
Abstract
Keywords
Introduction
Multidrug-resistant (MDR) bacterial infections in intensive care units (ICUs) pose a significant public health risk.1,2 They are considered the leading cause of mortality in ICUs in Egypt.1-3 In 2016, Egyptian national surveillance of healthcare-associated infections found that MDR bacterial infections in ICUs had a prevalence of 54%. 2 Cefoperazone-sulbactam can effectively treat MDR gram-negative bacteria, including Pseudomonas, Acinetobacter, and Klebsiella.4,5 Although cefoperazone is extensively used in ICUs, it can induce coagulopathy.6-10 Coagulation events typically happen a few days after starting cefoperazone-sulbactam therapy.6-10 These events can result in severe adverse drug reactions, such as bleeding, which may necessitate discontinuing the use of cefoperazone-sulbactam and switching to another antibiotic. 6
There are 2 mechanisms by which cefoperazone can cause coagulopathy.6,11,12 The first mechanism, as with most antibiotics, is that cefoperazone kills gut flora, which produces vitamin K2. Vitamin K2 has an important role in the liver’s carboxylation of prothrombin precursors. The second mechanism, the cefoperazone molecule, contains a side chain called N-methylthiotetrazole (NMTT), which alters the hepatic glutathione redox state. The cefoperazone molecule inhibits the vitamin K-dependent carboxylation process by increasing oxidized glutathione levels, which antagonizes blood clotting factors.6,11,12 Therefore, prothrombin assembly and coagulation may be impeded in cases of vitamin K deficiency in the absence of an external source of vitamin K.6,11,12
Cefoperazone-sulbactam-induced coagulopathy is uncommon in healthy volunteers and patients with sufficient vitamin K supplementation; instead, it usually affects critically ill patients with impaired nutritional status, particularly vitamin K deficits.13-15 Vitamin K insufficiency in critically ill patients can arise from a variety of factors, such as the use of drugs like warfarin or broad-spectrum antibiotics that kill normal flora, malabsorption, pre-existing deficiencies, and poor long-term oral, enteral, or parenteral nutrition intake.16,17
Vitamin K is a crucial anti-hemorrhagic factor because it promotes the production of clotting factors II, VII, IX, and X. 18 The manifestation of vitamin K deficiency is coagulopathy, characterized by easy bruising, hematuria, or melena. 17 The requirements for supplementation with vitamin K are different between patients and may vary for the same patient on different occasions. This requirement depends on the patient’s history, such as comorbidities, prior deficiency, gastrointestinal malabsorption, and the ability to tolerate food and drinks taken orally or through a feeding tube. 17
The recommended nutritional supplemental dose for vitamin K, based on the guidelines of the American Society for Parenteral and Enteral Nutrition (ASPEN), published in 2016, is 0.5 to 1 mg/day or 5 to 10 mg once per week. 19 Different routes of vitamin K are available, including intramuscular (IM), intravenous (IV), and subcutaneous (SC). In ICU units, IV injection of vitamin K is the recommended method due to its superior bioavailability.15,17,20,21
Vitamin K is an antihemorrhagic agent that is usually used to treat coagulopathy in ICU patients, 17 particularly, anticoagulant reversal or treatment of prothrombin deficiency secondary to other factors in adults.15,22 On the other side, in neonates, vitamin K is used as both a prophylaxis and a treatment for hemorrhagic disease. 22 The FDA has approved vitamin K in the treatment of anticoagulant-induced prothrombin deficiency, treatment of prothrombin deficiency secondary to other drug therapy or factors, prophylaxis, and treatment of newborn hemorrhagic disease. 22 However, it is not commonly used in adult patients as a prophylactic or nutritional supplement in most hospitals. 17
Vitamin K has a high safety profile, except for a warning about the risk of hypersensitivity with parenteral vitamin K. 22 However, the incidence of hypersensitivity is 3 per 10 000 intravenous vitamin K doses. 22 The use of prophylactic doses of vitamin K could prevent coagulopathy without significant adverse effects. 23 Our study aimed to determine the impact of co-administering prophylactic doses of vitamin K with cefoperazone-sulbactam on coagulopathy prevention.
Patients and Methods
Patients
Patients’ selection
Adult patients who were admitted from February to October 2023 at the ICU of 6-October Hospital, General Health Insurance Organization, Ministry of Health, Egypt, were recruited for this study.
Inclusion criteria
Patients admitted to the ICU were given either prophylactic or therapeutic doses of cefoperazone-sulbactam.
Patients who are 18 years or older.
Exclusion criteria
Patients who were treated with cefoperazone-sulbactam for less than 1 day (received less than 2 doses).
Active bleeding at baseline.
Bleeding disorder at baseline.
Patients with an abnormal coagulation profile at baseline.
Hepatic dysfunction at baseline.
Septic shock.
Patients who received therapeutic doses of anticoagulant.
Patients who received total parenteral nutrition were supplemented with vitamin K on a regular basis.
Pregnant women.
Breastfeeding women.
Patients who refused to sign the written informed consent.
Methods
Study design
Our study was an interventional, single-center, prospective randomized controlled trial.
Methodology
The study included eligible patients after taking a full history, conducting a physical examination, and performing complete investigations. Randomization was used to assign the included patients to 2 groups: the control group (Gp-C) and the intervention group (Gp-I). Gp-I received prophylactic doses of vitamin K (10 mg) slowly given intravenously every week until systemic cefoperazone-sulbactam antibiotic therapy was ended; Gp-C received systemic cefoperazone-sulbactam antibiotic alone. A randomization algorithm that was generated by a computer was used for block randomization. An independent statistician kept the allocation sequence hidden and communicated it to the investigator by telephone.
