
Abstract
Introduction
Patients with end-stage renal disease (ESRD) receiving dialysis are at an inherently increased risk of bleeding compared to patients with normal renal function due to various factors including uremic platelet dysfunction and anemia, among others. This risk is further increased with use of oral anticoagulant therapies, particularly in patients with a history of prior gastrointestinal bleeding. 1 As a result, this patient population has been historically excluded from major clinical trials of direct oral anticoagulants (DOAC).2 -6 Consequently, vitamin K antagonists (VKA) remain widely prescribed for venous thromboembolism (VTE) treatment for patients on dialysis. More recently, results of pharmacokinetic and observational studies have provided increased evidence supporting the safety of DOAC use compared with VKAs in patients with ESRD on dialysis, resulting in more widespread adoption of DOAC prescribing in this population.7 -11
Of the 4 DOACs currently available in the United States, apixaban undergoes relatively less renal elimination, making it an attractive option for use in patients receiving dialysis. Based on limited pharmacokinetic data, apixaban received FDA approval for use in dialysis patients with atrial fibrillation in 2014. This change included a recommendation for a dose reduction to 2.5 mg twice daily for patients receiving therapy for the indication of atrial fibrillation meeting at least 2 of the following characteristics: serum creatinine ≥ 1.5 mg/dL, weight ≤ 60 kg, age ≥80 years. 11 However, this labeling change did not address dosing recommendations for dialysis patients receiving apixaban for the indication of VTE and a dose reduction is not recommended for this indication. For VTE treatment, manufacturer prescribing information recommends an apixaban dose of 10 mg twice daily for 7 days followed by 5 mg twice daily for treatment of VTE, and no dose adjustment is suggested for any degree of renal dysfunction. 12 However, a dose reduction is suggested for extended VTE prophylaxis after completion of at least 6 months of full dose treatment of VTE. As a caveat, the manufacturer does not provide clarity on whether this recommendation applies to patients with a persistent indication for therapeutic anticoagulation, such as residual vein thrombosis after completion of initial anticoagulation therapy. In addition to atrial fibrillation and extended VTE prophylaxis, a 50% dose reduction is suggested in patients receiving a 5 or 10 mg dose of apixaban with concomitant dual P-gp and strong cytochrome P450 3A4 inhibitors, such as itraconazole or ketoconazole. 11 Previous reports of pharmacokinetic studies of apixaban 5 mg doses revealed an increase in area under the curve of 36% to 44% as well as a linear relationship between anti-Xa levels and drug levels in hemodialysis patients compared to those with normal renal function. Hemodialysis has been stated to have no clinically significant impact on apixaban clearance. Despite this information, renal dose adjustments for the indication of VTE treatment are not recommended.7 -12 Retrospective studies comparing apixaban to warfarin for treatment or prevention of VTE in ESRD patients have suggested a similar or lower risk of bleeding between treatments, but safety and efficacy outcomes of apixaban use in a population inclusive of only dialysis patients have yet to be examined in randomized, controlled studies.8-15 Notably, the indication for anticoagulation in these studies has included patients with atrial fibrillation and data exclusive to VTE in patients on dialysis is scarce. The lack of apixaban dose adjustment recommendations for patients with VTE, combined with limited, observational outcomes data in dialysis patients leads to uncertainty among providers as to the optimal apixaban dosing strategy. Dialysis patients receiving treatment of thromboses with empiric dose reductions of apixaban may be at risk of treatment failure. The study investigators hypothesized that significant dosing variation exists in apixaban prescribing for chronic dialysis patients for the indications of treatment and prevention of thrombotic indications excluding atrial fibrillation. This study aimed to characterize apixaban dosing variation in hospitalized patients in order to highlight the urgent need for additional research in this patient population.
Methods
This retrospective review took place between May 2018 and December 2020 at 3 large, regional referral healthcare systems in the southeast United States: Erlanger Health System, Huntsville Hospital, and Methodist LeBohneur Healthcare System. Study approval was received by each facility’s respective Institutional Review Boards prior to study initiation.
Adult patients receiving dialysis for at least 6 months were included if they were admitted to the hospital and received at least 2 doses of apixaban during the study period for the treatment or prevention of a VTE or other thrombotic event unrelated to atrial fibrillation. These inclusion criteria time points were designed to help identify patients on permanent dialysis and to try to exclude patients who only received a short course of apixaban during hospitalization before being switched to an alternative anticoagulant before discharge. Patients were excluded if pregnant or incarcerated at the time of admission.
The primary outcome was incidence of deviation from manufacturer recommended dosing for treatment or prevention of a VTE or other thrombotic event unrelated to atrial fibrillation. For data analysis, patients were divided into categories by indication for treatment, including acute VTE, history of VTE, chronic VTE, acute arteriovenous graft thrombosis (AVGT), chronic AVGT, and cardiac thrombus (Table 1). If the apixaban dose was modified by the prescriber during the index hospitalization, the final prescribed regimen was used for both primary and secondary outcomes.
