
Abstract
Each month, subscribers to The Formulary Monograph Service receive 5 to 6 well-documented monographs on drugs that are newly released or are in late phase 3 trials. The monographs are targeted to Pharmacy & Therapeutics Committees. Subscribers also receive monthly 1-page summary monographs on agents that are useful for agendas and pharmacy/nursing in-services. A comprehensive target drug utilization evaluation/medication use evaluation (DUE/MUE) is also provided each month. With a subscription, the monographs are available online to subscribers. Monographs can be customized to meet the needs of a facility. Through the cooperation of The Formulary, Hospital Pharmacy publishes selected reviews in this column. For more information about The Formulary Monograph Service, contact Wolters Kluwer customer service at 866-397-3433.
Indications
Terlipressin is indicated to improve kidney function in adults with hepatorenal syndrome with rapid reduction in kidney function; patients with a serum creatinine (SCr) greater than 5 mg/dL are unlikely to experience benefit. 1
Other possible uses for terlipressin include management of living organ donors, gastroesophageal variceal bleeding, cirrhosis with refractory ascites, septic shock, and multiple other uses. 2
Clinical Pharmacology
Terlipressin is a synthetic vasopressin analog that is more selective for vasopressin V1 receptors than V2 receptors, with selectivity for V1 receptors twice that of V2 receptors. Terlipressin acts as a prodrug for its metabolite (lysine-vasopressin), and also has pharmacologic activity on its own. 1 Lysine-vasopressin is a nonselective vasopressin analog that binds to V1 and V3 receptors. 3 Terlipressin is thought to increase renal blood flow in patients with hepatorenal syndrome by reducing portal hypertension and blood circulation in portal vessels and increasing effective arterial volume and mean arterial pressure (MAP).1,3
In patients with hepatorenal syndrome, terlipressin increased diastolic, systolic, and MAP and decreased heart rate within 5 minutes after a single intravenous (IV) dose of 0.85 mg. The maximum changes in blood pressure and heart rate occurred at 1.2 to 2 hours after administration. The estimated maximum effect for MAP was an increase of 16.2 mm Hg, and the maximum effect for heart rate was a decrease of 10.6 bpm. The effects on blood pressures and heart rate were maintained for at least 6 hours. 1
No clinically meaningful changes from baseline in QTc interval were observed in 41 patients with hepatorenal syndrome given terlipressin every 6 hours for 14 days. 1
Pharmacokinetics
After IV administration of terlipressin 1 mg, median Cmax was 70.5 ng/mL, AUC24h was 123 ng/hour/mL, and Cave was 14.2 ng/mL for terlipressin and 1.2 ng/mL, 11.2 ng/hour/mL, and 0.5 ng/mL, respectively, for its active metabolite (lysine-vasopressin). Changes in terlipressin and lysine-vasopressin pharmacokinetics were linear, and the plasma concentrations increased proportionally to the dose administered. 1
Terminal half-life was 0.9 hours for terlipressin and 3 hours for lysine-vasopressin. Volume of distribution was 6.3 L for terlipressin and 1370 L for lysine-vasopressin. Clearance was 27.4 L/hour for terlipressin and 318 L/hour for lysine-vasopressin; increased body weight was associated with increased clearance of terlipressin and no change in the clearance of lysine-vasopressin. 1
Terlipressin is metabolized by cleavage of the N-terminal glycyl residues of terlipressin by various tissue peptidases, resulting in release of lysine-vasopressin. The metabolite is then metabolized by body tissue via various peptidase-mediated pathways. It is unlikely that the metabolism of terlipressin and lysine-vasopressin will be affected by disease state or other drugs. 1
Urinary excretion accounts for less than 1% of terlipressin excretion and less than 0.1% of lysine-vasopressin excretion. 1
Sex, age, creatinine clearance, liver impairment, serum alkaline phosphatase, serum ALT, serum AST, and total bilirubin do not appear to have any clinically significant effect on clearance of either terlipressin or lysine-vasopressin. 1
Comparative Efficacy
Indication: Hepatorenal Syndrome
Guidelines
Studies
At baseline, mean patient age in both treatment groups was approximately 54 years; 60% of patients in the terlipressin group and 58% in the placebo group were male; the main cause of liver cirrhosis was alcohol use (67% and 66%, respectively), and nonalcoholic steatohepatitis (21% and 24%); alcoholic hepatitis was present in 41% and 39%; systemic inflammatory response syndrome was present in 42% and 48%; SCr was 3.5 mg/dL in both groups; albumin level was 3.7and 4 g/dL, respectively; Child-Pugh score was 10 and 10.2; MEDL score was 32.7 and 33.1; and 61% and 60% had received midodrine and octreotide.
