
Abstract
Purpose:
Bacterial exotoxins play a crucial role in the pathogenicity of necrotizing skin and soft tissue infections (NSTI). Clindamycin has historically been utilized as an adjunctive antitoxin in empiric therapy along with broad-spectrum antibiotics, commonly vancomycin. However, due to toxicity concerns associated with this combination, and the similar mechanism of action, linezolid’s role as a toxin suppressing agent has gained interest in recent years. The objective of this study was to assess the safety and efficacy of linezolid versus adjunctive clindamycin in the empiric treatment of NSTI.
Methods:
This multicenter retrospective cohort study included 144 adults admitted from April 2022 to December 2024 with a diagnosis of NSTI who received either linezolid or adjunctive clindamycin for at least 48 hours. The primary outcome was 30-day mortality. Secondary outcomes measured 60- and 90-day mortality, as well as hospital readmission, infection recurrence, and incidence of acute kidney injury (AKI), Clostridioides difficile infection (CDI), suspected serotonin syndrome, and new onset of thrombocytopenia.
Results:
There were no patients in the linezolid cohort that met the primary outcome (0% vs 4.4%; P = .12). The incidence of AKI was significantly higher among patients treated with adjunctive clindamycin (9.4% vs 33.0%; P = .001).
Conclusion:
There were no differences in mortality, hospital readmission, or infection recurrence between the linezolid and adjunctive clindamycin cohorts. The lower incidence of AKI observed in patients treated with linezolid suggests it may be considered a reasonable antitoxin alternative to adjunctive clindamycin in the empiric treatment of NSTI.
Keywords
Background
Necrotizing skin and soft tissue infections (NSTI) are associated with bacterial toxin penetration into endothelial cell structures leading to tissue injury and vascular damage. Rapid progression of the infection triggers a hyperactive immune response, which may result in multiorgan failure and lead to mortality.1,2 The reported global mortality rate of 23.1% is reflective of the high acuity of illness and poor patient outcomes NSTI may be associated with.2,3
A variety of bacterial organisms have been implicated in the etiology of NSTI, ranging from polymicrobial to monomicrobial infections. Toxin-producing organisms such as Staphylococcus aureus (including methicillin-resistant Staphylococcus aureus [MRSA]), Streptococcus pyogenes, and Clostridium species have been identified among clinically significant cases. 4 As pathogenicity is correlated with toxin production, protein synthesis inhibiting antibiotics are considered a mainstay in empiric therapy. This is illustrated by the 2014 Infectious Disease Society of America (IDSA) guidelines, which recommend the addition of a toxin-suppressing agent, such as clindamycin, when streptococcal and clostridial species are the suspected causative organisms of infection. 5 There is additional literature suggesting benefits in utilizing a protein synthesis inhibitor, or antitoxin, for other Gram-positive organisms including staphylococcal species. 6 A joint statement provided in 2022 by global emergency medicine, infectious diseases, and surgical societies also endorsed the use of an antitoxin antibiotic in empiric NSTI treatment. 7
Clindamycin has traditionally assumed the role of an antitoxin agent in clinical treatment regimens due to its mechanism of binding to 50S bacterial ribosomal subunits, disrupting peptide formation, and inhibiting bacterial protein synthesis. 8 Despite its theoretical antitoxin benefit, the use of clindamycin has been associated with the risk of clinically significant adverse drug effects. One of the associated side effects includes Clostridioides difficile infections (CDI), a serious complication that may exacerbate poor patient outcomes and lead to prolonged hospital admissions.9,10 As a result of growing global resistance of streptococci and staphylococci to clindamycin, it is necessary to include an additional anti-MRSA agent, such as vancomycin, for adequate empiric coverage.11,12 In addition to the unfavorable side effects observed with clindamycin individually, the adjunctive use of vancomycin introduces another well-established antibiotic-associated toxicity in acute kidney injury (AKI). 13
Since the approval and commercial availability of linezolid, shifts in clinical practice patterns have been observed with its inclusion in the approach to NSTI treatment. Due to the similar mechanism of action and potentially more favorable safety profile compared to adjunctive clindamycin therapy, the use of linezolid as a toxin-suppressing agent in empiric NSTI treatment has also been explored in recent retrospective studies.14,15