Definitions.
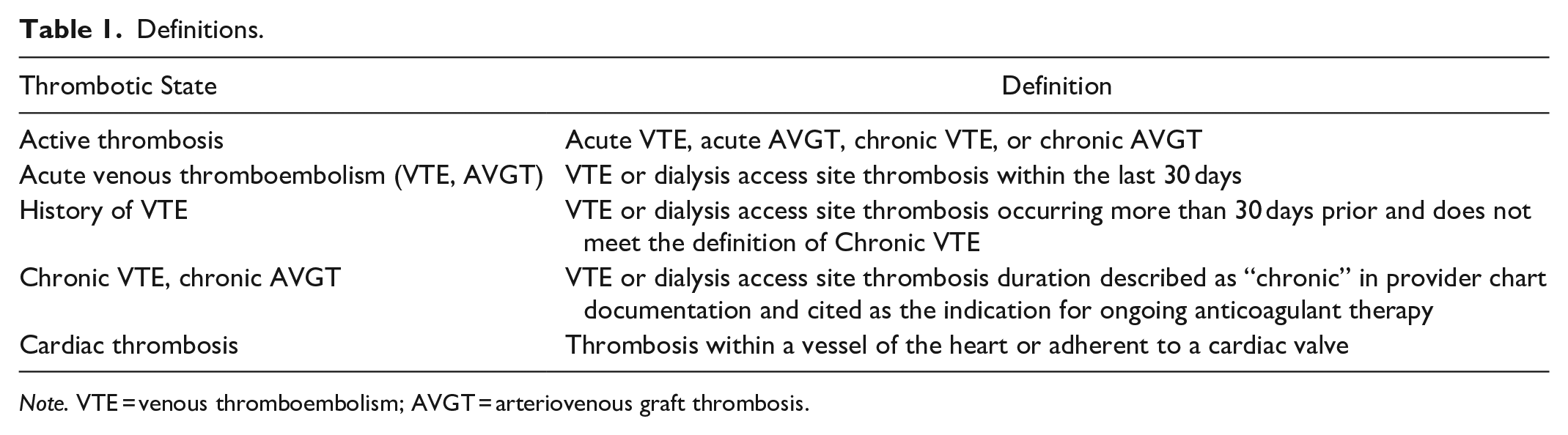
Note. VTE = venous thromboembolism; AVGT = arteriovenous graft thrombosis.
ICD-10 codes were used for identification of chronic events when documented, and by review of prior hospital encounters that revealed duration of anticoagulant use for the indication of thrombosis prior to the index hospitalization event with concurrent prescriber documentation of chronicity in the index encounter record. If patients met multiple VTE categories (ie, having an acute VTE and a history of a previous VTE), they were categorized as acute VTE. Deviation from manufacturer dosing recommendations was assessed for each type of thrombotic indication. 12 A reduced dose of apixaban 2.5 mg twice daily was considered a deviation if the treatment indication was acute VTE, or chronic VTE (including chronic arteriovenous graft thrombosis). For the purposes of this study, a chronic VTE or chronic AVGT was deemed as an indication for ongoing therapeutic anticoagulation defined as apixaban 5 mg twice daily, which does not include patients with a resolved history of a VTE. These definitions are consistent with both CHEST guideline recommendations, though it is notable that recommendations for management of chronic VTE are vague. 16 The final selected dose by the prescriber during admission was used for the primary outcome, and the discharge apixaban dose was used for reporting on recurrent thrombotic or bleeding events after hospital discharge. Receipt of an initial apixaban loading dose could not be assessed in patients with acute VTE who had apixaban continued from prior to admission due to the nature of this retrospective chart analysis and inability to assess patient records prior to the index hospitalization. In such cases, the investigators considered only a reduced dose of 2.5 mg a deviation from recommended dosing. For cases in which patients had a concomitant anticoagulation indication of atrial fibrillation, consideration was given to whether patients met criteria for a dose reduction based on manufacturer recommendations for that indication and is addressed in the results and discussion.