Treatment
The included patients received systemic intravenous cefoperazone-sulbactam doses of 1.5 to 2 g every 12 hours, according to the decisions of their responsible physicians and based on the hospital treatment protocol. The given antibiotics were either cefoperazone-sulbactam of 1.5 g (Cefazone Plus®, Pharco B International, Alexandria, Egypt) or cefoperazone-sulbactam of 2 g (Trexotaz 2 g®, Rameda, Giza, Egypt), while intravenous vitamin K was given as a dose of 10 mg (Epikavit®, EIPICO, 10th of Ramadan city, Egypt).
Data collection
Patient demographics such as age, gender, history of comorbidities, investigational data, and laboratory data, including a complete blood count, and coagulation profile were reported during the total hospital stay. The reports included information on the severity of the adverse drug events, type of bleeding, bleeding category (minor or major), the intervention to the bleeding events, and the incidence time for adverse events from the antibiotic exposure.
Measured outcomes
A clinical assessment was performed for each patient during the whole antibiotic treatment period. As per the local antibiotic policy, the cefoperazone-sulbactam antibiotic is assessed every 3 days. The patients’ data was collected daily from baseline until the last day of cefoperazone-sulbactam administration. The data included INR, hemoglobin, platelet count, renal function tests, and liver enzyme tests. The measured outcomes included the highest INR level while receiving the antibiotic, the percentage of INR increase from the baseline, the proportion of patients with coagulopathy (INR increase more than 30% of the baseline), and the proportion of patients with bleeding. Time to coagulopathy and time to bleed were calculated. Coagulopathy and bleeding incidences were also reported in the 2 groups to evaluate the role of vitamin K in preventing coagulopathy induced by cefoperazone-sulbactam. Coagulopathy (based on local hospital policy) was indicated by unstable INR, which was defined by increasing INR > 30% above the baseline; the last INR was recorded before starting cefoperazone-sulbactam. 9 INR was calculated using a formula that incorporated patient prothrombin time and the normal prothrombin time. 24
Two categories of bleeding, according to the International Society on Thrombosis and Hemostasis, were applied: major and minor bleeding. Major bleeding is defined as bleeding causing falls in hemoglobin levels of 2 g/dL or more or required transfusion of 2 units or more of whole blood or red cells, and/or serious bleeding such as intracranial hemorrhage. Minor bleeding was considered any bleeding that could not be categorized as major.25,26
Statistical Analysis
Sample size calculations
Based on our preliminary observations, the incidence of coagulopathy with cefoperazone is up to 45%, 27 and the expected incidence of coagulopathy in patients who received vitamin K concurrently with cefoperazone-sulbactam is 5%. According to this effect size, the sample size calculator estimated that each group would need 25 patients to address this effect (with a power of 80% and an alpha error of 5%). We took the potential loss of follow-up into account and overrecruited. Therefore, a total of 56 patients; 28 patients for each group, were recruited and participated in the study.
Data analysis
Data analysis was performed using the R software version 4.2.2 (The R Project for Statistical Computing, Vienna, Austria). In all analyses, a level of 0.05 was considered significant.
Categorical variables were presented as frequencies and percentages, and associations between the categorical variables in the 2 treatment groups were tested using either the Chi-square test or the Fisher exact test, as appropriate.
For testing the normal distribution of continuous data, the Shapiro-Wilk test was used. Means and standard deviations were used to describe parametric data, while medians were used to describe non-parametric data. The extreme values in non-parametric data were presented through range instead of IQR to describe the real difference between the 2 groups. For normally distributed variables, the t-test was used, while the Mann-Whitney U test was used for non-normally distributed variables.
We conducted a survival analysis to examine the time to bleed and the time to develop coagulopathy. We used Kaplan-Myers curves and log-rank tests for both outcomes. We conducted a Cox proportional hazards regression analysis to determine the adjusted hazard ratios (HR) for coagulopathy between the intervention and control groups while controlling for all expected confounders.
Results
Patient Enrollment and Follow Up
A total of 68 patients were recruited and enrolled in the study. Twelve patients were excluded for the following reasons: 1 patient is 16 years old (below 18 years), 3 cases died before receiving more than 3 doses of the antibiotic, 2 cases declined to participate, 3 cases had septic shock, and 3 cases had hepatic encephalopathy with coagulopathy. A total of 56 patients participated in the study; they were randomly divided into 2 groups, with 28 patients in each group. There is no loss in following up; therefore, as shown in Figure 1, each group of 28 patients finished the study.
