
Abstract
Purpose:
The purpose of this article is to assist the pharmacist engaged in nutrition support therapy in staying current with pertinent literature.
Methods:
A group of board-certified nutrition support pharmacists compiled a list of articles relevant to pharmacy nutrition support that were published in 2025. Citations were organized into a spreadsheet, and each author independently assessed whether the article was important to nutrition support pharmacy practice. Articles receiving affirmative votes from at least 5 of the 8 participating authors were included in the final list of key publications. Guidelines, consensus statements, and recommendation papers considered important to practice were included, but not formally ranked.
Results:
A total of 124 articles were identified; 5 from the primary literature were voted by the group as being of high importance. Nine guidelines, position, recommendation, or consensus papers were also identified. The top-ranked articles from the primary literature were summarized and a narrative regarding its implications to pharmacy nutrition support practice were provided.
Conclusion:
Pharmacists engaged in nutrition support therapy should be familiar with these publications, as they may have important implications for clinical practice.
Keywords
Introduction
Maintaining an evidence-based clinical practice requires clinicians to remain current with the continually evolving literature. For pharmacists involved in nutrition support, this process can be particularly challenging because relevant research, guidelines, and position statements are dispersed across a wide range of journals. As a result, identifying literature that may inform, reinforce, or alter clinical practice can be time-intensive for individual practitioners. For the past 11 years, our goal as clinicians working in nutrition support has been to curate and summarize key publications of relevance to pharmacists. This manuscript identifies and discusses significant articles that were published in 2025.
Methods
To support pharmacists practicing in nutrition support in remaining current with clinically relevant literature, the corresponding author (A.L.B.) invited 7 clinical pharmacists to participate in this project. All participants are board certified nutrition support pharmacists, and several hold additional board certifications including critical care, pharmacotherapy, and pediatrics. The participants represent a wide range of professional experience, with individual clinical practice spanning from 11 years to more than 40 years following completion of postgraduate training. Members of this authorship group have advanced practice roles with direct patient care responsibilities for prescribing parenteral nutrition (PN) and/or enteral nutrition (EN), laboratory analysis, and pharmacotherapy integrated with nutrition therapy (eg, fluid and electrolytes, vitamins, trace elements, prokinetic drugs, insulin, antidiarrheal, and laxative therapy). Some members also hold administrative or supervisory responsibilities related to nutrition support services. Collectively, this authorship group represents diverse practice settings and patient populations. Most authors are acute care-based, but some have experience with long-term care (home PN and EN). Clinical practice among the authors spans the continuum of care from pediatrics to geriatrics, with some members managing broad patient populations and others focusing on specialized populations (eg, oncology, trauma).
The approach used to identify and prioritize articles was adapted from methodology originally developed by Dr Roland N. Dickerson, who led this effort through 2024. 1 A modified Delphi process was used to identify articles published from January 2025 to December 2025 that were considered important for clinical nutrition support practice. Potential articles were identified through several methods. Some authors collected articles through personal journal subscriptions, organizational membership newsletters, or institutional-based journal clubs, while others identified articles through online literature searches. This methodology has the limitation of not using a standardized, structured literature search strategy. As a result, relevant articles pertaining to pharmacy nutrition support practice, particularly those published in less commonly reviewed journals, may not have been identified.
Only articles that had appeared in final print format during the review period were considered eligible for evaluation. Publications available only as electronic preprints, including those expected to appear in print in 2026, were excluded. Citations of candidate articles were compiled into a spreadsheet, and each participating author was asked to evaluate whether the article was important to pharmacy nutrition support practice. An abstract and complete citation of each paper was provided along with the electronic scoring spreadsheet to assist the author participants with the evaluation process.
To ensure an independent voting process without influence from the other participant members, only the corresponding author was aware of the others’ rankings. To prevent influence from the other authors on the corresponding author, dichotomous grading by the corresponding author was completed prior to review of the results from the other contributors. Votes from all participants were then tallied. Articles receiving affirmative votes from at least 5 of the 8 participants were considered highly relevant and were included in the final culled list of key publications.
