
Abstract
Introduction:
The ability to obtain a quantitative drug level for apixaban and rivaroxaban exists using drug-specific calibrated anti-Xa assays; however, no standard exists defining when to obtain direct oral anticoagulant (DOAC) concentrations or how to adjust medication regimens based on the results.
Objective:
Describe the incidence of DOAC levels obtained, identify trends in prescribing DOAC levels in clinical practice, and qualitatively assess level appropriateness and actions taken based on level results.
Methods:
A qualitative, retrospective analysis was conducted using the electronic medical record to identify adult inpatients within a 10-hospital health system with a calibrated apixaban or rivaroxaban anti-Xa level result from April 1, 2020, to November 1, 2022. The primary endpoint was the incidence of DOAC levels drawn. Secondary outcomes included the percentage of DOAC concentrations that prompted a dose change, association between dose or agent change and concentrations outside the on-therapy range, and association between indication for obtaining DOAC levels and resultant concentrations.
Results:
One-hundred thirty-two calibrated anti-Xa levels were obtained in 101 inpatients during the study period, representing a level drawn in 0.48% of all apixaban and rivaroxaban orders. Eighty-three (63%) patients were on apixaban. Primary reasons to draw DOAC levels were extreme body weight (35%), treatment failure concerns (23%), bleeding concerns (18%), and drug interactions (14%). Only 42 (31.8%) of all levels were drawn appropriately as a peak. Seventeen (40.4%) of the peak levels were within the on-therapy range. Of the 25 levels outside the on-therapy range, 14 (56%) resulted in no change in therapy. For all levels drawn, 70 (53%) resulted in no change to therapy.
Conclusions:
DOAC concentrations are often drawn at inappropriate times and seldom influence a dose or agent change. Future research is needed to determine if DOAC concentrations may be clinically meaningful in a select subgroup of patients.
Keywords
Introduction
The use of direct oral anticoagulants (DOACs) has increased significantly over the past decade with concurrent declines in warfarin use. 1 DOACs are considered an alternative to warfarin for many thromboembolic indications such as prevention of stroke in atrial fibrillation as well as prevention and treatment of venous thromboembolism (VTE). 2 DOACs inhibit coagulation by binding to the active site of either factor Xa (apixaban, edoxaban, and rivaroxaban) or thrombin (dabigatran). 1 Benefits to using DOACs include fewer drug and food interactions and a wider therapeutic range which enables fixed dosing regimens without routine coagulation monitoring. 3
The ability to obtain calibrated apixaban and rivaroxaban anti-Xa levels is currently available; however, there is a paucity of data on if and when these levels should be drawn and if a medication regimen should be adjusted based on these results. 4 Quantitatively evaluating the concentrations of a DOAC may be useful in certain situations to manage the care of a patient such as thrombotic or bleeding events while on DOAC therapy, upcoming or emergent surgeries, and overdose suspicion.3,4 Certain populations are more at risk of having levels outside of what is expected such as patients with extreme weights (≥120 kg or ≤50 kg), absorption concerns such as following gastric bypass procedures, renal and/or hepatic dysfunction, and increased age. Combining DOACs with agents known to modify CYP3A4 and P-gp function can alter DOAC exposure, especially if renal clearance is impaired. 5 Despite having clinically appropriate situations for obtaining DOAC anti-Xa levels to determine if a patient is actively anticoagulated, there are no evidence-based recommendations on how to adjust therapies based on levels or if drug-concentration levels correlate with outcomes. 4 More research is needed to identify the most appropriate patient populations and clinical scenarios in which to utilize these levels. The objective of this study was to quantify the incidence of DOAC levels obtained, identify trends in prescribing DOAC levels in clinical practice, and qualitatively assess level appropriateness and actions taken based on level results.
Methods
This retrospective analysis was approved by the University of Minnesota Institutional Review Board (STUDY00017547). A health record report was conducted to identify all adult hospitalized patients with an inpatient calibrated apixaban or rivaroxaban anti-Xa level result across the ten-hospital health system from April 1, 2020 to November 1, 2022. All levels were evaluated with and without documented timing of the dose prior to the level. Levels were excluded if patients were pregnant or opted out of research. The health system has no standard protocol for what clinical scenarios apixaban or rivaroxaban levels should be drawn.
Testing for apixaban and rivaroxaban was performed using a chromogenic anti-factor Xa assay (STA Liquid Anti-Xa, Diagnostica Stago, Parsipanny, NJ) calibrated for apixaban and rivaroxaban, respectively (STA-Apixaban Calibrator and STA-Rivaroxaban Calibrator, Diagnostica Stago). Testing was initially performed on a STA-R Evolution analyzer (Diagnostica Stago) until April 13, 2022 and then was performed on a STA-R Max analyzer (Diagnostica Stago, Parsipanny, NJ). All levels were run at one of the hospitals within the health system but were available to be ordered at all sites. For this assay, excess factor Xa is added to the patient’s plasma sample which forms a complex with any available DOAC present. 6 A chromogenic substrate is then added to bind to any factor Xa that remains which produces a color change. The brightness of the sample is inversely proportional to the amount of DOAC present. “On-therapy” ranges or levels in the pharmacokinetic studies during apixaban and rivaroxaban development are peak levels, drawn 2 to 4 hours after a dose.7,8 These ranges vary depending on the dosing regimen and indication (Table 1). Apixaban peaks were defined as any level drawn within 3 to 4 hours after a given dose and rivaroxaban peaks were defined as any level drawn within 2 to 4 hours after a given dose. Non-peak levels were defined as levels obtained 0 to 2 hours or greater than 4 hours after a rivaroxaban dose; drawn 0 to 3 hours or greater than 4 hours after an apixaban dose. Levels were deemed unknown if there was no clear documentation of when the last DOAC dose was administered/taken.