While linezolid has also been associated with certain adverse drug effects, the reported incidences are historically low and risk is often heightened by external factors. As linezolid acts similarly to monoamine oxidase inhibitors (MAOi), concomitant use should be avoided to mitigate the risk of serotonin syndrome. 16 Clinicians may also be hesitant to initiate linezolid in combination with other serotonergic agents, like selective serotonin reuptake inhibitors (SSRI) or serotonin and norepinephrine reuptake inhibitors (SNRI). However, studies have reported no significant difference in the incidence of serotonin syndrome with either linezolid monotherapy, or in combination with SSRI/SNRI therapy. 17
Another well documented adverse effect associated with the use of linezolid is myelosuppression, specifically thrombocytopenia. However, it has been reported that patients having platelet counts within normal limits at baseline have a lower risk of developing thrombocytopenia compared to those with an existing deficit. 18 Furthermore, clinically significant reductions in platelet count have primarily been observed with parenteral administration and long-term use, more than 14 days. 19
Although previously published literature has supported the clinical efficacy of linezolid in NSTI treatment, widespread adoption into empiric therapy may be tempered by static clinical practice habits and an absence of robust research directly comparing linezolid to adjunctive clindamycin in this disease state.
The objective of this study was to assess the safety and efficacy of linezolid versus adjunctive clindamycin in the empiric treatment of necrotizing skin and soft tissue infections.
Methods
Study Design
This was a multicenter retrospective cohort study that included 22 sites within a large community healthcare system in Florida. Adult patients admitted from April 2022 to December 2024 with a diagnosis of NSTI and initiation of empiric treatment with either linezolid or adjunctive clindamycin for at least 48 hours were assessed for inclusion. Patients were excluded from the final analysis if they received concomitant treatment with both study drugs for more than one dose, or the empiric regimen with clindamycin did not include a secondary anti-MRSA agent. This study received exemption through the institutional review board as it qualified as a quality improvement project.
Definitions
Using Kidney Disease Improving Global Outcomes (KDIGO) guidelines, AKI was defined as an increase in serum creatinine by 0.3 mg/dL or more, an increase of 1.5 times baseline serum creatinine within 48 hours, or a decrease in urine output to less than 0.5 mL/kg/hour for 6 or more hours after the first antitoxin dose. CDI was defined as a positive stool toxin nucleic acid amplification test (NAAT) on polymerase chain reaction (PCR) screening. Suspected serotonin syndrome was assessed based on provider documentation in the electronic medical record (EMR). New onset of thrombocytopenia was considered a decreased platelet count below 100,000/µL after the first antitoxin dose in patients with a baseline above this level. Hospital readmission was measured if patients presented at any site within the healthcare system for any diagnosis after the initial admission for NSTI. Infection recurrence was determined if patients were given an NSTI diagnosis on readmission. Stress-dose steroid use was classified as intravenous hydrocortisone at a daily dose of 200 mg or higher.
Outcomes
The primary outcome measured was 30-day mortality. Secondary efficacy outcomes included 60- and 90-day mortality, hospital readmission, and incidence of recurrent infection. Safety outcomes of AKI and CDI, suspected serotonin syndrome, and new onset of thrombocytopenia were also measured. Additional outcomes included the requirement of vasopressors, stress-dose steroids, or mechanical ventilation for more than 24 hours.
Statistical Analysis
Based on a historically published incidence of 30-day mortality at 8.06% in adjunctive clindamycin control groups and 6.45% with the experimental linezolid comparator, it was estimated that a total study population of 8,126 would provide the study 80% power to detect differences in the primary outcome. Dichotomous categorical data, such as primary and secondary outcome measurements, were assessed using chi-squared test. The Mann-Whitney U test was utilized to compare non-normally distributed and continuous baseline characteristic data. A logistic univariable regression analysis was conducted to assess covariate associations with the primary outcome. Patient data was processed and analyzed through the statistical analysis software JASP 0.19.3.0.