Results
A total of 124 articles were collated for initial evaluation by the author group. Nine articles comprising guidelines, consensus, recommendation, and position papers were excluded from the ranking process.2-10 An average of 18 articles (range: 13-28) from the primary literature were denoted as important by individual members of the author group. Five articles receiving 5 or more votes were collectively identified as the most important by the author group.11-15 Results from the sorting process are depicted in Figure 1.
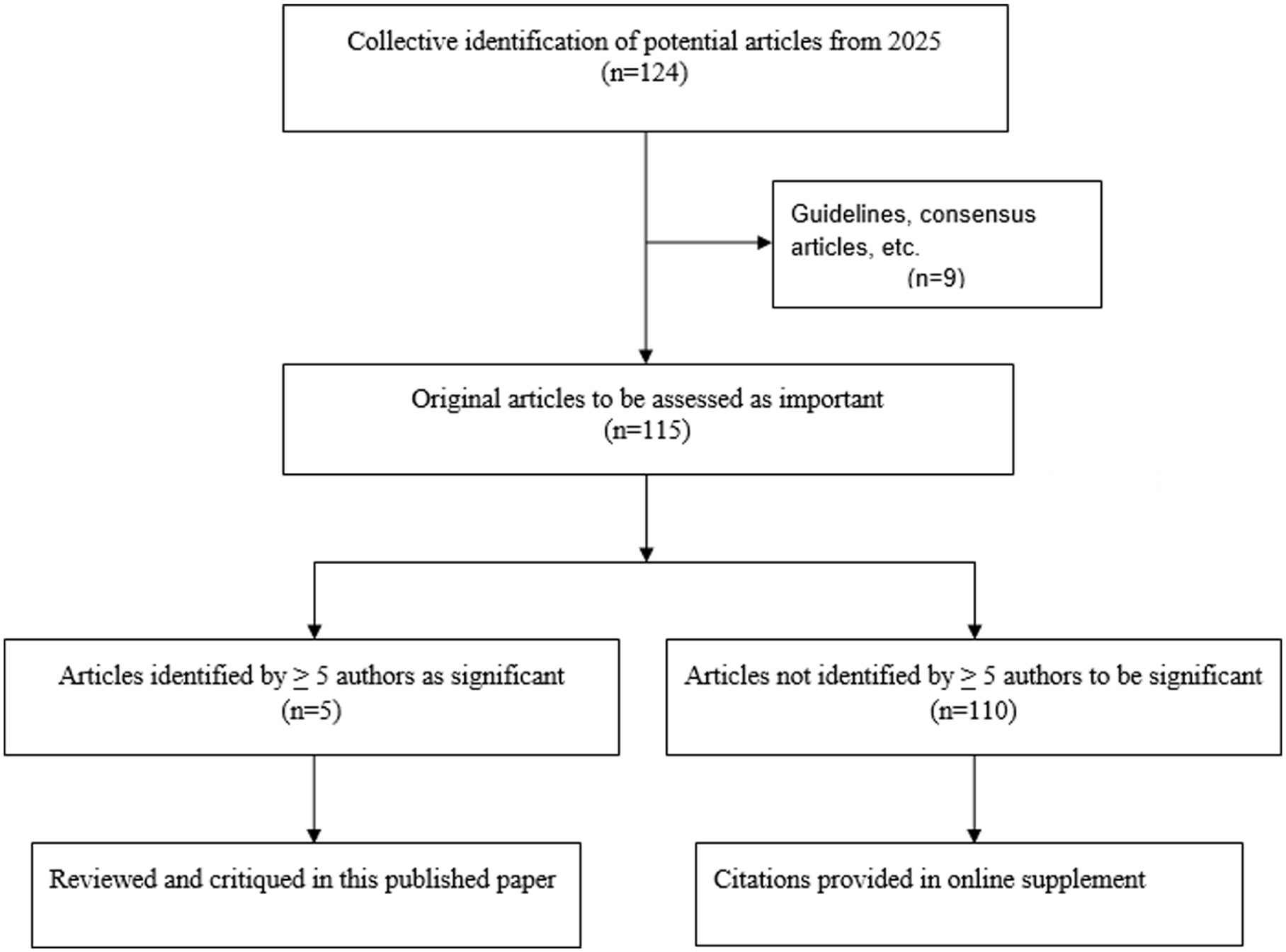
Flow diagram of identification and sorting of significant articles published in 2025 for nutrition support pharmacy practice.