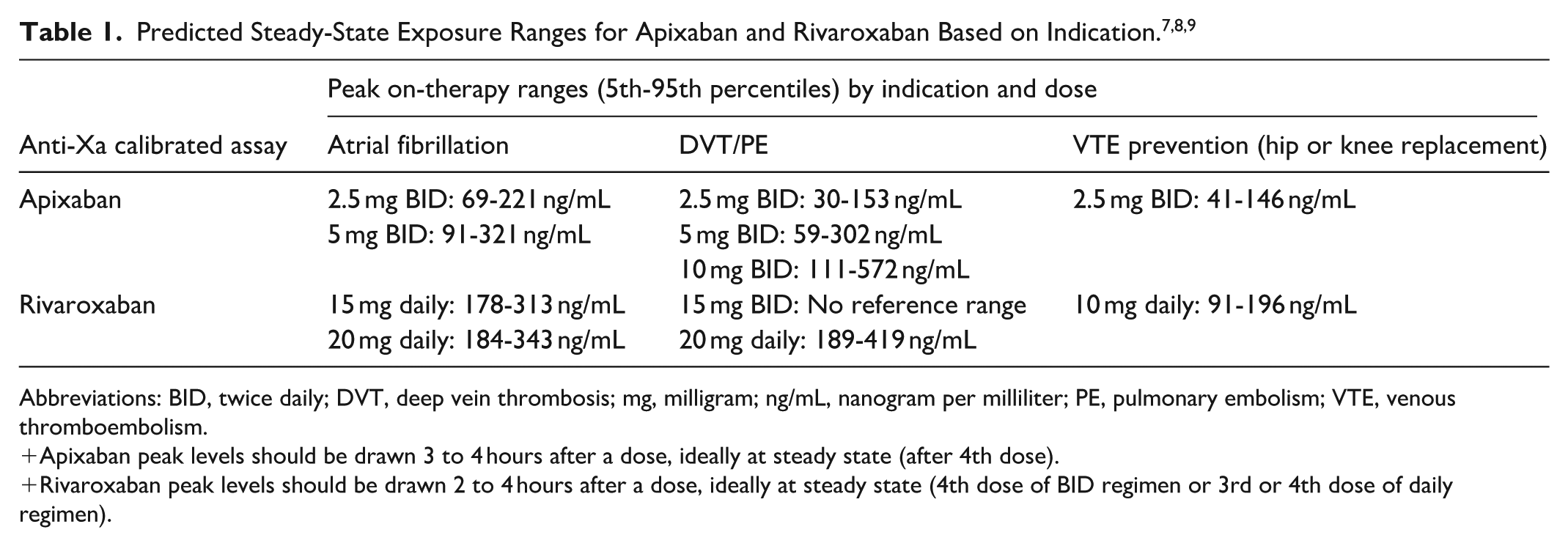
Abbreviations: BID, twice daily; DVT, deep vein thrombosis; mg, milligram; ng/mL, nanogram per milliliter; PE, pulmonary embolism; VTE, venous thromboembolism.
Apixaban peak levels should be drawn 3 to 4 hours after a dose, ideally at steady state (after 4th dose).
Rivaroxaban peak levels should be drawn 2 to 4 hours after a dose, ideally at steady state (4th dose of BID regimen or 3rd or 4th dose of daily regimen).
Hepatic dysfunction was defined as elevated liver function tests greater than three times the upper limit of normal. History of hepatic dysfunction was defined as a chronic diagnosis of hepatic cirrhosis or alcoholic cirrhosis per ICD-10 codes. Renal dysfunction was defined as creatinine clearance less than 30 mL/min calculated using the Cockcroft Gault equation or documented dependence on dialysis. 10
Patient characteristics and clinical decisions regarding reasons for ordering a level and actions following a level were obtained through chart review by one investigator (BM) and audited by another (JO). Patients with multiple levels obtained during a single encounter were all included in the final analysis. Continuous data from baseline characteristics are presented as median and interquartile ranges (IQRs).
Results
During the study period, 132 anti-Xa levels for apixaban and rivaroxaban met the inclusion criteria, representing a level drawn in 0.48% of all apixaban and rivaroxaban orders. There were 101 patients, and 31 levels were multiples for patients. Twenty of the patients had at least one repeat level. There were four patients who had a repeat level after a dose adjustment and the action for the repeat levels was no change. Baseline characteristics (Table 2) show most patients were female (58%) and many had a body mass index (BMI) above 30 kg/m2 (46.2%) (Figure 1).
Baseline Characteristics of Patients (n = 101) for Each Apixaban or Rivaroxaban Level.