Results
A total of 249 patients were screened, with 144 meeting eligibility for inclusion in the final analysis (Figure 1).
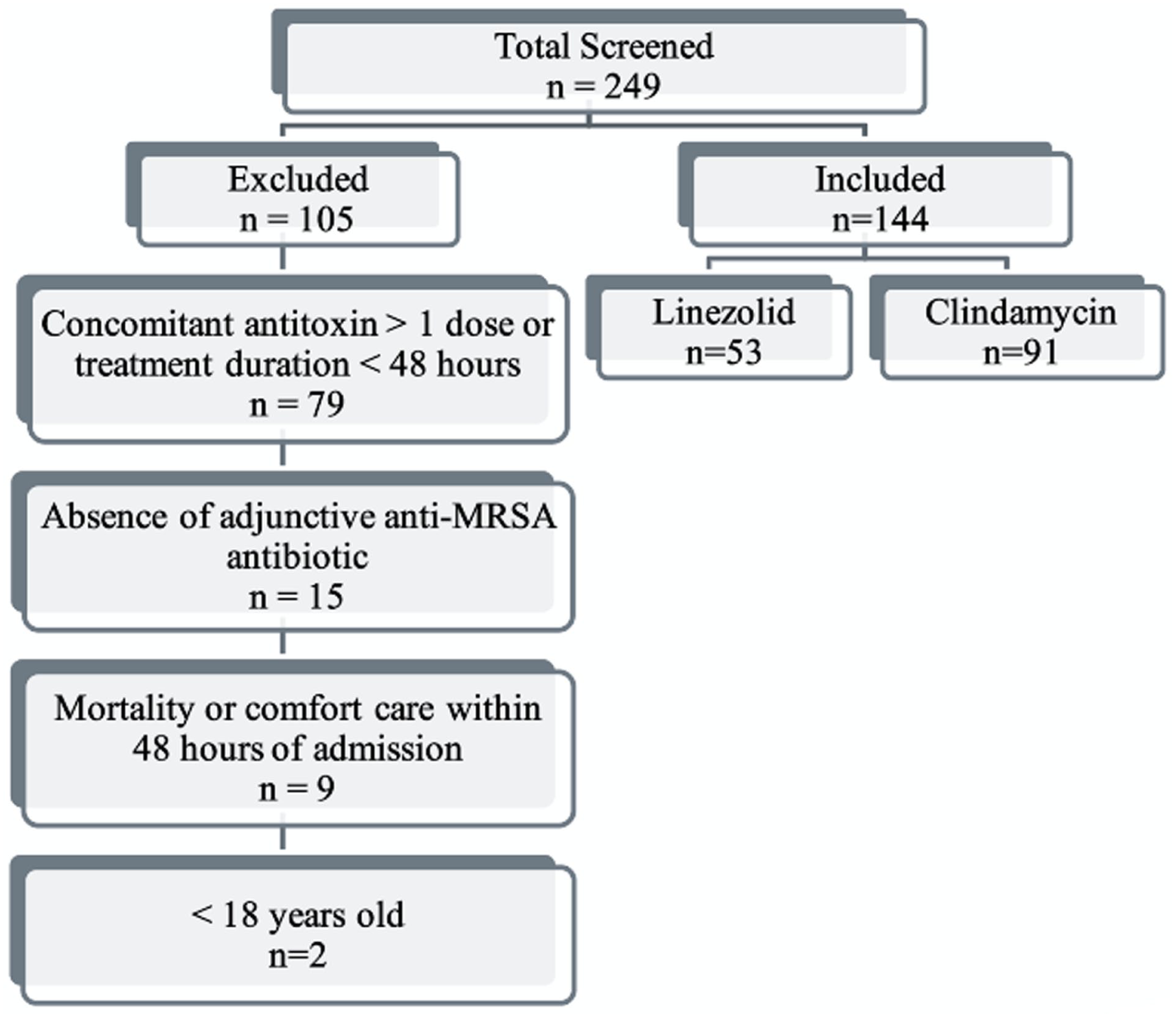
The primary reason for exclusion was due to inadequate treatment duration or overlapping use of both study agents.