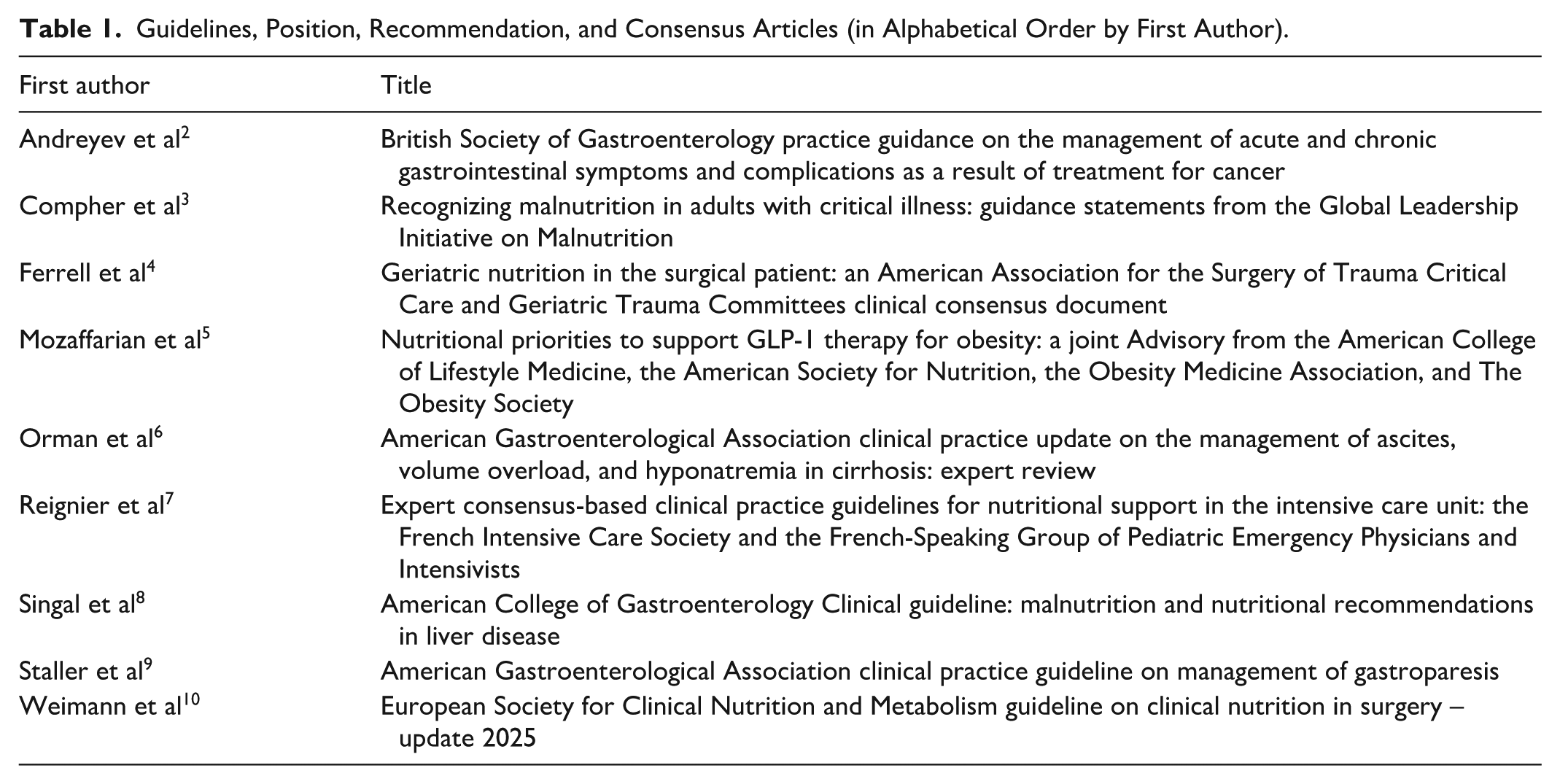
Of the 14 total primary literature and guidelines/consensus articles, 2 were published in Gastroenterology, 2 in the Journal of Parenteral and Enteral Nutrition, and 10 articles from other journals. The final publications from the primary literature are summarized in the discussion along with a narrative regarding their implications for pharmacy nutrition support practice. A list of guidelines, position statements, recommendations, and consensus articles are provided in Table 1. The remaining 110 citations from the primary literature not making the final selection are provided in the Supplemental Material.