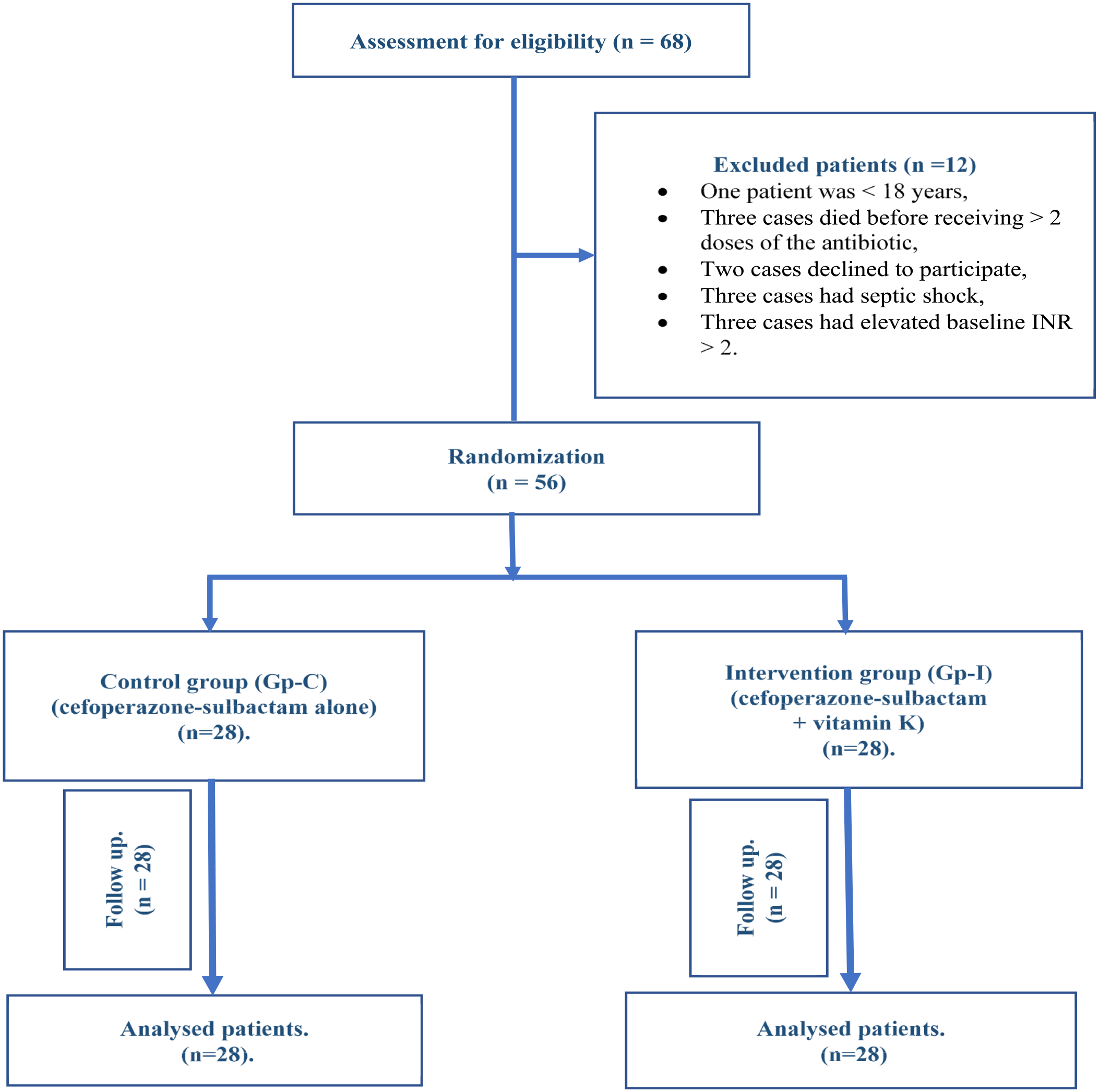
Patient enrollment and follow up.
Baseline Characteristics and Pre-treatment Clinical Data
The included patients had a median age of 64.5 (32-89), and 68% of them were males. Most of the patients were in the medical ICU (64.3%). Table 1 summarizes the baseline characteristics of the 2 studied groups. There were no significant differences in baseline characteristics between the 2 groups, except for the intervention group, which had a significantly lower baseline platelet count than the control group (P = .037).
Baseline Characteristics and Pretreatment Clinical Data of the 2 Studied Groups.
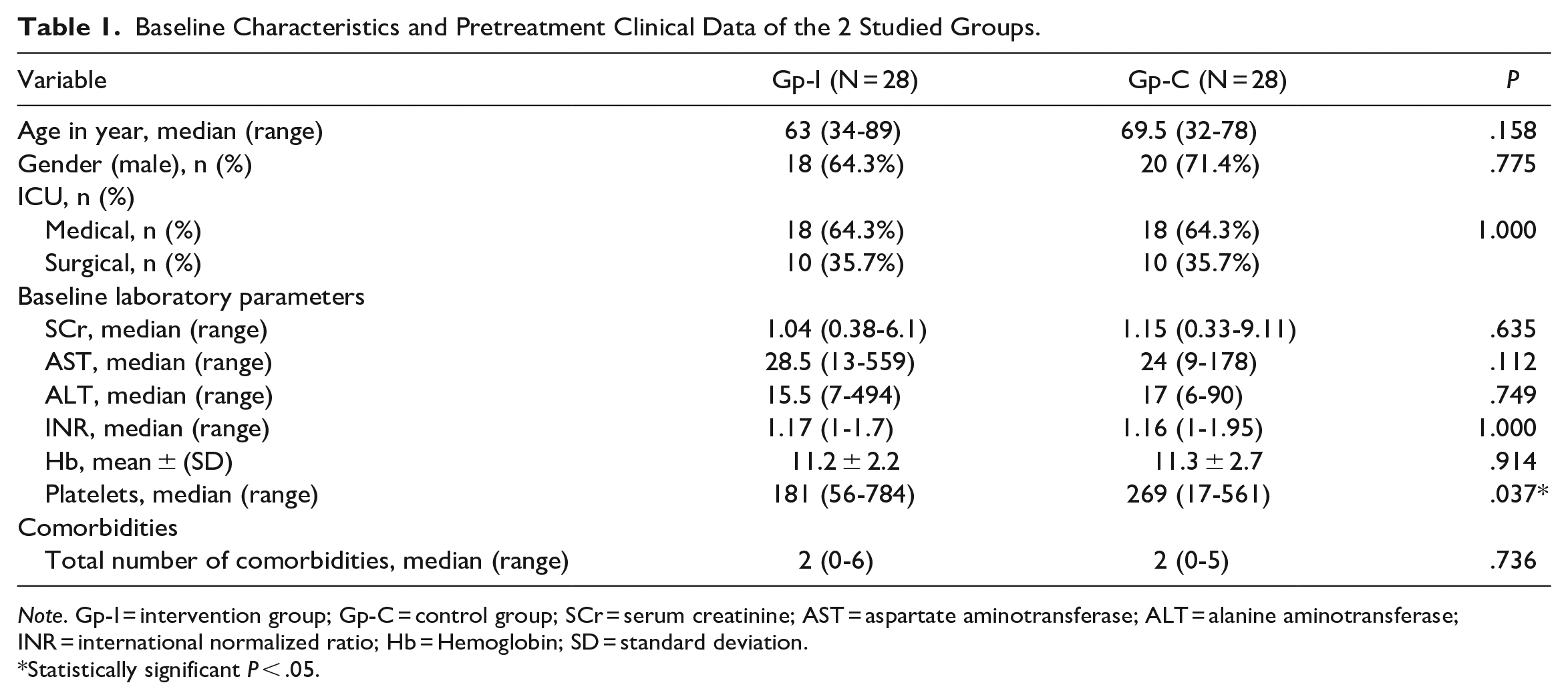
