
Abstract
Introduction
Purple glove syndrome (PGS) is a rare condition characterized by limb edema, discoloration, and pain associated with intravenous and oral phenytoin administration. The incidence following intravenous administration ranges from 1.7% to 5.9%, 1 and there are two cases in the literature following oral administration.2,3 The pathophysiology is poorly understood, but histopathologic studies have demonstrated that it occurs in three stages. 4 In the first 2 to 12 hours after infusion, a blue-purple discoloration appears at the site of cannulation; in the following 12 hours, this spreads distally and is accompanied by edema—with or without blistering. In the final stage, there is typically a resolution of signs within days to weeks, but it can progress to compartment syndrome, ischemia, and necrosis. 5 Some authors have speculated as to the pathophysiology of the condition is related to the administration—either due to poor technique or co-infiltration with other substances (the weak acids that stabilize it such as sodium hydroxide, propylene glycol and ethanol).6,7 Meanwhile, other authors have favored biochemical explanations for its occurrence, such as: its alkalinity stimulating vasoconstriction, thrombosis, and subsequent leakage/edema due to endothelial damage 8 ; or the protein-binding of the drug intravascularly increasing the oncotic pressure. 9 It is important at this point to distinguish PGS from what may happen following intra-arterial phenytoin administration. When phenytoin is administered intra-arterially, the affected distribution appears to follow that associated with the distribution of the vessel secondary to thrombosis—with secondary effects ranging from gangrene to reversible thrombotic events.10,11
Ultimately, the pathophysiology remains unknown, but its risk factors are fast infusion rates, older patients, small gauge cannulas, multiple infusions, and large doses. 6 The possible sequelae can range from mild edema to severe cases resulting in compartment syndrome, debridement, amputation, or even death.12,13 Despite this, there is no established treatment. Mild cases in the literature have been managed with simple elevation and warm/cold compresses 14 ; ulcers have been managed with saline cleaning and dressing changes 8 ; while various other proposals have been made for treatment of severe cases including systemic anti-coagulation, topical nitroglycerin, or local infiltration of one of many substances including hyaluronidase, hydrocortisone, triamcinolone, or heparin. 12 Many studies have also proposed the use of regional nerve blockade with mixed outcomes of skin or sensory deficits. 12 Where hyaluronidase has been used previously, a low fixed rate dose (24 units) has been utilized in infants (14-month old male). 15 There is no consensus on the appropriate dose of hyaluronidase in pediatric patients.
Methods and Results
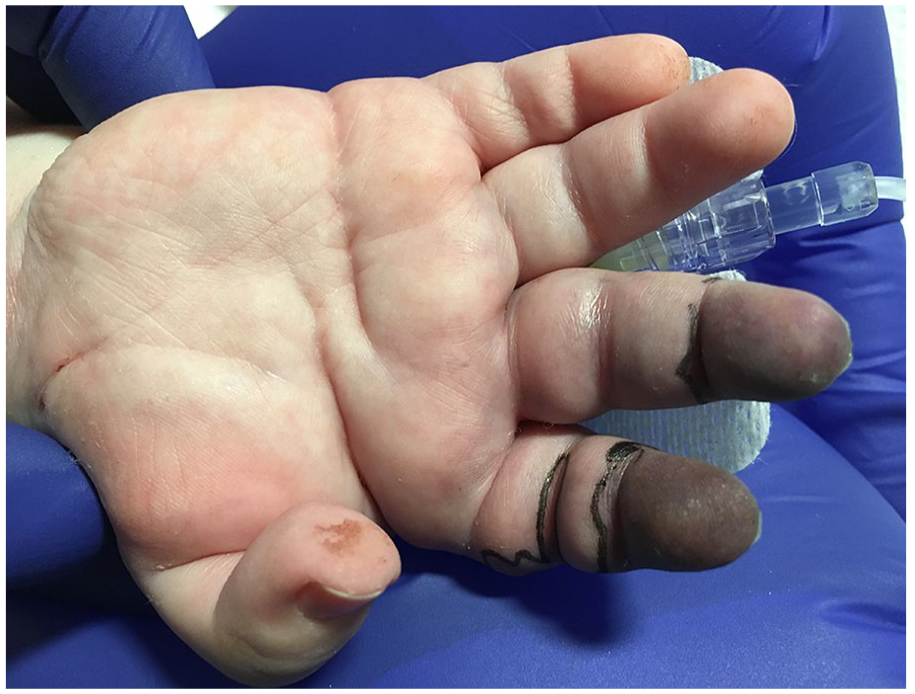
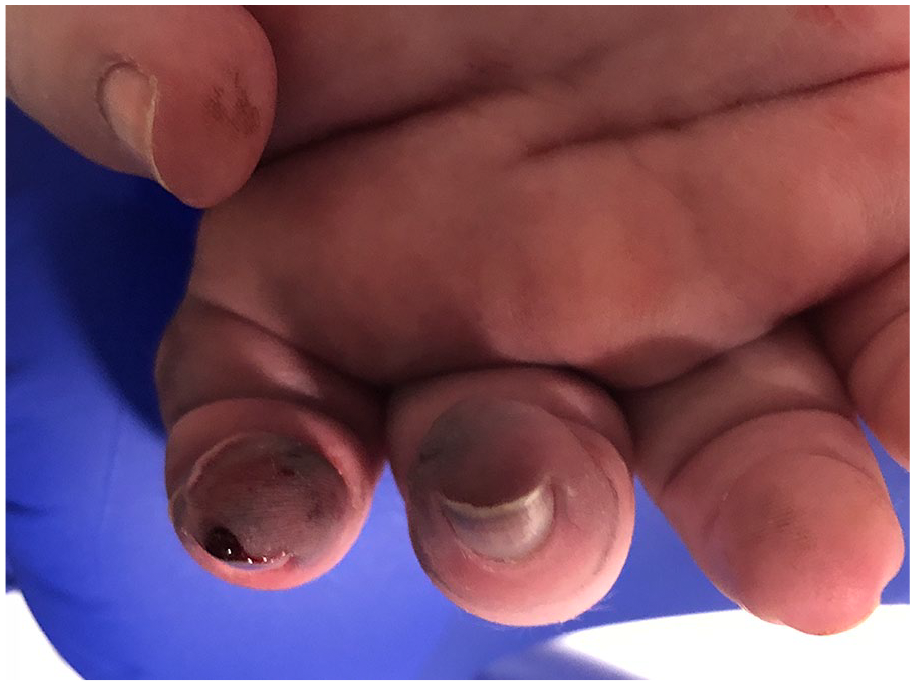
A 2 year-old boy (weighing 20 kg) was admitted with status epilepticus on a background of neonatal encephalopathy and epilepsy. He was already intubated and on the pediatric intensive care unit (PICU) at the time of referral to plastic surgery for purple discoloration to the digits of the right hand (Figures 1 and 2). He was also on opiate-based analgesia, ceftriaxone, acyclovir, sedation, and simple analgesia—as treatment management of his broader condition.