Baseline characteristics were similar between both treatment groups (Table 1). An exception was the observation of prolonged time to surgical intervention in patients treated with linezolid (0.8 vs 0.4 days, P = .03). While this group also displayed a higher rate of positive blood cultures, patients in the clindamycin cohort revealed a higher incidence of wound cultures colonizing a broad range of organisms. Significantly, vancomycin was the overwhelming anti-MRSA agent of choice, used in 75.8% of patients treated with adjunctive clindamycin.
Baseline Characteristics.
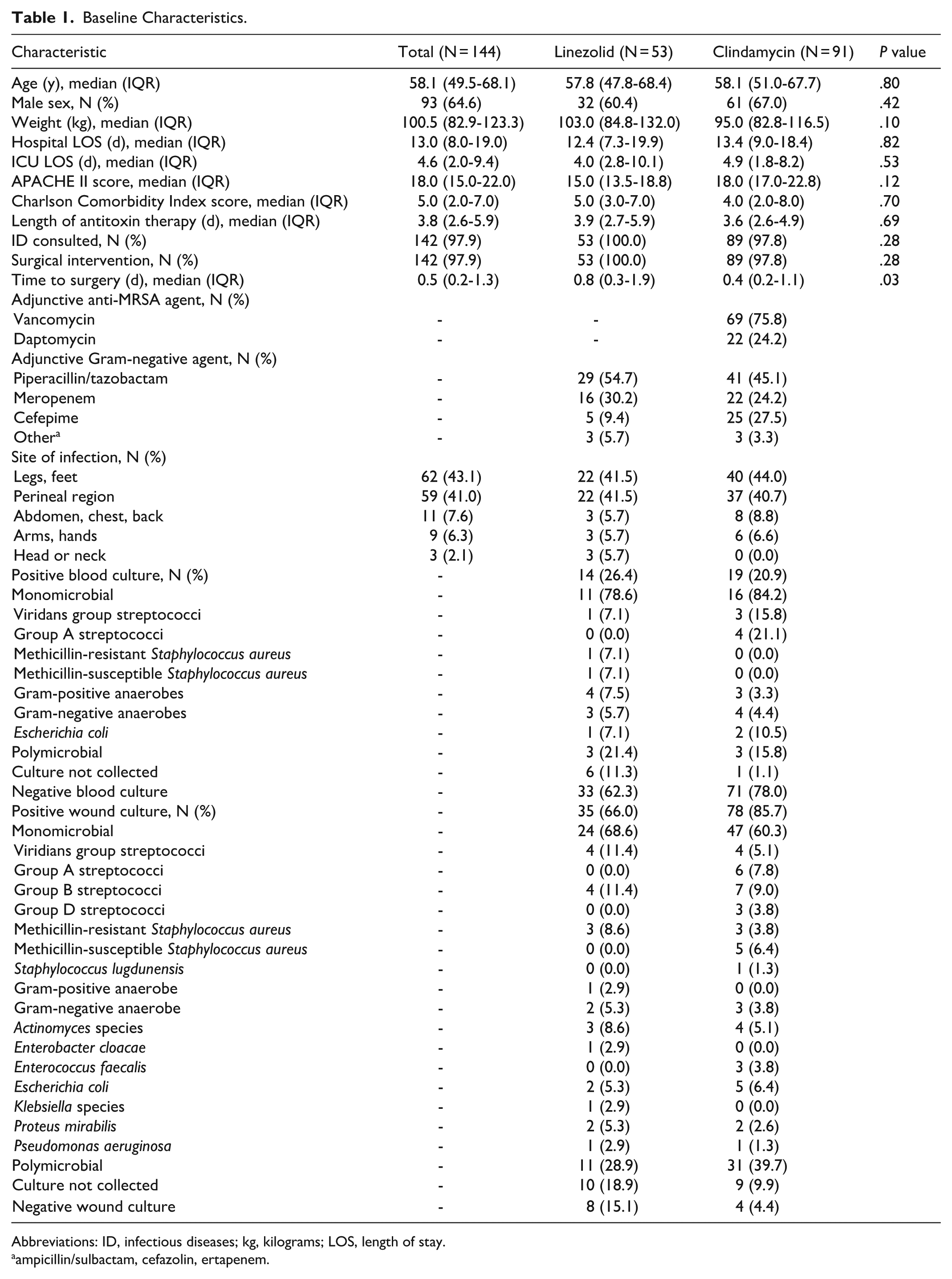
Abbreviations: ID, infectious diseases; kg, kilograms; LOS, length of stay.
