
Abstract
Each month, subscribers to The Formulary Monograph Service receive 5 to 6 well-documented monographs on drugs that are newly released or are in late phase 3 trials. The monographs are targeted to Pharmacy & Therapeutics Committees. Subscribers also receive monthly 1-page summary monographs on agents that are useful for agendas and pharmacy/nursing in-services. A comprehensive target drug utilization evaluation/medication use evaluation (DUE/MUE) is also provided each month. With a subscription, the monographs are available online to subscribers. Monographs can be customized to meet the needs of a facility. Through the cooperation of The Formulary, Hospital Pharmacy publishes selected reviews in this column. For more information about The Formulary Monograph Service, contact Wolters Kluwer customer service at 866-397-3433.
Indications
Belumosudil is indicated for the treatment of adults and pediatric patients 12 years and older with chronic graft-versus-host disease (GVHD) after failure of at least 2 prior lines of systemic therapy. 1
Chronic GVHD occurs in 30% to 70% of allogeneic hematopoietic cell transplant (HCT) patients and is the most common late complication post-HCT. Patients with chronic GVHD are at increased risk for late complications post-HCT, including metabolic syndrome, infections, renal or hepatic impairment, and secondary cancers. Chronic GVHD primarily affects mucocutaneous, respiratory, and musculoskeletal systems, often affecting multiple organs. Characteristic features resemble autoimmune conditions, resulting in sclerosis, fibrosis, and generalized inflammation. The mechanisms for the development of chronic GVHD are distinct from those of acute GVHD, although corticosteroids are the primary therapy for both. Chronic GVHD has 3 phases: (1) acute inflammation and direct tissue endothelial damage; (2) chronic inflammation; and (3) impaired tissue repair, wound healing, and release of profibrotic mediators. Prophylactic strategies have included use of a calcineurin inhibitor plus methotrexate, as well as several investigational strategies incorporating antithymocyte globulin and posttransplant cyclophosphamide. Mild manifestations of chronic GVHD may be managed with topical corticosteroids or calcineurin inhibitors. Moderate to severe disease requires the addition of systemic therapies. The standard initial systemic therapy is prednisone 1 mg/kg/day with or without a calcineurin inhibitor. Other combinations have not demonstrated superiority over prednisone-based regimens for initial therapy. Agents used in the treatment of steroid-refractory chronic GVHD have included ibrutinib, ruxolitinib, interleukin 2 (IL-2), proteasome inhibitors, and belumosudil. 2 The Bruton tyrosine kinase inhibitor ibrutinib is FDA approved for the treatment of chronic GVHD in adults after 1 or more lines of systemic therapy have failed. Ibrutinib is also approved for the treatment of mantle cell lymphoma, chronic lymphocytic leukemia/small lymphocytic lymphoma with or without 17p deletion, Waldenström macroglobulinemia, and marginal zone lymphoma. 3
Belumosudil is also being evaluated in clinical trials for the treatment of idiopathic pulmonary fibrosis and diffuse cutaneous systemic sclerosis. Several trials investigating a role in treatment of psoriasis have been completed. 4
Clinical Pharmacology
Belumosudil is an oral selective Rho-associated coiled-coil-containing protein kinase 2 (ROCK2) inhibitor.1,5 ROCKs/Rho-kinases are serine/threonine kinases introduced as downstream effectors of the small GTPase Rho. ROCKs are involved in a variety of cellular events, including actin cytoskeleton organization, cytokinesis, differentiation, apoptosis, glucose metabolism, cell adhesion/motility, and inflammation.6,7 ROCK2 inhibition leads to downregulation of signal transducer and activator of transcription 3 (STAT3) phosphorylation. Belumosudil has been associated with increasing CD4+ regulatory T (Treg) cells and decreasing type 17 helper T (Th17) cells, as well as with reducing secretion of IL-21, IL-17, and interferon gamma, which have been implicated in chronic GVHD and other autoimmune disorders.5,7-11 Selective ROCK2 inhibition also restores immune homeostasis by shifting the Th17/Treg cell balance via a signal transducer and activator of transcription 5 (STAT5)-dependent mechanism and has also been observed to impact fibrotic manifestations of disease. 8 Belumosudil has also been observed to suppress adipocyte differentiation and adipogenesis, but by modulation of key factors activated at the intermediate stage of differentiation rather than as a result of ROCK2 inhibition. 6 Belumosudil has 100-fold selectivity for ROCK2 over ROCK1.1,8