Concomitant albumin was used in 83% of the terlipressin group and 91% of the placebo group. The mean total dose of albumin was 199 g over a median of 5 days in the terlipressin group and 239.5 g over a median of 5.5 days in the placebo group.
Results
Verified reversal of hepatorenal syndrome (defined as 2 consecutive SCr measurements of 1.5 mg/dL or lower at least 2 hours apart up to day 14 and survival without renal replacement therapy for at least 10 days) occurred in 32% of patients in the terlipressin group and 17% in the placebo group (P = .006).
Competing events: Liver transplantation occurred in 5% of the terlipressin group and 2% of the placebo group, and death occurred in 3% and 0%, respectively.
Hepatorenal syndrome reversal (defined as SCr level of 1.5 mg/dL or lower while receiving terlipressin or placebo) occurred in 39% of patients in the terlipressin group and 18% in the placebo group (P < .001).
Durability of hepatorenal syndrome reversal (defined as hepatorenal syndrome reversal without renal replacement therapy through 30 days) occurred in 34% of patients in the terlipressin group and 17% in the placebo group (P = .001).
Hepatorenal syndrome reversal among patients with systemic inflammatory response syndrome occurred in 37% in the terlipressin group and 6% in the placebo group (P < .001).
Verified reversal of hepatorenal syndrome without recurrence through day 30 occurred in 26% in the terlipressin group and 17% in the placebo group (P = .08).
At day 90, liver transplantations had occurred in 23% of patients in the terlipressin group and 29% in the placebo group, and death occurred in 51% and 45%, respectively.
In an analysis of patients 65 years and older (53 patients [35 in the terlipressin group and 18 in the placebo group]), results showed terlipressin may improve post–liver transplant outcomes. Mean Model for End-Stage Liver Disease (MELD) score was 27.5 in the terlipressin group and 30.3 in the placebo group; however, there were too few patients for a statistical assessment. 7
Other studies have shown terlipressin with albumin can have a beneficial effect in some patients with hepatorenal syndrome-acute kidney injury, but its use is also associated with some important adverse reactions.8 -12
Pooled analysis from 3 phase 3 studies (OT-0401, REVERSE, and CONFIRM) found terlipressin-treated patients with hepatorenal syndrome and lower baseline SCr had a higher rate of hepatorenal syndrome reversal and survival than placebo. 8 In a subgroup analysis of patients with SCr of 3 to 5 mg/dL, both males and females had improvement in overall response rate (complete [defined as hepatorenal syndrome reversal with a SCr of 1.5 or less] and partial response [at least 30% improvement in SCr]) with terlipressin compared with placebo, but males were more likely to have an improvement in complete response and overall response rates. 13
A cost effectiveness analysis using data from a university medical center in Brazil determined that terlipressin in combination with albumin for the treatment of hepatorenal syndrome is cost-effective compared with norepinephrine in combination with albumin. 14
Contraindications, Warnings, and Precautions
Contraindications
Terlipressin is contraindicated in patients experiencing hypoxia or worsening respiratory symptoms and in patients with ongoing coronary, peripheral, or mesenteric ischemia. 1 Though not stated in the product labeling, a potential contraindication is hypersensitivity to terlipressin or any of its inactive ingredients (ie, mannitol, glacial acetic acid, and sodium hydroxide).