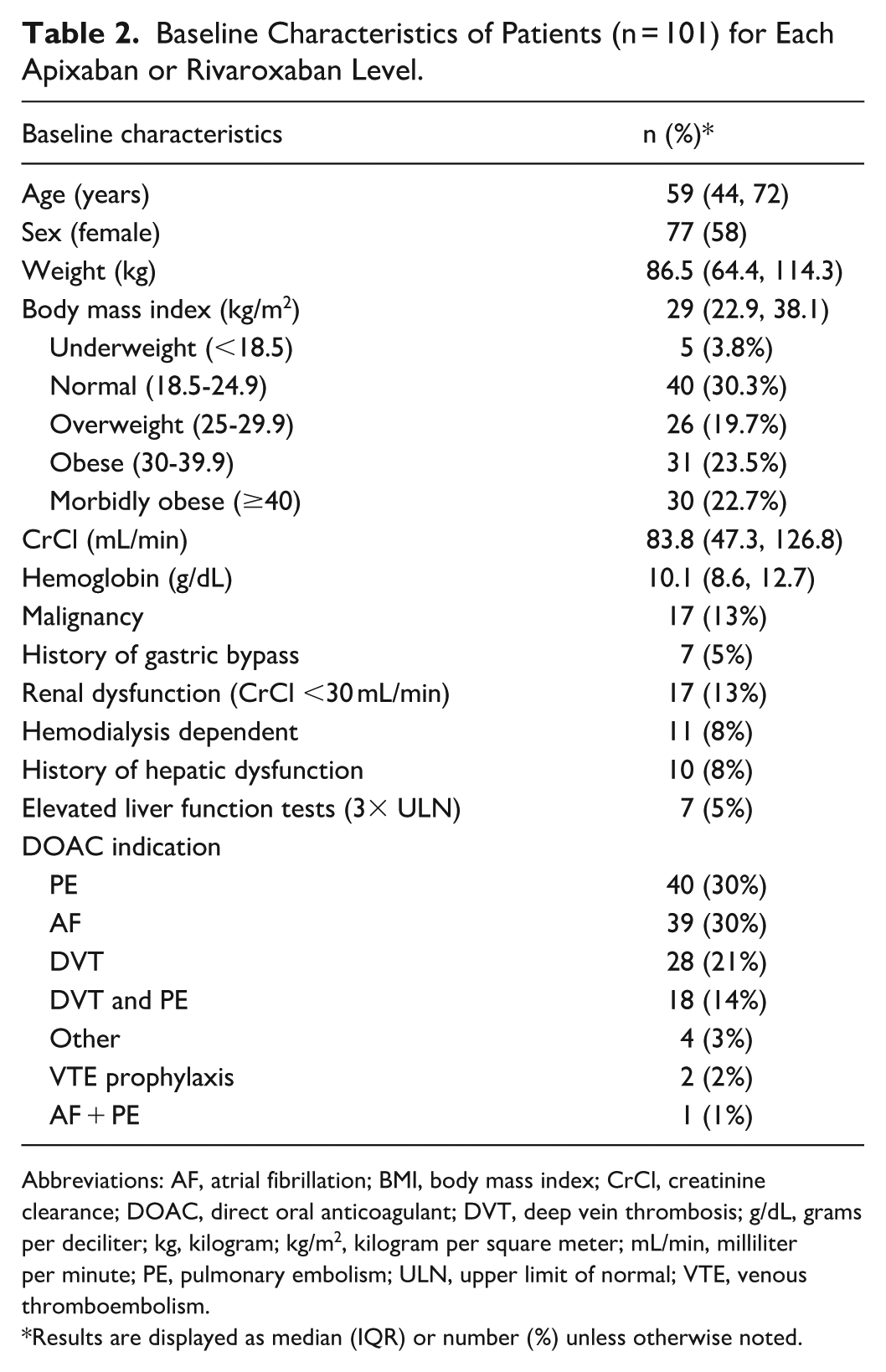
Abbreviations: AF, atrial fibrillation; BMI, body mass index; CrCl, creatinine clearance; DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; g/dL, grams per deciliter; kg, kilogram; kg/m2, kilogram per square meter; mL/min, milliliter per minute; PE, pulmonary embolism; ULN, upper limit of normal; VTE, venous thromboembolism.
Results are displayed as median (IQR) or number (%) unless otherwise noted.
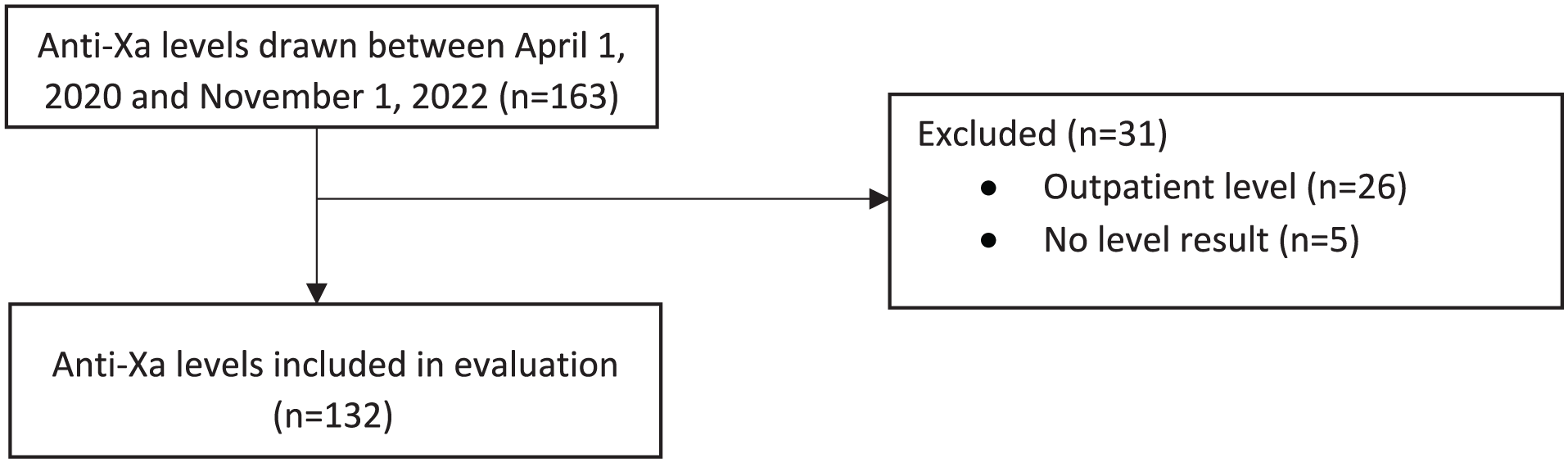
Flow diagram for anti-Xa level inclusion in final analysis.
