
Abstract
Introduction
Although it has been approximately a year and a half since the coronavirus disease 2019 (COVID-19) was first detected, during which time several vaccines have been approved, the consequences of the pandemic, including threats to the physical, financial, and social safety of people, are still impacting all communities around the world. 1 Health reports from the U.S indicated that from the beginning of 2021, COVID-19 had become the third leading cause of death in the country. 2
Medication use has been proposed as a key intervention in the treatment of COVID-19 patients.1,3 Because there has been no unified treatment protocol for COVID-19, many medications that have been used for different conditions were retested against COVID-19. Several of these medications are well-known to cause severe adverse effects or interactions with other drugs or food. 4 This includes hydroxychloroquine-related cardiotoxicity and the modulatory impact of lopinavir and darunavir on the body’s enzymes and transporters.5,6 Furthermore, many patients may take drugs to relieve specific symptoms or to prevent the disease without any firm evidence of their benefits. Therefore, ensuring medication safety in COVID-19 patients has been an arduous challenge, especially in outpatient settings, given the “infodemic” or the considerable spread of dis- and misinformation related to the pandemic. 7 The core element of the challenge is preventing medication errors (MEs), which refer to a preventable failure in the processes of prescribing, transcribing, dispensing, monitoring, or counseling on medications. 8 In addition to being a leading cause of mortality and morbidity, medication errors have cost the world more than 500 billion dollars annually. 9
Prescribing errors (PEs), which result from a mistake in a prescription or drug order, are considered the most common and serious subcategory of MEs.10,11 Because prescribers have felt overwhelmed and experienced high levels of stress and burnout during the pandemic,12,13 the rates and seriousness of MEs, especially PEs, are expected to increase dramatically based on Shanafelt et al’s study. 14 They demonstrated a strong correlation between MEs and the levels of burnout and mental stability. Another factor that may have influenced the rate of PEs is the conflicting reports regarding the safety and efficacy of several drugs used to inhibit the virus. 15
Ensuring the safety and appropriateness of medication use is one of the major roles of community pharmacists, 16 who receive many prescriptions for COVID-19 patients treated at home. To fulfill this role and conduct a successful pharmaceutical intervention (PI), pharmacists should be involved more in patient treatment and management. 17 Nevertheless, there has been no effective and applicable tool that can improve the clinical skills of community pharmacists in regard to medication safety during COVID-19 pandemic. Additionally, physicians may reject pharmacists’ interventions regarding patient therapy.
Although conventional educational approaches have been implemented to enhance pharmacists’ skills and knowledge on medication safety,18,19 issues related to poor applicability, high cost, and the time-consuming nature, decrease pharmacists’ engagement in these approaches, and thus limit its effectiveness. 20 Clinical case scenarios have been widely used as an effective assessment method for the clinical skills and knowledge of healthcare professionals. 21 We adopted this approach into our study to enhance pharmacists’ ability to detect PEs in patients with COVID-19. The major challenge we encountered was how to deliver this intervention, given that traditional (ie, face-to-face workshops) and virtual methods (ie, videoconferencing) consume time and resources. Additionally, face-to-face events can increase the risk for COVID-19 transmission. WhatsApp, which is a free messenger application used by roughly one-fifth of the world’s population, offers unlimited messaging, immediate contact with people in different geographic locations, and access to messages even if the user is offline. Previous studies indicated that WhatsApp is a useful platform that can be used widely in medical practice to assess clinical skills of clinicians and help improving communications between different professionals.22,23 Rathbone et al, also demonstrated that WhatsApp is an efficient tool to enhance communication and maintain relationships between pharmacy professionals. 24
The vast majority of COVID-19 patients in Jordan are vulnerable to PEs, because those patients have been treated at home with prescriptions from primary care physicians, and because healthcare authorities in Jordan monitor only the dispensing of controlled drugs, without effective restrictions on dispensing of other drugs. 25 While PEs in hospital settings in Jordan have been well-documented,26,27 this is be the first study to address PEs in community settings during the COVID-19 pandemic.
Consequently, we used WhatsApp to send a group of PEs-related clinical scenarios to community pharmacists. In addition to documenting the incidence, nature, and the seriousness of PEs involving COVID-19 patients in community settings, we aimed to test the effectiveness of our strategy on pharmacists’ ability to identify these errors and conduct successful PIs. This two-component educational strategy could improve the outcomes of patient safety and optimize pharmacotherapy for home-treated COVID-19 patients.
Methods
Research Designs
This was a 4-month randomized, controlled study (1st January-1st April 2021) conducted in 110 community pharmacies, which were equally allocated to either an active or control group. Over the course of 4 weeks PE-related clinical case scenarios involving COVID-19 patients were sent to pharmacists randomized to the active group. However, the control group participants received no clinical case scenarios. After completion of the clinical scenario phase in the active group, pharmacists from both groups were asked to document PEs in COVID-19 patients and their recommendations using a data collection form. The Consolidated Standards of Reporting Trials (Supplemental Appendix 1) was used as a reference to design the procedures of the study.
Sample Size Calculation
According to a previous study measuring the influence of educational interventions on pharmacists’ ability to provide specialized care, 20 we assumed that our proposed approach would enable pharmacists to detect 18% more PEs. Additionally, based on previous mathematical equations, 28 considering a 95% confidence interval (CI), (Power: 80%, alpha: <0.05, effect size: 0.2), and 10% attrition rate, 110 community pharmacies (55 for each group) were included in the study.