Secondary outcomes were assessed in all study patients captured by rehospitalization at the study site, and included recurrent VTE, major bleeding, and clinically relevant non-major bleeding. If a patient experienced more than one rehospitalization, only the first event was captured for analysis. Recurrent VTE was defined as a new diagnosis of VTE upon a subsequent hospitalization. Bleeding is classified by the International Society on Thrombosis and Hemostasis where major bleeding was defined as any acute, clinically overt bleeding plus at least one of the following: decrease in hemoglobin of at least 2 g/dL, bleeding that required the transfusion of 2 units or more of blood products (packed red blood cells or fresh frozen plasma), bleeding in at least 1 critical site (intracranial, intraspinal, intraocular, pericardial, intra-articular, intramuscular with compartment syndrome, or retroperitoneal), or fatal bleeding. 17 Clinically relevant non-major bleeding was defined as clinically overt bleeding that did not satisfy the criteria for major bleeding and led to hospital admission for bleeding, physician-guided medical or surgical treatment for bleeding, or a change in anticoagulation therapy due to bleeding. Finally, recurrent VTE and bleeding events were described according to patient dosing regimen. After data collection at each site, de-identification of patient records was completed and data were combined for analysis. Data were recorded in Research Electronic Data Capture and analyzed with descriptive statistics. (Version 6.18.1, 2019; Vanderbilt University, Nashville, TN). 18
Results
A total of 101 charts were included for analysis, divided as: Erlanger Health System (n = 26), Huntsville Hospital Health System (n = 17), and Methodist Le Bonheur Healthcare (n = 58). Demographics and baseline characteristics are displayed in Table 2.
Demographics (n = 101).
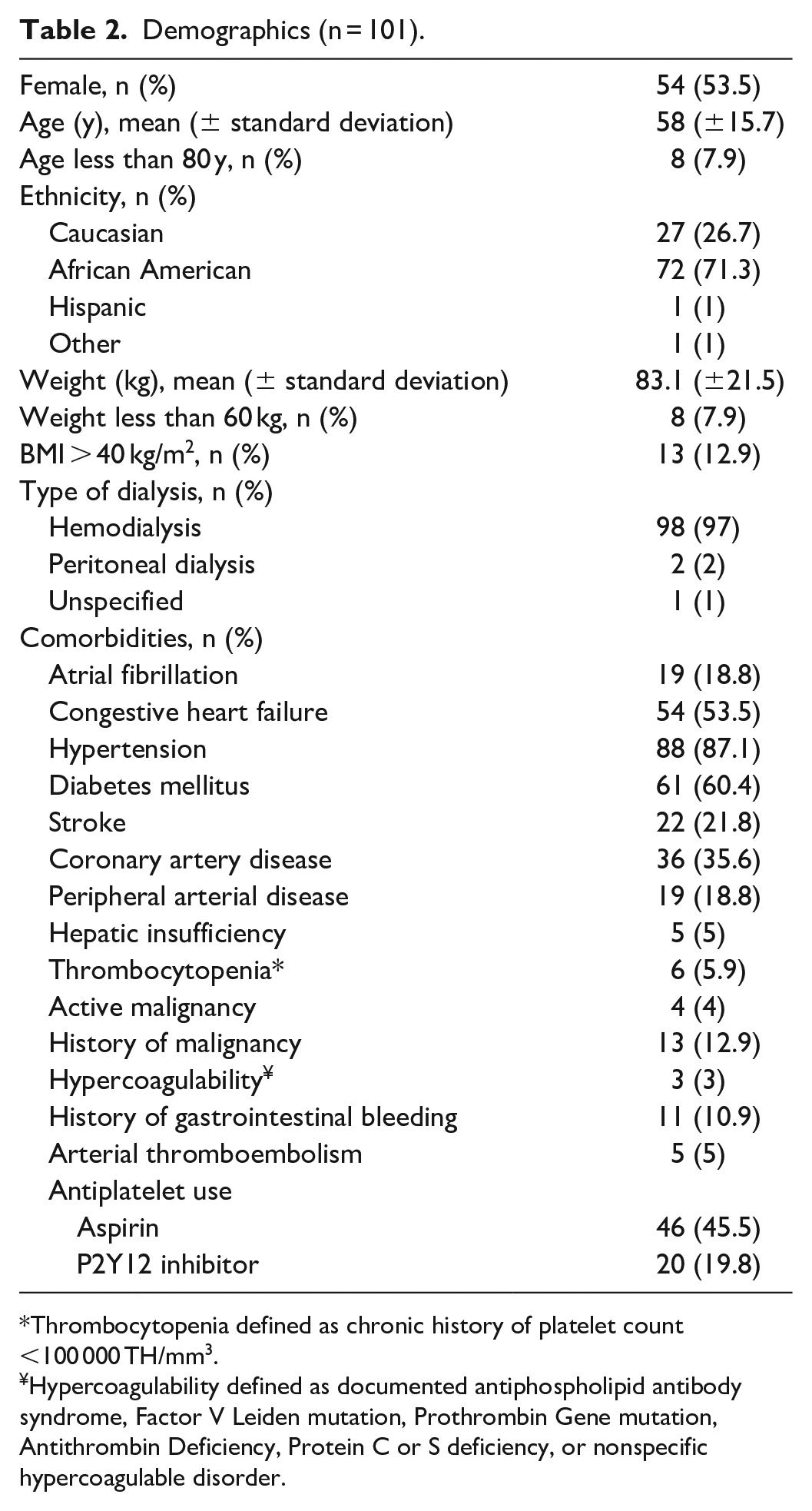
Thrombocytopenia defined as chronic history of platelet count <100 000 TH/mm3.