Rivaroxaban accounted for 49 (37%) of the levels, and apixaban 83 (63%) levels. Indications for ordering anti-Xa levels for apixaban and rivaroxaban varied among all defined categories (Figure 2). One third of the levels (43, 33%) were drawn in patients with multiple reasons for obtaining a level, all reasons were counted in the final analysis. The most common indication for obtaining a level was extreme body weight. Of the 46 levels associated with extreme body weight, 34 (74%) were for patients with either a BMI over 40 kg/m2 or a bodyweight over 120 kg. The 12 other levels were obtained in patients with either a BMI less than 18 kg/m2 or a bodyweight less than 50 kg. Of the peak levels in patients with an extreme weight (14), most (78.6%) had no change in treatment following the level. There were two dose adjustments and one anticoagulation agent change.
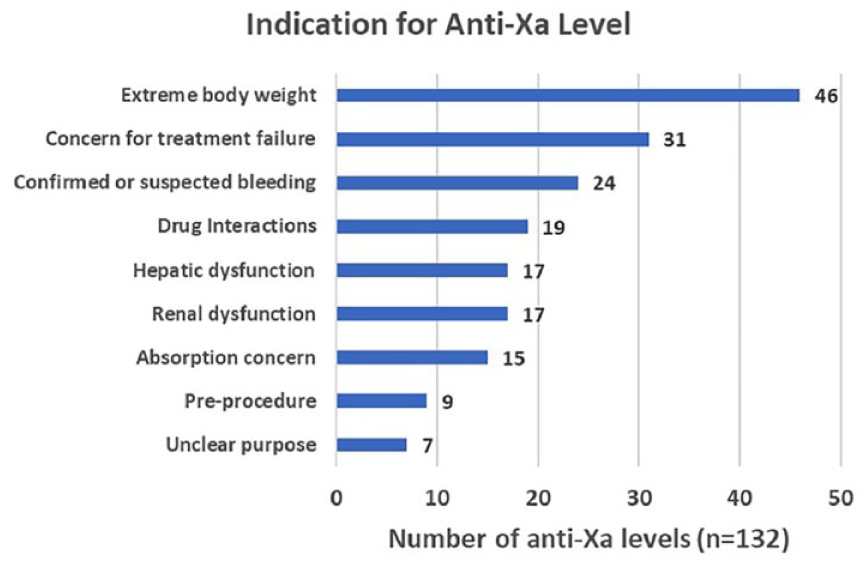
Indications for ordering an anti-Xa level.
Excluding pre-procedure levels timed as troughs, 41 (33.3%) levels were timed as a peak, 60 (48.8%) were not timed for a peak and considered random, and 22 (17.9%) levels had unknown timing based on no documented last dose time. Most of the levels were determined to be outside of the on-therapy range (defined in Table 1) with 20 levels (15.2%) above the goal range and 58 levels (43.9%) below the on-therapy range (Table 3). Half of the levels above goal range did not result in any change in anticoagulation, whereas four levels (20%) led to dose reductions and four (20%) resulted in a change in anticoagulant agent. Of the levels that were within goal range, most (70%) had no change in dose or therapy after the level.
Results.