The equation adopted was:
where: n = sample size required in each group, p1 = proportion of active group participants. p2 = proportion of control group participants . Zα/2: This depends on level of significance, for 5% this is 1.96. Zβ: This depends on power, for 80% this is 0.84.
The Study Procedure
This study was carried out sequentially over 4 stages (Figure 1):
Recruitment of the study sample was performed at 2 levels: pharmacy level and pharmacist level. First, the main investigator (DAQ) used an updated list of community pharmacies issued by the Jordanian Pharmacists Association to screen pharmacies to determine their eligibility using phone calls with pharmacy managers. To recruit a representative sample, we approached pharmacies from different regions using proportionate random sampling, which ensures that the number of pharmacies recruited from 1 region is proportionate to the relative proportion of pharmacies in Jordan. Pharmacies open 5 to 6 days per week, with at least 2 shifts per day, providing pharmaceutical services for more than 30 patients/customers per day, connected to a stable Wi-Fi network, with an adequate pharmacy staff to cover any absence of colleagues were considered eligible to participate in the study. Pharmacies, newly opened, located more than 7 kilometers from the nearest medical facility (ie, clinics, medical centers), in which the pharmacy manager was the only pharmacy staff were excluded from the study. After completion of the screening activity, the main investigator created an electronic list of eligible pharmacies, and then invited the pharmacy managers to participate in the study. Those that accepted the invitation completed a consent form and were asked to provide a list of their pharmacy staff. Second, the pharmacy staff working in the included pharmacies were screened for eligibility. The inclusion criteria for pharmacists were: having a Ministry of Health license, having regular working hours, currently a WhatsApp® user, and English and Arabic speaker. Pharmacists who had been enrolled in an educational program specializing in MEs or PEs or had participated in a study focusing on PEs were excluded from the study. For a pharmacy to be included in the study, both the pharmacy manager and the pharmacy staff had to agree to participate and provide a consent form.
Randomization and allocation of the study sample to the active and control group was conducted at a pharmacy level using the random number generator in IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, N.Y., USA). The data entry officers, medical statistician, and the co-authors of this study were blinded to the allocation process.
The educational intervention stage was carried out over 4 weeks by sending a group of PE-related clinical scenarios via WhatsApp® to pharmacy staff working in the active group. No clinical scenarios were delivered to pharmacists in the control group. The intervention tool (PE-related clinical case scenarios) was designed by the main investigator (Consultant Pharmacotherapist in Infectious Disease) and 2 infectious disease specialists with COVID-19 experience. They developed 28 clinical scenarios including PEs in COVID-19 patients based on their observations in clinical practice, the experiences of their colleagues from different countries (ie, Saudi Arabia, Kuwait, United Kingdom, Canada), and the published international literature. The clinical scenarios comprised of 36 prescriptions, 88 medications, and 63 PEs; 8 of the scenarios included 1 PE, 10 included 2 PEs, 5 included 3 PEs, and 5 included 4 PEs. Each clinical scenario consisted of 2 main elements: the case and the solution. Information included in the case was limited to that required to identify the PEs and the appropriate intervention. For instance, in some clinical scenarios, all of the following were reported in the case part: current medication orders, past medical history, patient information (ie, age, body mass index, gender, and allergies), current COVID-19 status (mild, moderate, severe), signs and symptoms, comorbidities, radiology and laboratory findings. In other clinical scenarios, only some of the previous information was mentioned. The novelty of our approach was that the solution to the clinical scenario was included and provided to the pharmacy staff. The solution for each scenario comprised the PE, its type, clinical seriousness, and most appropriate PI. The experts who designed the clinical scenarios ensured that each case was written in English and Arabic, and the word count for each case did not exceed 110 words. The clinical scenarios centered on 3 major PEs. First, a wrong drug PE; for example, prescribing antibiotics and multivitamins to COVID-19 patients with mild symptoms. 29 In such cases, only overt symptoms should be treated. Antibiotics should not be prescribed. Vitamins and supplements should be prescribed based on blood tests. Another example of wrong drug error was prescribing favipiravir for a pregnant woman, or prescribing antimotility drugs (ie, loperamide) in COVID-19-associated diarrhea. 30 Second, an omission error, which can result from the absence of a necessary drug from the prescription. For example, stopping an angiotensin converting enzyme inhibitor (ACEI) drug in COVID-19 patients with hypertension. 31 Third, a wrong dose PE, in which the prescriber did not consider the patient’s body mass index or the organs’ functionality (ie, kidney function) of the patient. The clinical scenarios were transcribed into WhatsApp® messages and sent to pharmacists in the active group on a daily basis over 4 weeks. The research team addressed the inquiries raised by the pharmacy staff and followed with them until the completion of the stage.