Affected right hand with cannula in situ at referral.

Anterior-posterior view of purple discoloration to the right index finger and right middle finger at referral.
The patient was given his first dose of IV phenytoin for status epilepticus via a cannula on the dorsum of the right hand (loading dose of 20 mg/kg over 20 minutes; dose, drug, and administration as per local policy). Purple discoloration was noted by the nursing staff and eventually a referral to plastic surgery was made 5 hours after the dose was given. The purple lesions involved the tips of the index and middle fingers within 2 minutes before spreading to the radial aspect of the index finger and the middle finger over the next hour. The hand was kept elevated and warm with the use of clinical gloves filled with warm water and blankets. Two percent glycerol trinitrate ointment was applied. At this point, the provisional diagnosis by the intensive care team was discoloration secondary to hypervolemia or thrombosis/micro-emboli; the patient was not on any inotropic or vasopressor medicines.
Five hours following the infusion, the fingertips were non-blanching and firm on palpation and the hand was mildly swollen. Importantly, palpation of the purple area appeared to be painful—with the child retracting to pain despite being intubated. The PICU staff had kept the cannula in situ.
Following a plastic surgery review, this was recognized as an isolated injury affecting a single limb that appeared following administration of IV phenytoin. A provisional diagnosis of PGS was made after consulting product/drug literature. A decision was made to treat with hyaluronidase as it was the reagent that practitioners were most familiar with, and it was easily accessible. It was preferred to local anesthetic and regional block techniques, considering the diagnosis of status epilepticus and a concern that further local anesthetic may be clinically detrimental. Hyaluronidase was prepared with 1500 IU, dissolved into 1 ml of 0.9% normal saline. The dose was selected based on the available formulation (1500 IU vials) and the dosage that the plastic surgery team was experienced with in administration—known to have very low complication rate at this dosage (albeit in adults). 16 The hyaluronidase saline solution was injected with an insulin needle into the subcutaneous tissue of the affected area. A total of 0.5 ml was injected (750 IU). Initially 0.4 ml over 15 minutes. The discoloration was seen to recede within 5 to 10 minutes (Figures 3 and 4). A further 0.1ml was given 2 hours later and improvements seen at 6 hours post-infiltration (Figures 5-7). No further phenytoin was given and IV access was sought elsewhere, with the culprit cannula removed.

Two minutes following treatment administration with receding of the purple discoloration (lateral view).
Two minutes following treatment administration with improvement in the purple discoloration (anterior-posterior view).

Six hours following treatment administration with improvement in the purple discoloration (anterior-posterior view).

Six hours following treatment administration with receding of the purple discoloration (lateral view).