Hypercoagulability defined as documented antiphospholipid antibody syndrome, Factor V Leiden mutation, Prothrombin Gene mutation, Antithrombin Deficiency, Protein C or S deficiency, or nonspecific hypercoagulable disorder.
Approximately 19% of patients had concomitant atrial fibrillation. Thrombosis sites are characterized in Table 3. No patient had a sole indication of a superficial vein thrombosis. For data analysis, apixaban dosing regimens were divided into 2 groups based on timing of therapy initiation: during index hospitalization (n = 54, 53.4%) or prior to admission (PTA; n = 47, 46.5%).
Thrombosis Sites.
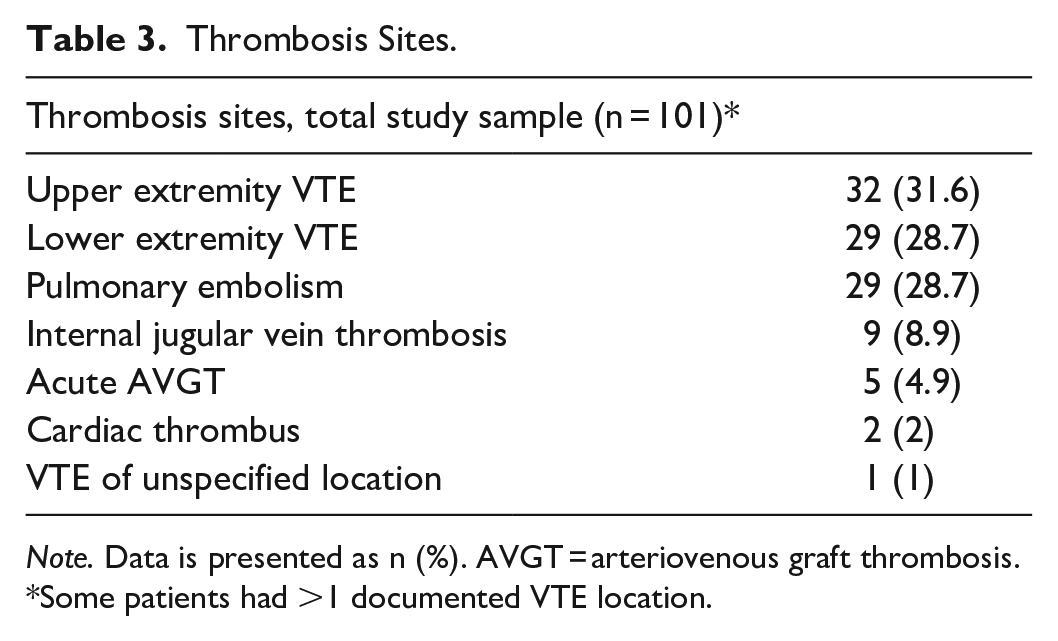
Note. Data is presented as n (%). AVGT = arteriovenous graft thrombosis.
Some patients had >1 documented VTE location.
A detailed breakdown of VTE types is displayed in Figure 1. The primary prescribing specialty was hospitalist (79.6%), followed by hematology (5.5%) and cardiology (5.5%). Of the patients who were started on apixaban during the index hospitalization (n = 54), 38 (70.3%) received a dose incongruent with manufacturer recommendations, as follows. Forty-four (81.4%) patients had an acute VTE. Of those, only 9 (20.4%) received a regimen that included the recommended loading dose. Twelve (27.2%) of these patients received an off-label reduced dose of 2.5 mg twice daily (Figure 1A). Two patients with a chronic VTE and 1 patient with an acute AVGT received an off-label dose of 2.5 mg twice daily.