ROCK2 inhibition has been associated with decreased inflammation, restored immune homeostasis, and decreased fibrosis, suggesting potential effects in GVHD and other autoimmune or fibrotic diseases including psoriasis, rheumatoid arthritis, systemic lupus erythematosus, and systemic sclerosis.5,10-12 Belumosudil has been shown to ameliorate GVHD in several animal models.9,12 It has also demonstrated activity in patients with psoriasis. 13
Pharmacokinetics
Following oral administration, belumosudil Cmax and AUC increased in an approximately proportional manner over a dosage range of 200 to 400 mg. Median Tmax at steady state was 1.26 to 2.53 hours. Mean bioavailability was 64% following a single dose. Administration of a single belumosudil dose with a high-fat and high-calorie meal in healthy subjects increased Cmax and AUC 2.2 times and 2 times, respectively, compared with administration in the fasted state; median Tmax was delayed 0.5 hours. 1
Mean volume of distribution after a single dose was 184 L. In vitro, belumosudil exhibited extensive binding to human serum albumin (99.9%) and human alpha 1-acid glycoprotein (98.6%). 1
Mean elimination half-life of belumosudil was 19 hours, and clearance was 9.83 L/hour in patients with chronic GVHD. In vitro, belumosudil is primarily metabolized by CYP3A4 and to a lesser extent by CYP2C8, CYP2D6, and UGT1A9. Following a single oral radiolabeled dose in healthy subjects, 85% of radioactivity was recovered in the feces (30% as unchanged drug) and less than 5% was recovered in the urine. 1
No clinically significant differences in belumosudil pharmacokinetics were observed with regard to age (18-77 years), sex, weight (38.6-143 kg), or mild to moderate renal impairment (estimated glomerular filtration rate 30-90 mL/minute/1.73 m2). Belumosudil pharmacokinetics have not been assessed in patients with severe renal impairment. 1 The FDA is requiring a study to assess belumosudil pharmacokinetics in subjects with mild, moderate, and severe hepatic impairment, as well as a pharmacokinetic study among US racial and ethnic groups. 14
Comparative Efficacy
Indication: Chronic Graft-Versus-Host Disease
Studies
Overall response rate (ORR), defined as the proportion of patients who achieved a complete response or partial response per 2014 National Institute of Health (NIH) Chronic GVHD Consensus Criteria, was 65% (95% CI, 51%-77%) in the entire safety population (N = 54).
ORR by cohort: 65% (95% CI, 38%-86%) in cohort 1, 69% (95% CI, 41%-89%) in cohort 2, and 62% (95% CI, 38%-82%) in cohort 3. ORR by key subgroup: 60% (25 of 42 patients) in those with severe chronic GVHD, 66% (23 of 35 patients) in those who had received at least 2 prior systemic lines of therapy, 63% (22 of 35 patients) in those who were refractory to their last line of therapy, and 70% (19 of 27 patients) in those with 4 or more organs involved.
All responses at the patient level were partial; however, organ-specific analyses showed that complete response was achieved across all affected organs, with the exception of the lungs, where partial response was the best response achieved. Median Kaplan-Meier duration of response was 35 weeks overall and 38 weeks for patients who had received 2 or more prior systemic lines of therapy.
Kaplan-Meier median time to next treatment was 14 months. Subsequent therapies included tacrolimus, sirolimus, ibrutinib, ruxolitinib, extracorporeal photopheresis, and mycophenolate mofetil.
Response rate by organ system varied from complete response rates of 100% for upper (n = 6) and lower (n = 2) GI involvement to a partial response rate of less than 30% and no complete response for lung involvement (n = 12).
