
Abstract
Introduction
Antiarrhythmic drugs (AAD) play a critical role in the treatment of cardiac arrhythmias. Dofetilide, a class III antiarrhythmic agent, is indicated for the conversion and maintenance of normal sinus rhythm in patients with symptomatic atrial fibrillation or atrial flutter. 1 Because of its proarrhythmic effects (primarily torsade de pointes [TdP]), dofetilide initiation requires hospital admission for continuous electrocardiogram (ECG) monitoring under the presence of personnel trained in the management of atrial and ventricular arrhythmias.
The risk of TdP may be affected by numerous variables including advanced age, baseline QTc interval prolongation, bradycardia, cardiac structural or conduction abnormalities, concurrent use of more than one QTc-prolonging drug, electrolyte abnormalities, female sex, and impaired drug metabolism (hepatic dysfunction, renal dysfunction, or drug-drug interactions [DDIs]). 2 To reduce the risk of TdP associated with dofetilide, the Clement J. Zablocki Veterans Affairs Medical Center (ZVAMC) has a standard operating protocol in place for dofetilide initiation that involves assessment of each planned admission by the electrophysiology provider and the inpatient cardiology pharmacist (Figure 1). Historically, this process has not included inpatient cardiology pharmacist assessment prior to admission.
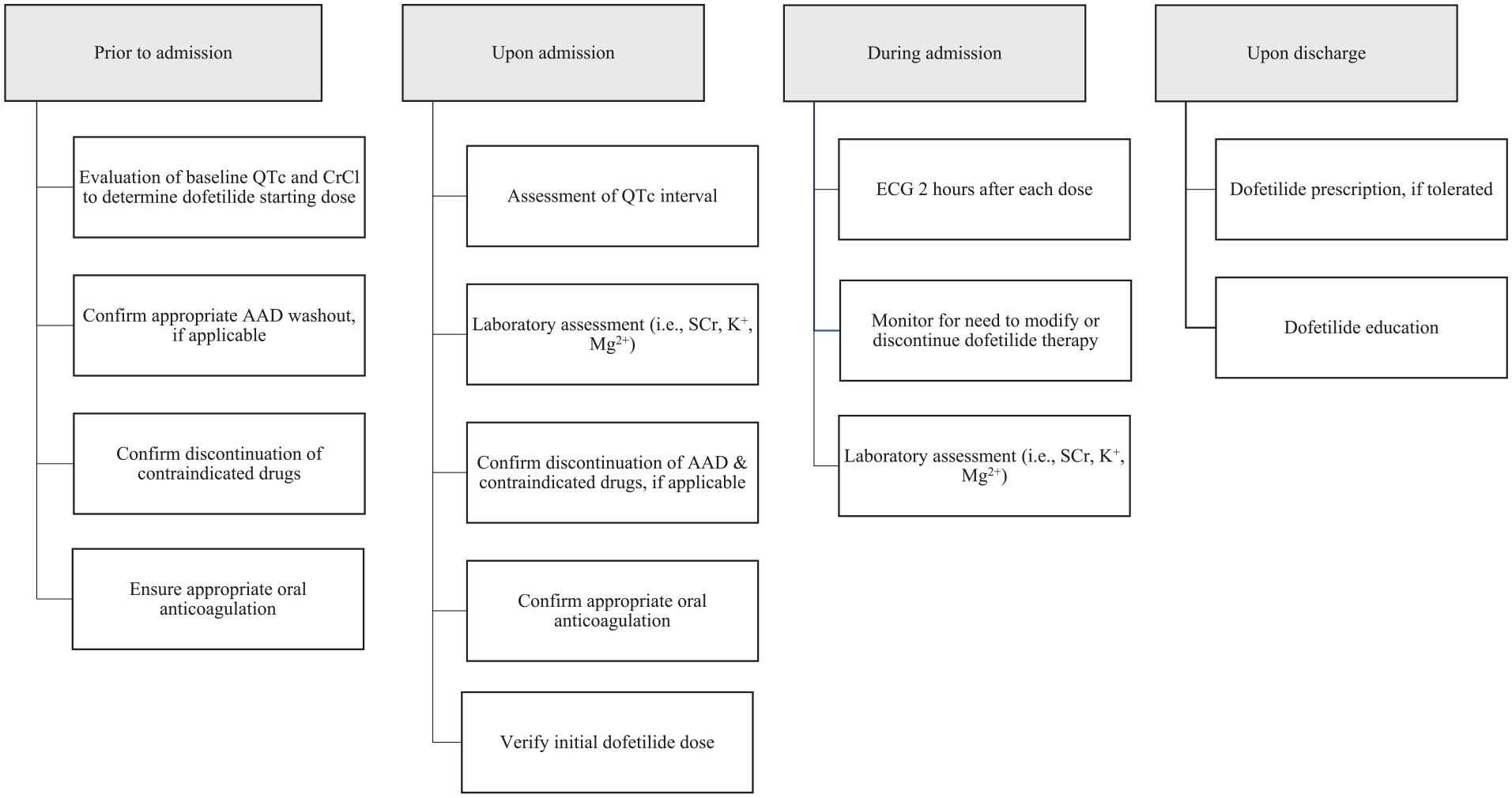
ZVAMC Standard operating protocol for dofetilide initiation (simplified process)Note. AAD= antiarrhythmic drugs; CrCl= creatinine clearance; ECG= electrocardiogram; K+= potassium; Mg2+= magnesium; SCr= serum creatinine; ZVAMC= Clement J. Zablocki Veterans Affairs Medical Center.
Dofetilide initiation has occasionally been delayed or canceled upon admission because of potential safety concerns identified by the inpatient cardiology pharmacist. These safety concerns primarily include the presence of significant DDIs and inadequate oral anticoagulation. Although assessment of DDIs and anticoagulation status should be completed when scheduling an admission for dofetilide initiation, this assessment is not always done thoroughly or accurately for reasons including incomplete or inaccurate medication history taking, failure to identify and address significant DDIs, incomplete assessment of anticoagulation status, and lack of coordination with outpatient anticoagulation providers to ensure appropriate anticoagulation prior to admission. These problems may be exacerbated in patients who obtain their primary care outside of the ZVAMC, as healthcare records must be accessed through a