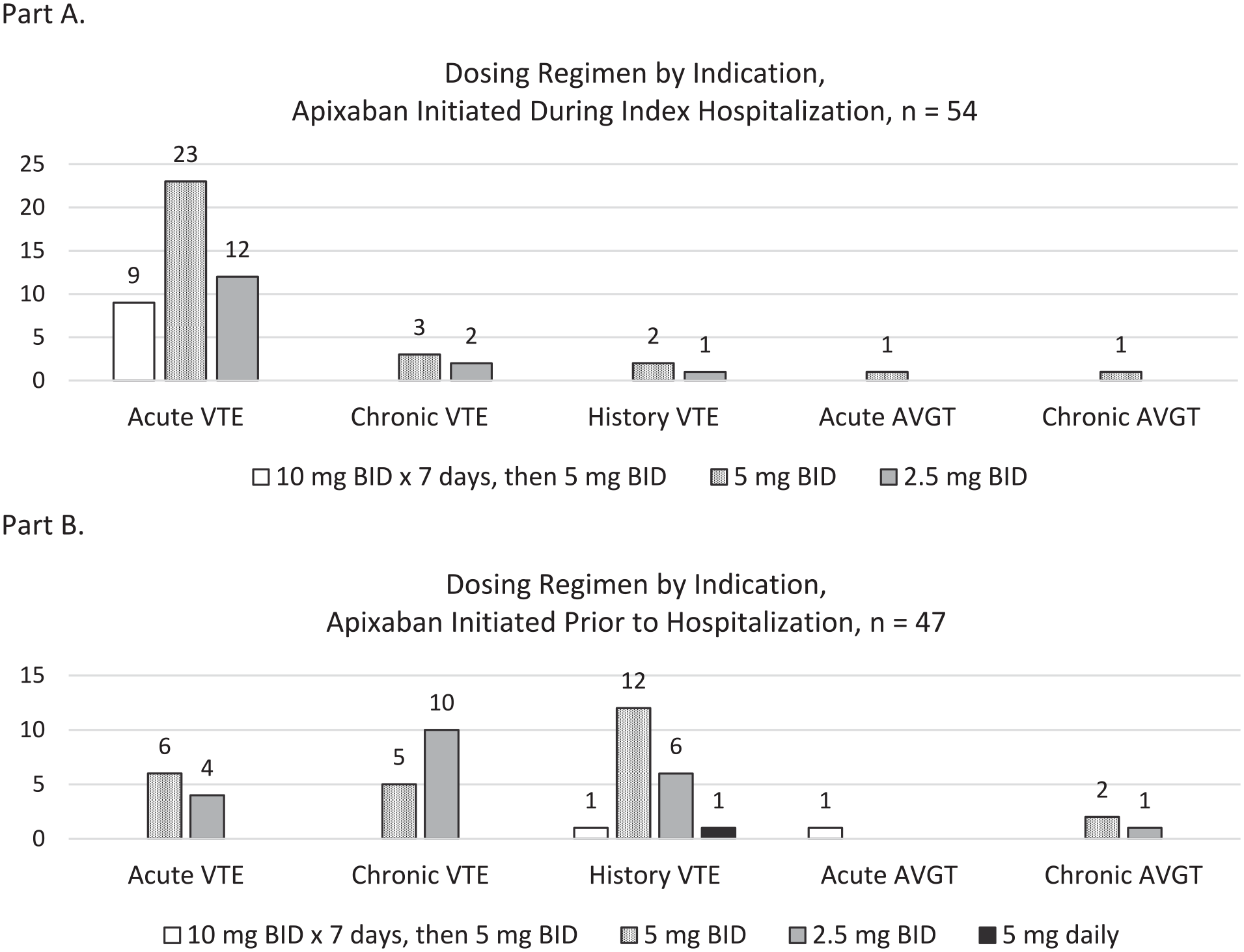
Apixaban dosing regimens by indication: Part (A) Initiated during index hospitalization and Part (B) initiated prior to index hospitalization.
Examination of dosing regimens for the 47 patients who were taking apixaban prior to hospitalization revealed similar variance in hospital prescribing patterns (Figure 1B). Of the patients with an acute VTE who were taking apixaban PTA, 4 (10%) patients received an off-label dose of apixaban 2.5 mg twice daily. In the PTA group, determination of receipt of a loading dose from chart review was not possible, thus lack of an observed loading dose was not considered as a deviation from recommended dosing for this group. Additionally, in the combined analysis of both PTA and initiation-on-hospitalization groups for active thrombotic indications (acute VTE, acute AVGT, chronic VTE, chronic AVGT), 53 of 80 (66.2%) patients received an off-label dose. This included a 5 mg twice daily regimen with omission of a loading dose in 24 patients with an acute DVT started on apixaban during hospitalization (23 acute VTE and 1 acute AVGT), initiation of 2.5 mg twice daily in 16 patients with acute VTE (started both during hospitalization and PTA), and 2.5 mg twice daily in 13 patients with chronic VTE and chronic AVGT. No patient with concomitant atrial fibrillation met manufacturer criteria for a dose reduction, however a history of gastrointestinal or intracranial hemorrhage was observed in 6 patients receiving a reduced dosing regimen. A dose adjustment prior to hospital discharge was observed in 9 patients in the group receiving apixaban initiation during hospitalization.
