid but resistant to ampicillin and doxycycline. The patient was deemed clinically cured after 42 days of combination therapy with daptomycin and chloramphenicol. After 6 years of follow-up, the patient has not had a recurrent VRE infection. To our knowledge, this is the first case of endocarditis secondary to VRE that was successfully managed with the combination of daptomycin and chloramphenicol.
Keywords
Introduction
For over 2 decades, Enterococcus spp. have been recognized as a significant cause of hospital acquired infection and account for approximately 10% of cases.1-3 This is concerning given Enterococcus are the second most common cause of infective endocarditis (IE) and those who develop invasive infections due to Enterococcus spp. are often elderly, immunosuppressed, and are burdened with several co-morbid conditions.3-5 To make matters worse, up to 80% of E. faecium are vancomycin resistant in the United States, which significantly limits our armamentarium of antimicrobials that are active against this pathogen. 6
For the treatment of IE secondary to VRE, few antimicrobial agents have been shown to be efficacious. Current guidelines suggest utilizing linezolid or daptomycin for IE caused by VRE; however, VRE has been documented to demonstrate resistance to both antimicrobials.5,7,8 Furthermore, linezolid use is limited by the risk of drug-drug interactions, neuropathy, ocular toxicities, and myelosuppression that occurs with prolonged use. 9
Chloramphenicol, a bacteriostatic agent against VRE, has been shown to be effective in the management of VRE blood stream infections.10-12 However, therapy with chloramphenicol for the treatment IE caused by VRE is limited to case reports which describe inconsistent antimicrobial combination regimens with conflicting outcomes.13-15 In an effort to better elucidate the role of chloramphenicol in the treatment of IE, we report a novel case of IE secondary to VRE which was successfully managed with daptomycin and chloramphenicol.
Case Report
A 38-years-old female underwent an aortic valve replacement (AVR) with a mechanical valve for the treatment of aortic stenosis. Her course was complicated by persistent VRE (E. faecium) bacteremia which was susceptible to linezolid and managed with a 6-week course of oral linezolid. Approximately 9 months following aortic valve replacement, she had presented to an outside hospital (OSH) with fevers and malaise. Blood cultures revealed VRE which was resistant to linezolid (<20 mm by disk diffusion), resistant to ampicillin (<16 mm by disk diffusion), and non-susceptible to daptomycin (ETEST® MIC of 8 mcg/mL). 16 The patient was therefore initiated on intravenous (IV) daptomycin 6 mg/kg q24h and gentamicin IV 1 mg/kg q8h. However, after 14 days of therapy with daptomycin and gentamicin, the patient was transferred to our institution for the management of cardiogenic shock and hypoxemic respiratory failure.
Upon admission, she was mechanically intubated for inadequate oxygen saturations despite noninvasive methods and started on a fentanyl drip. She was also hemodynamically unstable requiring IV norepinephrine, epinephrine, and vasopressin to maintain a MAP of 65 mmHg. Blood cultures were drawn which revealed no growth. Given the concern for possible treatment failure on day 1 of hospitalization, her antimicrobial regimen was modified to IV chloramphenicol 12.5 mg/kg every 6 hours with IV daptomycin 10 mg/kg every 48 hours given an estimated creatinine clearance (eCrCl) of 30 mL/minutes. Gentamicin was discontinued on day 1 of hospitalization due to acute renal injury. In vitro susceptibilities of chloramphenicol were performed on the VRE bloodstream isolate from the OSH which confirmed susceptibility to chloramphenicol (18 mm by disk diffusion). A transesophageal echocardiogram revealed a possible abscess at the left coronary cusp and an area of echolucency between the valve apparatus and aortic root in the region of the native non-coronary cusp, consistent with valve dehiscence. Subsequently, the patient was taken to the operating room for aortic valve replacement with a 21 mm Trifecta™ biologic valve and aortic root reconstruction using bovine pericardial patch. The aortic valve culture grew VRE susceptible to linezolid but resistant to ampicillin and doxycycline. The isolate had a daptomycin MIC of 4 mcg/mL (ETEST®) and a tigecycline MIC of 0.25 mcg/mL (ETEST®). On day 5 of hospitalization, the patient was noted to have an asymptomatic creatine kinase (CK) of 1320 U/L. Since daptomycin was being administered at a dose of 10 mg/kg every 48 hours and none of the patient’s other medications were suspected to cause an elevation in CK, daptomycin was discontinued and the patient was continued on chloramphenicol monotherapy. The patient was extubated on day 6 of hospitalization. Vasopressor requirements were titrated down and were ultimately discontinued on day 7 of hospitalization. On day 8 of hospitalization, the patient’s CK decreased to 109 U/L and, considering the recent adverse event, daptomycin was restarted at a lower dose of approximately 7 mg/kg every 48 hours in the setting of an eCrCl of 30 mL/minutes.