ampicillin/sulbactam, cefazolin, ertapenem.
The primary outcome was not observed in any patient treated with linezolid. However, this did not result in a statistically significant difference in 30-day mortality among the treatment groups, (0/53 [0.0%] vs 4/91 [4.4%]; P = .12; Table 2). While there were no differences observed in many of the measured safety outcomes, significantly, an increased incidence of AKI emerged from the adjunctive clindamycin cohort (5/53 [9.4%] vs 30/91 [33.0%]; P = .001).
Primary and Secondary Outcomes.
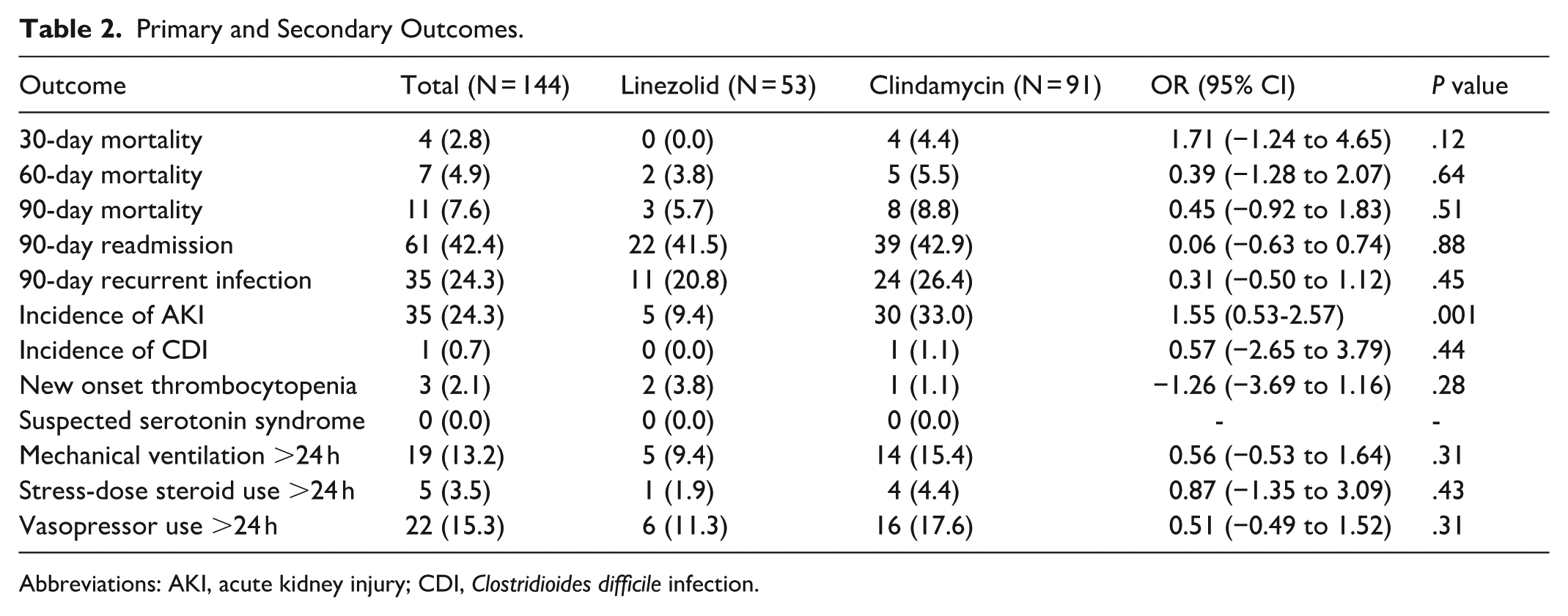
Abbreviations: AKI, acute kidney injury; CDI, Clostridioides difficile infection.
