
Abstract
Introduction
Pharmacists are key players in the healthcare field. Traditionally, they have been recognized primarily for their role in dispensing medicines, manufacturing, compounding, and supplying pharmaceuticals. However, with the modern shift toward improving the quality of healthcare services and addressing the emerging trend of patient-centric care, the role of pharmacists has significantly expanded.1,2 This transformation is particularly evident in the emergence and evolution of the role of hospital pharmacists. Hospital pharmacists hold diverse roles that transcend mere drug provision. 3 They dispense medications, conduct quality checks, manage drug safety and budgets, strategize medication storage, and contribute to drug review committees and pharmacoeconomic units. Furthermore, some engage in patient-centric care within pharmacy-managed clinics in specialized and university hospitals. Therefore, the role of hospital pharmacists extends to an even more patient-focused approach, providing direct and personalized patient care, in line with global trends toward patient-centered healthcare services.
Psychological distress represents a prevalent concern in the community, 4 particularly among healthcare workers who are continually exposed to job stress, tense situations, and constant encounters with illness and death. This emotional distress is typically characterized by symptoms of depression, anxiety, and stress. 5 Employees’ physical and mental health is related to a wide range of work conditions, which can be classified as job demands and job resources, as conceptualized within the Demands-Resources (JD-R) theory.6,7 These aspects have been found to be associated with a variety of outcomes, such as turnover intention, job satisfaction, and service quality, and are suggested to be influenced through the mediating pathways of burnout and engagement. 6 In the context of modern pharmaceutical care, the focus is on safe and effective treatment and improving patients’ quality of life, 8 introducing new psychological challenges for healthcare professionals, including pharmacists. Several studies and reports affirm that working in the pharmaceutical sector is considered stressful and demanding, requiring high skill levels and patience. 9 Previous research suggests that working in a hospital environment, with daily contact with numerous patients and other healthcare staff, 10 as well as disruptions in work, heavy workloads, and inadequate staffing, enhances psychological burdens and job stress among hospital pharmacists. 11 Consequently, hospital pharmacists are at risk of mental health disorders, potentially impacting their job satisfaction and ability to meet job demands.
Job satisfaction, a subjective evaluation of a worker’s own perception of their occupation, pertains to the extent to which they enjoy their role. It could relate to the job as a whole or specific facets thereof, such as autonomy, stress, usefulness, creativity within the role, wages, sector, size of organization, and job stability. 12 Job satisfaction fosters and encourages better performance among employees, thereby enhancing labor productivity.13,14 Studies in the United States have indicated that over 60% of pharmacists are satisfied with their job. Nevertheless, concurrently, more than 70% of pharmacists report feeling overworked and stressed in their role. 15 This aligns with other research, such as the study by Scott and Judge 16 and Visser et al, 17 which revealed a direct correlation between job satisfaction and mental health. More specifically, hospital pharmacists typically experience lower job satisfaction compared to their counterparts in other areas, as suggested by a study conducted in Saudi Arabia. 14 Hence, the mental health of hospital pharmacists needs to be prioritized and addressed promptly and effectively. Job satisfaction plays a critical role in employee behavior at the workplace. 18 Only in a comfortable working environment can pharmacists operate efficiently, optimizing the communication process with other healthcare professionals and patients. 19 This ensures the highest level of safety and quality in healthcare services.
Job satisfaction has been discovered to negatively correlate with mental health issues such as stress, anxiety, and depression among both non-medical and medical staff, 20 including doctors and nurses.21 -26 This correlation has also been identified in pharmacists, according to previous studies. For instance, Stavrou et al 27 found that job satisfaction and perceived stress levels among pharmacists in both private pharmacies and the public sector in Cyprus were inversely related. Likewise, a study by Teong et al 28 revealed a significant negative correlation between overall job satisfaction score and stress score among community pharmacists in Malaysia. Further, Aldaiji et al 14 reported a significant negative relationship between occupational stress and job satisfaction among pharmacists across different sectors in Saudi Arabia, including academic institutions, hospitals, the drug industry, and conferences. However, it appears that no studies have simultaneously addressed all 3 issues—stress, anxiety, and depression—among pharmacists. Furthermore, there seems to be a dearth of research focusing on hospital pharmacists in prior global and Vietnamese studies, to the best of our knowledge. Therefore, this study aims to determine the correlation between stress, anxiety, depression and job satisfaction among hospital pharmacists in Vietnam.
Methods
Study Design
The study was conducted using a cross-sectional survey from December 2022 to March 2023 in Can Tho City, Vietnam. Located in the Mekong Delta region of South Vietnam, Can Tho City spans over 55 km along the west bank of the Hau River. With an area of 1439 km2, it is home to a population of 1.3 million people. 29 Can Tho City has 13 public hospitals at the city level and 3 district-level hospitals under the Can Tho Department of Health. Additionally, there is 1 hospital under the Logistics Department—Military Region 9, 1 hospital under the Ministry of Health, and 1 hospital under the university. The study population consisted of pharmacy staff in public hospitals in Can Tho City. Among these hospitals, 11 were selected using a convenience sampling method for inclusion in this study. The selection of the 11 hospitals was based on specific criteria, such as the approval from hospital authorities to conduct the survey within their premises and the nearest geographical accessibility from the center of Can Tho City. Subsequently, all staff members from these healthcare facilities were recruited to participate in the study. Pharmacy staff who were absent during the survey period or those who declined to participate were excluded from the study. In the context of this study, the term “hospital pharmacist” was used to refer to pharmacy staff working in hospitals with different levels of pharmacy education, including postgraduate, undergraduate, and below undergraduate. This covers multiple job positions in hospitals, including drug storage and distribution, clinical pharmacy, outpatient drug distribution, pharmacy official work, pharmacy statistics, and administration.