Six hours following treatment administration with receding of the purple discoloration (oblique view).
The child was reviewed daily by the Plastic Surgery team until being discharged. Focal lesions began to demarcate after 36 hours and were confined only to the pulps of both fingers (Figures 8 and 9), with epidermal loss but no deeper trauma. These focal areas were found to bleed when pricked with a needle at the time and 4 days after injury (Figures 10 and 11), with no sign of necrosis. The epidermis peeled within 1 month, with healthy underlying skin found underlying when followed up in clinic.

Thirty six hours following treatment administration with improvement in the purple discoloration (posterior-anterior view).

Thirty six hours following treatment administration with improvement in the purple discoloration and small areas of epidermolysis (lateral view).

Four days following treatment administration with significant improvement in the purple discoloration and pin-prick test demonstrating bleeding (lateral view).
Four days following treatment administration with significant improvement in the purple discoloration and pin-prick test demonstrating bleeding (anterior-posterior view).
For this likely drug reaction, the Naranjo et al.17,18 score is 6. Scores were given for previous conclusive reports (+1), sequence of events (+2), improvement with antagonist (+1), and no alternate cause (+2). There were no point deductions on the scoring on any other questions as the response would be “do not know” (score “0”) to re-administration, placebo, drug detection, dose changes, previous exposure, and objective evidence. This means that this is a technical classified as a “probable” drug reaction, as it is followed a reasonable temporal sequence, a recognized response, and could not be reasonably explained by other means. 17
Discussion
This case study adds to the literature that supports the use of hyaluronidase in the treatment of PGS. In this case, it was used successfully within 6 hours in the early phase of the disease before proximal progression had occurred. This is the first publication to advocate for titrating the dose of hyaluronidase to effect in pediatric patients—with a safe outcome achieved with a dose of 750 IU. The patient was re-dosed as a partial response was demonstrated after the first dose, prompting a smaller second dose to be infiltrated. The intention was to continue with these smaller doses (0.1 ml, 75 IU) until satisfactory resolution occurred—which did after only two doses.
This is the first case report to demonstrate the effective subcutaneous intralesional infiltration of a hyaluronidase dose titrated to response in PGS in pediatric patients. It shows a safe and effective resolution of signs with a dose of 750 IU with the patient followed-up in the outpatient setting following discharge. It adds to the limited literature on the subject. The drawbacks are that it is a single case report (level IV evidence) with no case-control and where the exact mechanism of action is unknown.
There is no current consensus on the management of extravasations with hyaluronidase in pediatric patients with literature demonstrating a range from 15 to 1500 units. 19 In a standard extravasation, the standard dose is 15 units in pediatric patients and 150 units in adults. 20 However, in the treatment of severe extravasation injury (classed as grade 3 or 4 [ie, with evidence of epidermolysis or necrosis 21 ]), then a pediatric dose of 150 units is recommended for vesicant chemotherapeutics. 22 A recent survey of pediatric intensive care units in the NHS found that teams would like to see more information on the use of hyaluronidase as a tool in the management of their patients—particularly in extravasation injuries. 23 The last published case report on the use of hyaluronidase in an infant (14 month old) with PGS was over 25 years ago; in that study, a fixed-rate dose of 24 units was used. 15 In this case we have successfully managed the patient by locally infiltrating subcutaneous hyaluronidase diffusely to the affected area, and titrating its dose to effect, rather than aiming to adhere to any specific dosing limitation. The total dose administered was 750 IU (0.5 ml of a standard 1500 IU/ml solution).
The exact mechanism by which PGS occurs is unknown, with several theories proposed—as previously discussed. Hyaluronidase is an endoglycosidase and breaks down hyaluronic acid into monosaccharides; hyaluronic acid is a major component of the extracellular matrix (ECM) and is found in multiple organs (testis, spleen, skin, eyes, liver, kidneys) as well as in body fluids (tears, blood, semen). 24 Its utility in drug-induced injuries (eg, extravasation) is thought to be as this depolymerization of the ECM increases tissue permeability to aid in dispersion of the infiltrated agents. 20 Accordingly, it can only be assumed here a similar mechanism for dissolution was employed when the hyaluronidase was injected.
The implications here are twofold. First, this case report further supports the use of hyaluronidase in PGS. Secondly, that a dose can be selected dependent on the response to the agent and—in our case—safely at 750 IU. Further study of this condition and its potential treatments is required. This includes developing a better understanding of the mechanism of PGS, the action of hyaluronidase, and the best management of PGS.
Conclusions
This case and importantly titrating to effect, with no fixed dose (up to the maximum safe reported limits for the pediatric population), provides an effective and safe treatment for treating distal cases of early cases of PGS in children. In more proximal cases, clinician discretion regarding dosage and the practicalities of subcutaneous injections should be considered.
Footnotes
Acknowledgements
A special thank you to Ms Hasu Patel who helped greatly in preparing this manuscript but passed away—we are grateful to her expertise, knowledge, and guidance.
Author Contribution
All authors contributed to the writing, design, editing, and submission of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Written consent has been obtained from the parents of the patient.