Guidelines, Position, Recommendation, and Consensus Articles (in Alphabetical Order by First Author).
Discussion
The 5 finalist articles, listed in alphabetical order by the first author, are summarized and critiqued below.
Correction Rates and Clinical Outcomes in Hospitalized Adults With Severe Hyponatremia: A Systematic Review and Meta-Analysis
Severe hyponatremia, defined as a serum sodium concentration of 120 mEq/L or lower, occurs in ~1% of hospitalized patients. Prior treatment guidelines have recommended limiting the sodium correction rate during the first 24 hours to reduce the risk of osmotic demyelination syndrome (ODS). 16 Ayus et al conducted a systematic review and meta-analysis of studies published between 2013 and 2023 to evaluate the association between sodium correction rates and mortality in adults with hyponatremia, including patients with serum sodium <125 mEq/L and severe symptoms. 11 In this meta-analysis, 24-hour sodium correction rates were categorized as rapid (defined as ≥8 and <12 mEq/L), slow (<8 or 6-10 mEq/L), and very slow (<4-6 mEq/L). They identified 16 cohort studies, most of which were retrospective and 2 of which were prospective, including 11 811 patients with an average age of 68.2 years, 57% of whom were female. The primary outcome showed higher adjusted in-hospital mortality with slow (3.2%) or very slow (22.1%) sodium correction when compared with rapid correction. Similarly, the 30-day mortality rate was greater for slow (6.2%) or very slow (13.4%) sodium correction when compared with rapid correction. Rates of ODS were low across all groups and did not differ significantly, occurring in 0.04% of patients with very slow correction, 0.2% with slow correction, and 0.5% with rapid sodium correction. Rapid sodium correction was also associated with shorter hospital length of stay, reducing stay by 1.2 days compared with slow correction and by 3.09 days compared with very slow correction.
The results of this meta-analysis differ from prior expert guideline recommendations that favor slower correction of severe hyponatremia, suggesting that more rapid correction may be associated with improved patient outcomes.11,16 Key limitations include the authors’ inability to classify patients as experiencing acute or chronic hyponatremia and the very low incidence of ODS, which may have limited the ability to detect meaningful differences in risk and raises the possibility of underreporting. A recent retrospective cohort study of 13 988 adult hospitalized patients with severe hyponatremia also found a lower risk of 90-day mortality and delayed neurologic events with fast (>12 mEq/L/24 hours) or medium (8-12 mEq/L/24 hours) compared with slow (<8 mEq/L/24 hours) sodium correction. 17 Overall, current evidence has not clearly demonstrated a clinical advantage to slower correction of severe hyponatremia compared to more rapid correction rates.
Complete Shielding of Multivitamins to Reduce Toxic Peroxides in the Parenteral Nutrition (C-SMART-PN): A Randomized Controlled Pilot Study
Peroxides are generated when intravenous (IV) multivitamin is exposed to light, potentially leading to oxidative stress, which has been associated with neonatal bronchopulmonary dysplasia, retinopathy of prematurity, necrotizing enterocolitis, and intestinal failure. 18 Preterm neonates lack reduced glutathione, a required cofactor for peroxide detoxification. Multivitamin injection is the predominant source of peroxide contamination in PN solutions, so this study sought to evaluate the impact of complete photoprotection of IV multivitamin during PN compounding and administration versus standard processes in neonates. 12 In vitro evaluation found that photoprotection reduced peroxide generation by 44% (P < .001). Twenty-eight infants were enrolled in the randomized controlled pilot arm for in vivo evaluation. Photoprotection was associated with lower urinary peroxide levels during the first week of life (P < .05) compared to standard processes. No differences were observed between the groups in respiratory or other clinical outcomes.
ASPEN recommends complete PN photoprotection to reduce peroxide contamination in neonatal PN; however, implementation may be challenging in the United States because of the lack of appropriate sterile compounding products. 18 In this trial, IV multivitamin was prepared in a photoprotected syringe and infused via syringe pump through a photoprotected trifurcated extension set. Based on study results, the authors propose collaboration with industry partners on the development of a commercially available photoprotected syringe and extension set for IV multivitamin preparation and administration. Further evaluation in larger samples, over longer durations, is necessary to delineate clinical impacts of IV multivitamin photoshielding in the neonatal population.