To collect data, the survey team first contacted the hospital leaders of the selected hospitals to request their approval for the study implementation. Then, the pharmacy department leaders and their staff were provided with printed questionnaires immediately after the end of the pharmacy department meeting. It took approximately 5 to 10 minutes to complete the questionnaire, and the response forms were collected immediately after respondents finished. Out of the total of 305 distributed questionnaires, 303 completed questionnaires were collected (2 questionnaires were left incomplete as 2 participants declined to participate), resulting in a response rate of 99.3%.
Survey Questionnaire
This study utilized a printed questionnaire consisting of 3 sections. The first section collected data on participant characteristics, including sex, age, religion, marital status, number of children, place of residence, educational level, duration of employment at the hospital, daily working hours, position at the hospital, monthly on-duty times, job responsibilities, average monthly income, presence of additional duties beyond primary responsibilities, and housing status.
The second section of the questionnaire assessed stress, anxiety, and depression using the depression anxiety stress scale (DASS)-21, which has been validated in Vietnam by Tran et al. 30 This scale comprises 21 items divided into 3 subscales: stress, anxiety, and depression. Each subscale comprises 7 items. The stress subscale includes items 1, 6, 8, 11, 12, 14, and 18; the anxiety subscale includes items 2, 4, 7, 9, 15, 19, and 20; and the depression subscale includes items 3, 5, 10, 13, 16, 17, and 21. Each item is scored from 0 to 3, reflecting the degree and frequency of symptom occurrence: 0—not at all, 1—somewhat or occasionally, 2—moderately or most of the time, and 3—almost always or always. The total score for each disorder was calculated by summing the scores of the 7 items and doubling the sum. Thus, scores range from 0 to 42, with larger scores indicating greater severity. The cutoff scores to determine the presence of stress, anxiety, and depression are 14, 7, and 9, respectively. 31 The Cronbach’s alpha coefficients for stress, anxiety, and depression in this study were .89, .88, and .90, respectively, indicating satisfactory reliability of the subscales.
In the third section, job satisfaction was assessed using a questionnaire consisting of 44 items, which were divided into 5 subscales: (i) satisfaction with the work environment (9 items), (ii) satisfaction with direct leadership and colleagues (9 items), (iii) satisfaction with internal regulations, salary, and benefits (12 items), (iv) satisfaction with job, learning opportunities, and career advancement (7 items), and (v) satisfaction with the hospital overall (7 items). This section was adapted from the survey tool of the Vietnamese Ministry of Health under Decision 3869/QD-BYT. 32 Each question was evaluated on a Likert scale ranging from 1 to 5 (1: Very dissatisfied; 2: Dissatisfied; 3: Neutral; 4: Satisfied; 5: Very satisfied). The satisfaction score of each subscale was calculated as the sum of all items on that subscale. Therefore, the satisfaction score of each subscale would vary depending on the number of items in that subscale. For example, the satisfaction score for “the work environment” comprising 9 items would range from 9 to 45. The overall satisfaction score was calculated as the sum of all items on the scale, ranging from 44 to 220. Participants with scores above 75% 33 of the total score (equivalent to 165 points) were classified as satisfied, while the remaining participants were classified as dissatisfied. In our study, the responses had a Cronbach’s alpha coefficient of .98 for the satisfaction scale, indicating very high reliability.
Ethical Considerations
Our study was approved by the Institutional Review Board of the Can Tho University of Medicine and Pharmacy (No. 22.009.HV/PCT-HDDD, July 25, 2022). Written consent letters were obtained from all participants prior to their involvement in the study.
Data Analysis
The collected data were analyzed using IBM SPSS Statistics 22 software (IBM, Chicago, IL, USA). Descriptive statistics such as frequencies and percentages were used to present categorical variables. Univariate analysis employed chi-squared tests (or Fisher’s exact test where appropriate) and binary logistic regression to determine (i) the demographic and job-related characteristics associated with stress, anxiety, and depression, as well as (ii) the relationships between stress, anxiety, depression, and job satisfaction. Variables with an inclusive threshold of P < .25 in the univariate analysis were included in the multiple logistic regression model. 34 A level of P < .05 was chosen to indicate statistical significance.