On day 15 of hospitalization, the patient was discharged on daptomycin and chloramphenicol for 27 more days to complete a 42 days course of therapy. On day 42 of therapy with daptomycin and chloramphenicol the patient was deemed clinically cured by an Infectious Diseases Physician. Since the patient was considered to have a high risk of relapse due to aortic valve replacement, she was closely monitored for several years. After 6 years of follow up, the patient has not had a recurrence of VRE infection.
Discussion
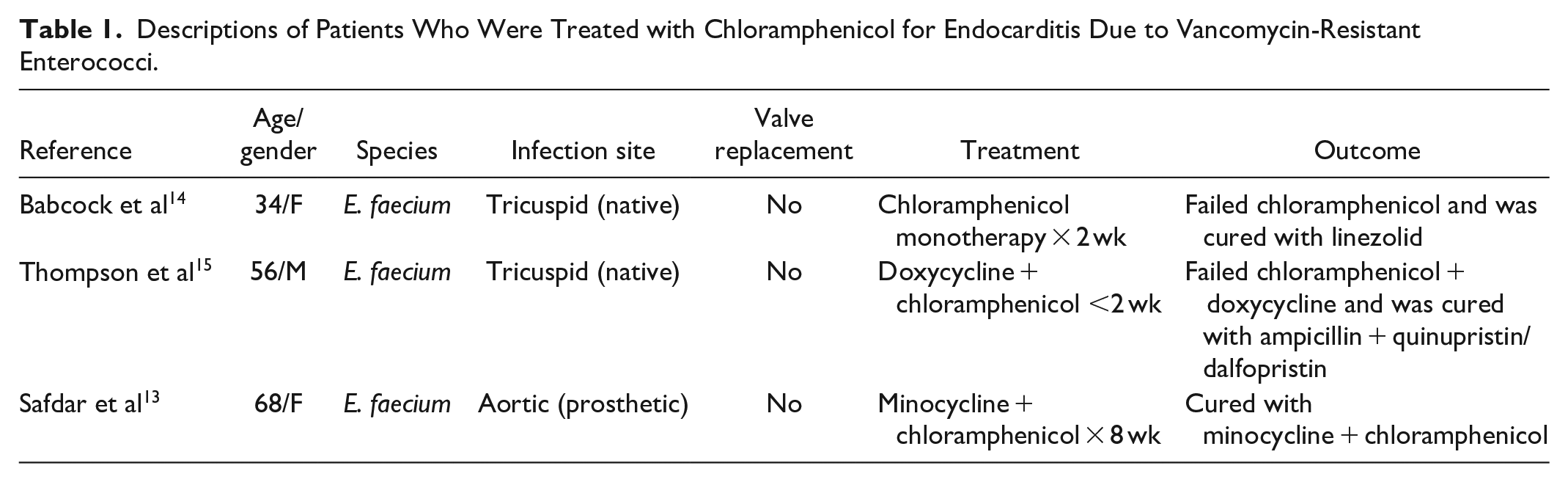
To our knowledge, this is the first reported case of IE secondary to VRE that was successfully managed with daptomycin and chloramphenicol and therefore represents a novel therapeutic option when first line agents cannot be used. Published observational studies have revealed that chloramphenicol has a 57% to 61% clinical response rate for the treatment of blood stream infections secondary to VRE.10-12 In order to identify the success rate of chloramphenicol for the treatment of IE secondary to VRE, a literature review of articles written in English was performed in MEDLINE, PUBMED, and Google Scholar, using the search terms “Enterococcus,” “Endocarditis,” and “Chloramphenicol” between 1988 and 2021. Cases were included if a definitive diagnosis of IE secondary to VRE was made by the Duke Criteria. 7 Although articles prior to this time frame were not included since VRE was not identified until 1988, anecdotal reports of chloramphenicol used for the treatment of IE secondary to vancomycin susceptible enterococcus are available and generally support combination therapy. 17 Otherwise, a total of 3 cases in which chloramphenicol was used for the treatment of IE secondary to VRE were identified (Table 1). Among these 3 cases of IE secondary to VRE, treatment failure occurred when administered in an adult patient who received chloramphenicol as monotherapy. 14 As for the remaining patients identified in the literature review, treatment success and treatment failure resulted when chloramphenicol was given in combination with minocycline and doxycycline, respectively.13,15
Descriptions of Patients Who Were Treated with Chloramphenicol for Endocarditis Due to Vancomycin-Resistant Enterococci.