separate electronic interface that electrophysiology providers may be unaware of or fail to review when evaluating patients for dofetilide initiation. Lack of review or access to this information may contribute to unaddressed pharmacotherapy issues upon admission. The above concerns provided the impetus to have a pharmacist prospectively evaluate planned dofetilide admissions for pharmacotherapy concerns.
Objective
The purpose of this quality improvement initiative was to characterize interventions associated with pharmacist evaluation of scheduled dofetilide admissions prior to hospitalization.
Methods
The ZVAMC is a tertiary care and academic medical center located in Milwaukee, Wisconsin that serves the Veteran population of Southeastern Wisconsin. The medical center has 113 acute care operating beds, 3 including a 15-bed cardiology unit managed by a dedicated inpatient cardiology service. In addition, there is an inpatient electrophysiology service that admits approximately 50 patients per year for the purpose of dofetilide initiation.
A Plan-Do-Study-Act 4 quality improvement framework was used to characterize interventions identified through pharmacist evaluation of planned dofetilide admissions prior to hospitalization. Evaluations were conducted from September 2021 to May 2022 and were led by an internal medicine pharmacy resident as part of a year-long residency research project. During this time period, both the pharmacy resident and inpatient cardiology pharmacist were alerted to all scheduled dofetilide initiations via the electronic health record (EHR) prior to admission. Upon receiving notification of a scheduled admission for dofetilide initiation, the EHR was reviewed for assessment of appropriate AAD selection as per current atrial fibrillation guidelines. 5 This assessment included review of past and current antiarrhythmic therapy for atrial fibrillation and/or atrial flutter, transthoracic echocardiogram (TTE) for assessment of left ventricular ejection fraction and interventricular septal wall thickness, ECG for assessment of cardiac rhythm and evaluation of baseline QTc interval, medication list for assessment of current oral anticoagulant therapy and DDIs with dofetilide (including current use of QTc-prolonging drugs), vitals for assessment of heart rate, laboratory assessment of renal function (serum creatinine and calculated creatinine clearance), serum potassium and magnesium levels, and international normalized ratio (INR) for patients on warfarin. Lexicomp®, 6 a tertiary drug information resource, was utilized to assess and categorize DDIs.
