
Abstract
Purpose:
To evaluate unfractionated heparin (UFH) dosing guided by antifactor Xa levels during targeted temperature management (TTM) post-cardiac arrest.
Methods:
Single-center, retrospective, observational study between January 1, 2014 and September 1, 2020. Patients initiated on TTM post-cardiac arrest and UFH were evaluated for inclusion. Patients included were ≥18 years of age and received weight-based UFH for ≥6 hours with 2 antifactor Xa levels drawn at target temperature. Excluded patients had no available temperature readings, received extracorporeal membrane oxygenation (ECMO) or factor Xa inhibitor (within 72 hours), or had hypertriglyceridemia or hyperbilirubinemia. The primary endpoint was to evaluate the proportion of patients that achieved a therapeutic antifactor Xa level between 0.3 and 0.7 IU/mL at steady state during TTM. Secondary endpoints included average UFH dose and average time to therapeutic antifactor Xa level at steady state; percent of first and total antifactor Xa levels subtherapeutic, therapeutic, and supratherapeutic during TTM.
Results:
A total of 73 patients met inclusion criteria. Of these, 21 patients achieved steady-state therapeutic antifactor Xa levels during TTM. The average time and dose to steady-state therapeutic antifactor Xa levels were 8.1 ± 4.5 hours and 9.9 ± 3.2 units/kg/hour. Overall, 61.7% of first and 47.4% of all antifactor Xa levels were supratherapeutic during TTM. Three (4.1%) patients experienced a major bleeding event.
Conclusions:
Guideline recommended UFH dosing, 12 or 18 units/kg/hour, during TTM resulted in more supratherapeutic antifactor Xa levels. Reduction of UFH infusion dose to 10 units/kg/hour may be required during TTM to maintain therapeutic antifactor Xa levels.
Introduction
Sudden cardiac arrest is a common medical emergency with a low incidence of survival. 1 Patients who are comatose post-cardiac arrest have worse neurological outcomes due to hypo-perfusion and subsequent lack of oxygen delivery to the brain.2,3 Guidelines recommend targeted temperature management (TTM) to improve neurological function post-cardiac arrest in comatose adult patients with return of circulation (ROSC) after cardiac arrest. 4 However, recent literature has shown overall survival of patients experiencing an out-of-hospital cardiac arrest at 6 months is similar between target temperatures (33°C vs 36°C vs <37.5°C), thus creating equipoise that further questions the efficacy of TTM.4-6 Sudden cardiac arrest is commonly caused by thromboembolic events, such as pulmonary embolism (PE) or acute coronary syndrome (ACS), that warrant treatment with anticoagulation. 7 During hypothermia various enzymatic reactions within the body are slowed, thus impacting the metabolic processes involved in medication pharmacokinetics. Pertinent medications include but are not limited to anticoagulants, with a resulting change in overall requirements during TTM.8,9
Unfractionated heparin (UFH) is the preferred anticoagulant in the inpatient setting for multiple reasons: rapid onset, short half-life, full reversibility, monitoring ability, and lack of renal elimination/adjustment. 4 UFH monitoring and dosing has traditionally been guided by activated partial thromboplastin time (aPTT); however, several drawbacks such as interpatient variability and reagent specificity have led to a shift in the monitoring and dosing of UFH to be guided by antifactor Xa levels.4,9,10 The antifactor Xa assay serves as a direct measurement of the functional activity of UFH and is subject to less interference by both analytical and biologic factors. Clinical studies have demonstrated higher accuracy in normothermic patients via an increased proportion of assays within goal range compared to aPTT. Historically, monitoring UFH by antifactor Xa was not widely available; however, it is becoming more available across institutions and health systems. 10
Two studies evaluated UFH dosing based on aPTT levels during TTM post-cardiac arrest. Notably, both found significantly reduced UFH requirements.11,12 Currently, there is limited data on UFH dosing by antifactor Xa levels during TTM. The purpose of this study is to evaluate UFH dosing by antifactor Xa levels during TTM post-cardiac arrest.