Lee Symptom Scale (LSS) score was improved to a clinically meaningful extent (defined as a decrease of at least 7 points) in 50% of patients.
Corticosteroid dose reductions were accomplished in 67% of patients, and corticosteroids were discontinued in 19%. Mean corticosteroid dose was reduced by 45% (55% in responders; 26% in nonresponders). Median time to corticosteroid discontinuation was 29 weeks (range, 8-77 weeks).
Failure-free survival (FFS) rate, defined as the time from the first belumosudil dose to a failure event, was 76% (95% CI, 62%-85%) at 6 months, 47% (95% CI, 33%-60%) at 12 months, and 33% (95% CI, 21%-46%) at 24 months. Failure events included initiation of a new systemic therapy (n = 27), relapse of the underlying disease (n = 7), and death (n = 2).
Overall survival rate was 91% (95% CI, 79%-96%) at 12 months and 82% (95% CI, 69%-90%) at 24 months.
Best ORR, defined as the proportion of patients achieving complete response or partial response at any time per 2014 NIH Consensus Criteria, was 74% (95% CI, 62%-84%) in the once-daily arm and 77% (95% CI, 65%-87%) in the twice-daily arm.
Patients previously treated with ruxolitinib: ORR was 68% (95% CI, 51%-83%). Patients previously treated with ibrutinib: ORR was 74% (95% CI, 59%-86%). Best ORR did not significantly differ when assessed by subgroups based on dose frequency (once or twice daily), severity of chronic GVHD at screening (severe or not severe), best response to last systemic line of therapy (refractory or nonrefractory), number of organs involved at baseline (less than 4 or 4 or more), and concomitant use of proton pump inhibitors. In the modified intention-to-treat population, best ORR by affected organs was 37% for skin, 42% for eyes, 55% for the mouth, 39% for the liver, 26% for lungs, 71% for joints/fascia, 52% for upper GI tract, 69% for lower GI tract, and 45% for the esophagus. Seven patients achieved a complete response in all affected organs.
Duration of response was 20 weeks or more in 59% of responders. Median duration of response was 54 weeks in the responder population.
Median time to response was 5 weeks (range, 4-66 weeks); 91% of responses occurred within 6 months of treatment, and the remaining 9% were seen after 6 to 12 months of treatment.
LSS summary score was improved to a clinically meaningful extent in 59% of patients treated with belumosudil once daily and in 62% of those treated with belumosudil twice daily. Clinically meaningful improvements in symptom scores were observed in responders (69% and 71% with once-daily and twice-daily dosing, respectively) and nonresponders (29% and 33%, respectively).
FFS rate was 73% (95% CI, 61%-83%) in the once-daily group and 76% (95% CI, 63%-84%) in the twice-daily group at 6 months and 57% (95% CI, 44%-68%) in the once-daily group and 56% (95% CI, 43%-67%) in the twice-daily group at 12 months.
During belumosudil treatment, 65% of patients reduced their corticosteroid dose (64% in the once-daily group and 67% in the twice-daily group). The mean dose was reduced by 45% in the modified intention-to-treat population and by 54% in responders. Corticosteroid discontinuation occurred in 21% of patients (20% in the once-daily group and 23% in the twice-daily group); calcineurin inhibitor discontinuation occurred in 22% of those patients.
The 2-year overall survival rate was 89% (95% CI, 82%-93%).