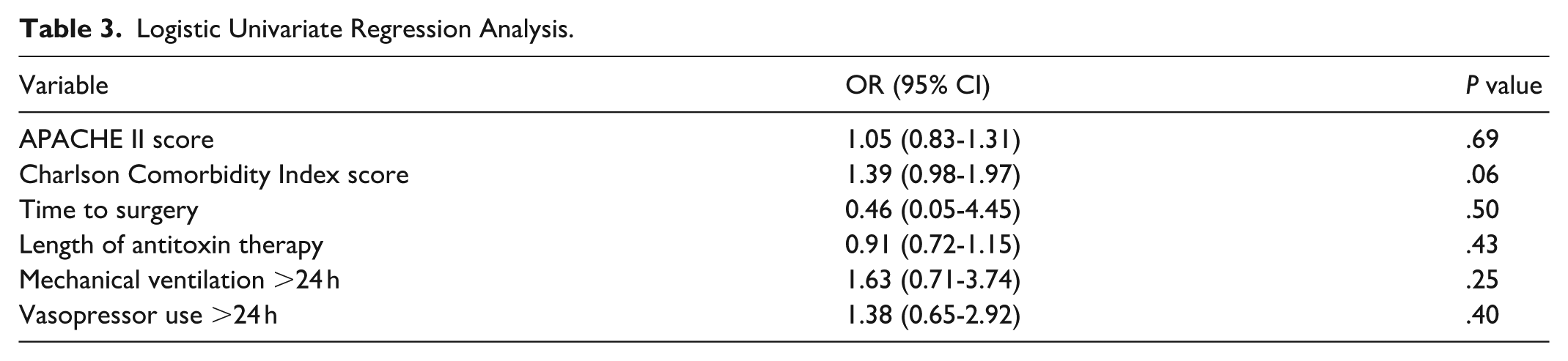
A logistic univariate regression analysis revealed that neither acuity of illness, as measured by severity scoring and use of vasopressors or mechanical ventilation, nor initial treatment approach including time to surgery and length of antitoxin duration were positive predictors of association with the primary outcome (Table 3).
Logistic Univariate Regression Analysis.
Discussion
This observational study evaluated clinical safety and efficacy outcomes associated with the use of linezolid versus adjunctive clindamycin in the treatment of necrotizing skin and soft tissue infections. A growing body of evidence supports the use of linezolid as a potentially viable alternative to clindamycin for toxin suppression in empiric NSTI treatment. Bernardo et al reported linezolid significantly suppressed virulence factor expression in S. aureus, including α- and β-hemolysins and enterotoxins, without promoting resistance. 20 Additionally, the use of linezolid in animal models with necrotizing MRSA pneumonia found that early therapy led to suppressed exotoxin production and improved survival compared to vancomycin, validating linezolid’s suggested in vivo antitoxin potential. 21
Along with in vitro and animal model studies, direct retrospective comparisons of linezolid and clindamycin in clincial settings have been conducted in recent years. In 2023, Dorazio et al documented 30-day mortality rates of 8.06% with the use of adjunctive clindamycin and 6.45% in patients treated with linezolid. Our study mirrored the numerically lower event rate of 30-day mortality observed in the linezolid treatment group. The 2023 retrospective comparison observed linezolid presented a significantly lower incidence of AKI at 1.6% versus 9.7%. 14 A parallel finding was reported by Lehman et al, where AKI was observed in up to 38.1% of surgical ICU patients treated with adjunctive clindamycin plus vancomycin, but no incidence in linezolid-treated patients. 22 Similarly, our study participants experienced significantly higher rates of AKI when treated with adjunctive clindamycin. Due to the known nephrotoxic effects of vancomycin, the difference this study observed in the incidence of AKI is likely associated with its selection as the anti-MRSA agent of choice in over 75% of patients treated with adjunctive clindamycin.