Note. Gp-I = intervention group; Gp-C = control group; SCr = serum creatinine; AST = aspartate aminotransferase; ALT = alanine aminotransferase; INR = international normalized ratio; Hb = Hemoglobin; SD = standard deviation.
Statistically significant P < .05.
Table 2 summarizes the Concurrent medications and antibiotic dosage regimen in the 2 groups. There were no significant differences in the concomitant diseases and concurrent medications between the 2 treatment groups. The daily dose of cefoperazone-sulbactam differed significantly between the 2 groups (P = .002); however, the total cumulative doses were comparable (P = .811).
Concurrent Medications and Antibiotic Dosage Regimen in the 2 Studied Groups.
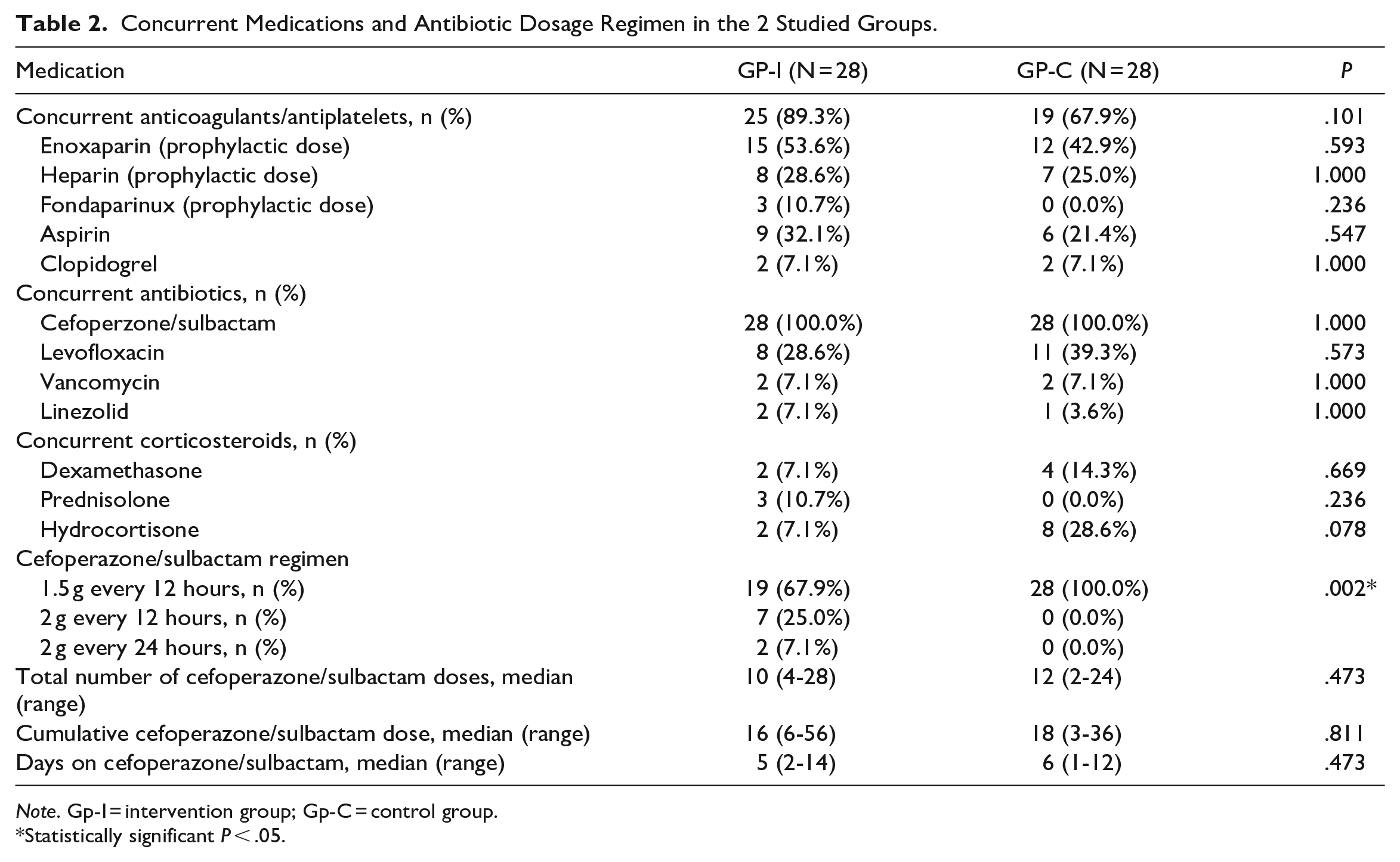
Note. Gp-I = intervention group; Gp-C = control group.