Contraindications, Warnings, and Precautions
Contraindications
The belumosudil prescribing information states there are no contraindications to its use. 1 Though not stated in the product labeling, a potential contraindication is hypersensitivity to belumosudil or any of its inactive ingredients (ie, microcrystalline cellulose, hypromellose, croscarmellose sodium, colloidal silicon dioxide, magnesium stearate, polyvinyl alcohol, polyethylene glycol, talc, titanium dioxide, yellow iron oxide). 1 In clinical trials, patients taking moderate or strong inhibitors or inducers of CYP3A4 were excluded, as were patients with known hypersensitivity to belumosudil or other ROCK2 inhibitors. 15
Warnings and Precautions
Belumosudil can cause fetal harm if administered during pregnancy. In animal studies, administration during organogenesis caused adverse developmental outcomes, including embryofetal mortality and malformations at maternal exposures less than those in patients at the recommended dose. Females of reproductive potential and males with female partners of reproductive potential should be advised to use effective contraception during treatment and for at least 1 week after the last dose. 1
There are no data regarding the presence of belumosudil or its metabolites in human milk, or their effects on breastfeeding infants or milk production. Because of the potential for serious adverse reactions in a breastfeeding infant, the manufacturer recommends that patients be advised not to breastfeed during belumosudil therapy and for at least 1 week after the final dose. 1
Safety and effectiveness of belumosudil have not been established in pediatric patients younger than 12 years. Use in patients 12 years and older is supported by evidence from studies in adults and pharmacokinetic data demonstrating exposure is similar between adults and pediatric patients 12 years and older. 1 A postmarketing clinical trial to assess belumosudil safety, efficacy, and pharmacokinetics in pediatric patients 3 months to 17 years of age is required, as is a study to compare the relative bioavailability of a pediatric formulation to the available tablets. 14