Essential Fatty Acid Deficiency in Children Treated With Long-Term 100% Fish-Oil Lipid Injectable Emulsion: A Longitudinal Descriptive Cohort Study
When parenteral nutrition-associated cholestasis (PNAC) develops in children with intestinal failure receiving long-term PN, fish oil-based lipid injectable emulsion (ILE) is commonly used to reverse cholestasis and prevent progression to end-stage liver disease and transplantation. Compared with traditional soybean oil ILE, fish oil formulations contain substantially lower amounts of linoleic acid (LA; ω-6 fatty acids) and α-linolenic acid (ALA; ω-3 fatty acids), raising concern for development of essential fatty acid deficiency (EFAD). This single-center, prospective, longitudinal cohort study evaluated 127 infants and young children (<2 years of age) with PNAC treated with open-label 10% fish oil ILE (Omegaven®) under a compassionate-use protocol. 13 Patients were followed up to 4 years with serial clinical and biochemical assessment of EFAD. The cohort consisted largely of premature infants (median age 14 weeks [interquartile range (IQR) 8-26]) with median direct bilirubin of 5.8 mg/dL (IQR 3.8-8.9). At study completion, defined as PN discontinuation (mean duration 368 days; median 132.5 days), 68% achieved resolution of PNAC. Direct bilirubin declined by a mean of 2.03 mg/dL, with an estimated median time to resolution of 8.4 weeks. Biochemically, median triene:tetraene (T:T) ratios increased modestly early (peak 0.027 at week 8) but remained below the EFAD threshold (<0.05) throughout the study. Ten patients had mildly elevated baseline T:T ratios (≥0.05-<0.2); all but 1 normalized (early PN discontinuation). At the end of the study, 7 patients had mildly elevated ratios. Three patients met biochemical EFAD criteria (T:T ≥0.2), including 1 severe case (≥0.4). No patient developed clinical EFAD. Two infants with baseline physical findings suggestive of EFAD (growth failure, alopecia) improved despite normal initial T:T ratios. Over time, serum docosahexaenoic acid and eicosapentaenoic acid increased, whereas LA, ALA, eicosatrienoic acid, and arachidonic acid decreased and stabilized, reflecting expected shifts in fatty acid composition.
Despite inherent limitations of a nonrandomized compassionate-use design, this study provides robust longitudinal safety data supporting the use of 100% fish oil ILE at 1 g/kg/day in infants with PNAC. The low incidence of biochemical EFAD, absence of clinical EFAD, and high rates of cholestasis resolution are reassuring. Larger controlled studies are needed to address the applicability of standard T:T thresholds in PN-dependent infants, diagnostic criteria for EFAD, optimal ILE dosing, and the impact of enteral intake.
Micronutrient Status in Patients With Short Bowel Syndrome Weaned Off Parenteral Support
While a subset of adult patients with short bowel syndrome (SBS) may be successfully weaned from PN, the need for long-term monitoring of micronutrient status is unknown. This is a retrospective study conducted in 42 patients (mean age 62 ± 18 years when PN was initiated) to determine the prevalence and risk factors of micronutrient depletion in patients with SBS after PN had been weaned off for at least 1 year. 14 Sixty-four percent of patients had Type II SBS, a mean small bowel length of 109 ± 42 cm, and 75% had colon remaining. Micronutrient status was determined by plasma, serum, or whole blood concentration. Overall, 95% of the patients had at least 1 micronutrient deficiency despite micronutrient supplementation upon discontinuation of PN. The prevalence of vitamin and trace element deficiencies were 86% and 83%, respectively. The 5 most common deficiencies were selenium (65.7%), copper (62.9%), vitamin D (57.5%), zinc (47.2%), and vitamin E (45.9%). The least common deficiencies were folate (2.8%) and thiamin (2.8%). No patient developed riboflavin deficiency. It was notable that despite supplementation of vitamin D and cobalamin, 75% of the patients still developed deficiencies. Deficiency in vitamin C, vitamin D, and/or selenium was common among patients with type I SBS (ie, end-jejunostomy or end-ileostomy) or absence of colon. Among patients with continuity of colon, the most frequently observed deficiencies were copper, selenium, and vitamin D. Long-term proton-pump inhibitor use and prolonged PN use (>87 months) were associated with a high number of micronutrient deficiencies, whereas colon continuity, chronic kidney disease, inflammatory bowel disease, sarcopenia, or >10% weight loss after PN weaning were not. The authors concluded that weaning from PN does not guarantee adequate micronutrients absorption, and long-term monitoring of micronutrients is essential.