Methods
This was a single-center, retrospective study conducted at a 914-bed tertiary-care hospital. Patients admitted to the intensive care unit who achieved ROSC following cardiopulmonary resuscitation (CPR) and underwent TTM between January 1, 2014 and September 1, 2020 were screened for enrollment. Patients were included if they were ≥18 years of age, received a weight-based UFH infusion for ≥6 hours and had at least 2 antifactor Xa levels drawn at goal temperature. Exclusion criteria included unavailable temperature readings at the time of antifactor Xa level collection, extracorporeal membrane oxygenation (ECMO), direct oral anticoagulant (DOAC) or low molecular weight heparin (LMWH) within 72 hours, hyperbilirubinemia (defined as >6.6 mg/dL), or hypertriglyceridemia (defined as >300 mg/dL). Hyperbilirubinemia and hypertriglyceridemia were excluded due to interference with antifactor Xa assay accuracy. 10 Following enrollment, patients were stratified according to dosing regimen and targeted temperature. This study was approved by the Institutional Review Board with the reference number 351795.
Patient characteristics were obtained via review of the electronic medical record (EMR), EPIC (Epic Systems Corporation, Verona, WI) and AllScripts (Allscripts Healthcare Solutions, Inc, Chicago, IL). A computerized UFH dosing flow sheet within the EMR was used to obtain information on UFH bolus (units/kg), infusion (units/kg/hour), and antifactor Xa levels. TTM was implemented in our unresponsive post-cardiac arrest patients’ utilizing the Artic Sun Temperature Management System® (Medvance Inc., Covington, GA). This system uses external cooling techniques to achieve set target temperature monitored by an esophageal temperature probe. The TTM protocol includes a rapid-cooling induction phase to achieve the target temperature (33°C or 36°C) over 4 hours, followed by a maintenance cooling phase at target temperature for 24 hours; after which a slow (8 hours) rewarming phase (0.25°C/hour) to goal (36.5°C) is initiated. The indication for UFH during TTM post-cardiac arrest guided the dose chosen for the infusion and bolus. Bolus administration was based on provider discretion. For an indication such as PE, deep vein thrombosis (DVT), or atrial fibrillation, an infusion of 18 units/kg/hour with or without a bolus of 80 units/kg was selected. No max initial infusion rate is defined for the PE/DVT/atrial fibrillation institutional protocol. However, the max initial bolus was 10 000 units. For an indication such as ACS, an infusion of 12 units/kg/hour with or without a bolus of 60 units/kg was selected. Per institutional ACS UFH protocol, the max initial UFH infusion rate is 1000 units/hour and max initial bolus is 4000 units. Data was grouped into 3 distinct temperature ranges: TTM (33°C vs 36°C) and normothermia (>36.5°C). For the purposes of statistical analysis, any antifactor Xa level value >2.00 IU/mL was rounded to 2.00 IU/mL.
The primary endpoint was to evaluate the proportion of patients that achieved a therapeutic antifactor Xa level of 0.3 to 0.7 IU/mL at steady state during TTM. Steady state was defined as 2 consecutive antifactor Xa levels being therapeutic at a stable UFH infusion rate. Secondary endpoints included evaluating the average UFH dose with a therapeutic antifactor Xa level and average time to therapeutic antifactor Xa level at steady state; percent of all antifactor Xa levels subtherapeutic, therapeutic, and supratherapeutic; and percent of first antifactor Xa levels subtherapeutic, therapeutic, and supratherapeutic during TTM. Patients were further stratified according to UFH dosing strategy and temperature (33°C or 36°C) with outcomes compared among groups.
Safety outcomes assessed the incidence of bleeding events during TTM. Major bleeding was defined as fatal bleeding, symptomatic bleeding in a vital organ, such as intracranial, intra-spinal, intraocular, retroperitoneal, intra-articular or pericardial, or intramuscular with compartment syndrome, a drop in hemoglobin >2 g/dL in 24 hours, or a non-operational transfusion of ≥2 packed red blood cells (PRBC). Clinically relevant minor bleeding was defined as bleeding that did not meet major bleeding criteria but prompted a clinical response.
Summary statistics were used with the appropriate measures of central tendency for baseline characteristics. Point estimates were used to summarize the proportion among all patients that achieved the primary and secondary outcomes. Subgroup analyses were depicted utilizing Loess-curve fittings. For the safety endpoint, count and percentages were utilized to summarize major bleeding events and clinically-relevant minor bleeding events.
Results
During the study period, 112 patients were initiated on TTM and weight-based UFH. Of these, 73 patients met study criteria and were included in the analysis. The remaining 39 patients were excluded due to ECMO (n = 21), UFH administration for less than 6 hours (n = 14), <2 antifactor Xa levels during TTM (n = 3), and hypertriglyceridemia (n = 1). Table 1 shows demographic information, severity scores, data associated with cardiac arrest event, and reason for anticoagulation. The majority of patients received UFH as a 60 units/kg bolus (65.8%) followed by 12 units/kg/hour infusion (76.7%). Two patients were initiated on UFH 10 units/kg/hour without an initial bolus due to provider preference.