In addition to AKI, literature has reported a clinically relevant increased risk of CDI associated with the use of clindamycin as compared to other antibiotic groups. 23 Despite this, our study did not display an increased risk of CDI in patients treated with adjunctive clindamycin. However, the measurement of this outcome may have been complicated by the nature of pathogenicity of CDI and possible hospital discharge prior to infection development.
A 2023 meta-analysis revealed an incidence of linezolid-induced thrombocytopenia in up to 37% of patients. However, the review identified that this risk is augmented with older age, liver disease, and renal dysfunction, as well as prolonged treatment duration. 24 New onset of thrombocytopenia was not observed at a higher rate in this study’s linezolid cohort, possibly due to the median duration of therapy of 3.9 days and age of 57.8 years, among other patient-specific factors.
As outlined by a 2023 systematic review, a reported incidence of serotonin syndrome occurred in 0.005% of patients on linezolid monotherapy. Notably, the frequency remained below 0.1% despite concomitant use of serotonergic agents, suggesting that the interaction between linezolid and SSRI/SNRI therapy is not clinically significant. 25 The absence of outcome observed in our patients further substantiates the low risk of this complication with the use of linezolid. However, as the measurement of suspected serotonin syndrome in our study relied solely on assessing documentation of a stated diagnosis and did not capture measurements of standardized diagnostic criteria or scoring tools, this outcome reporting may reflect a risk of underestimation.
The assessment of multiple hospitals within a large community healthcare system contributed to the study’s favorable total inclusion relative to previously published retrospective comparisons. This study is further strengthened by the evaluation of numerous clinically relevant safety and efficacy outcomes.
The retrospective design of this study presents a potential for inherent bias. Based on the nature of this disease state and reported infection rate, the total sample size of this study was constrained. Both the limited sample size and event rate of the primary outcome prevented the study from meeting power to detect differences in 30-day mortality among the treatment groups. Given these limitations and absence of statistical significance observed in the incidence of the primary outcome, equivalence in efficacy cannot be demonstrated in the comparator versus control group. The mortality rate observed in this study did not align with published global incidence rates. This may be explained by a lower burden of disease, or presentation at earlier stages of progression in our patients, limiting generalizability. Additional factors that may have limited outcome incidence are the incapacity to measure adherence to oral antibiotic continuation after hospital discharge and clinical failure treated at an external healthcare system. Although the treatment groups had predominantly similar baseline characteristics, internal validity was weakened by the significant difference in the linezolid cohort’s longer time to surgery. Since early surgical intervention is a key determinant of favorable outcomes in the treatment of NSTI, this difference may have impacted the mortality data collected in the linezolid group and underestimated its apparent efficacy. While this study displayed an imbalance in treatment group sample size, the unequal inclusion may have been attributed to the absence of linezolid in institutional disease state treatment panels within the electronic ordering system.
Conclusion
In this retrospective multicenter cohort study, a lack of significant difference was observed in mortality, hospital readmission, and infection recurrence between linezolid and adjunctive clindamycin. Despite the study limitations preventing a comparison in efficacy between these two antimicrobials, the decreased incidence in AKI associated with the use of linezolid suggests it may be considered a potential antitoxin alternative to adjunctive clindamycin in the empiric treatment of NSTI. This study contributes to a limited pool of literature addressing a topic that may remain a source of clinical hesitancy, and these observations demonstrate the need for additional investigation of this relevant question in clinical care.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.