While neither minocycline nor doxycycline susceptibilities were available for our patient’s case, the MIC to tigecycline from the VRE isolated from the patient’s aortic valve was 0.25 mcg/mL. Although no interpretive criteria for tigecycline and VRE breakpoints exist, an MIC of <0.25 mcg/mL is considered susceptible for vancomycin susceptible E. faecalis by the Food and Drug Administration. 18 No clinical studies have evaluated the role of tigecycline for IE, however, an anecdotal report notes its success in combination with daptomycin for the treatment of IE secondary to VRE. 19 Given the lack of clinical data for tigecycline for endovascular infections, the drug’s large volume of distribution resulting in low serum levels, and the elevated tigecycline MIC in our patient, the drug was avoided. 18 Additionally, in vitro antagonism against daptomycin non-susceptible Enterococci has been demonstrated with the combination of daptomycin and tigecycline. 20 Although this unique case would support the notion that daptomycin in combination with chloramphenicol is synergistic against enterococci, we are unaware of any in vitro or in vivo studies to confirm if the combination of daptomycin and chloramphenicol are indeed synergistic or antagonistic against the pathogen.
Prior to being transitioned to chloramphenicol in combination with daptomycin, our patient experienced treatment failure with daptomycin and gentamicin which was likely due to an elevated daptomycin MIC. Data supporting enhanced daptomycin bactericidal activity with the addition of gentamicin have been conflicting.21,22 The VRE isolate in the aortic valve culture exhibited a daptomycin MIC of 4 mcg/mL, whereas the bloodstream isolate possessed a daptomycin MIC of 8 mcg/mL. Although Etest® can slightly overcall daptomycin resistance compared to broth microdilution, it is interesting that the MIC of both isolates differed even though both were tested by Etest®. 23 Although Enterococcus spp. may possess mutations in LiaFSR rendering daptomycin non-susceptible at MICs of both 4 and 8 mcg/mL, current CLSI guidelines suggest that daptomycin doses of 8 to 12 mg/kg are effective in VRE isolates with an MIC of 4 mcg/mL.16,24 While this recommendation is controversial, 1 retrospective study of over 900 patients identified daptomycin doses of >10 mg/kg to be associated with improved survival and microbiological clearance in patients with VRE bloodstream infections. 25 Approximately 5% of VRE isolates had a daptomycin MIC available and most of these isolates were noted to have an MIC of 4 mcg/mL. Although high dose daptomycin was initiated in our patient in combination with chloramphenicol, an asymptomatic elevation in CK developed warranted temporary daptomycin discontinuation before reinitiating the drug at 7 mg/kg.
Although chloramphenicol is not recommended by the American Heart Association for the treatment IE as it is bacteriostatic against enterococci, the antimicrobial was required in our patient since the isolated VRE demonstrated susceptibility to chloramphenicol per Clinical and Laboratory Standards Institutes guidelines in the setting of resistance to first line agents.7,16 Concern for chloramphenicol induced blood dyscrasias has diminished routine use of the antimicrobial in the United States and stems from 2 landmark case reports.26,27 However, the true incidence of chloramphenicol induced blood dyscrasias is low with an estimated incidence of occurrence of once in every 24 000 to 40 000 patients, its routine use in the United States has diminished significantly. 28 Nevertheless, it is often not considered as a potential treatment option and it is noted that long term therapy with chloramphenicol was well tolerated in our patient.
In conclusion, we report a case of IE secondary to VRE that was successfully managed with daptomycin and chloramphenicol. In an era of increasing drug resistance in enterococci, chloramphenicol may be a useful option in the management of IE secondary to VRE when resistance precludes the use of first line agents. However, further investigation is warranted to confirm our experience.
Footnotes
ICMJE Statement
All authors meet criteria and acknowledge responsibility and accountability for this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.