Statistically significant P < .05.
Post-Treatment Monitoring
The post-treatment laboratory parameters and coagulopathy markers are presented in Table 3. All cases of bleeding occurred in Gp-C in 7 patients (P = .010). A significantly higher INR level of median 1.6 (the highest-level post-antibiotic) was observed in Gp-C compared with Gp-I (P < .001). A significantly higher proportion of patients with coagulopathy was observed in Gp-C as compared to Gp-I (64.3%vs 3.6%, P < .001). Furthermore, a significantly higher proportion of patients in Gp-C had INR levels that increased above double the baseline when compared to Gp-I (21.4% vs 0, P = .002).
Post-treatment Laboratory Parameters of the 2 Studied Groups.
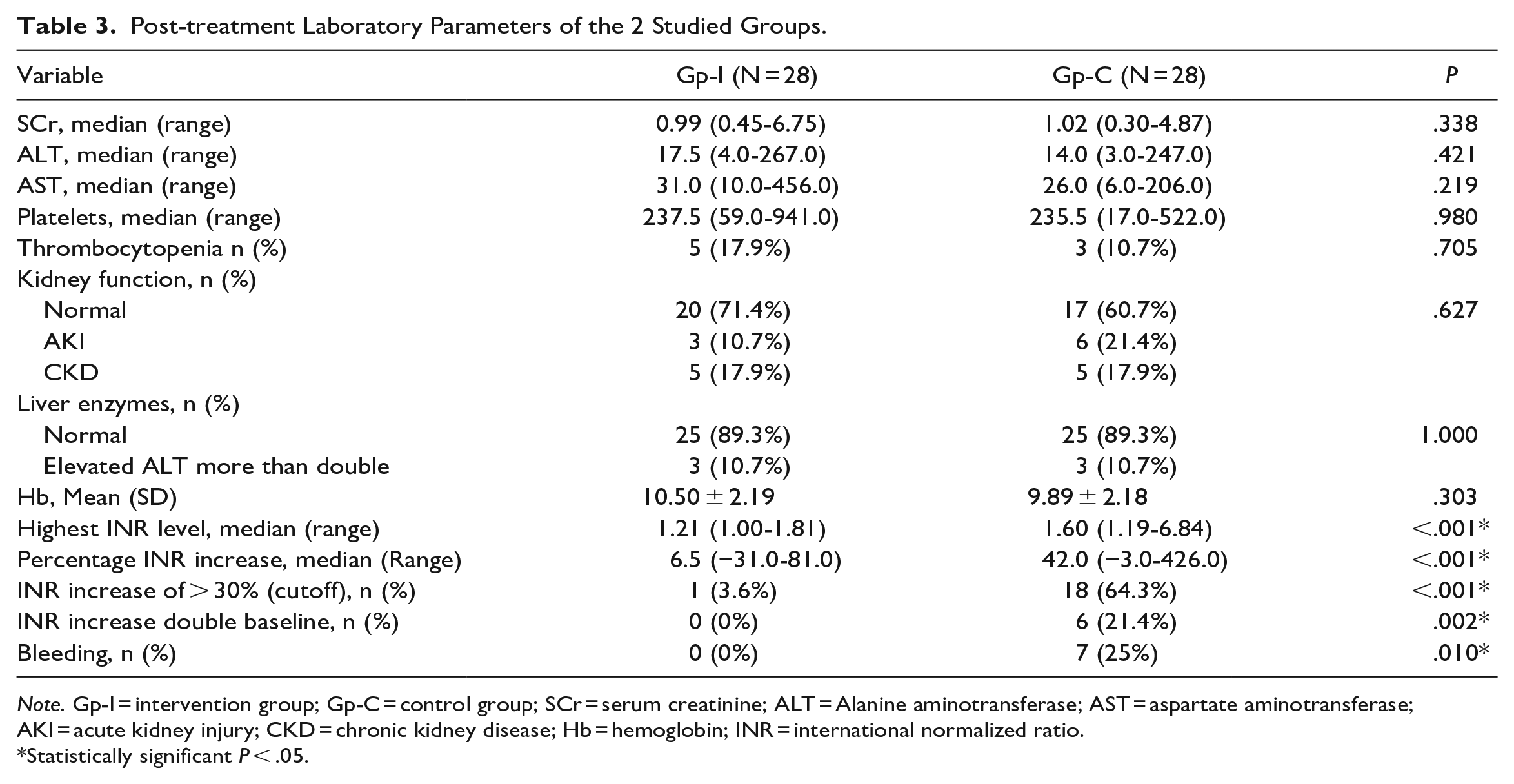
Note. Gp-I = intervention group; Gp-C = control group; SCr = serum creatinine; ALT = Alanine aminotransferase; AST = aspartate aminotransferase; AKI = acute kidney injury; CKD = chronic kidney disease; Hb = hemoglobin; INR = international normalized ratio.
Statistically significant P < .05.