Outcome assessment was carried out using a data reporting form prepared by the study researchers and completed by the pharmacy staff over a period of 3 months. The data collection form was designed to test 4 main outcomes. First, the incidence of PEs. Second, types of PEs, as categorized by Dean Franklin 10 (Supplemental Appendix 2). Third, clinical seriousness of PEs, which was assessed by quantification of 3 experts’ judgments on the severity of errors- senior clinical pharmacist, an internist, and an infectious disease specialist using Overhage’s severity scale 32 (Supplemental Appendix 3) to rate the errors on a 10-point scale; 0 (no error), 1-3 (minor error), 4-6 (significant error), 7-9 (serious error), and 10 (lethal error). The mean across all experts was calculated and considered an indicator for the clinical seriousness of a PE. The Kappa statistic was calculated to test whether the experts’ opinions were consistent. 33 Fourth, mean time needed to detect PEs and to persuade physicians/patients with pharmacist recommendations were recorded. Fifth, the rate of physician acceptance of PIs. We also asked pharmacists to record cost-reduction per patient after the PI was implemented. The pharmacy staff had the choice to fill out the form either in Arabic or English.
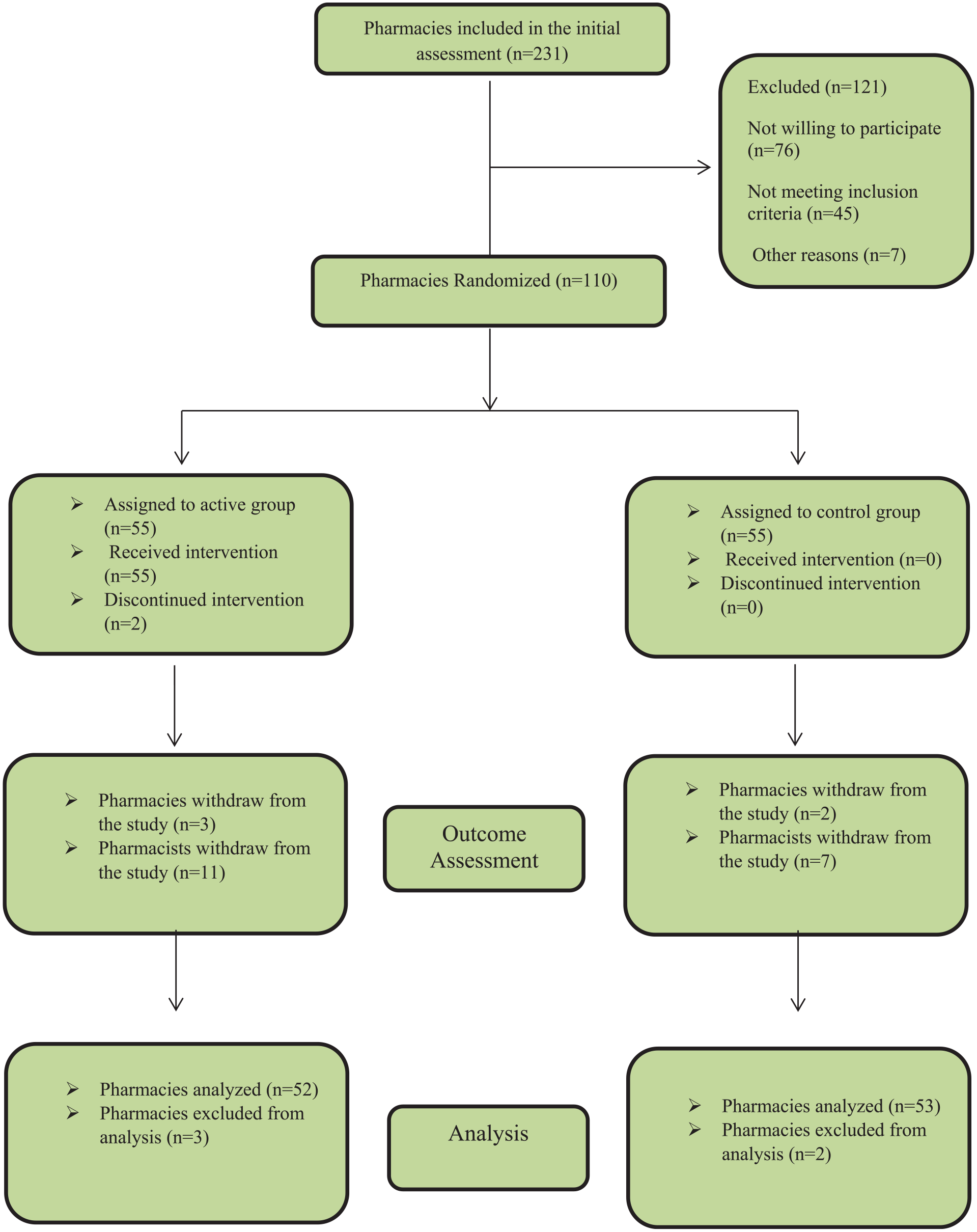
The work flow of the study.
Data Analysis
The data collection forms were firstly gathered by 5 data officers who created an electronic database using Excel software (Microsoft Corporation, 2018, Albuquerque, New Mexico, United States). Two independent data officers were hired to check the accuracy of the database by comparing it with the intimal sheets filled out by the pharmacy staff. The final version of the database was sent to an independent statistician who used SPSS version 26 to apply both descriptive and inferential statistical procedures. To test potential differences in general outcomes (ie, patient, medication, and prescription characteristics) across the study groups, we used chi-square test. To compare the mean values between the active and control groups, independent samples t-test was performed. To test predictors for physician/patient acceptance of PI (dependent variable), a multivariable logistic regression model was conducted. Types of PIs (reference: cessation of drug therapy), clinical seriousness of PEs (reference: lethal errors), patient status (reference: minor polypharmacy), and type of prescribers (reference: general practitioner) were considered independent variables. The findings of the regression model are expressed in this paper as adjusted odds ratio, with 95% confidence intervals (CIs), whereas, descriptive data are illustrated as absolute numbers (n) and proportions (%).