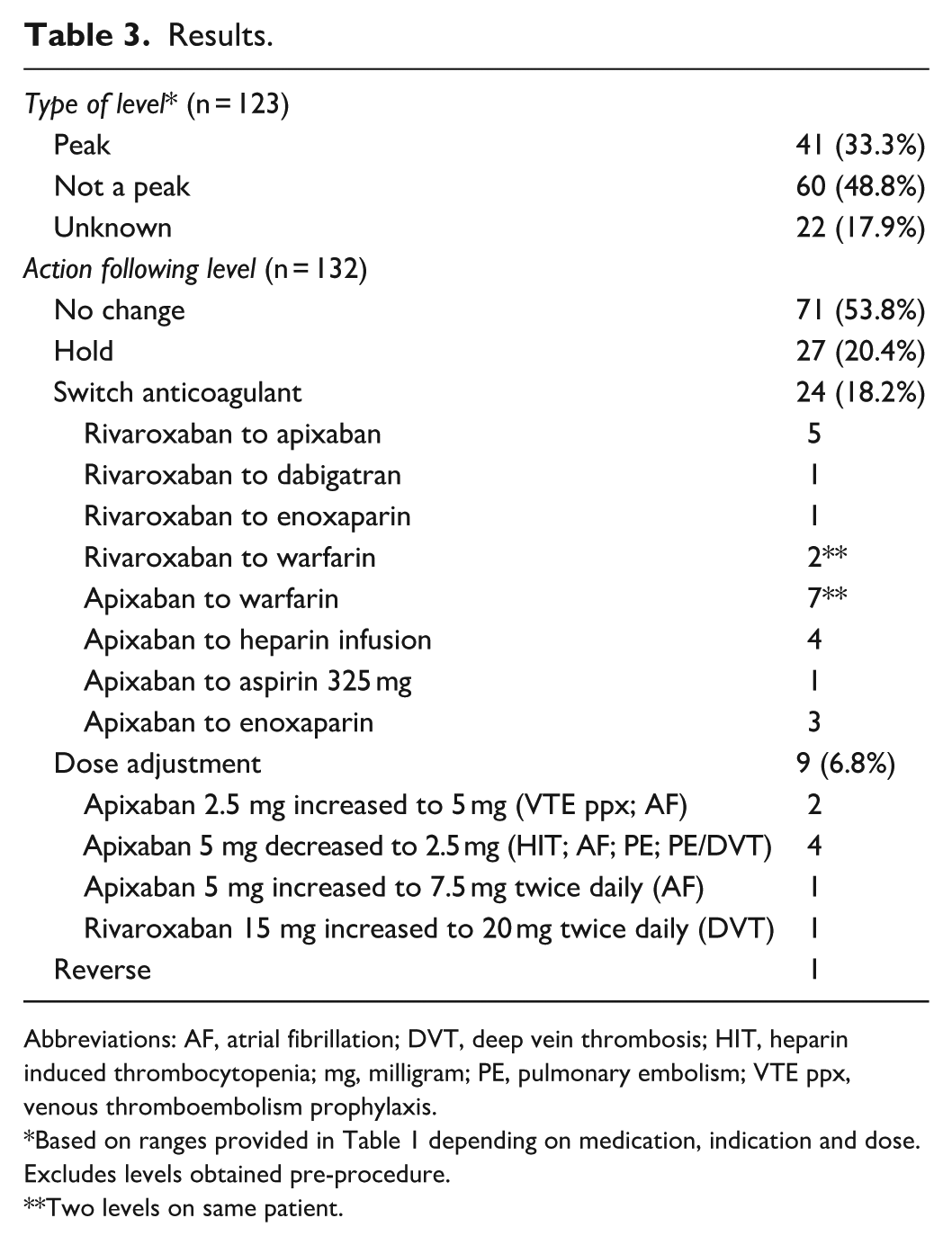
Abbreviations: AF, atrial fibrillation; DVT, deep vein thrombosis; HIT, heparin induced thrombocytopenia; mg, milligram; PE, pulmonary embolism; VTE ppx, venous thromboembolism prophylaxis.
Based on ranges provided in Table 1 depending on medication, indication and dose. Excludes levels obtained pre-procedure.
Two levels on same patient.
More than half of all levels, regardless of timing relative to last DOAC dose, resulted in no change to the anticoagulation therapy plan (Table 3). The second most common action was to hold therapy (20.4%) followed by switch to alternative anticoagulant (18.2%).
Sixty-nine of the levels (52%) were affiliated with a hematology consult. The ordering user was most commonly the primary team provider (67%), followed by pharmacists (25%), hematology providers (8%), and emergency department providers (8%).
When examining only true peak levels (41), many levels were within goal range (41%) (Table 4). The median peak level for apixaban was 153.5 ng/mL and the median peak level for rivaroxaban was 268 ng/mL. The average peak apixaban level was 217.6 ng/mL and rivaroxaban was 278.4 ng/mL. There were 11 levels (27%) above goal range which influenced a dose change in four cases, anticoagulant change in one case, and no change in six cases (54.5%). Eight levels were below goal range which led to no change in three cases, anticoagulant change in three cases, a dose change in one case, and one repeat level. The percentage of labs ordered and drawn as peak levels varied by ordering provider. True peaks were only drawn 19.2% of the time (19/99) when ordered by the primary team provider, 18.2% (2/11) when ordered by a hematology provider, and 60.6% of the time (20/33) when ordered by a pharmacist.
Peak Level Interpretation Based on Medication, Dose, and Indication for Reference Ranges.
