
Abstract
Sertraline, a selective serotonin reuptake inhibitor, is a medication recommended as a third line treatment of cholestatic liver injury pruritis. We report a case of a young male who developed liver injury secondary to self-administration of anabolic steroids and who complained of persistent pruritis leading to a treatment by sertraline. Two days later, the patient was admitted to the hospital with a severe hypoglycemia, while the liver function tests were in amelioration. Clinical and biological evaluation were in favor of sertraline-induced hypoglycemia, a side effect rarely reported in non-diabetic patients, and in the context of hepatic injury.
Keywords
Introduction
Pruritis is a common and potentially disabling symptom in patients with cholestatic liver injury. 1 It is frequently seen in patients with drug-induced liver injury (DILI). 1 Treatment of pruritis in cholestatic liver injury follows a stepwise approach. When drug-induced, withdrawal of the offending agent is the treatment of choice. 1 In persistent pruritis, bile acid sequestrants (eg, cholestyramine) are considered a first-line treatment. 1 Sertraline is also recommended for symptomatic relief, however its mechanism of action remains unclear. 1 We report a case of DILI complicated with invalidating pruritis, where treatment with sertraline led to a complication rarely reported in non-diabetic patients.
Case
A 22-year-old male developed liver injury secondary to oral and intramuscular self-administration of anabolic steroids. He complained of invalidating pruritis on presentation and treatment with cholestyramine (4 g 3 times daily) was immediately started in addition to anabolic steroids withdrawal. Due to the persistence of severe pruritis, fexofenadine 180 mg twice daily was added 1 week later, followed by sertraline 50 mg once daily 2 weeks after initial presentation.
After receiving 2 doses of sertraline, he presented to the emergency department with symptoms of sweating and altered mental status. Laboratory tests revealed improved liver function tests and a normal prothrombin time. There was no evidence of hyperammonemia (ammonia levels <15 µg/100 mL) or other metabolic abnormalities, except for severe hypoglycemia (blood glucose at 47 mg/dL).
This patient had no history of diabetes mellitus and denied self-administration of antidiabetics agents. Cortisol levels were at 158 ng/mL (normal range: 50-250 ng/mL), insulin levels at 17.1 µIU/mL (normal range: <29 µIU/mL), and peptide C levels at 4.3 ng/mL (normal range: 0.9-7.1 ng/mL).
The patient’s symptoms improved with administration of glucose. He received 7 infusions of 6 g/20 mL glucose 30% solutions. Given the presence of the Whipple triad (presence of hypoglycemia with symptoms of hypoglycemia, that resolve after glucose administration) and the low ammonia levels, an altered mental status due to hypoglycemia was the established diagnosis.
Upon admission, sertraline treatment was discontinued. No further hypoglycemia events were reported after the discontinuation of sertraline. Two months later, on follow-up, his liver function tests normalized.
Discussion
This is the case of a young male with hepatitis, that presented to the emergency department with altered mental status. The differential diagnosis of altered mental status in the setting of liver injury is wide. Hepatic encephalopathy was unlikely since the liver function tests were improving and the patient had low ammonia levels. Given the presence of the Whipple triad, an altered mental status due to hypoglycemia was the established diagnosis.
The etiology of hypoglycemia was to be determined. The patient had been eating well, there were no signs of sepsis, and insulinoma and adrenal insufficiency were ruled out. Self-administered antidiabetic therapy was denied by the patient. Anabolic steroids use is associated with diabetes mellitus and not hypoglycemia. 2 Our patient discontinued anabolic androgens 2 weeks prior to presentation and denies exogenous insulin use. In addition, his insulin and peptide C levels do not suggest this diagnosis. Sertraline and other SSRI have been reported to induce hypoglycemia in several case reports,3,4 some of which occurred in diabetic patients treated by oral antidiabetics and/or insulin, 3 and in the other cases there was no clear underlying mechanisms or precipitating factors. 4
The underlying mechanism of SSRI-induced hypoglycemia is still unclear. While some animal models suggest that sertraline increases insulin release, reduced gluconeogenesis and increased insulin sensitivity, others proved that it increases counterregulatory responses to hypoglycemia. 5 In an animal model, after infusion of fluvoxamine directly into the portal vein the net hepatic glucose uptake was increased. 6 This suggests that SSRIs enhance insulin sensitivity and that they may have a role in reducing postprandial hyperglycemia. 6 Sertraline has linear pharmacokinetics, but there is no clear correlation between plasma concentrations and therapeutic outcomes or adverse events. 7 Improvement after withdrawal of sertraline has led us to the conclusion that the patient suffered from sertraline-induced hypoglycemia.