Results
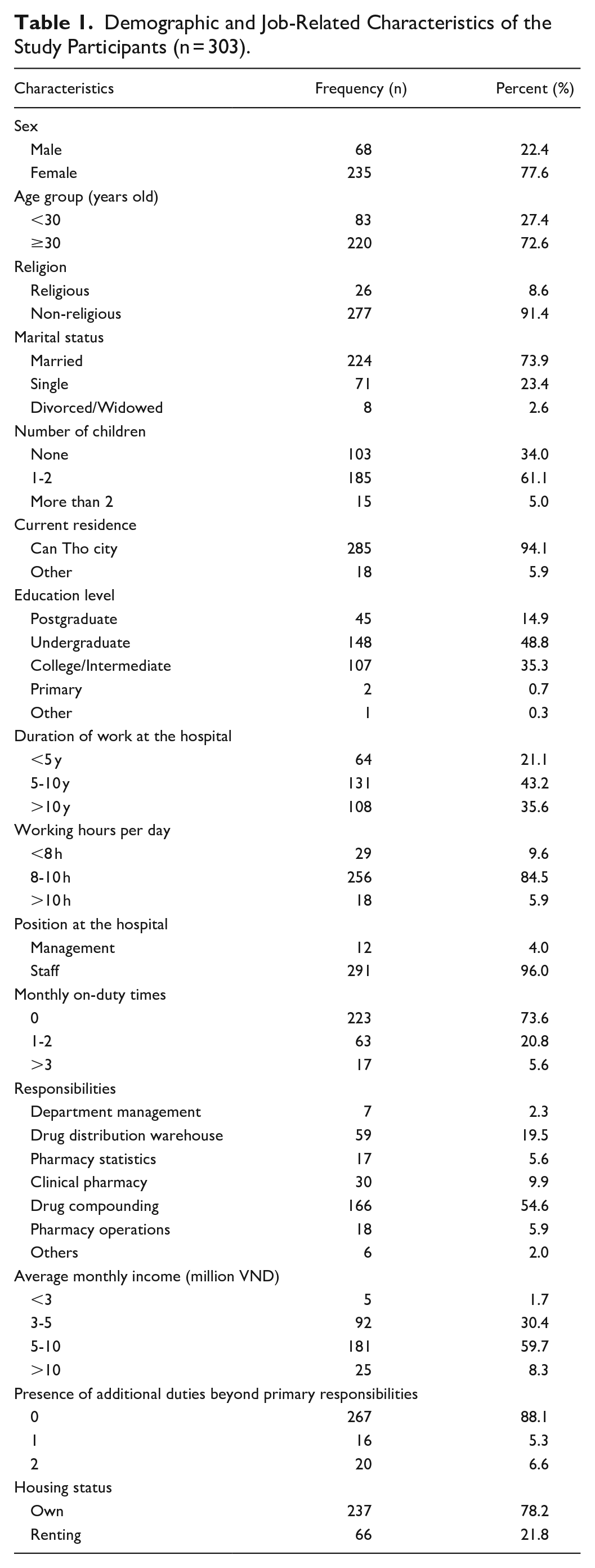
In this study involving a total of 303 participants, female respondents accounted for 77.6%, and individuals aged 30 and above constituted 72.6% (Table 1). The majority, 91.4%, did not affiliate with any religion. Approximately three-quarters, 73.9%, were married. Participants with 1 to 2 children made up 61.1% of the sample. The vast majority, 94.1%, resided in Can Tho. Over three-quarters, 78.2%, owned a private house. University graduates made up 48.8% of the participants. The 43.2% percentage had 5 to 10 years of experience working in a hospital. The majority of participants, 84.5%, worked 8 to 10 hours per day. Approximately 73.6% of participants did not work shifts in a hospital. More than half, 54.6%, were responsible for medication preparation tasks. Participants with monthly incomes ranging from 5 to 10 million VND (approximately 210-420 USD) constituted 59.7% of the sample.
Demographic and Job-Related Characteristics of the Study Participants (n = 303).
The prevalence of stress, anxiety, and depression was found to be 15.5% (n = 47), 27.1% (n = 82), and 20.5% (n = 62), respectively. The majority of hospital staff reported being satisfied with their jobs (n = 221, 72.9%), as shown in Table 2.
Prevalence of Stress, Anxiety, Depression, and Job Satisfaction (n = 303).