Recurrent VTE and bleeding events were observed in 21 (20.7%) patients during the study period. This was broken down as rehospitalization for a recurrent VTE in 12 (11.8%) patients, major bleeding in 9 (8.9%) patients, clinically relevant non-major bleeding in 1 patient. Recurrent VTE and major bleeding events stratified by apixaban dose are displayed in Table 4. Of 36 patients receiving a reduced dose of 2.5 mg, rehospitalization for a recurrent VTE was observed in 6 (16.6%) patients, and a major bleeding event was observed in 4 (11%) patients. Mean time to event was 2.3 months (range 1-6 months).
Recurrent VTE and Major Bleeding Events by Dosing Regimen at Hospital Discharge (n = 21).
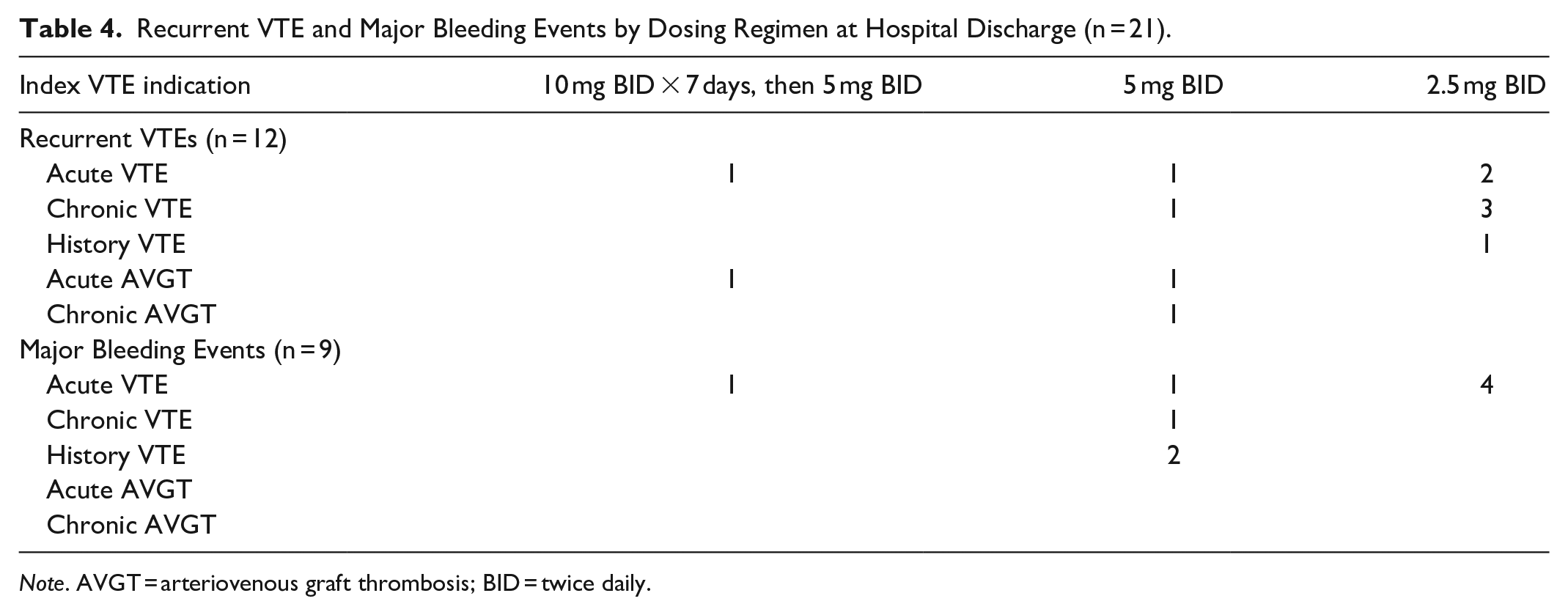
Note. AVGT = arteriovenous graft thrombosis; BID = twice daily.
Discussion and Conclusion
In this retrospective, multicenter study we observed common off-label apixaban dosing for thrombotic indications in dialysis patients. To our knowledge, this is the largest study of its kind to date inclusive only of a chronic dialysis population receiving apixaban for a thrombotic indication other than atrial fibrillation. Overall, there was a tendency to omit loading doses and frequent use of a reduced dose of 2.5 mg twice daily for acute VTE treatment, neither of which are recommended by the manufacturer. We also observed higher rates of bleeding and VTE recurrence compared to historic data, though it is important to consider the variable stages of renal failure and follow-up periods assessed in previous studies when making such a comparison.2 -5 While we chose to report on the occurrence of rehospitalization events for VTE and bleeding, it was not possible to make meaningful conclusions about possible correlation of such events with apixaban dosing regimens due to the limitations inherent to a small, retrospective analysis.