Results
Characteristics of Participants
Of the 242 pharmacists (working in 110 pharmacies) that agreed to participate in the study and were randomized into the active and control groups, 18 withdrew from the study, of which 11 were busy, 5 were infected with COVID-19, and 2 provided no reasons. Of the 224 pharmacists (working in 105 pharmacies) completing the trial, 171 (76.33%) were females. The proportions of daily usage of WhatsApp were similar (P > .05) across the groups (Table 1). The characteristics of pharmacies and pharmacists included in both groups were not statistically different. Examples of PEs detected by pharmacists were summarized in Supplemental Appendix 4.
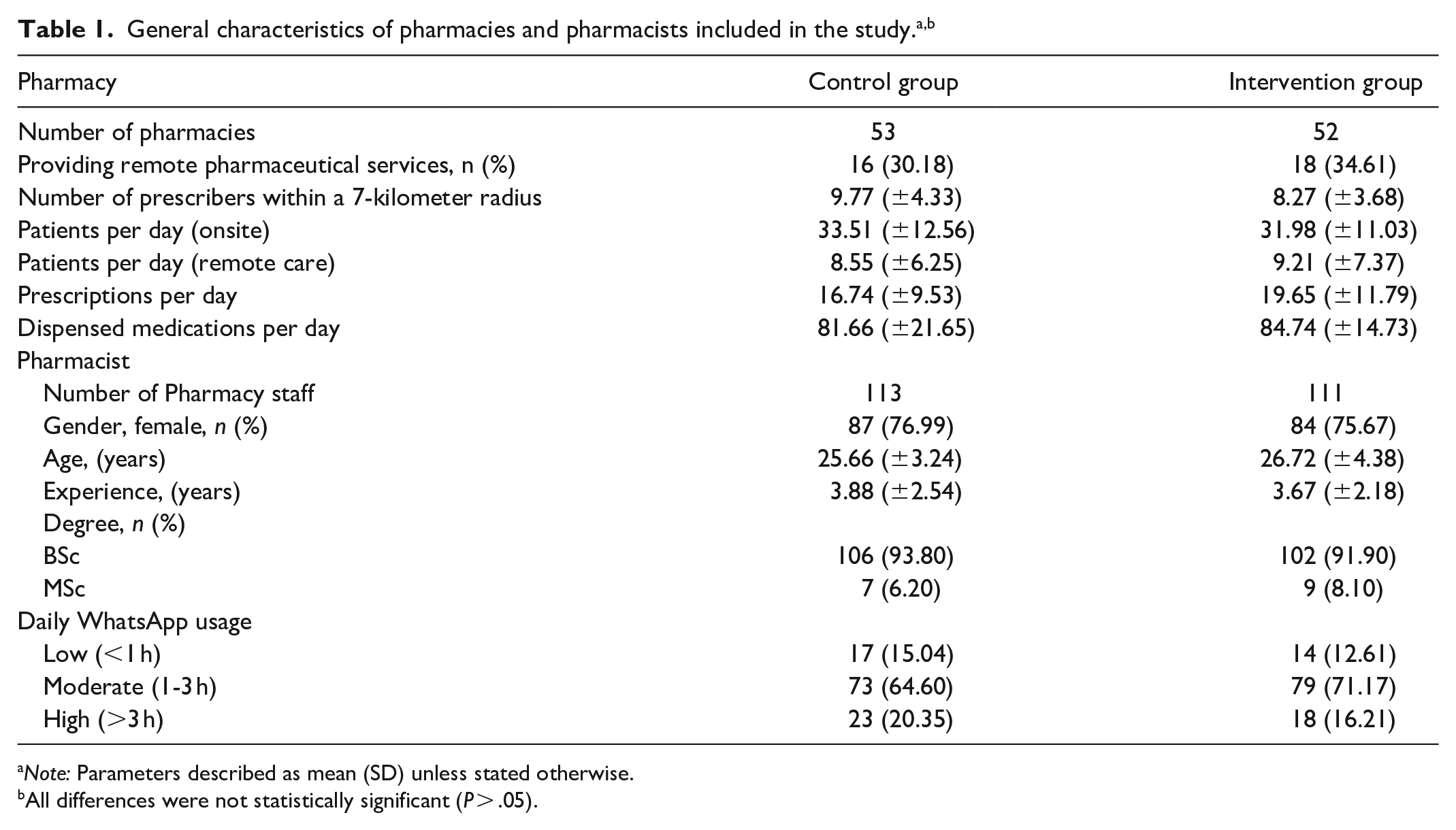
Note: Parameters described as mean (SD) unless stated otherwise.
All differences were not statistically significant (P > .05).