Adverse Reactions
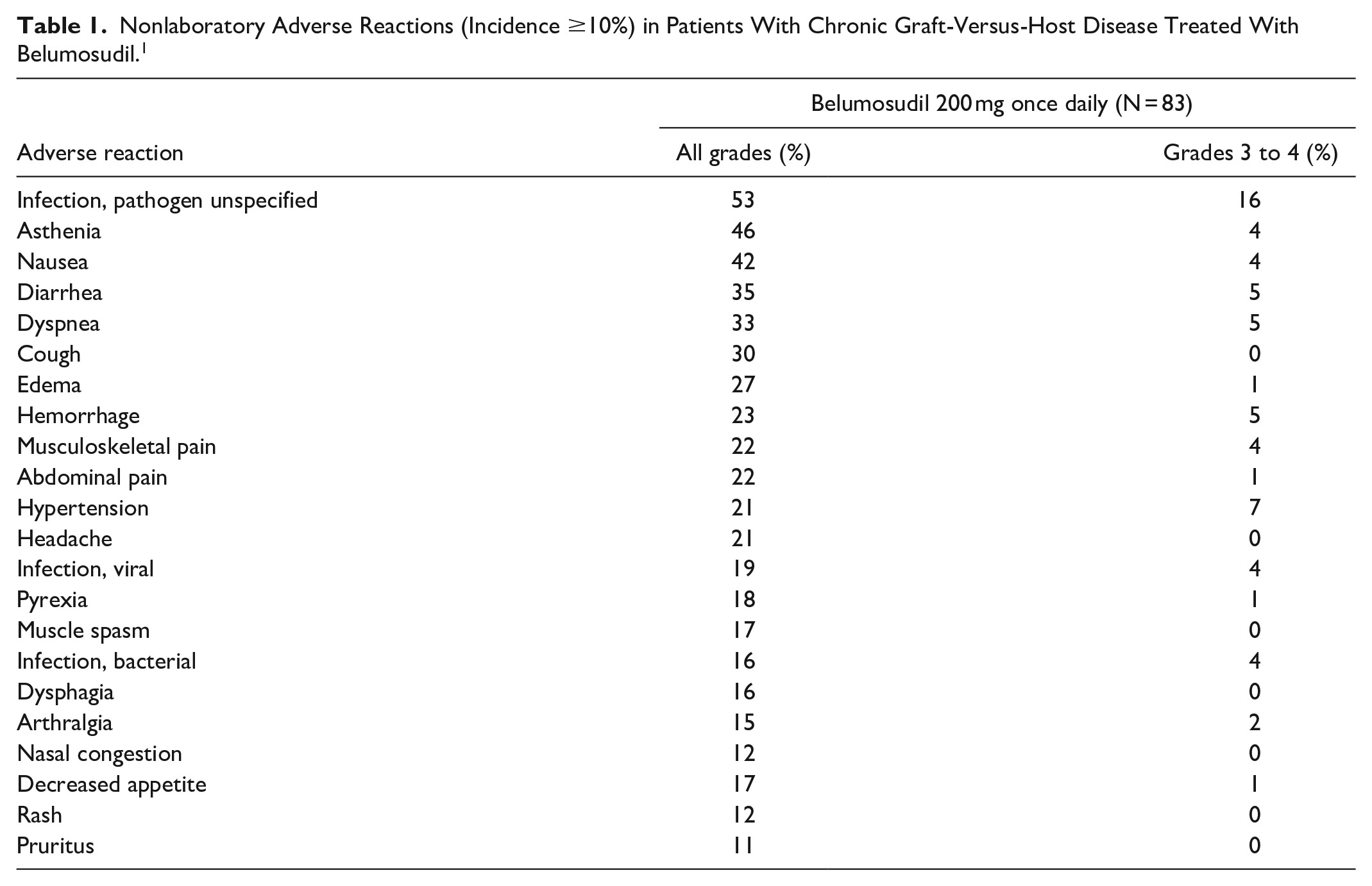
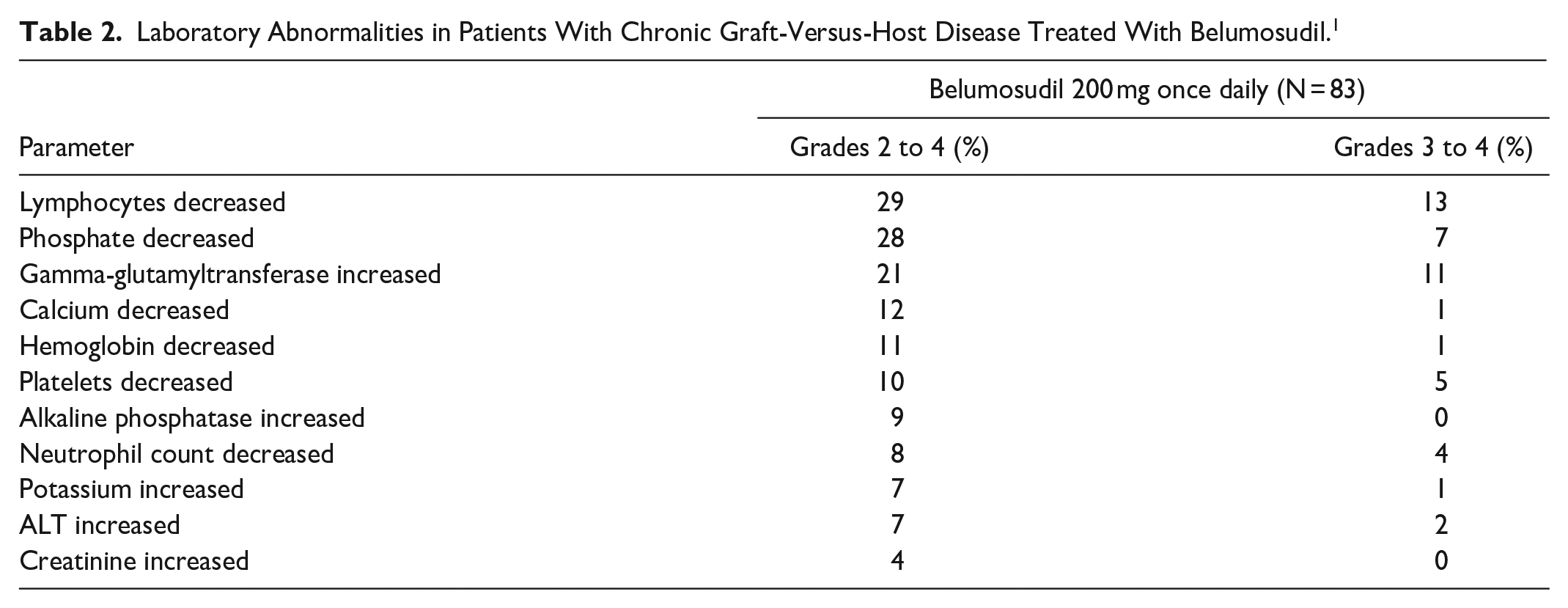
Common adverse reactions and laboratory abnormalities reported in at least 20% of patients treated with belumosudil included infections, asthenia, nausea, diarrhea, dyspnea, cough, peripheral edema, hemorrhage, abdominal pain, musculoskeletal pain, headache, decreased phosphate, increased gamma-glutamyltransferase, decreased lymphocytes, and hypertension.1,5,8 Adverse reactions occurring in at least 10% of patients are summarized in Table 1. Laboratory abnormalities are summarized in Table 2. Adverse reactions leading to dose interruption in at least 2% of patients were infections (11%); diarrhea (4%); and asthenia, dyspnea, hemorrhage, hypotension, abnormal liver function test, nausea, pyrexia, edema, and renal failure (2% each). Overall, adverse reactions leading to dose interruption occurred in 29% of patients. Permanent discontinuation of belumosudil due to adverse reactions occurred in 18% of patients. Nausea resulted in permanent discontinuation in 4% of patients. 1
Nonlaboratory Adverse Reactions (Incidence ≥10%) in Patients With Chronic Graft-Versus-Host Disease Treated With Belumosudil. 1
Laboratory Abnormalities in Patients With Chronic Graft-Versus-Host Disease Treated With Belumosudil. 1
The FDA is requiring a thorough QT/QTc trial to evaluate the effect of repeat doses of belumosudil on the QT/QTc interval and a clinical trial in a sufficient number of Black patients with chronic GVHD to assess risk of cardiac toxicities and further characterize grade 3 toxicities, including GI and vascular disorders associated with belumosudil. 14
Drug Interactions