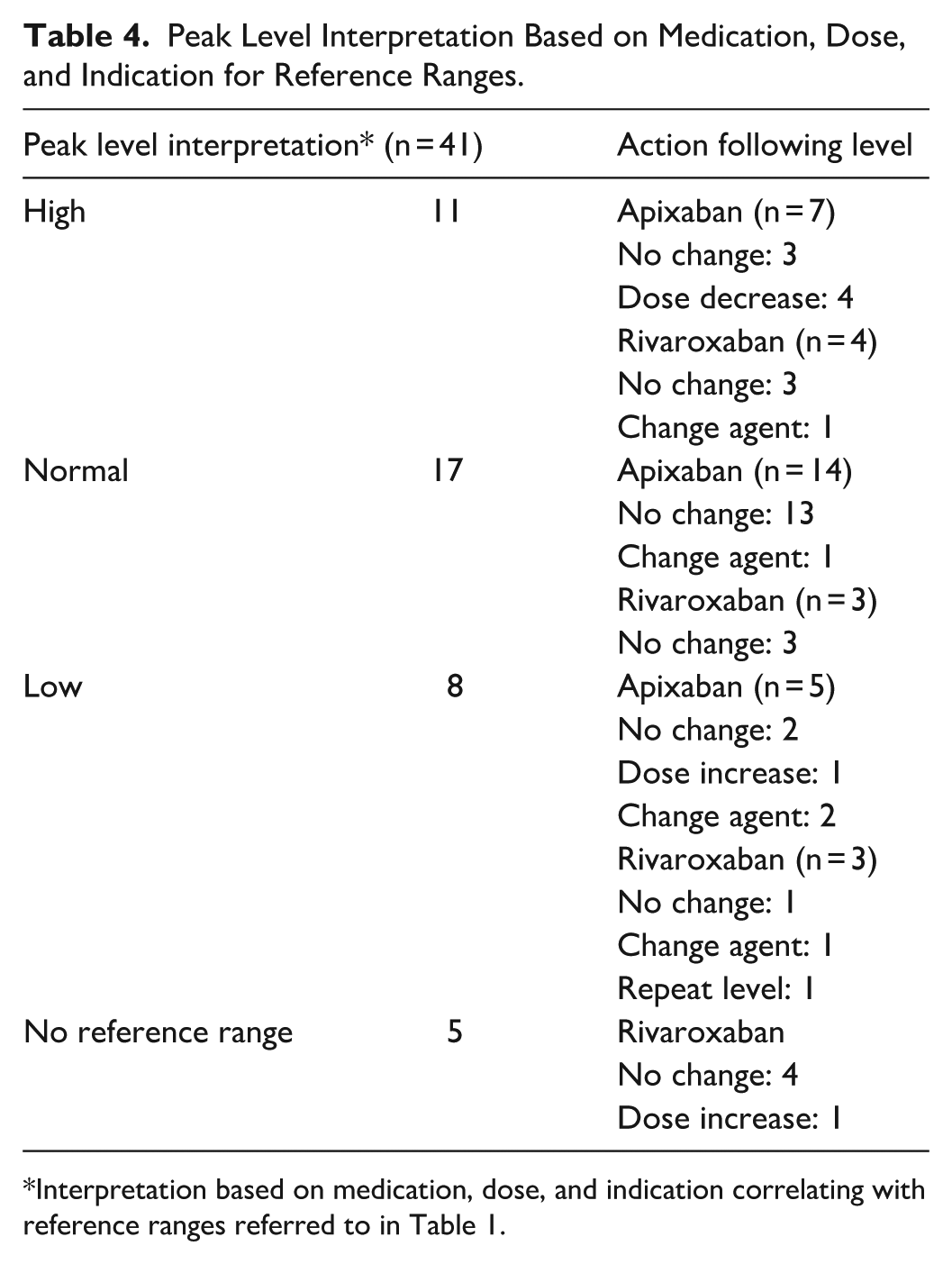
Interpretation based on medication, dose, and indication correlating with reference ranges referred to in Table 1.
When comparing the baseline characteristics of the high peak group (n = 11) to the normal/low level group (n = 25), the patients with high on-therapy peak levels were more likely to have a drug interaction (5/11 (45.5%) vs 4/25 (16%)) but less likely to have absorption concerns (4/11 (36.4%) vs 12/25 (48%)), extreme body weight (3/11 (27.3%) vs 11/25 (44%)), or concern for thrombosis (0% vs 24%). All other variables showed no difference between the groups, particularly bleeding events (0 vs 1/25 (4%)), renal function with CrCl <30 mL/min or on dialysis (1/11 vs 2/25), or hepatic dysfunction (1/11 (9%) vs 2/25 (8%)).
Of the 22 levels obtained that were associated with drug interactions, azole antifungals were a key driver in prompting levels (Table 5). There were eight levels associated with posaconazole, two levels with voriconazole, three with isavuconazole, and two with fluconazole. The other key interacting agent was rifampin which was associated with three levels. Only half of these levels were appropriately timed for peak levels, with five (45%) of these levels above on-therapy range. All five levels above on-therapy range were associated with azole antifungal agents. There was one level below on-therapy range due to rifampin (Figure 3).
Drug Interactions.