Baseline Hospital Characteristics.
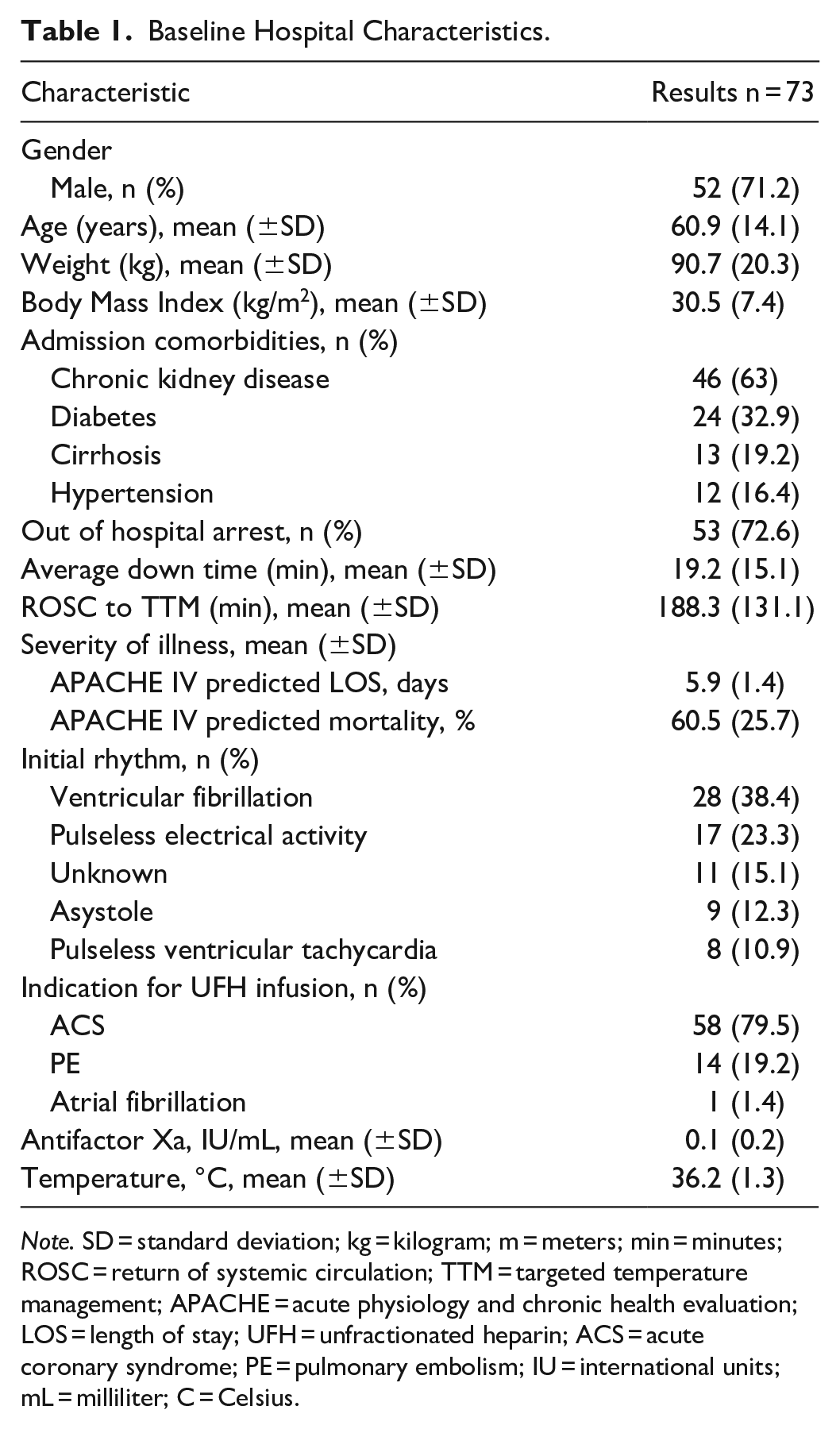
Note. SD = standard deviation; kg = kilogram; m = meters; min = minutes; ROSC = return of systemic circulation; TTM = targeted temperature management; APACHE = acute physiology and chronic health evaluation; LOS = length of stay; UFH = unfractionated heparin; ACS = acute coronary syndrome; PE = pulmonary embolism; IU = international units; mL = milliliter; C = Celsius.