Belumosudil is a CYP3A4 substrate. Coadministration with strong CYP3A inducers decreases belumosudil exposure and may reduce the efficacy of belumosudil. Coadministration with rifampin (a strong CYP3A inducer) decreased belumosudil Cmax by 59% and AUC by 72% in healthy subjects. Coadministration with efavirenz (a moderate CYP3A inducer) was predicted to decrease belumosudil Cmax by 32% and AUC by 35% in healthy subjects. The dosage of belumosudil should be increased when coadministered with strong CYP3A inducers. Administration with the strong CYP3A inhibitor itraconazole did not have a clinically meaningful effect on belumosudil exposure in healthy subjects. Use with moderate or strong inhibitors and inducers of CYP3A4 was not permitted during clinical trials. 15
Coadministration of belumosudil with proton pump inhibitors decreases belumosudil exposure and may reduce the efficacy of belumosudil. Coadministration with rabeprazole (a proton pump inhibitor) decreased belumosudil Cmax by 87% and AUC by 80%; coadministration with omeprazole decreased belumosudil Cmax by 68% and AUC by 47% in healthy subjects. The dosage of belumosudil should be increased when coadministered with a proton pump inhibitor. 1
Belumosudil is an inhibitor of CYP1A2, CYP2C19, CYP2D6, UGT1A1, and UGT1A9. It is also a substrate of P-gp and inhibits the BCRP, P-gp, and OATP1B1 transporter systems at clinically relevant concentrations. Coadministration of belumosudil with midazolam (a CYP3A substrate) was associated with a small increase in midazolam Cmax (1.3-fold) and AUC (1.5-fold). Coadministration of belumosudil is not expected to have clinically meaningful effects on exposure of CYP2C9 substrates and CYP2C8 substrates. 1 The FDA is requiring additional studies to assess the potential for drug interactions when belumosudil is coadministered with CYP1A2, CYP2C19, CYP2D6 enzymes and UGT1A1, P-gp, BCRP, and OATP1B1 substrates. 14
Recommended Monitoring
Pregnancy status of patients who may become pregnant should be verified prior to initiating belumosudil treatment. 1 Total bilirubin, AST, and ALT should be monitored at least monthly during therapy. 1
Dosing
The recommended belumosudil dosage is 200 mg orally once daily until progression of chronic GVHD that requires new systemic therapy. Doses should be taken with a meal at approximately the same time each day. If a dose is missed, extra doses should not be taken to make up for the missed dose. The tablets should be swallowed whole and not cut, crushed, or chewed. 1