Survival Analysis
Time to coagulopathy (increase INR >30% from the baseline) analysis
The time to coagulopathy analysis is shown in Figure 2. The log-rank test indicated a significantly higher survival probability in Gp-I than in Gp-C (χ2 = 25.5, degree of freedom = 1, P < .001). The median time to coagulopathy in Gp-C was 3 days, while the median time to coagulopathy in Gp-I couldn’t be calculated as the total number of cases of coagulopathy in Gp-I did not exceed 50%. The restricted mean survival time in Gp-I was 13.5 days (95% CI: 12.6-14.4 days) and in Gp-C was 6.1 days (95% CI: 4.1-8.1 days); the difference was statistically significant, with 7.4 days less in Gp-C (95% CI: 5.2-9.6 days, P < .001).
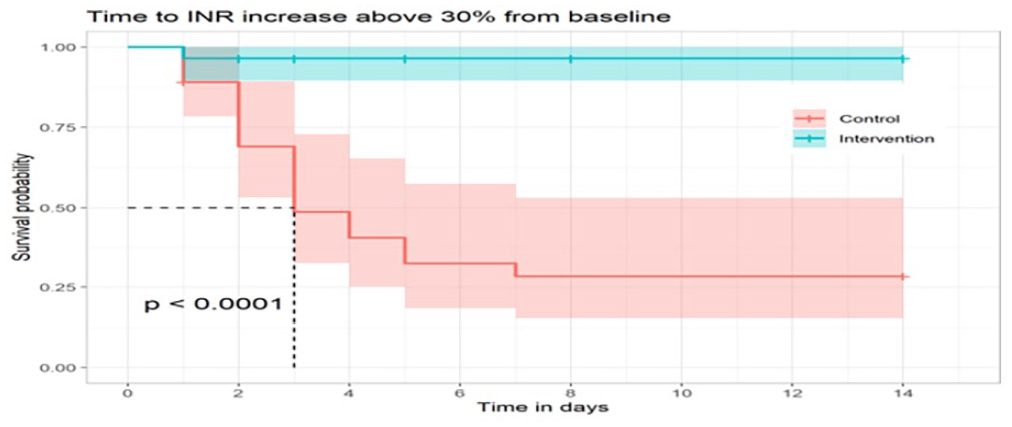
Time to coagulopathy (increase INR > 30% from baseline).
Regression analysis of the time to coagulopathy
Table 4 summarizes the adjusted hazard ratios for coagulopathy using the Cox regression analysis. Gp-I was significantly associated with a 99% reduction in the hazard of coagulopathy relative to Gp-C (95% CI: 84%-100%, P = .001). The data revealed no significant correlation between the incidence of coagulopathy and the expected confounding factors such as gender, age, and baseline laboratory data, including INR, platelet count, SCr, and ALT.
Summary of the Cox Proportional Hazards Regression Analysis for the Time to Coagulopathy (Increase INR > 30% From Baseline).
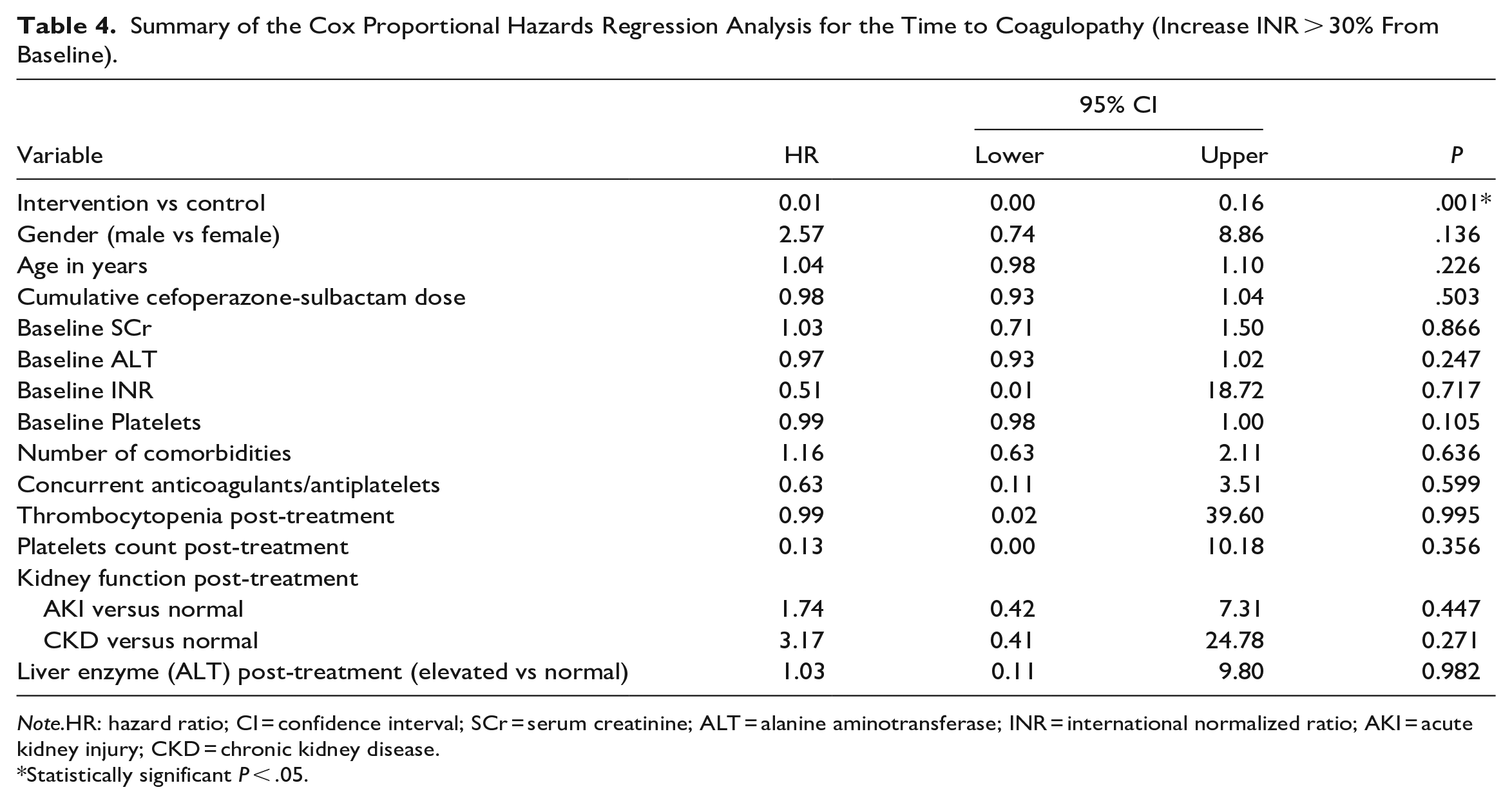
Note.HR: hazard ratio; CI = confidence interval; SCr = serum creatinine; ALT = alanine aminotransferase; INR = international normalized ratio; AKI = acute kidney injury; CKD = chronic kidney disease.