A steady-state therapeutic antifactor Xa level was achieved in 21 (28.8%) patients during TTM. The average time to steady state was 8.1 ± 4.5 hours with an average dose of 9.9 ± 3.2 units/kg/hour. Figure 1 represents the trend in UFH dose over aligned time during TTM and normothermia. When stratifying according to dosing strategy utilized, patients in the no bolus 12 units/kg/hour subgroup had the highest proportion of patients achieving steady state (Table 2).
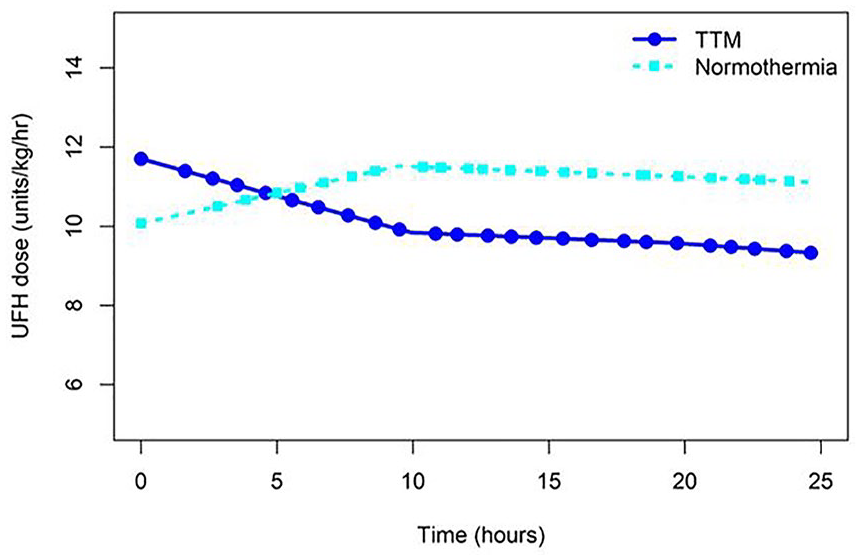
UFH dose over time during TTM versus normothermia.
Primary and Secondary Outcomes between Dosing Strategy Subgroups.
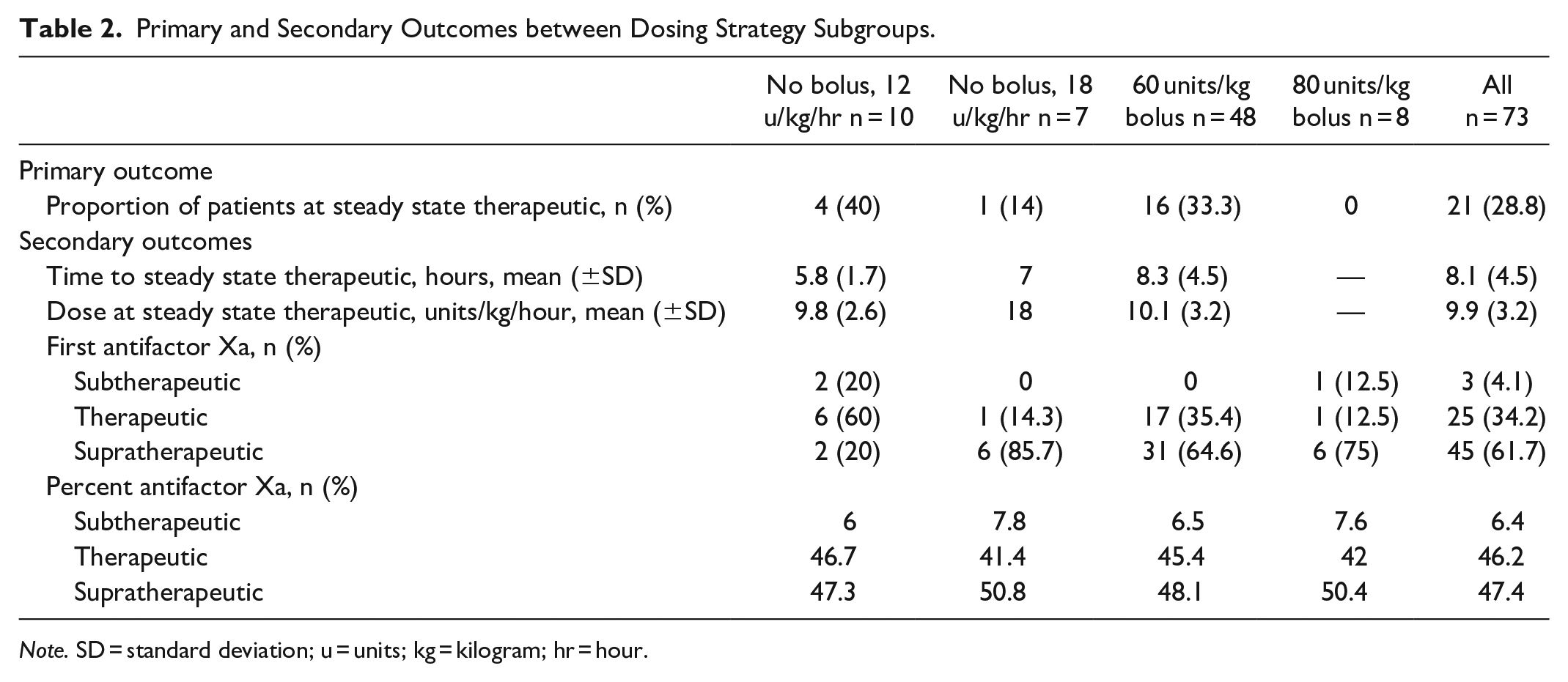
Note. SD = standard deviation; u = units; kg = kilogram; hr = hour.