After the EHR was reviewed, the dofetilide starting dose selected by the electrophysiology provider (if documented) was evaluated for appropriateness based on calculated creatinine clearance, concomitant DDIs, history of QTc interval prolongation, and history of bradycardia. The pharmacy resident then contacted the patient or caregiver via telephone approximately 1 week prior to admission to obtain a medication history and to assess adherence to oral anticoagulation. Next, a note titled “Pharmacy Antiarrhythmic Assessment Note” was entered into the EHR for documentation of medication history, pertinent labs and vitals, pertinent ECG and TTE findings, and interventions and recommendations by the pharmacy resident. Any pertinent findings that needed to be addressed prior to admission (ie, missed oral anticoagulant doses) were discussed with the inpatient cardiology pharmacist and electrophysiology provider so that a plan could be formulated to address the concern (ie, reschedule admission after 3 consecutive weeks of therapeutic anticoagulation or admit as scheduled and proceed with a transesophageal echocardiogram [TEE] to rule out left atrial appendage thrombus prior to initiating dofetilide). Lastly, the EHR was re-reviewed after patient discharge to assess for acceptance of pharmacist recommendations. Figure 2 demonstrates the process for evaluation of each scheduled dofetilide admission.
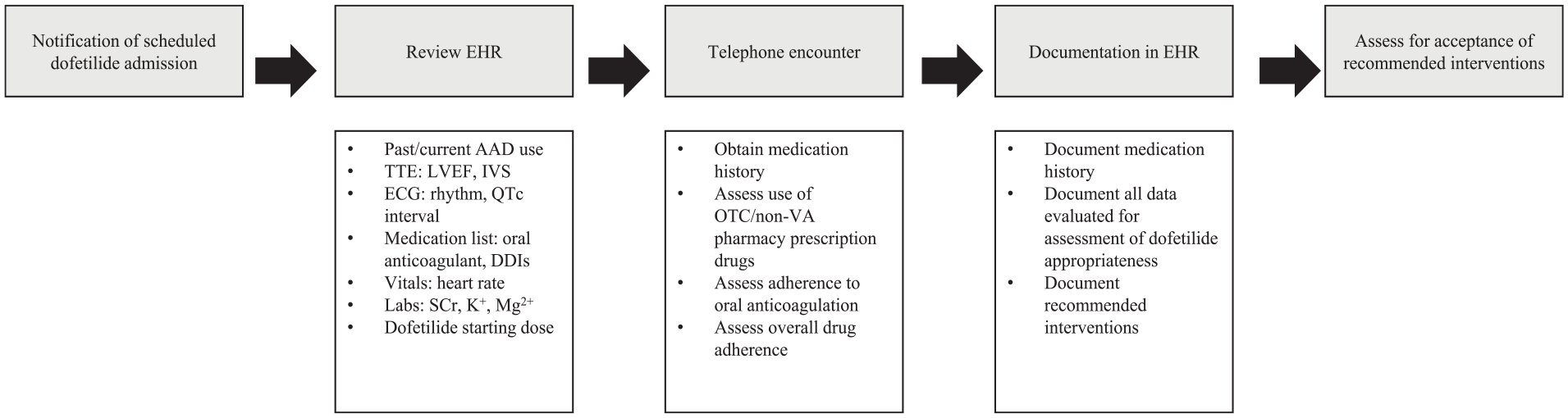
MethodologyNote. AAD= antiarrhythmic drugs; DDIs= drug-drug interactions; ECG= electrocardiogram; EHR= electronic health record; IVS= interventricular septum; K+= potassium; Mg2+= magnesium; OTC= over-the-counter; TEE= transesophageal echocardiogram; TTE= transthoracic echocardiogram; VA= Veterans Affairs.