Statistically significant P < .05.
Time to bleed analysis
The time-to-bleed analysis showed that all bleeding cases happened in Gp-C (Figure 3). Descriptive statistics of bleeding cases in the control group showed that the median age of bleeding cases is 70 (34-77) years, and 57.1% of the bleeding cases are in the major bleeding category. The types of bleeding were hematuria (42.9%), hematemesis (28.6%), melena (14.3%), and coffee ground emesis (14.3%).
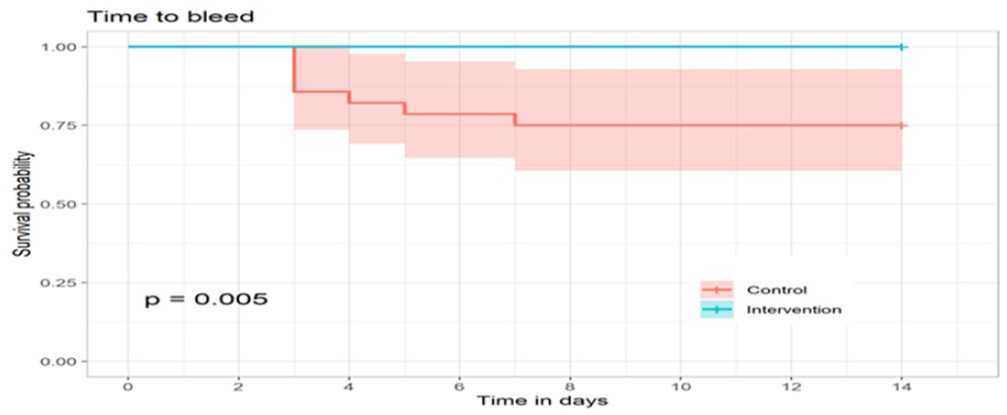
Time to Bleed analysis in the 2 treatment groups.
The log-rank test indicated a significantly higher survival probability in Gp-I than in Gp-C (χ2 = 9, degree of freedom = 1, P = .005). No median time to bleed could be calculated in Gp-C as the total number of bleeding cases did not exceed 50%. The restricted mean survival time in Gp-I was 14 days (95% CI: 14-14 days) and in Gp-C was 11.5 days (95% CI: 9.9-13.1 days); the difference was statistically significant, with 2.5 days less in Gp-C (95% CI: 0.9-4.1 days, P = .003). No Cox regression could be conducted between the 2 groups as no bleeding events occurred in Gp-I.
Regression analysis of the time to bleed in the control group
The adjusted hazard ratios for the time to bleed in the control group resulting from the Cox regression analysis are summarized in Table 5. The analysis found no statistically significant correlation between gender, age, the presence of thrombocytopenia post-treatment, and the incidence of bleeding in the control group.
The Cox Proportional Hazards Regression Analysis for the Time to Bleed in the Control Group.
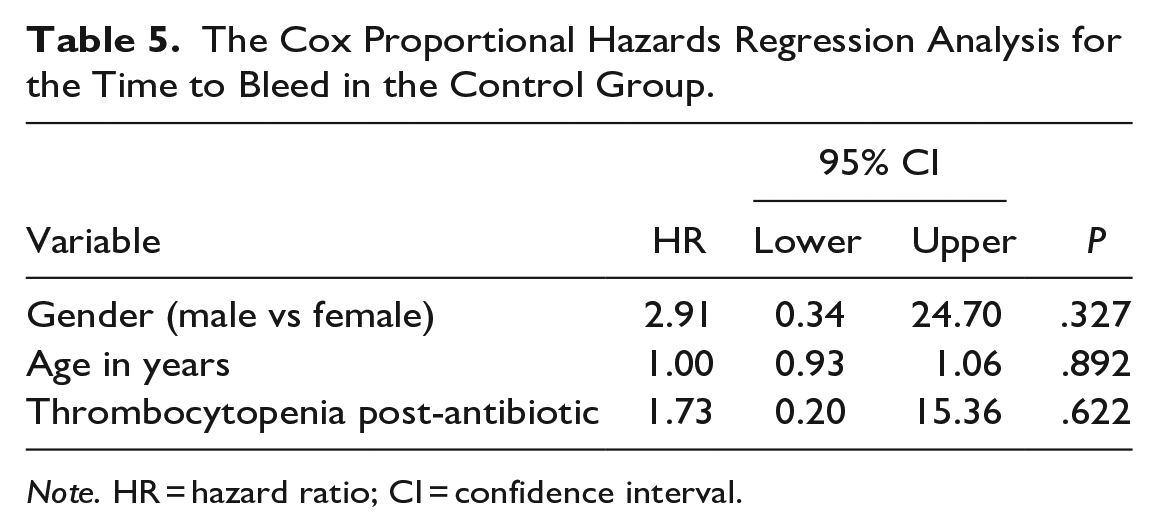
Note. HR = hazard ratio; CI = confidence interval.