Incidence, Nature, and Clinical Seriousness of PEs
The incidence of PEs in COVID-19 patients, PEs per patient, and number of patients with at least one PE reported by participants in the active and control groups were 18.54% versus 3.09% (P = .001), 0.83 versus 0.16 (P = .02), and 2274 versus 595 (P = .01), respectively. There were statistically significant differences in the types and clinical seriousness of PEs across the groups (Table 2). The proportions of wrong drug (contraindication), wrong drug (unnecessary drug prescribed/no proof of its benefits), and omission of a drug across the active and control groups were 15.30% versus 7.21% (P = .001), 11.85% versus 6.29% (P = .03), and 17.78% versus 10.50% (P = .01), respectively. Additionally, the proportions of lethal, serious, and significant errors were 0.74% versus 0.35% (P = .04), 10.52% versus 2.57% (0.002), and 47.88% versus 9.57% (P = .001), respectively. While antibiotics accounted for the most common type of erroneous drugs in the active (30.98%) and control groups (30.65%), the proportions of vitamins and corticosteroids were 21.86% versus 5.87% (P = .005) and 8.65% versus 3.14% (P = .007), respectively.
Frequency and nature of prescribing errors reported during the study.
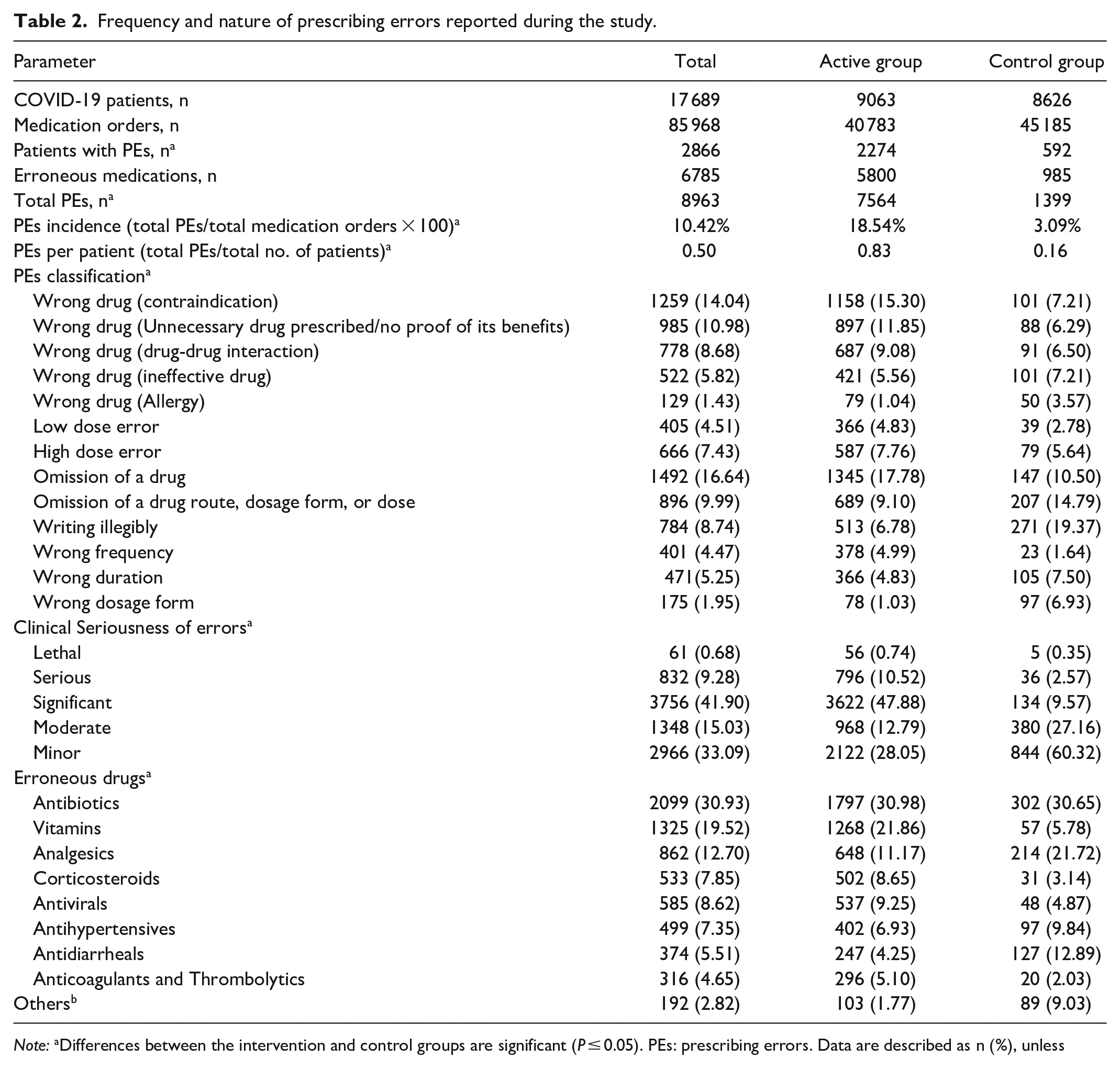
Note: aDifferences between the intervention and control groups are significant (P ≤ 0.05). PEs: prescribing errors. Data are described as n (%), unless stated otherwise.
others; refers to drugs with less than 1%.
Time Feasibility of the Study Approach
The time taken to detect PEs and the time needed to persuade physicians/patients with PIs between the active and control groups were (3.87 ± 2.78 min) versus (8.29 ± 6.38 min) and (2.03 ± 1.76 min) and (5.02 ± 4.22 min), respectively (all with P < .05). Nonetheless, the money saving rate per PI was similar in both groups. Within the active group, the time needed to detect PEs across the errors with high severity (lethal, serious, and significant errors) and errors with low severity (moderate and minor errors) was (5.32 ± 4.22 min) versus (2.42 ± 1.09 min), respectively (Table 3).