Of all antifactor Xa levels drawn during TTM, 47.4% were supratherapeutic, 46.2% were therapeutic, and 6.4% were subtherapeutic (Table 2). Furthermore, 61.7% of first antifactor Xa levels drawn were supratherapeutic. The relationship between UFH dose and antifactor Xa level is depicted in Figure 2. During TTM, doses ≥11 units/kg/hour resulted in supratherapeutic antifactor Xa levels. The UFH dose that commonly resulted in therapeutic antifactor Xa levels correlated with our reported average dose of 9.9 ± 3.2 units/kg/hour. During normothermia, doses ≤10 units/kg/hour resulted in more subtherapeutic antifactor Xa levels, while our standardized doses of 12 to 18 units/kg/hour resulted in therapeutic antifactor Xa levels. A higher proportion of patients had an initial supratherapeutic antifactor Xa level when started on 18 units/kg/hour compared to 12 units/kg/hour (80% vs 56.9%), regardless of bolus administration. Approximately one third of initial antifactor Xa levels were therapeutic, with a majority (92%) of these patients receiving UFH 12 units/kg/hour. Of the first antifactor Xa levels, approximately one third were therapeutic with the majority (92%) in the 12 units/kg/hour subgroup. Only 3 (4.1%) of the first antifactor Xa levels were subtherapeutic across all subgroups (Table 2). When comparing the various dosing strategies utilized, dosing strategies with a bolus were associated with a more rapid dose reduction over time. The higher dosing strategy of 18 units/kg/hour, regardless of bolus, correlated with a more dramatic decrease in UFH dose over time (Figure 3).
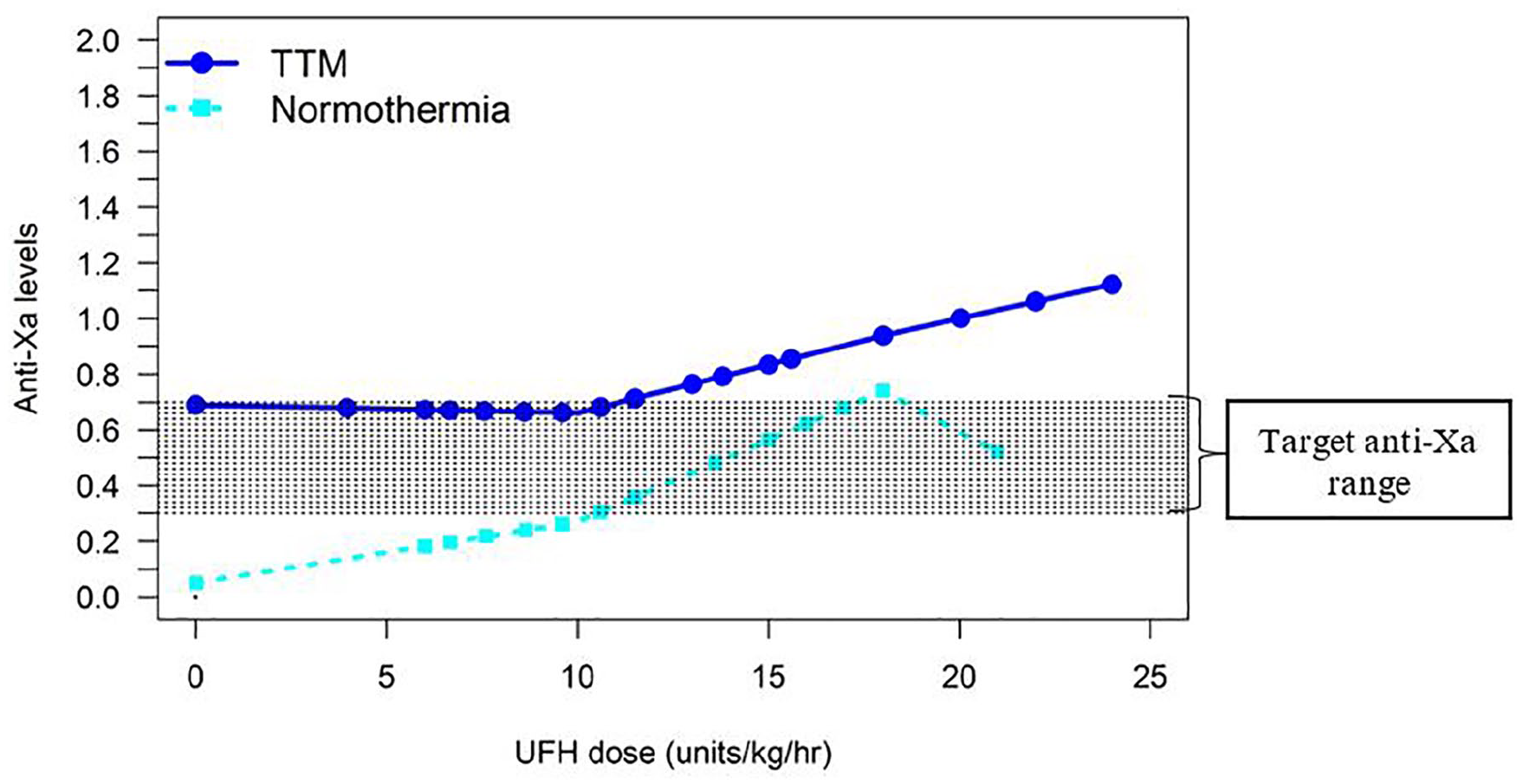
Heparin dose and antifactor Xa response during TTM versus normothermia.
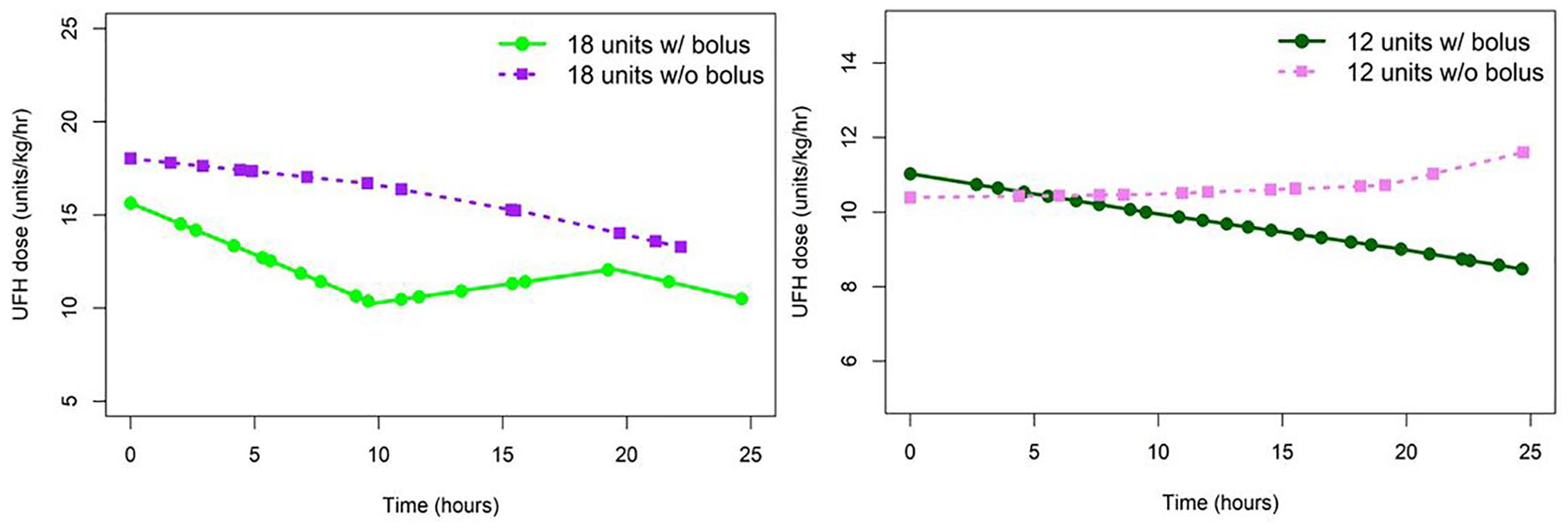
UFH dose over time between dosing strategies.