The primary outcome measure was the frequency and types of identified and accepted interventions. Interventions were classified into 7 categories including recommendation for: (1) against the use of dofetilide; (2) dofetilide starting dose adjustment; (3) appropriate washout of previous AAD; (4) TEE prior to dofetilide initiation; (5) discontinuation or dose adjustment of interacting drug; (6) electrolyte supplementation upon discharge; (7) other intervention. Descriptive statistics were performed to characterize identified interventions.
This study was considered exempt by the ZVAMC Institutional Review Board as it was determined to be an internal quality improvement operations activity.
Results
Twenty-two patients were prospectively evaluated by the pharmacy resident over the course of the study period. On average, patients or caregivers were contacted 3.6 days prior to admission. A total of 14 interventions were identified (Table 1), 13 of which were accepted by an electrophysiology provider. The most common intervention was recommendation for a TEE prior to dofetilide initiation because of inadequate oral anticoagulation (n = 6; 43%). Other accepted interventions were as follows: recommendation for discontinuation or dose adjustment of an interacting drug (n = 3, 21%), recommendation for dofetilide starting dose adjustment (n = 2, 14%), recommendation for electrolyte supplementation upon discharge (n = 2; 14%), and other intervention (n = 1; 7%).
Identified Interventions.
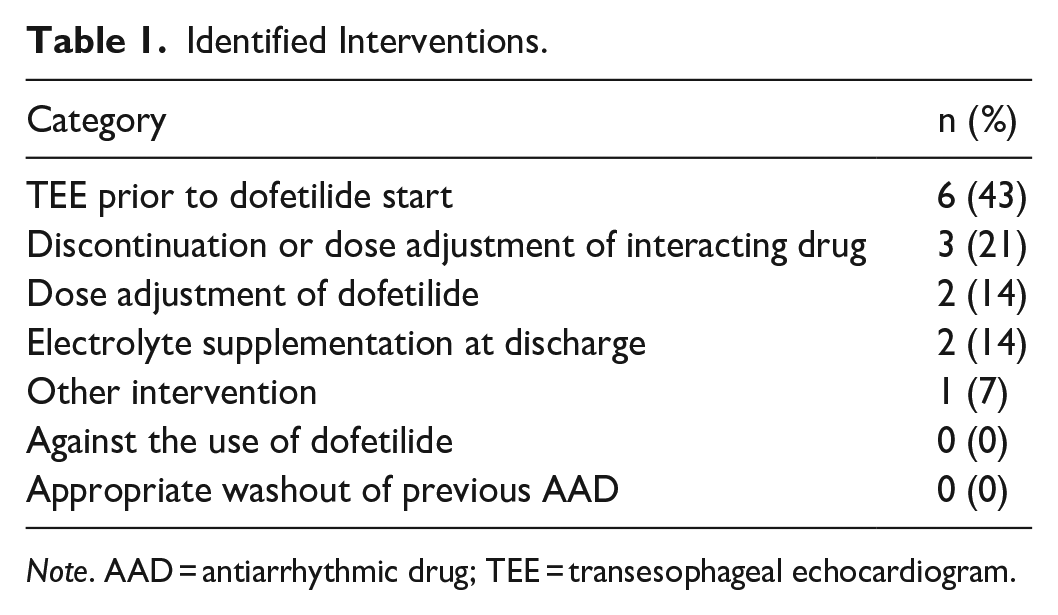
Note. AAD = antiarrhythmic drug; TEE = transesophageal echocardiogram.