Warnings and Precautions
The terlipressin product labeling includes a boxed warning regarding the risk of serious or fatal respiratory failure. Patients with volume overload or with grade 3 acute-on-chronic liver failure (ACLF) are at increased risk. Assess oxygenation saturation (eg, SpO2) before initiating terlipressin. Treatment should not be initiated if the patient is experiencing hypoxia (eg, SpO2 less than 90%) until oxygenation levels improve. Monitor patients for hypoxia using continuous pulse oximetry during treatment, and discontinue treatment if SpO2 decreases below 90%. In addition, monitor for intravascular volume overload and manage accordingly, including by reducing or discontinuing administration of albumin and/or other fluids, judicious use of diuretics, or temporary interruption, reduction, or discontinuation of terlipressin treatment until patient volume status improves.1,15
Some adverse reactions associated with terlipressin therapy (eg, respiratory failure and ischemia) may make the patient ineligible for liver transplant. The potential benefits of terlipressin may not outweigh its risks in patients with a high prioritization for liver transplantation (MELD score of 35 or greater).1,16
Ischemic events (ie, cardiac, peripheral, or mesenteric ischemia) may occur because of terlipressin’s vasoconstrictive properties. Adjustments in terlipressin therapy (ie, interruption, discontinuation) may be necessary. Terlipressin therapy should be avoided in patients with a history of severe cardiovascular conditions, cerebrovascular disease, and ischemic disease. 1
Use during pregnancy is not recommended; terlipressin may cause fetal harm or induce uterine contractions and endometrial ischemia if used during pregnancy. If used during pregnancy, the patient should be informed of the potential risk to the fetus. 1
There are no data regarding the presence of terlipressin or its metabolites in human milk, or their effects on breastfeeding infants or milk production. 1
Safety and effectiveness of terlipressin have not been established in pediatric patients. 1 The requirement for pediatric studies has been waived because of terlipressin’s orphan drug status. 17
Adverse Reactions
The most common adverse reactions (10% or greater incidence) associated with terlipressin therapy included abdominal pain, nausea, respiratory failure, diarrhea, and dyspnea (see Table 1). 1
Adverse Reactions (≥4% Incidence) Reported in the CONFIRM Trial. 1
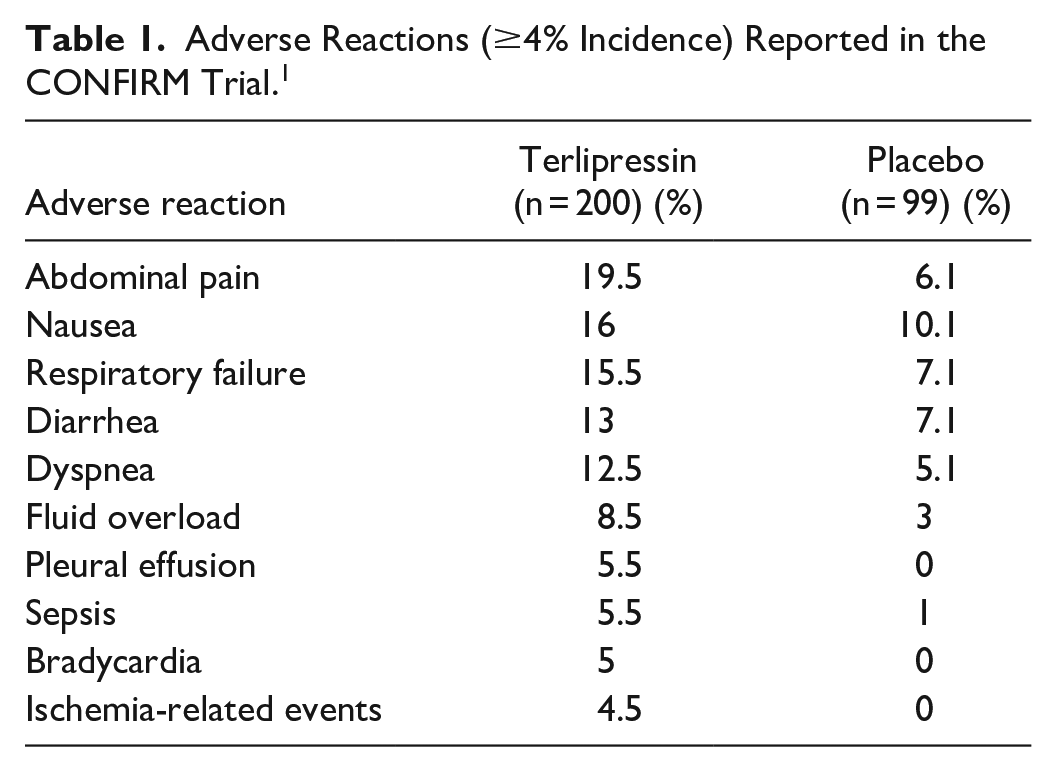
The average terlipressin dose in the CONFIRM trial was 3.1 mg (range, 0.8-5.8 mg), with a mean duration of exposure of 6.2 days (range, 1-15 days). Discontinuation related to adverse events (ie, respiratory failure, abdominal pain, intestinal ischemia/obstruction) was required in 12% of patients in the terlipressin group and 5.1% in the placebo group. 1