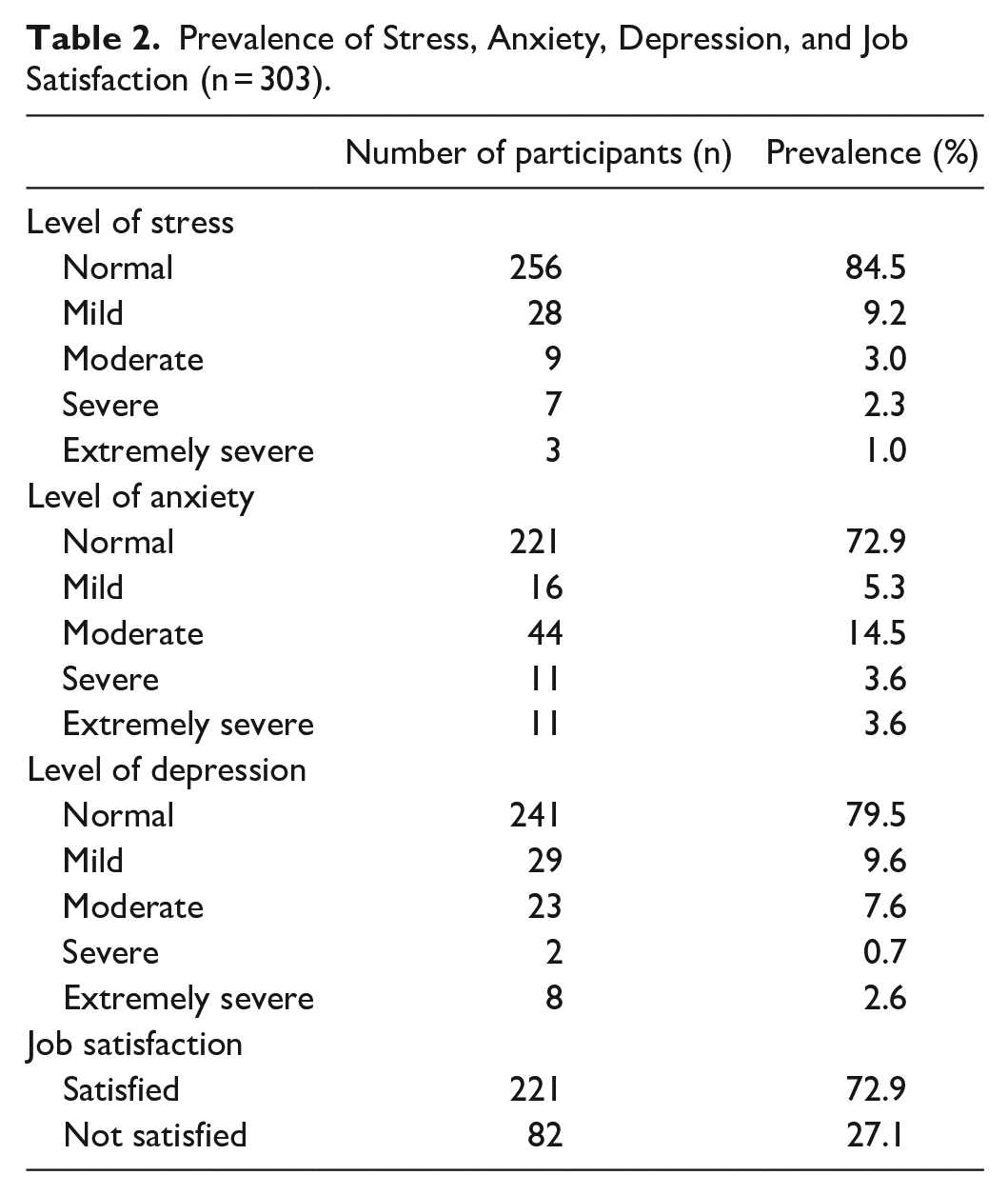
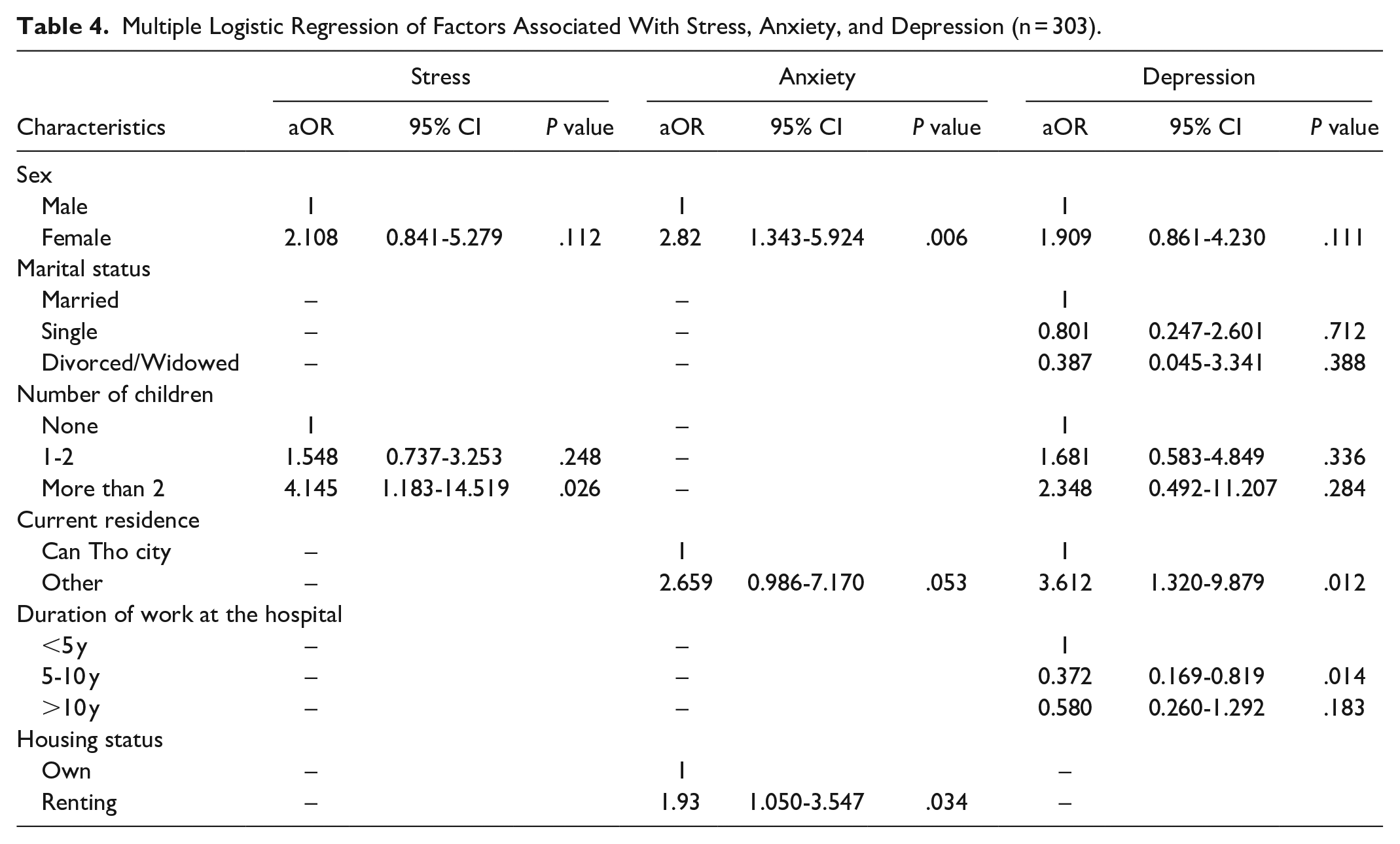
Table 3 presents a bivariate analysis between the participants’ characteristics and the prevalence of stress, anxiety, and depression. When performing the comparative statistical analysis between the group of hospital pharmacists with symptoms of stress, anxiety and depression with the group that did not present these symptoms, it was determined that sex (P = .009) was found to have a statistically significant association with anxiety, and place of residence (P = .016) was related to depression. In the multiple logistic regression analysis (Table 4), sex was found to be significantly associated with anxiety (P = .006). Female participants were 2.82 times more likely to encounter anxiety (95% CI = 1.34-5.92) compared to male participants. Place of residence (P = .012) and the duration of employment at the hospital (P = .014) had significant relations with depression. Those living