Deviation from apixaban prescribing recommendations for dialysis patients is not surprising given the lack of robust outcomes data and the available pharmacokinetic data indicating an increased serum drug exposure with unadjusted dosing when compared to patients with normal renal function. 7 In an evaluation of apixaban steady state pharmacokinetics in dialysis patients, Mavrakanas et al 19 demonstrated an increased area under the curve by 2- to 5.7-fold with a regimen of 5 mg twice daily compared to 2.5 mg twice daily. Although clinical outcomes were not assessed in this study, this information may lead prescribers to empirically reduce the apixaban dose for dialysis patients with a VTE due to an inferred increased risk of bleeding, especially since 10 mg doses have not previously been studied in patients receiving dialysis.
A more recent retrospective cohort study of 124 dialysis patients receiving either apixaban or warfarin demonstrated reduced rates of overall bleeding with an apixaban 5 mg twice daily regimen (18.9% vs 42%, P = .01). 13 In this study, 34 (46%) patients received apixaban for treatment of VTE, and 11 (14.9%) patients received apixaban for VTE prophylaxis. Patients receiving apixaban had reduced rates of major bleeding (5.4% vs 22.0%, P = .01) and a numeric but non-significant reduction in recurrent VTE in compared to warfarin (4.4% vs 28.6%, P = .99). Notably, 79% of all patients on apixaban received the manufacturer recommended dose of apixaban 5 mg twice daily for the indication of VTE treatment yet, 20.9% of patients study still received a reduced dose of 2.5 mg twice daily. The authors pointed out that these patients met criteria for a dose reduction based on the previously mentioned manufacturer dosing recommendations for atrial fibrillation or lifelong prophylactic dosing after initial treatment for VTE. This is in contrast to our study, where none of the patients with concomitant atrial fibrillation met criteria for a dose reduction. Thus, it is unlikely that dose reductions were employed for this reason, and leads us to believe that prescribers utilized empiric dose reductions due to concerns for bleeding with standard, therapeutic apixaban dosing. It is notable that only one patient met 2 of 3 of these criteria and was receiving a reduce dose of apixaban 2.5 mg twice daily without a history of atrial fibrillation. Similar to our study, the authors reported a low rate of apixaban loading doses for patients with acute VTE of just 8.8%, compared with 20.4% of patients in our study. Another retrospective analysis of apixaban dosing across 4 healthcare systems in 861 patients with a calculated creatinine clearance less than 25 mL/min based on exclusion criteria from landmark studies of apixaban was performed by Hanni et al. In this study, 25 patients were receiving apixaban for VTE treatment or prevention or for a cardiac thrombus, and 21 (16%) patients were receiving dialysis. The authors reported an incorrect apixaban dose reduction to 2.5 mg twice daily was observed in 16.4% of the total study sample but did not specifically report the frequency of reduced dosing in patients receiving dialysis. 14 While it is important to note the findings of this study and the contribution to the aggregate data of apixaban use in dialysis patients, the findings cannot be directly compared to our data due to differences in sample size and study populations. When combining the evidence provided by Reed et al and Hanni et al with the results of our study, it is clear that apixaban dosing deviations from manufacturer recommendations are common which is attributed to a lack of outcomes-based guidance.
Prescriber concerns for bleeding may lead to off-label dose reductions that pose risk for therapy failure. Our observation of documented history of either gastrointestinal bleeding or intracranial hemorrhage in 6 of 36 patients receiving reduced dosing indicates that an increased risk of bleeding is likely a factor when prescribing lower doses. In addition to omission of loading doses for acute VTE treatment, the use of the 2.5 mg twice daily regimen for treatment of an acute thrombosis is concerning. Prospective studies evaluating rates of VTE recurrence with a reduced-dose apixaban treatment regimen are lacking. However, this concept of a reduced-dose approach was recently studied in a population of dialysis patients receiving rivaroxaban for atrial fibrillation. De Vriese et al 20 conducted a randomized, controlled study evaluating cardiovascular event rates in 132 patients with ESRD receiving either warfarin or reduced-dose rivaroxaban for atrial fibrillation. Use of rivaroxaban 10 mg once daily resulted in reduced rates of a composite endpoint of fatal and non-fatal stroke and cardiovascular events (HR 0.41, 95% CI 0.025-0.68) as well as major bleeding (HR 0.39, 95% CI 0.017-0.90) compared with warfarin. Although these results raise questions about the possibility of extrapolated data into a possible benefit of reduced DOAC doses for VTE treatment, implementation of a reduced-dose approach with apixaban for treatment of VTE in dialysis patients is premature and may place patients at increased risk of VTE recurrence.