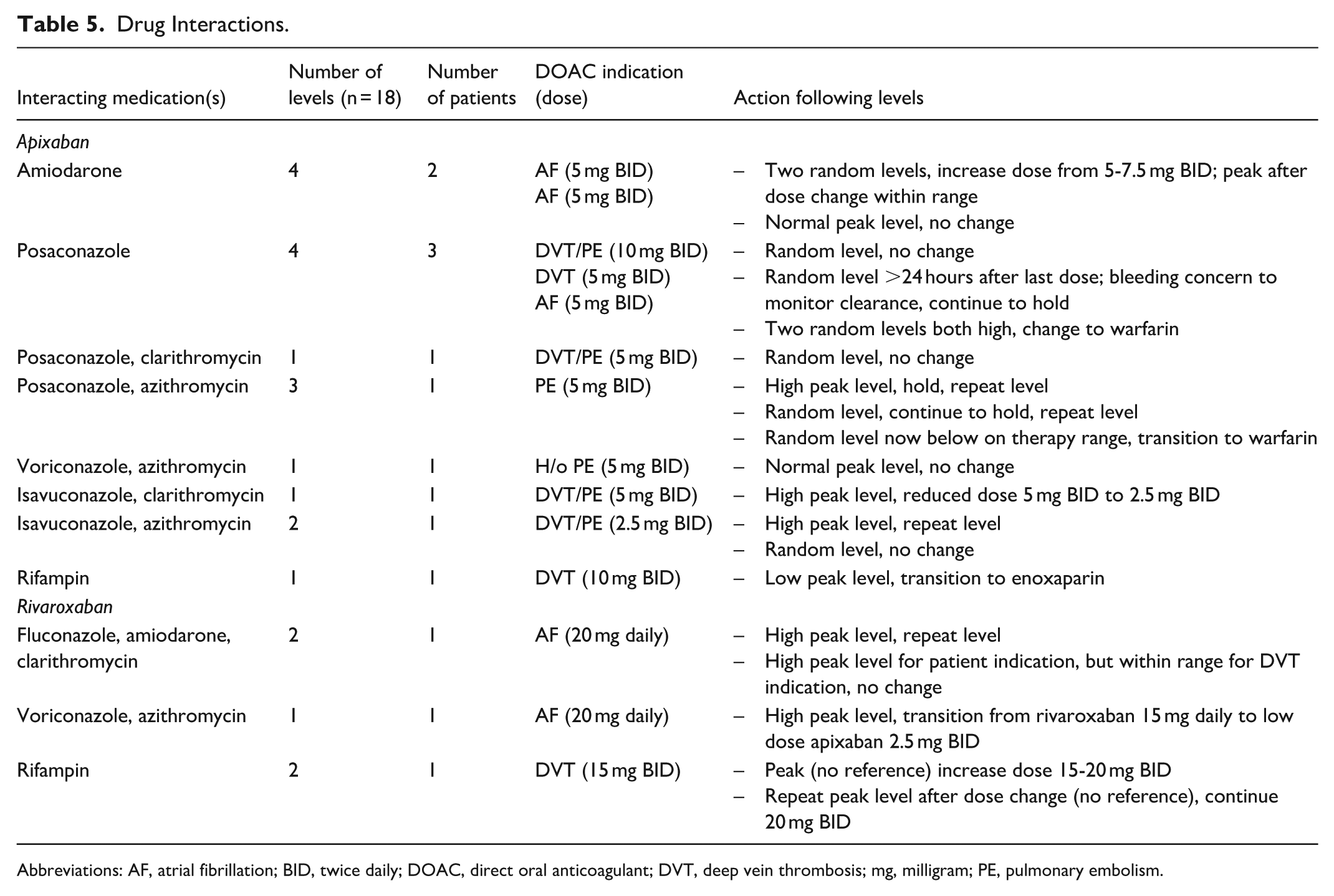
Abbreviations: AF, atrial fibrillation; BID, twice daily; DOAC, direct oral anticoagulant; DVT, deep vein thrombosis; mg, milligram; PE, pulmonary embolism.
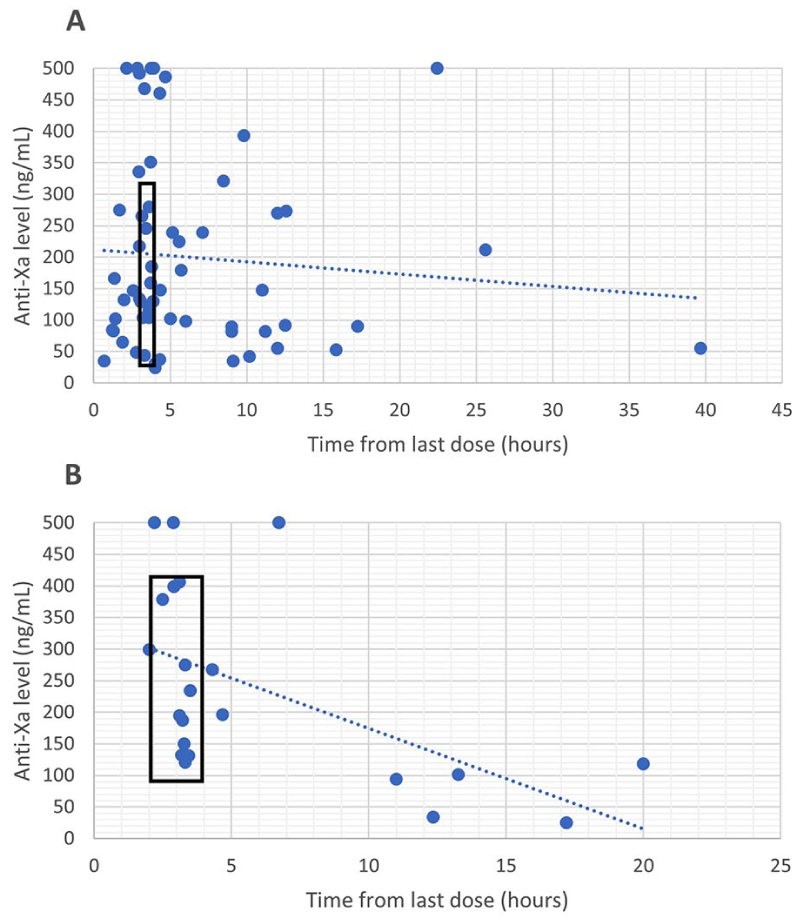
Anti-Xa levels after a documented dose of apixaban (A) and rivaroxaban (B).