outside Can Tho City were at a 3.61 times higher risk of depression (95% CI = 1.32-9.88) than those residing in Can Tho City. The number of children significantly correlated with the stress levels of individuals. Those with more than 2 children were nearly 4 times as likely to experience higher stress (95% CI = 1.183-14.519) compared to those without children. Individuals who had been working at the hospital for 5 to 10 years had a lower risk of depression (95% CI = 0.17-0.82) compared to those who had worked for less than 5 years. Housing situation was found to correlate with anxiety (P = .034). Those who rented were 1.93 times more likely to experience anxiety (95% CI = 1.05-3.55) compared to homeowners. The multiple logistic regression models for stress, anxiety, and depression each demonstrated a satisfactory fit as evidenced by the Hosmer and Lemeshow test. For the stress model, the test yielded χ² = 0.354, df = 3, P = .950; for the anxiety model, the test resulted in χ² = 0.071, df = 2, P = .965; and for the depression model, the test indicated χ² = 4.233, df = 6, P = .645.
Bivariate Analysis of Factors Associated With Stress, Anxiety, and Depression (n = 303).
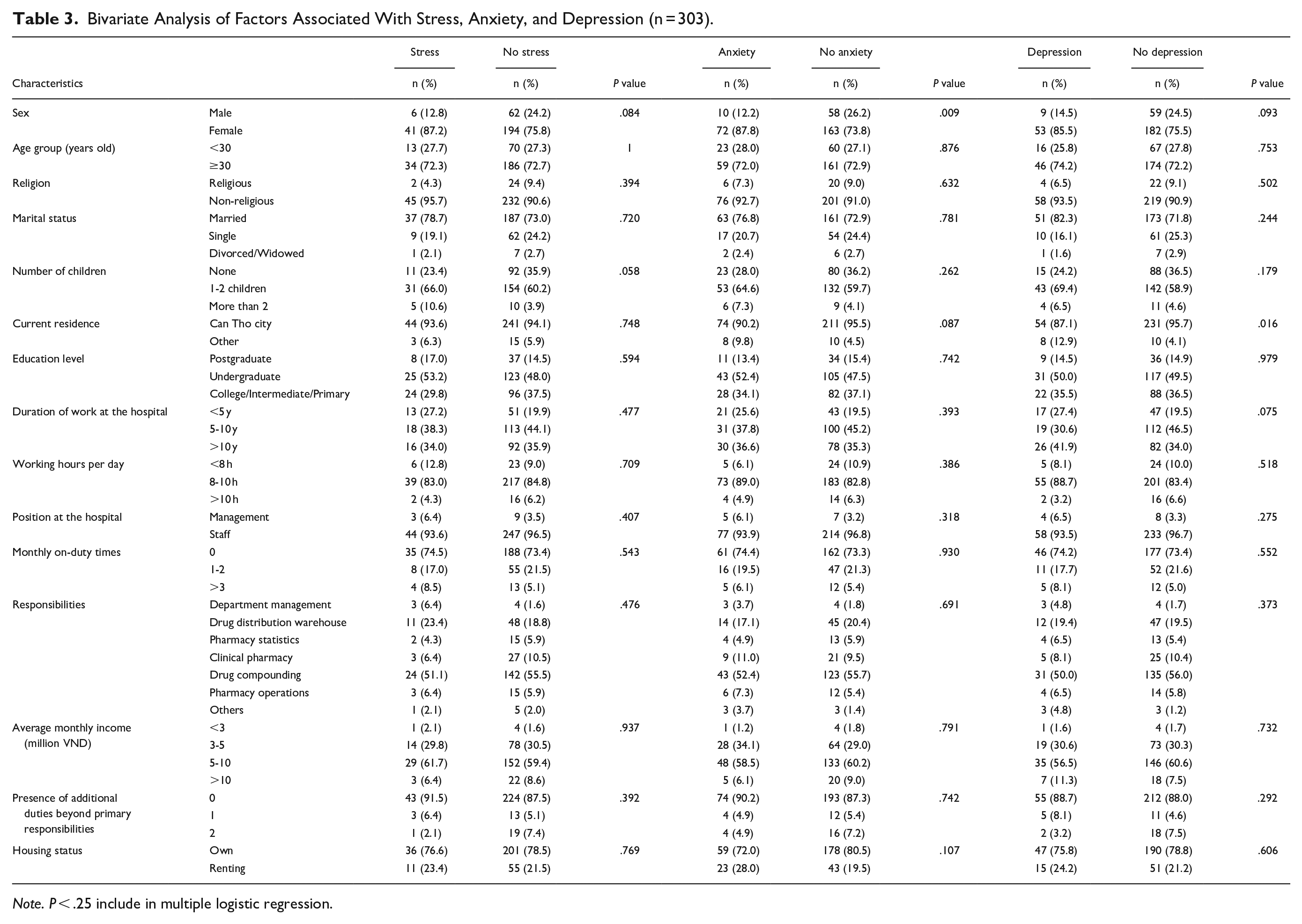
Note. P < .25 include in multiple logistic regression.
Multiple Logistic Regression of Factors Associated With Stress, Anxiety, and Depression (n = 303).
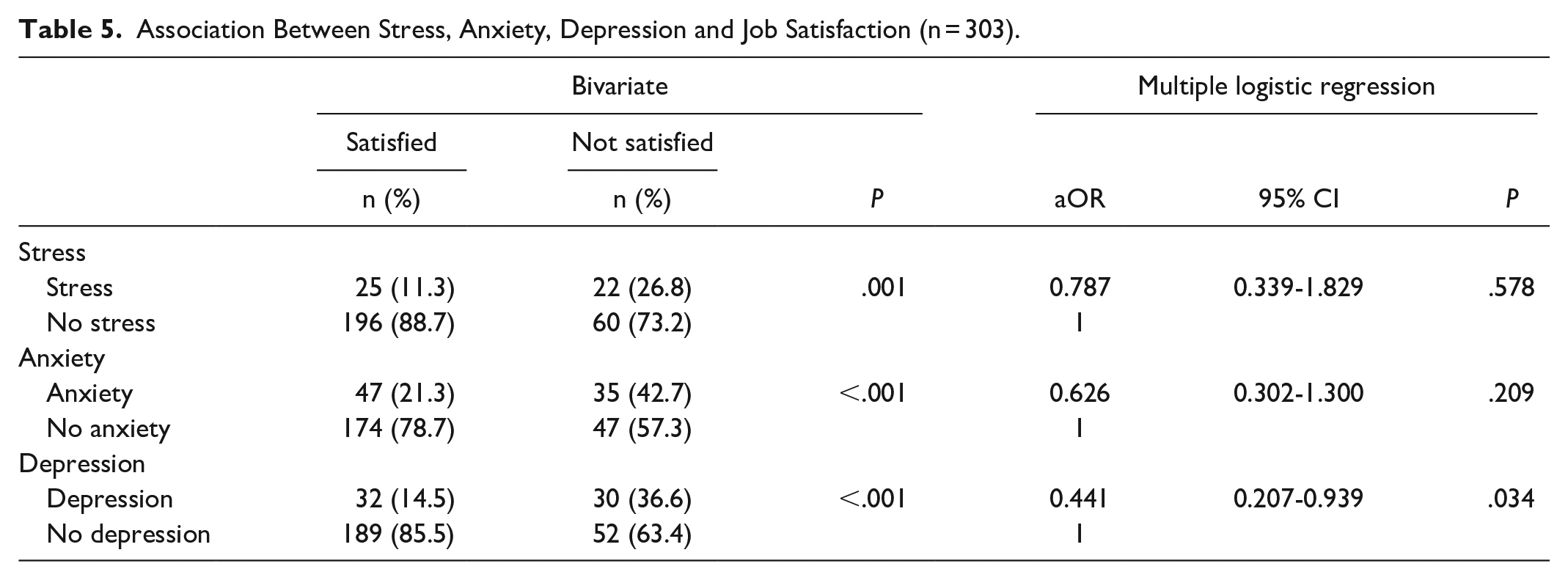
The bivariate analysis revealed a significant association between job satisfaction and stress (P = .001), anxiety (P < .001), and depression (P < .001). However, in the multiple logistic regression analysis, only depression (P = .034) was found to have a significant association with job satisfaction. Increased depression (aOR = 0.441; 95% CI = 0.21-0.94) was linked to greater job dissatisfaction (Table 5). The model provided a good fit as indicated by the Hosmer and Lemeshow test (χ2 = 2.111; df = 3; P = .550).