Analysis of time and cost-reduction parameters.*
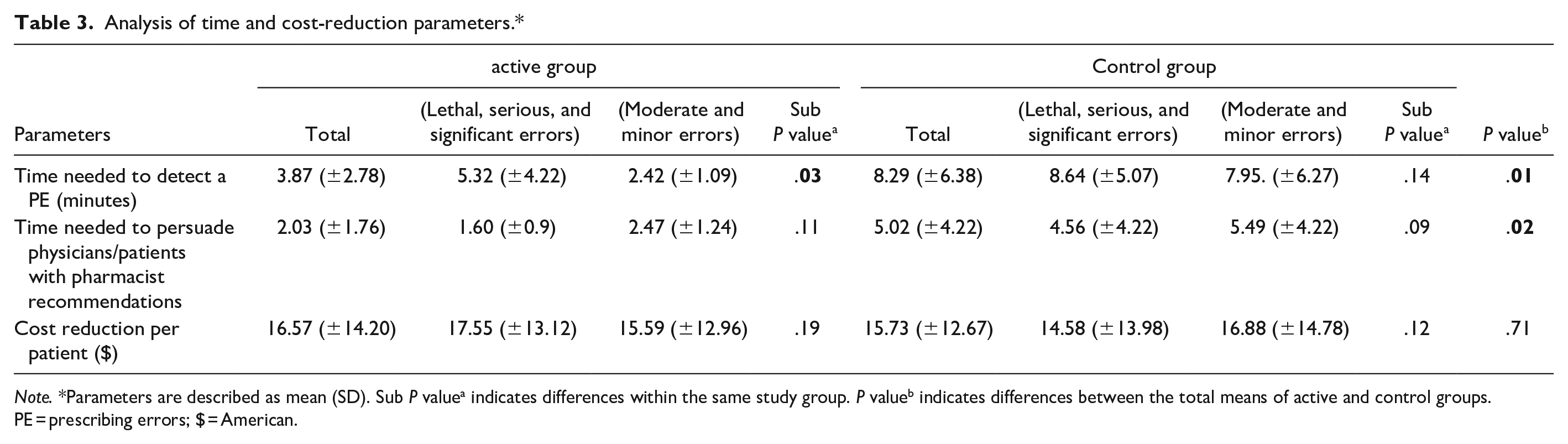
Note. *Parameters are described as mean (SD). Sub P valuea indicates differences within the same study group. P valueb indicates differences between the total means of active and control groups. PE = prescribing errors; $ = American.
Frequency, Nature, and Acceptance of Pharmaceutical Interventions
Of the 6598 and 968 PIs conducted by participants working in the active and control group pharmacies, which 6013 (91.13%) and 651 (67.25%) were accepted, respectively. The most common PIs carried out by the active group were cessation of drug therapy (48.51%) and addition of a drug therapy (23.65%). There were three significant predictors for physician/patient acceptance of PIs conducted by pharmacists in the active group; addition of drug therapy interventions (AOR = 0.62; 95% CI, 0.21-0.84), errors with significant clinical seriousness (AOR = 0.32; 95% CI, 0.16-0.64), and interventions conducted on patients with major polypharmacy (AOR = 5.65; 95% CI, 2.35-7.85) (Table 4).
Predictors for physician/patient acceptance of pharmaceutical interventions.
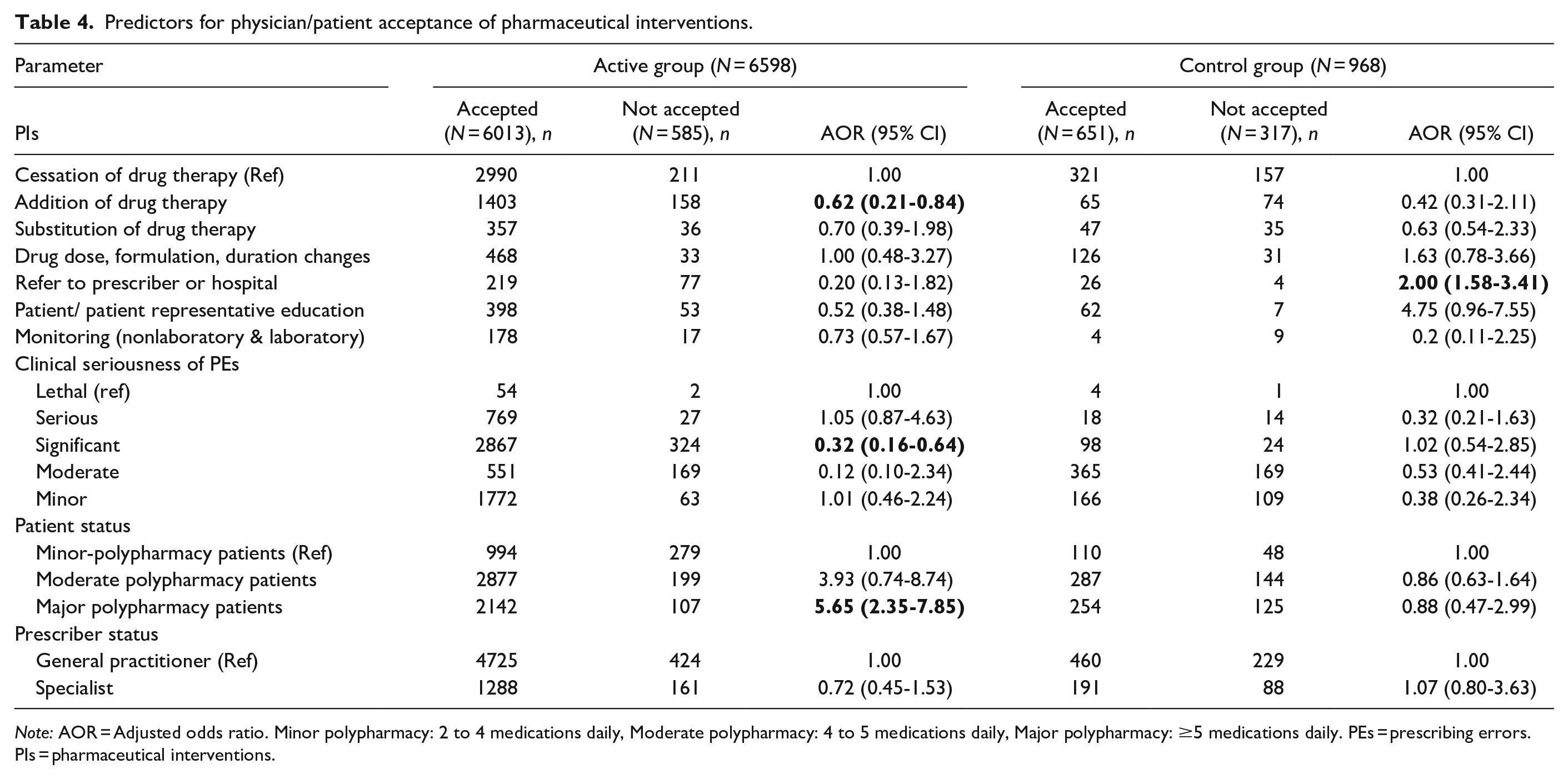
Note: AOR = Adjusted odds ratio. Minor polypharmacy: 2 to 4 medications daily, Moderate polypharmacy: 4 to 5 medications daily, Major polypharmacy: ≥5 medications daily. PEs = prescribing errors. PIs = pharmaceutical interventions.
Discussion
The current pandemic has increased the risk for PEs through applying heavy pressure and stress on prescribers, who have received conflicting reports on pharmacotherapy management in COVID-19 patients,12,34 which could result in higher rates of morbidity and mortality. 35 Although pharmacists have demonstrated themselves as key players in reducing the burden on healthcare systems and improving patient safety, 36 the COVID-19 pandemic has brought new challenges that require constant learning and improving of clinical skills. Accordingly, we aimed to assess the effectiveness of an educational intervention (PE-related clinical scenarios) designed by clinical experts and delivered to pharmacists working in community settings through WhatsApp in improving their ability to detect PEs and conduct successful PIs. This study addressed a new educational interventional approach that has never been tested for reducing PEs involving COVID-19 patients in the community.
Using WhatsApp to deliver these clinical scenarios reduced barriers to effective communication, which can hinder the advancement of clinical practice. Nonetheless, the effect of our new intervention on pharmacists’ involvement in educational events was beyond the scope of this study.