Sertraline is an agent that can be used to treat cholestatic pruritis, as evidenced by the EASL clinical practice guidelines for management of cholestatic liver diseases. 1 It has been shown to be efficient and well tolerated in the context of liver injury at 75 to 100 mg/day. 8 Given that it is metabolized by the liver, it should be cautiously titrated1,8 even if it is usually well tolerated in the context of liver injury. 8
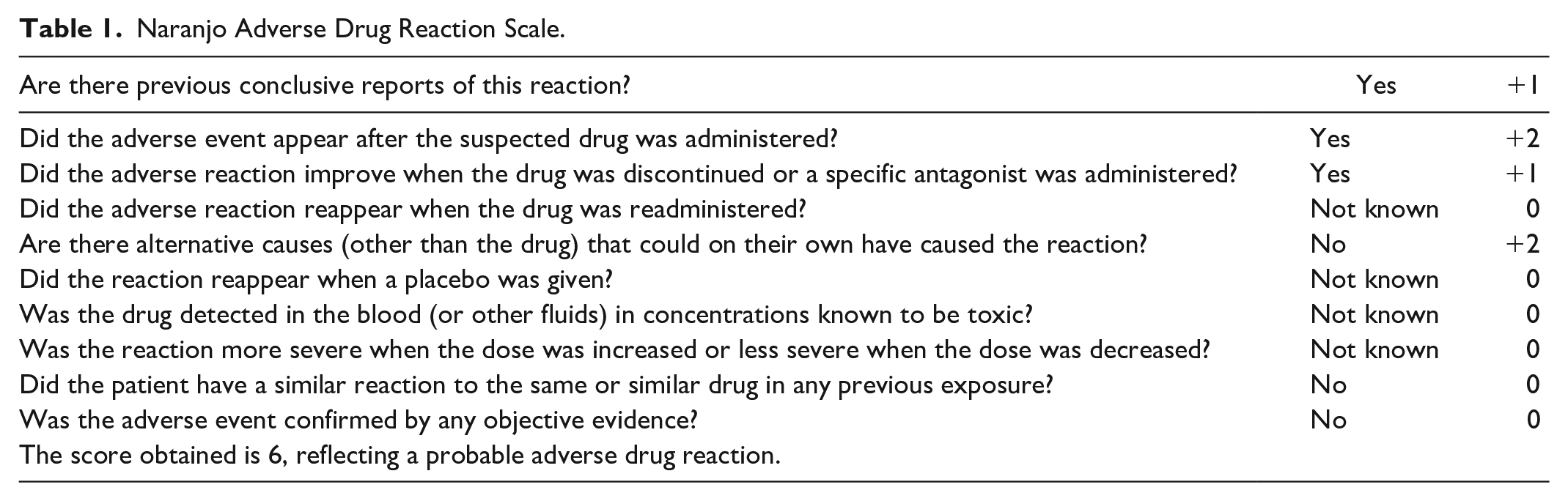
To our knowledge, this is the first case of sertraline-induced hypoglycemia in the setting of hepatitis. We used the Naranjo adverse drug reaction scale was used to determine the causality. 9 The score obtained was 6, reflecting a probable adverse drug reaction (Table 1). 9
Naranjo Adverse Drug Reaction Scale.
This raises the question of whether liver injury increases the risk of hypoglycemia events in patients taking sertraline or other SSRIs. The main route of sertraline metabolism is through the liver via the CYP 450 enzyme, and dose modification is only recommended in patients with hepatic impairment and decompensated cirrhosis. 10 Note that our patient did not have evidence of liver failure. Further studies need to be done to investigate the potential role of liver injury in sertraline-induced hypoglycemia. Our case raises concerns about this side effect and implies a close follow-up of blood glucose levels in patients with active hepatitis on sertraline or other SSRIs.
Conclusion
Particular attention must be warranted in patients with active hepatitis on SSRIs, as altered mental status can be falsely attributed to hepatic encephalopathy. When putting patients on sertraline for depression or pruritis in the setting of liver injury, close follow-up of blood glucose levels is necessary.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
An informed consent was obtained from the patient.