Association Between Stress, Anxiety, Depression and Job Satisfaction (n = 303).
Discussion
Our investigation DASS-21 scores in hospital pharmacists in Can Tho revealed a prevalence of stress, anxiety, and depression at rates of 15.5%, 27.1%, and 20.5%, respectively. This is lower than previously reported rates among government hospital pharmacists in Malaysia, 35 where the reported prevalence of work stress, anxiety, and depression were 55.8%, 50.6%, and 48.7% (not assessed with the DASS-21). Our findings also showed lower rates than those observed in Qatar and China. 36 Specifically, community pharmacists in Qatar, 37 evaluated with the DASS-21, reported stress, depression, and anxiety at rates of 25.4%, 44.8%, and 53.2% respectively. Moreover, amid the COVID-19 pandemic in China, 36 41.9% and 29.4% of hospital pharmacists reported mild to severe levels of anxiety and depression symptoms, respectively, as assessed using the General Anxiety Disorder-7 and the Patient Health Questionnaire-9. The lower rates found in the present study could be attributed to geographical, cultural, and occupational differences among the countries, as well as the impacts of employing different assessment scales and conducting investigations at different times.
Job satisfaction is widely recognized as a critical factor affecting employee motivation and productivity. Satisfied employees tend to be more committed and productive, thus better equipped to provide services that meet or exceed expectations. In the present study, the majority of hospital staff (72.9%) reported job satisfaction. This aligns with a study conducted in Lebanon, 38 where most hospital pharmacists (72.2%) were more satisfied with their work environment (P = .03). Our results indicate a higher level of job satisfaction compared to those of studies in Ethiopia, 39 where only about 32.7% of pharmacy professionals in public hospitals reported job satisfaction, and in Malaysia, 40 where approximately 52% of pharmacists in public hospitals and healthcare clinics reported being “satisfied.” The variation in these findings could be influenced by differing work conditions and the measures of satisfaction used in each study. From the perspective of dissatisfaction, over a quarter of the pharmacists in the present study reported job dissatisfaction. This provides evidence supporting the need for hospital management to implement and improve measures to enhance job satisfaction among hospital pharmacists. Pharmacist job dissatisfaction has been demonstrated to correlate with medication mismanagement, neglect in detecting adverse drug reactions, and inferior patient interactions. Thus, addressing these issues is crucial to maintaining service quality and patient safety. 38
Our study found that individuals with more than 2 children are nearly 4 times as likely to experience higher levels of stress compared to their childless counterparts. This aligns with findings from the United States, 41 where first year postgraduate pharmacy residents with children reported higher stress scores than those without children. In the present study, female pharmacists were found to be more likely to experience anxiety compared to their male counterparts, a finding that aligns with those of numerous studies revealing higher anxiety reports among female members of staff.42,43 This could be attributable to societal expectations for women to spend more time and effort communicating with patients and providing patient care services. 43 Additionally, women may grapple with conflicts between work and family life.43,44 Conversely, societal norms may condition men to conceal their anxieties, making them less likely to express and discuss emotional difficulties. 45 Thus, understanding and addressing these gender-specific experiences and pressures can be crucial in managing mental health issues among pharmacists.
This study found that individuals who rent their homes were more likely to experience anxiety compared to homeowners. Typically, those with more challenging social circumstances and fewer financial resources are more likely to rent from housing associations or local authorities. 46 Renters generally report poorer physical and mental health outcomes than homeowners. 47 These findings suggest that encouraging and facilitating homeownership might be associated with better mental health and could help mitigate the impact of other socio-economic characteristics on the quality of life among hospital pharmacists.46,48 Therefore, understanding and addressing housing disparities may be an important consideration for improving mental health and overall well-being in this population.
Pharmacists surveyed in our study who lived outside Can Tho City were found to have a higher risk of depression compared to those residing within the city. Several factors might explain this finding. Longer commute times not only reduce the time available for social activities and physical recreation49,50 but also increase exposure to uncomfortable environments such as noise, vibrations, uncomfortable postures, and unwanted contact with others during the journey to work, all of which can directly contribute to poorer health outcomes. Additionally, longer commute times are associated with reduced time for hobbies with family or friends, which can hinder stress relief efforts and negatively impact mental health. 51 Long commute times are also associated with sleep issues.52,53 Lower sleep quality may be a part of the negative impact of long commute times on overall health. 54 To address these issues, institutions could consider implementing flexible work schedules, promoting remote work options, or providing support for housing near the workplace, which could help to reduce commute times and improve the mental well-being of pharmacists.