PEs related to wrong drug (contraindication, drug-drug interaction, unnecessary drug prescribed, no proof of its benefits) and omission of a drug were the top PEs detected by the active group participants. The types of errors identified by the control group pharmacists differed significantly. Two key messages can be concluded from this outcome. First, COVID-19 patients were vulnerable to a broad range of PEs, of which more than half were clinically lethal, serious, or significant. This supports the discussion of İrfan Aygün and his colleagues in their reports regarding the consequences of high multiple drug usage among COVID-19 patients. 37 We can explain the high rates of clinically serious and significant PEs involving COVID-19 patients by 2 ways: 1) the nature of errors which include prescribing medications that may lead to severe adverse effects (ie, hydroxychloroquine), major drug-drug interactions, and negative long-term effects, and 2) the nature of drugs involved in PEs, which includes antimicrobials (without clinical justification), vitamins (without blood tests), and corticosteroids for mild cases of COVID-19. The second key message is that using technology platforms (eg, WhatsApp®) to deliver clinical scenarios involving PEs in COVID-19 patients to community pharmacists might have enhanced the skills of those pharmacists in terms of conducting clinically significant interventions, such as stopping unnecessary drugs, suggesting a new pharmacotherapy, or changing the dose and duration of a drug. There are 2 previous studies in the literature, which used clinical cases to solidify pharmacists’ knowledge with regard to drug-related problems (DRPs). However, we identified 3 main points that could limit the generalizability and reliability of their outcomes. First, the vehicle used to deliver the intervention was face-to-face workshops, which could negatively influence the engagement of pharmacists due to the high cost and time-consuming nature of such educational events. Second, the intervention itself was unclear and delivered over a short period, which is unlikely to considerably influence the skills and knowledge of pharmacists on a particular topic. Third, the outcome assessment of those studies was conducted using questionnaires, a method that cannot provide clear evidence about the impact of their approaches on practice.
In this study, the rate of physician/patient acceptance of PIs in the active group was significantly higher than that reported by the control group and other studies conducted in the Netherlands 38 and France. 39 This could be attributed to the structure of clinical scenarios used in the intervention phase, which included not only the case, but also an evidence-based solution.