Discussion
Cefoperazone-sulbactam-induced coagulopathy is typically seen in critically ill patients.16,17,28 Our study results declared that vitamin K had a prophylactic benefit in preventing cefoperazone-sulbactam-induced coagulopathy. We revealed that these prophylactic doses of vitamin K showed many clinically significant outcomes. First, a 99% reduction in the hazard of coagulopathy in Gp-I. Second, keeping a stable INR with a significantly higher survival probability in Gp-I. Third, delaying the incidence of coagulopathy events in Gp-I. Fourth, a total prevention of the bleeding events in Gp-I. Fifth, no anaphylaxis reaction was reported in both groups.
The only significant factor responsible for the reduction in coagulopathy incidence in the intervention group is the administration of prophylactic doses of vitamin K. We found no significant differences between the 2 groups except for the baseline platelet count and the dose of cefoperazone-sulbactam used. Therefore, we performed the regression model, which revealed no statistically significant association between either baseline platelet count or the presence of thrombocytopenia during the antibiotic treatment or cefoperazone-sulbactam cumulative doses and the incidence of coagulopathy in both groups. No effect modifier was observed for all expected confounders such as gender, age, total cumulative dose of cefoperazone-sulbactam, baseline data including INR, platelet count, SCr, and ALT, number of comorbidities, concurrent anticoagulant prophylactic doses, post-treatment laboratory data including platelet count, thrombocytopenia, kidney function state (normal, acute kidney injury, chronic kidney disease), and liver enzymes (normal, elevated ALT more than double).
Previous literature data agreed with our results; many case reports and case series reported the incidence of coagulopathy or bleeding with the administration of cefoperazone in the absence of vitamin K supplementation.6,8,10,27,29 Two observational studies found that using vitamin K prophylactic doses was effective in preventing bleeding incidence and reducing the frequency of cefoperazone-sulbactam-induced coagulopathy.30,31 On the contrary, a retrospective cohort study was performed at a teaching hospital in Philadelphia in 1999. 32 They studied the incidence of hypoprothrombinemia and bleeding in 3 groups of patients administered cefoperazone or other cephalosporin antibiotics. Hypoprothrombinemia has been linked to the use of cefoperazone. They assumed that prophylactic doses of vitamin K are not necessary. The rationale that could be behind this controversy is that the study participants had a high risk of potential confounding variables, such as concurrent use of anticoagulants, particularly warfarin. This masked the prophylactic effect of vitamin K among patients with hypoprothrombinemia.
In 1992, another retrospective study in the USA concluded that routine administration of vitamin K during prophylactic use of cefoperazone in urologic surgery is unnecessary in patients without major risk factors for bleeding. 33 Their study was conducted on 50 patients who underwent urologic procedures and were given cefoperazone-sulbactam at a daily dose of 2 g for 3 days to prevent infection. Before receiving cefoperazone, 10 mg of subcutaneous vitamin K was administered to 11 of 50 patients. This controversy is due to several factors. First, the cefoperazone treatment was only administered for a duration of 3 days as part of a surgical prophylaxis regimen. Second, there was no evidence indicating that the urologic surgical patients were malnourished or at risk of developing vitamin K deficiency. On the other hand, our study was a randomized controlled trial that focused on critically ill patients who were at higher risk for vitamin K deficiency. Our findings revealed that over 50% of the cases developed coagulopathy on day 3, which means the prophylactic effect of vitamin K should be evaluated for a study duration of more than 3 days.
In Conclusion
Coagulopathy is a common complication among ICU patients who receive cefoperazone-sulbactam therapy in Egypt. However, vitamin K, which is often used to treat this condition, is not typically administered for prevention or as a nutritional supplement in most hospitals. Therefore, after careful consideration of its benefits and the risk of anaphylactic reactions with the vitamin K IV route, we cautiously recommend the addition of vitamin K to prevent the coagulopathies associated with this mechanism.
Recommendations
We recommend adding vitamin K prophylaxis doses to the local ICU protocols for critically ill patients who are treated with cefoperazone-sulbactam at a dosage of 3 to 4 g per day for more than 3 days. This will help in the prevention of the development of cefoperazone-sulbactam-induced coagulopathy. We suggest that the parent company of cefoperazone-sulbactam in Egypt should modify the medicine’s package insert to encourage the usage of prophylactic doses of vitamin K and implement educational programs to ensure the safe usage of the medicine.
Footnotes
Availability of Data and Materials
The data that support the findings of this study are available on request from the corresponding author [Hebatallah A. Abdeen].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Approval from the ethical committee at the Faculty of Pharmacy, Helwan University, was obtained (approval number: 04H2021) and from the ethical committee of the Ministry of Health and Population (approval number: 21-2021/9). All included patients signed informed consent to participate and publish.