Discussion
In this single health system, retrospective study, apixaban and rivaroxaban calibrated anti-Xa levels were drawn infrequently with an incidence of 0.48% for all apixaban and rivaroxaban inpatient orders. Anti-Xa levels were often drawn at inappropriate times relative to the last medication dose with only 33% of levels drawn as peaks, which complicates their interpretation. Most levels (53%) did not influence a change in the anticoagulation therapy plan. Of the peak levels that were within the reference range, no change was made in 94% of cases which is consistent with standard therapeutic drug monitoring practices.
As mentioned previously, a peak DOAC concentration is preferred to allow for optimal interpretation of the result. Only 33% of levels were appropriately drawn as peaks, making the interpretation of the level difficult in almost two of three cases. No previous literature has discussed the accuracy of sample timing for therapeutic drug monitoring when comparing pharmacists to other providers. Of the total 132 levels, 49% were drawn as peaks when ordered by a pharmacist compared to 46% when ordered by the primary care team versus 2% by hematology providers. There were 12 levels that were repeated in our study for various patients due to inappropriate timing of the initial level, adding unnecessary cost and wasting resources. Studies have shown that pharmacists contribute to reductions in cost in various healthcare settings. 11 This would be another opportunity to minimize healthcare waste by utilizing pharmacists to appropriately time levels for drug monitoring.
The most common reasons for obtaining an anti-Xa level in our study were extreme body weight, concern for treatment failure, and confirmed or suspected bleeding. One study compared patients with a major bleeding event compared to those without a major bleeding event and found median apixaban and rivaroxaban levels were similar between groups. Factors that were associated with an increased risk for major bleeding were age of 80 years or greater for apixaban, and inappropriately high dosing regimen with anti-Xa level of 100 to 300 ng/mL for rivaroxaban. 12 Despite great concern for out-of-range levels in patients with extreme body weights, most of the appropriately timed peak levels were within the on-therapy goal ranges resulting in no treatment changes. We have further recommended that routine monitoring of DOAC levels in patients with elevated BMI alone on apixaban or rivaroxaban is not necessary. Another study shares our finding that out of range levels oftentimes do not result in a change in therapy. 13
Our study did find a trend in azole antifungal agents contributing to higher DOAC concentrations and rifampin with lower DOAC concentrations. The concomitant use of azole antifungals and rifampin with DOACs could theoretically raise or reduce DOAC concentrations, respectively, through CYP3A4 inhibition and induction. The package insert for apixaban states that concomitant use of specific azoles (ketoconazole, itraconazole, voriconazole, and posaconazole) is not recommended, but the interaction is less significant with fluconazole and other moderate CYP3A4 inhibitors. 8 The rivaroxaban package insert specifies the interaction with fluconazole is not clinically relevant, but other azoles (specifically ketoconazole) should have routine pharmacovigilance activities, but no specific recommendations. 14 In a 2022 study, azole antifungal use in patients taking apixaban and rivaroxaban showed significant interactions with ketoconazole, but suggest that relevant interactions can only be achieved if multiple elimination pathways are modified, and one of them is intestinal Pgp/BCRP. 15 In general, adjusting DOAC doses based on DOAC concentrations is not recommended due to insufficient evidence-based data, however, concentrations may be warranted if the results contribute to the decision of whether to change therapy. 5 One study found a significant increase in bleeding risk when patient took fluconazole while on apixaban for atrial fibrillation. No increased bleeding risk was found when patients were on fluconazole and rivaroxaban. 16
This study has several limitations to consider. There are inherent limitations associated with a retrospective, chart review study design. This was a single health system study with a small sample size, however, it is one of the largest reviews of DOAC levels in the acute care setting. Identifying the reason for ordering a level was often challenging to determine, as it is not always clearly documented in the medical record. The last DOAC dose was not always documented (especially if taken prior to admission), thus some of the levels we labeled as “unknown” could have been peak level. This also made us unable to determine clinical significance of the level. Given our health system does not have a standard in place for which clinical scenarios to draw DOAC levels, we were unable to determine how many patients were taking apixaban or rivaroxaban that may have been indicated for a level but didn’t have one obtained. The decision to obtain anti-Xa levels was provider dependent and it is possible that routine anti-Xa testing in unselected patients may yield different results. We were also unable to determine how many patients on apixaban or rivaroxaban may have had a less specific lab drawn, such as a heparin anti-Xa level, to glean information about the patient’s level of anticoagulation without specifically checking a DOAC specific concentration. The reportable range for apixaban and rivaroxaban on our institutions anti-Xa assay is 23 to 500 ng/mL and 25 to 500 ng/mL, respectively. Levels above these ranges may be underestimated compared to the full exposure of the DOAC. Finally, we did not follow the patients longitudinally to evaluate clinical outcomes associated with the levels and would be a potential niche for future research.
Conclusion
Calibrated anti-Xa levels for apixaban and rivaroxaban were often not drawn appropriately, and in most patients, the pharmacotherapy plan did not change. Future research is needed to determine if DOAC concentrations may be clinically meaningful in a select subgroup of patients.
Footnotes
Ethical Considerations
Ethical approval for this study was obtained from University of Minnesota Institutional Review Board (IRB; STUDY00017547) on November 18th, 2022.
Author Contributions
B.M. completed data collection, analysis, and initial manuscript writing. J.O. conceived project idea, contributed to the design and analysis of the results. Both authors discussed the results and contributed to the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.