In total, the findings of this study have 2 major implications. First, the magnitude and the severity of PEs involving COVID-19 patients in the community was concerning and corrective actions are needed to prevent such errors and reduce their burden on patient safety and healthcare systems. Second, the strategy proposed in this study can help in developing a feasible and time-efficient interventional tool to encourage pharmacists’ involvement in identifying and correcting PEs in light of COVID-19. Nonetheless, further research projects are needed to establish and optimize collaborative practice and communication tools between community pharmacists and prescribers in primary and secondary care units; for example, assessment of an instant communication system that links pharmacists with prescribers to facilitate correcting PEs, if any. Additionally, the influence of WhatsApp usage as a vehicle for medical education on rate of pharmacists’ involvement in educational events needs to be evaluated.
The outcomes of the current study need to be considered in light of its limitations. First, this study focused on a new strategy established to improve proactive measures to prevent PEs, and no assessment for outcome-based parameters, such as rates of mortality, recovery, hospitalization was conducted. Therefore, before providing a final and robust judgment on the efficacy of the new strategy, an assessment of outcome-based parameters should be conducted. Nevertheless, several authors have established a link between the prevention of PEs and improved pharmacological outcomes.40,41 Second, the participants of the study self-reported the outcome measures, which might have incorporated some reporting bias, influencing the validity of the outcome assessment process. Nonetheless, direct observation was not a feasible technique to report the study outcomes given the COVID-19 situation. Third, we did not investigate whether missing data during the outcome assessment could have affected the accuracy of our outcomes. Fourth, the biggest validity limitation of this study is the ambiguity of some of the stated interventions the intervention group were primed to detect. This may skew the results in favor of the intervention group given they were told to view these as mistakes and to intervene where an unbiased observer might see them as too clinically insignificant to require intervention. Finally, although we applied proportionate random sampling to recruit pharmacies from different geographic regions across Jordan, a few regions were not included in the recruitment study due to practical reasons. This might have affected the generalizability of our findings. However, the pharmaceutical and medical regulations across Jordan are unified and no significant differences in clinical practice are expected to be seen between different regions.
Conclusion
A high incidence of PEs involving COVID-19 patients in community settings were identified. The educational tool proposed in this study can help in designing a feasible and time-efficient interventional tool to encourage pharmacists’ involvement in identifying and correcting PEs in light of COVID-19.
Supplemental Material
sj-doc-1-hpx-10.1177_00185787211073506 – Supplemental material for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies
Supplemental material, sj-doc-1-hpx-10.1177_00185787211073506 for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies by Derar H. Abdel-Qader, Ahmad Z. Al Meslamani, Abdullah Albassam, Nadia Al Mazrouei, Asma A. El-Shara, Husam El Sharu, Samah Bahy Mohammed Ebaed and Osama Mohamed Ibrahim in Hospital Pharmacy
Supplemental Material
sj-docx-2-hpx-10.1177_00185787211073506 – Supplemental material for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies
Supplemental material, sj-docx-2-hpx-10.1177_00185787211073506 for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies by Derar H. Abdel-Qader, Ahmad Z. Al Meslamani, Abdullah Albassam, Nadia Al Mazrouei, Asma A. El-Shara, Husam El Sharu, Samah Bahy Mohammed Ebaed and Osama Mohamed Ibrahim in Hospital Pharmacy
Supplemental Material
sj-docx-3-hpx-10.1177_00185787211073506 – Supplemental material for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies
Supplemental material, sj-docx-3-hpx-10.1177_00185787211073506 for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies by Derar H. Abdel-Qader, Ahmad Z. Al Meslamani, Abdullah Albassam, Nadia Al Mazrouei, Asma A. El-Shara, Husam El Sharu, Samah Bahy Mohammed Ebaed and Osama Mohamed Ibrahim in Hospital Pharmacy
Supplemental Material
sj-docx-4-hpx-10.1177_00185787211073506 – Supplemental material for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies
Supplemental material, sj-docx-4-hpx-10.1177_00185787211073506 for Assessment of A new Strategy to Prevent Prescribing Errors Involving COVID-19 Patients in Community Pharmacies by Derar H. Abdel-Qader, Ahmad Z. Al Meslamani, Abdullah Albassam, Nadia Al Mazrouei, Asma A. El-Shara, Husam El Sharu, Samah Bahy Mohammed Ebaed and Osama Mohamed Ibrahim in Hospital Pharmacy
Footnotes
Acknowledgements
Our thanks go to data professionals, the statistician, pharmacists, and physicians who facilitated this work.
Author Contributions
DAQ: Proposal writing, Conceptualization, and study design development, data collection, data analysis, results’ interpretation, manuscript drafting. AZM, AB: study design development, manuscript drafting and review, data analysis, and critical appraisal. NM, AAE, and HEE: Manuscript-drafting and review, study design development, data analysis, and literature review, EJ, SBMH, and OMI: Study design development, manuscript drafting, data analysis, results’ tabulation, and critical appraisal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The ethical aspects of this study were addressed and approved by the ethics committee at the University of Petra (No: Q1/6/2020).
Availability of Data and Material
Data are available upon reasonable request.
Consent to Participate
Participants read and approved a consent form
Consent for Publication
All study participants agreed to publish this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.