The ischemia-related adverse reactions include skin discoloration, cyanosis, ischemia, and intestinal ischemia.1,18
Drug Interactions
No pharmacokinetic drug-drug interactions are anticipated with terlipressin. 1
Recommended Monitoring
Serum creatinine (baseline and periodically during therapy); oxygen saturation (baseline and during therapy via continuous pulse oximetry and clinical assessments); ACLF grade and volume status (baseline and periodically during treatment); signs and symptoms of fluid overload or ischemia. 1
Dosing
The recommended initial terlipressin dose is 0.85 mg IV every 6 hours on days 1 to 3. Administration is via slow IV bolus injection over 2 minutes. On day 4, dose should be adjusted based on changes from baseline in SCr: if SCr is decreased by at least 30% from baseline, the dose should be continued at 0.85 mg every 6 hours; if SCr is decreased by less than 30% from baseline, the dose should be increased to 1.7 mg IV every 6 hours; if SCr is at or above baseline, terlipressin should be discontinued. Terlipressin should be continued until 24 hours after 2 consecutive SCr levels of 1.5 mg/dL or lower at least 2 hours apart, or for a maximum of 14 days. 1
No dosing adjustments are necessary for patients with hepatic impairment. 1
The vial is reconstituted with 5 mL of sodium chloride 0.9% injection to prepare a 0.85 mg per 5 mL solution. The drug can be administered through a peripheral or central line; the IV line should be flushed after each administration. A dedicated central line is not required. 1
If the solution is not used immediately, it should be stored at 2°C to 8°C (36°F-46°F) for up to 48 hours. Do not freeze. The reconstituted solution does not require protection from light. 1
Product Availability and Storage
Terlipressin was approved by the Food and Drug Administration (FDA) on September 14, 2022. 17 Terlipressin is available as a sterile, lyophilized powder for reconstitution in a single-dose vial containing terlipressin 0.85 mg. 1
The vials should be stored refrigerated at 2°C to 8°C (36°F-46°F) in the original carton to protect from light until time of reconstitution. 1
Drug Safety/REMS
No REMS is required for terlipressin. 17
Conclusion
Terlipressin is FDA approved to improve kidney function in adults with hepatorenal syndrome with rapid reduction in kidney function; patients with a SCr greater than 5 mg/dL are unlikely to experience benefit. Terlipressin is the first drug approved for this indication. Prior to FDA approval, the European treatment guidelines recommended terlipressin plus albumin as first-line treatment for acute kidney injury from hepatorenal syndrome.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.