This study found that respondents who had been working at the hospital for 5 to 10 years were less likely to experience depression compared to those who had worked for fewer than 5 years. This finding is consistent with a study conducted in Saudi Arabia, where healthcare workers with 5 to 10 years and more than 10 years of experience were at a significantly lower risk of developing depression compared to those with less than 5 years of experience. 55 As newcomers to a working environment, healthcare professionals often face various challenges, which might account for higher levels of depression among those with less experience. 55 However, it is worth noting that some studies have found higher depression rates among more experienced healthcare workers,56,57 suggesting a complex relationship between work experience and mental health in this professional context.
Numerous studies have identified a relationship between psychological distress and job satisfaction among pharmacists. For instance, Afulani et al 58 found that high levels of stress were correlated with lower job satisfaction. Similarly, Aldaiji et al 14 reported a significant negative association between occupational stress and job satisfaction. In contrast, the relationship between stress and job satisfaction was not significant in the multiple logistic regression model in the present study. However, our study found that increased depression was linked to greater job dissatisfaction. One possible explanation could be that healthcare workers, including pharmacists, invest a significant amount of their time in work, and dissatisfaction could lead to emotional exhaustion and burnout, culminating in mental health issues. 59 Clearly, further investigations with larger sample sizes are necessary to explore this relationship further. To the best of our knowledge, this is the first study to report associations between depression and job satisfaction among hospital pharmacists in Vietnam.
To improve the mental health and job satisfaction of hospital pharmacists, management can take several steps, as follows. Firstly, monitor and manage employee workload to prevent excessive responsibilities and reduce burnout risk. Offering flexible work schedules or remote options can help employees with family responsibilities achieve a better work-life balance. Secondly, organizing workshops and training sessions on stress management and coping strategies can raise awareness of mental health issues among employees and management. Establishing peer support groups fosters camaraderie and open communication. Thirdly, considering the provision of support or benefits related to housing for employees living far from the workplace to reduce stress from long commutes. Implementing these proposals can create a supportive work environment, enhancing the health and job satisfaction of hospital pharmacists.
Limitations
This study has several limitations. Firstly, it employed a cross-sectional descriptive design, which does not allow the inference of causal relationships. Therefore, it remains uncertain whether depression causes job dissatisfaction, or conversely, job dissatisfaction leads to depression. Additionally, the study may have potential sources of bias due to the survey being administered during the year-end and New Year period. Busy schedules and holiday distractions could lead to selection bias, and participants’ mood during this time might influence their responses to questions relating to stress, anxiety, depression, and job satisfaction. Secondly, although data were collected from 11 public hospitals in Can Tho, the hospitals were selected conveniently rather than randomly. This might introduce selection bias and limit the generalizability of the findings. Thirdly, the use of self-report questionnaires might lead to recall and confirmation biases. Participants may not accurately remember their levels of stress, anxiety, depression, or job satisfaction. They might also be influenced by the desire to provide socially acceptable or positive responses. Some ideas are proposed for future research. Firstly, a longitudinal study following participants over an extended period would allow for the assessment of changes in mental health, job dissatisfaction, and other variables over time. Secondly, implementing random hospital selection would improve the generalizability of the study. Furthermore, expanding the study to include data collection from multiple cities or regions to provide a more diverse and representative sample across Vietnam. Thirdly, combining qualitative and quantitative methods would allow future studies to gain a deeper understanding of participants’ experiences and perceptions. Additionally, incorporating a control group in the study design with which to compare responses and outcomes between participants surveyed during the year-end and New Year period and those surveyed at other times of the year would overcome any bias introduced by conducting the study at a single timepoint. By addressing these proposed ideas in future research, it may be possible to overcome the limitations of the current study and more comprehensively expand the understanding of the associations between mental health, job dissatisfaction, and relevant underlying trends.
Conclusion
Our study revealed a significant prevalence of stress, anxiety, and depression among hospital pharmacists, where depression was significantly associated with lower job satisfaction. Number of children was identified as a predictive factor for higher stress levels, while sex and housing status were associated with increased anxiety. Simultaneously, location and years of work experience were also found to correlate with the risk of developing depression. As hospital pharmacists constitute a crucial force in the healthcare system, administrative bodies should implement preventative strategies and interventions to alleviate these mental health concerns among hospital pharmacists.
Footnotes
Acknowledgements
We acknowledge the contribution and support provided by staff from the Can Tho University of Medicine and Pharmacy. The authors would like to acknowledge the hospital pharmacists in Can Tho, Vietnam who participated in this study.
Author Contributions
Conceptualization: VDT, KNN; Methodology: VDT, KNN, TNNP; Investigation: KNN, TNNP; Resources: VDT, TNNP, MHL, VVD; Writing – original draft: VDT, KNN, TNNP, TNPD, TQT, DTMH, MHL, VVD, RSD; Writing – review & editing: VDT, KNN, TNNP, TNPD, TQT, DTMH, MHL, VVD, RSD.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Medical Ethics Council of Can Tho University of Medicine and Pharmacy, Can Tho, Vietnam (reference: 22.009.HV/PCT-HDDD, 25th July 2022). Participants were informed that taking part in the study was voluntary. Survey responses were anonymized at source.
Data Availability
The data that support the findings of this study are available from the corresponding author TNNP (ie, upon reasonable request).