The target temperature was 33°C and 36°C for 56 (76.7%) and 17 (23.3%) patients, respectively. UFH was continued into normothermia for 47 patients. The proportion of patients achieving a steady-state therapeutic antifactor Xa level, average time, and average dose during steady state was similar between the 2 target temperatures (Table 3).
Primary and Secondary Outcomes Between Temperature.
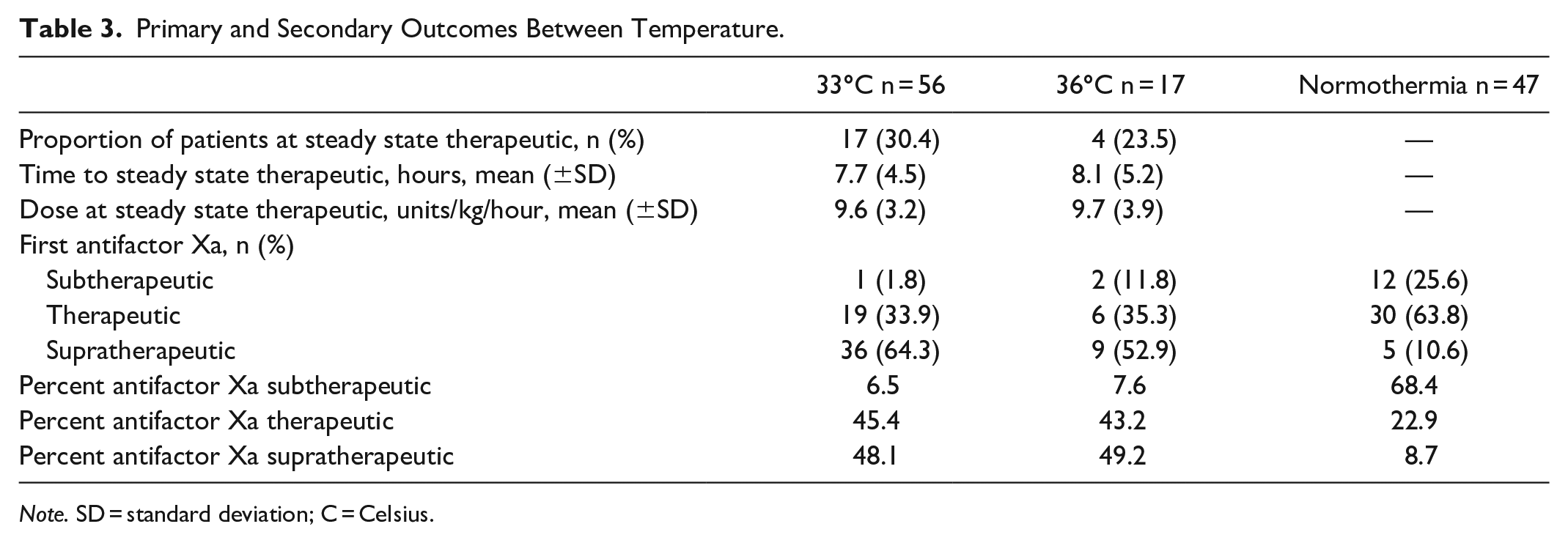
Note. SD = standard deviation; C = Celsius.
There were 4 episodes of major bleeding in 3 patients during the study. One of the 3 patients had a drop in hemoglobin >2 g/dL in 24 hours and all 3 patients had non-operational transfusion of ≥2 PRBCs. No episodes of clinically-relevant minor bleeding were observed.