Patients that warranted recommendation for a TEE prior to dofetilide initiation were those who were currently in atrial fibrillation or atrial flutter and had missed at least 1 dose of a direct-acting oral anticoagulant (DOAC) in the 3-week period leading up to admission or patients on warfarin that did not have 3 weekly therapeutic INRs prior to dofetilide initiation as recommended by current atrial fibrillation guidelines. 5 Of the 6 recommendations included in this category, the majority were for patients that had missed at least 1 dose of a DOAC (n = 4, 67%). The other 2 patients in this category were on warfarin and did not have the requisite number of INR assessments in the 3-week period leading up to admission. Recommendations for discontinuation or dose reduction of an interacting drug were for discontinuation of hydrochlorothiazide (n = 2, 67%), a category X interaction per Lexicomp®, 6 and dose reduction of diltiazem (n = 1, 33%), a category C interaction per Lexicomp®. 6 A dose reduction of diltiazem was recommended to increase resting heart rate and consequently, decrease QTc interval in a patient with a history of bradycardia. Table 2 lists the number of identified DDIs according to the Lexicomp® risk rating category.
Summary of Identified DDIs.
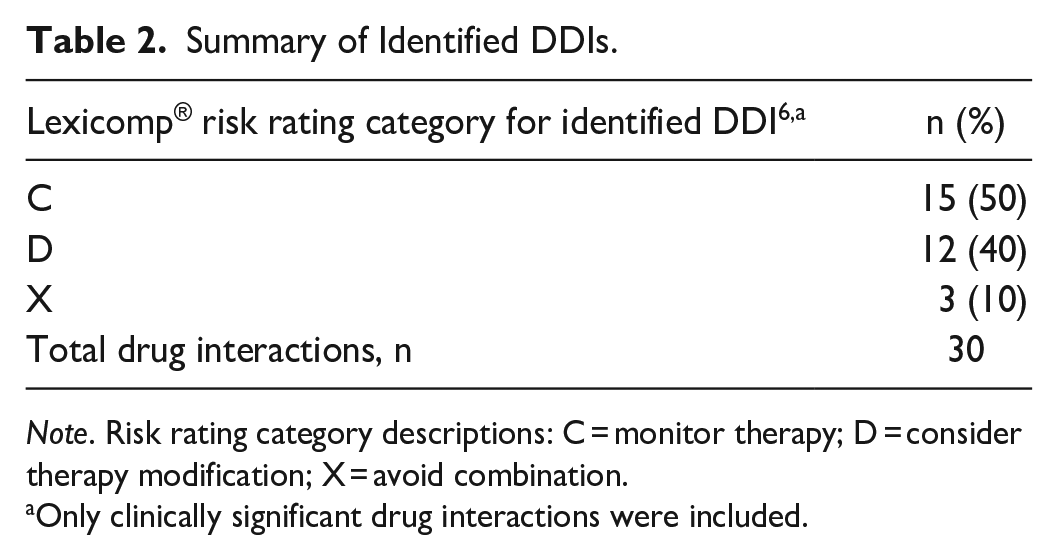
Note. Risk rating category descriptions: C = monitor therapy; D = consider therapy modification; X = avoid combination.
Only clinically significant drug interactions were included.
Of the recommendations made for a dofetilide starting dose adjustment, one was for a higher dofetilide dose based on renal function and one was for a lower dofetilide dose based on a history of QTc prolongation with a previous dofetilide trial. The recommendation for a lower dofetilide starting dose was not accepted. However, the patient did ultimately require a dose reduction to the pharmacist recommended starting dose because of QTc prolongation during hospitalization for dofetilide initiation. Recommendations for electrolyte supplementation upon discharge were all for magnesium supplementation because of a history of magnesium levels below 2 mg/dL (n = 2; 100%). Lastly, a recommendation was made for remeasurement of interventricular septal wall thickness because of documentation of an interventricular septum that was greater than 1.5 cm on the most recent TTE (n = 1; 100%). Remeasurement of the interventricular septal wall thickness by an electrophysiologist determined that the original measurement was inaccurate and admission for dofetilide initiation proceeded as scheduled.
Discussion
The study results demonstrate that despite the small sample size, prospective evaluation by a pharmacist resulted in a relatively high frequency of identified interventions (14 interventions out of 22 patients) during the short 9-month study period and high intervention acceptance rate (93%), as well as diversity in the types of interventions made (5 distinct categories of interventions were identified). Prospective evaluation by a pharmacist allowed for identification of potential safety concerns related to dofetilide use prior to admission for dofetilide initiation.