Belumosudil has not been studied in patients with preexisting severe renal or hepatic impairment. In these populations, the risks and potential benefits should be considered prior to initiating therapy with belumosudil. 1
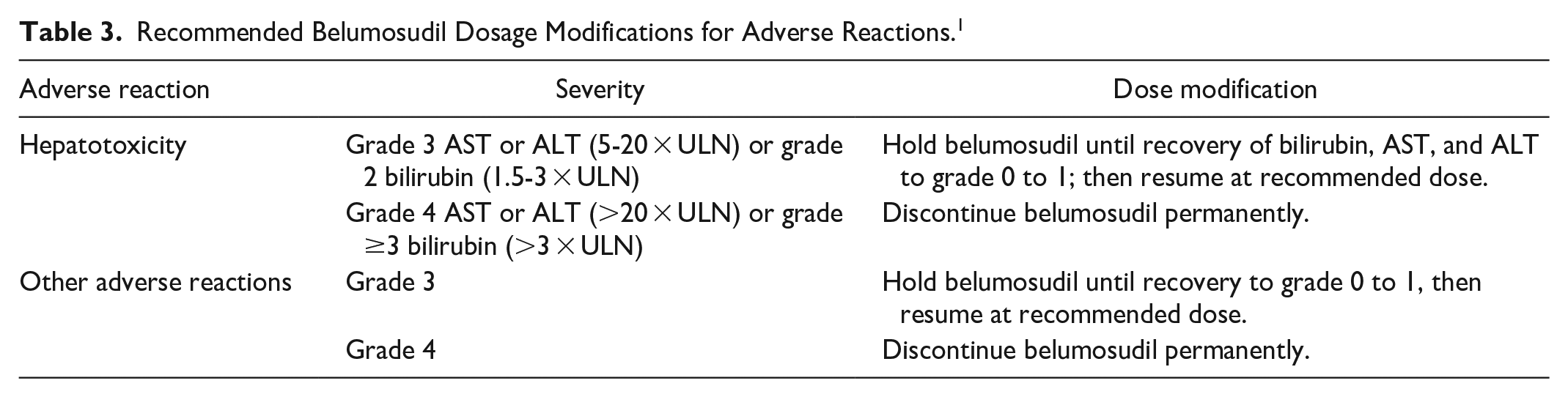
Dosage modifications are recommended for adverse reactions (see Table 3) and select drug interactions. The belumosudil dosage should be increased to 200 mg twice daily if coadministered with a strong CYP3A inducer or with a proton pump inhibitor. 1
Recommended Belumosudil Dosage Modifications for Adverse Reactions. 1
Product Availability and Storage
Belumosudil was approved by the FDA on July 16, 2021. 14 Belumosudil is available as 200 mg tablets in bottles of 30. 1
Store belumosudil tablets at 20°C to 25°C (68°F-77°F); excursions are permitted between 15°C and 30°C (59°F and 86°F). Belumosudil tablets must be dispensed and stored in the original container to protect from moisture. The cap should be securely replaced each time after opening, and the desiccant should not be discarded. 1
Drug Safety/REMS
No REMS is required for belumosudil. 14
Conclusion
Belumosudil is an orally active ROCK2 inhibitor indicated for the treatment of adults and pediatric patients 12 years and older with chronic GVHD after failure of at least 2 prior lines of systemic therapy. Belumosudil has demonstrated objective responses in patients previously treated with ibrutinib or ruxolitinib, as well as in patients refractory to prior systemic therapies and in those treated with 4 or more prior lines of therapy. Head-to-head studies comparing belumosudil with another active therapy have not been conducted. Comparison of efficacy and tolerability of belumosudil with ibrutinib and ruxolitinib is necessary to determine the roles of these agents in patients requiring therapy beyond corticosteroids and calcineurin inhibitors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.