Discussion
The present study evaluated UFH dosing guided by antifactor Xa levels during TTM post-cardiac arrest. Only 21 (28.8%) patients achieved steady-state therapeutic antifactor Xa levels with an average dose of approximately 10 units/kg/hour regardless of target temperature. The subgroup with the highest proportion of patients achieving a steady-state therapeutic antifactor Xa level received 12 units/kg/hour without a bolus followed by the 12 units/kg/hour with a bolus subgroup (Table 2). The bolus subgroups had a more rapid dose reduction over time compared to the no bolus subgroups (Figure 3). These findings further support the need for a dose reduction during TTM and provides a reasonable initial UFH infusion rate of 10 units/kg/hour without a bolus.
Two observational studies have been published on UFH dosing guided by aPTTs during TTM with a target temperature of 33°C.11,12 Both reported over 75% of aPTTs as supratherapeutic during the cooling phase. Fevold et al. created dose-response equations using a linear model based on aPTT response to various UFH doses at different temperature stages. Based on the linear model, Fevold et al. predicted a reduction in UFH by 43% to 54% at a temperature of ≤33°C would be required to maintain a therapeutic aPTT. Wahby et al reported only 3 patients achieved a therapeutic aPTT with a review of those patients revealing the initial rate of UFH was 7 ±1 units/kg/hour. Additionally, both studies recommended reduced UFH dosing (5-8 units/kg/hour) during TTM. Similar to previous studies, we found the majority of first and all antifactor Xa levels were supratherapeutic. However our average UFH dose was higher (10 units/kg/hour) during TTM. This could be due to the multitude of biological and analytical factors falsely elevating aPTT values resulting in a lower UFH dose overall. Antifactor Xa levels directly measure UFH’s intrinsic activity indicating an empiric dose reduction is warranted. However, the empiric reduction recommended by the previous studies (5-8 units/kg/hour) could underestimate the average dose required to achieve a steady state, according to our study (10 units/kg/hour).
A large retrospective study by Zidane et al. evaluated the rates of major bleeding events in patients treated with UFH for DVT or PE in routine clinical practice. The study reported the rate of major bleeding events was 4%. 13 Furthermore, a meta-analysis comparing LMWH and UFH for the treatment of ACS reported the prevalence of major bleeding for the UFH group was 3.1%. 14 In our study, the rate of major bleeding was 4.1%, which is comparable to the rates of major bleeding reported in normothermic patients. This further supports the safety associated with initiating UFH during TTM when indicated.
Our study presents several strengths. It is the largest study evaluating UFH dosing guided by antifactor Xa during TTM to date. Additionally, our study provides dosing guidance on the implementation of weight-based UFH infusions for patients undergoing TTM. The multiple subgroup analyses assessed the impact between target temperature, boluses, and infusion rates, thus illustrating the expectations of a dosing strategy that will achieve a therapeutic target. The applicability of the results becomes useful in clinical practice as more institutions shift toward UFH dosing guided by antifactor Xa. Despite the aforementioned strengths, our study also presents several limitations. Due to the retrospective design, selection and/or information bias may have occurred. Lack of or inaccurate data, physiologic information or clinical outcomes may have therefore been incomplete. Another limitation was the various dosing strategies utilized due to provider preference. The standardized ACS protocol (12 units/kg/hour) has a maximum infusion rate of 1000 units/hour with a maximum initial bolus of 4000 units, while the standardized PE/DVT/atrial fibrillation protocol (18 units/kg/hour) only has a maximum initial bolus of 10 000 units. The study’s patient population had ACS as the most common indication, with an average weight of 91 kg, resulting in the majority of patients receiving a bolus <60 units/kg and initial UFH rate <12 units/kg/hour. The average bolus and initial UFH rate for the 12 units/kg/hour subgroup were 44 units/kg and 10.4 ± 2.6 units/kg/hour, respectively. Thus generalizability to patients with lower body weight would be affected. Additionally, the study was designed to assess UFH dosing requirements guided by antifactor Xa during TTM. Since no control group was included, it is unknown whether requirements of UFH guided by aPTT during TTM would have had similar implications.
Conclusion
Based on our study, reduction of the UFH starting infusion dose to 10 units/kg/hour without a bolus may be required during TTM to achieve therapeutic antifactor Xa levels. Utilization of UFH based on guideline recommendation may result in supratherapeutic antifactor Xa levels. Furthermore, UFH infusion during TTM was associated with a low incidence of major bleeding events.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.