The unclear definition of chronic VTE and lack of guideline recommendations on anticoagulation management of chronic venous thromboembolism may further contribute to uncertainty regarding on apixaban dose considerations. A recent VTE management guideline update published by the American College of Chest Physicians provides a weak recommendation for use of a reduced dose Xa inhibitor in patients who have been selected to receive extended phase anticoagulant therapy with very low certainty of evidence. 16 However, this guideline did not provide clarity as to whether this recommendation applies to patients with evidence of chronic VTE. 16 Chronicity of VTE was not elucidated in the demographics of the AMPLIFY-Extend trial in which reduced-dose apixaban was studied after completion of 6 months of full dose therapy. 21 Thus it is difficult to extrapolate the findings of this study to patients with chronic VTE. Moreover, presence of a residual thrombus after initial DVT treatment has been associated with an increased risk of recurrence. In a multicenter, prospective study, Siragusa et al compared rates of VTE recurrence in patients with residual vein thrombosis who received continued anticoagulation therapy beyond 3 months with those who stopped anticoagulation therapy. 22 Their findings suggested that patients with residual vein thrombosis who stopped anticoagulation therapy after 3 months were at increased risk for VTE recurrence. For the purposes of this study, we considered chronic VTE to be an indication for therapeutic anticoagulant dosing, given the known long term complications of chronic DVT in which there is failed vessel recanalization, the lack of a manufacturer recommendation for a dose adjustment in this population, and uncertainty as to whether guideline recommendations for extended therapy applies to patients with chronic VTE. 23
There are several limitations to our study. Although our study was comprised of patients from 3 health care systems, the study sample size was relatively small, and as with any retrospective evaluation, our data is dependent on accurate chart records. Assessment of safety outcomes was limited to the data available from subsequent hospitalizations and included only readmissions within participating hospital systems. Outpatient only data and data related to admissions at other facilities were not captured. Retrospective review may also limit interpretation of patients receiving therapy for history of a VTE. Although the CHEST guidelines use the terminology “Initiation Phase” for the time frame of 5 to 21 days after VTE diagnosis, the authors elected to use the prior 30 days to define “Acute VTE” as it is generally accepted that the first 30 days after VTE diagnosis is designated as a period of high risk for thrombus extension, particularly when untreated. 16 The indication for a reduced dose of 2.5 mg twice daily is designated for patients who have completed at least 6 months of therapy for VTE treatment and elect to continue chronic anticoagulation therapy for perceived continued risk factors for recurrent VTE, but may be at increased risk of bleeding with full therapeutic dosing. This was considered in our analysis of dosing appropriateness, and a primary reason for excluding patients receiving therapy PTA with a history of VTE of unspecified duration from this outcome, due to the fact that the exact timing of VTE diagnosis could not always be determined from retrospective chart analysis. Statistical analysis for correlation of dose with recurrent events was not conducted due to small sample size and number of recurrent events. Data on administration of dual P-glycoprotein and strong CYP3A4 inhibitors was not collected, however, the number of these agents mentioned in the medication prescribing information is few and prescribing of such agents in uncommon.
Additionally, anticoagulation practice for thrombosis of vascular access sites in dialysis patients may vary among providers and healthcare institutions given the lack of robust guidance on treatment. In the present study, the investigators confirmed through chart review that AVGT was the sole indication for apixaban therapy. However, provider rationale for adjusted doses of apixaban could not be elucidated and there is no consensus guidance on optimal anticoagulation strategies for this indication. Thrombotic events including AVGT may also have been managed with non-pharmacologic interventions and procedures also not captured in this analysis. Lead-in therapy with parenteral anticoagulation prior to initiation of apixaban was also not assessed. The manufacturer does not address this consideration in published prescribing information, and some providers may elect to omit or modify the duration of an apixaban loading dose for patients who have received parenteral anticoagulation prior to transitioning to oral anticoagulation therapy. However, it should be noted that this practice would be considered off-label until further information is available. Calibrated anti-Xa serum levels were not available for quantitative assessment of apixaban concentrations to guide dosing at any study site, though it is important note that such monitoring is not recommended in clinical practice. Finally, none of the included facilities have automatic dose-adjustment policies for apixaban but due to the retrospective nature of this study, we were not able to determine whether pharmacists had attempted to intervene or recommend a dose adjustment that was not accepted by the prescriber.
Although observational studies have provided evidence of safety with apixaban 5 mg twice daily in dialysis patients, our analysis suggests the possibility of prescriber unfamiliarity or hesitancy to utilize recommended doses and common omission of loading doses for acute VTE treatment.12,16,18 Such practice may place patients at increased risk of treatment failure. Further, while the finding of higher rates of recurrent thrombotic events as compared to historic studies in the present analysis is notable, a direct correlation cannot be made given the descriptive nature of this analysis and the fact that dialysis patients were not included in clinical trials with DOACs. Larger, prospective, controlled studies evaluating safety and efficacy outcomes of apixaban at both full therapeutic and dose-adjusted regimens in patients on dialysis are urgently needed to guide prescribing practices in patients with VTE. Further, updates to anticoagulation guidelines for VTE treatment are needed to include specific recommendations for dialysis patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.