The most notable and frequent intervention was identification of inadequate oral anticoagulation and consequently, contacting an electrophysiology provider to discuss proceeding with a TEE prior to dofetilide initiation or rescheduling dofetilide initiation after 3 weeks of uninterrupted DOAC therapy or after obtaining 3 weekly therapeutic INRs for patients on warfarin. Before prospective evaluation by a pharmacist, inadequate oral anticoagulation was occasionally identified by the inpatient cardiology pharmacist upon admission in patients presenting for dofetilide initiation. For patients presenting in atrial fibrillation or atrial flutter, this often led to dofetilide initiation cancelation and rescheduling or therapy initiation delay and possibly increased length of hospital stay as a result (ie, additional time needed to contact an electrophysiology provider to coordinate a TEE ± electrical cardioversion prior to starting dofetilide). Prospective evaluation by a pharmacist knowledgeable in the risks associated with antiarrhythmic initiation enabled the inpatient cardiology pharmacist to take a proactive approach in identifying inadequate oral anticoagulation prior to admission in order to prevent dofetilide initiation cancellation or delay upon admission.
It is important to note that assessment of anticoagulation status for all planned dofetilide initiations is completed by an electrophysiology provider prior to scheduling hospital admission. This includes assessment of adherence to DOAC therapy or coordination with outpatient anticoagulation providers to obtain the requisite number of weekly INRs for patients on warfarin. Despite electrophysiology provider assessment, 27% of patients scheduled for dofetilide initiation during the study period were identified by the pharmacist to have missed at least 1 dose of a DOAC in the 3-week period leading up to admission or did not have the requisite number of weekly INRs leading up to admission if on warfarin. Identification of inadequate oral anticoagulation by the pharmacist prior to admission accounted for almost one-half of the study interventions. This may be because of specialized pharmacist training in medication history taking, assessing medication adherence, and educating patients on the increased risk of stroke associated with oral anticoagulant non-adherence in the setting of potential chemical cardioversion with dofetilide.
Lastly, a pharmacist-obtained mediation history prior to admission allowed for accurate assessment of potential DDIs with dofetilide therapy and afforded time for the pharmacist to discuss therapy recommendations with the electrophysiology provider and patient prior to admission (ie, discontinuation of hydrochlorothiazide with appropriate wash-out period prior to admission). Prospective assessment of DDIs with dofetilide related to concomitant QTc-prolonging drugs also enables the pharmacist to have a discussion with the electrophysiology provider regarding an appropriate QTc prolongation mitigation strategy (ie, consideration for dose reduction or discontinuation of concurrent QTc-prolonging drugs prior to admission). This is important as previous literature has reported that dofetilide patients taking concomitant QTc-prolonging drugs were 1.9 times more likely to discontinue dofetilide compared to those who were not taking any other QTc-prolonging drugs. 7
Limitations to this study included a relatively short study duration and consequently, a small sample size. The sample size was also impacted by the COVID-19 pandemic, as the number of scheduled dofetilide admissions was reduced during the study period to accommodate the need for additional hospital bed availability during the Coronavirus Omicron surge. This likely limited the number of potential study interventions, including the possibility of encountering significant DDIs related to concomitant QTc-prolonging drugs and potential associated interventions to reduce QTc prolongation risk with dofetilide. Furthermore, the original plan was to include prospective assessment of all scheduled admissions for sotalol initiation as well. However, sotalol initiations were transitioned to the outpatient setting during the study period in response to the Omicron surge. This also may have limited the number of study interventions, as similar pharmacotherapy concerns related to anticoagulation status and concomitant QTc-prolonging DDIs exist with sotalol as well.
Conclusion
Pharmacist evaluation of scheduled dofetilide admissions prior to hospitalization can serve to identify and resolve pharmacotherapy concerns related to dofetilide use.
Footnotes
Authors’ Note
Inez E. Pabian is currently affiliated with the North Texas VA Health Care System in Dallas, TX, USA. This work was presented at the 2022 Wisconsin Pharmacy Residency Conference in Madison, WI, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.