This is the first adult study to longitudinally assess micronutrient status after weaning off long-term PN, showing that deficiencies (eg, vitamin C, vitamin D, copper, and selenium), are common despite supplementation. This study has several limitations. Monitoring was inconsistent and not well described, which may have led to underestimating deficiencies. Micronutrient status was assessed only with blood levels of the specific micronutrient and did not include additional markers (eg, ceruloplasmin, glutathione peroxidase). The impact of inflammation was not considered which can influence true body stores. Finally, supplementation practices were unclear and potentially uneven across patients, making it difficult to determine whether deficiencies were due to inadequate or inconsistent supplementation. Overall, this study emphasizes the importance of long-term micronutrient monitoring for patients with SBS despite being weaned off PN therapy.
Augmented Enteral Protein During Critical Illness: The TARGET Protein Randomized Clinical Trial
While guideline recommendations continue to support higher protein doses in critically ill patients, large, high-quality, randomized trials demonstrating improved patient outcomes are lacking. In this cluster-randomized, cross-over, open-label trial of 3397 critically ill adults, patients were randomized to isocaloric EN with augmented (100 g/L) or usual (63 g/L) protein. 15 The primary outcome was days alive and free of index hospital at 90 days. Patients were predominantly male (64%) with medical admissions (64%), median age 61 years, acute physiology and chronic health evaluation II score 19, and body mass index (BMI) 27.5 kg/m2. EN started early (median 19 hours) after intensive care unit (ICU) admission and continued for a mean of 85.5 hours. Caloric intake was similar (median 14 kcal/kg ideal body weight [IBW]/day) and a meaningful difference in protein delivery was achieved (median 1.1 vs 0.7 g/kg IBW/day). No difference was found for the primary outcome. Treatment effect favored usual protein in the subgroup of patients requiring renal replacement therapy after admission (P < .001). These findings are hypothesis-generating only with wide uncertainty (95% confidence interval −50 to 23.62) and warrant cautious interpretation.
These results align with findings from similar recent trials (EFFORT and PRECISe) evaluating higher versus lower protein during critical illness.19,20 Daily provision of protein was still below guideline recommended targets of 1.2 to 2 g/kg/day, and may reflect the relatively short duration for EN observed in the study. Interpretation of results is also limited by substantial gaps in EN intake documentation (after 5 days, intake was audited intermittently). Future studies should consider the impacts of patient selection (eg, surgical ICU subtypes) and timing of higher and lower protein doses relative to the phase of critical illness.
Conclusions
With the large volume of publications pertinent to pharmacy nutrition support from a variety of journals, it is challenging to stay current with the literature. We have identified a select group of articles from 2025 that we consider important for pharmacists engaged in nutrition support. Although only those highest ranked articles from primary literature were discussed, other publications may be important depending on the patient population and the role of the pharmacist at their respective institution.
Supplemental Material
sj-docx-1-hpx-10.1177_00185787261454527 – Supplemental material for Significant Published Articles in 2025 for Pharmacy Nutrition Support Practice
Supplemental material, sj-docx-1-hpx-10.1177_00185787261454527 for Significant Published Articles in 2025 for Pharmacy Nutrition Support Practice by Angela L. Bingham, Roland N. Dickerson, Titilola M. Afolabi, Todd W. Canada, Lingtak-Neander Chan, Sarah V. Cogle, Diana Mulherin and Anne M. Tucker in Hospital Pharmacy
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Angela L. Bingham and Roland N. Dickerson have no conflicts of interest. Dr Titilola M. Afolabi is a consultant for Wolters Kluwer (Lexidrug). Dr Todd W. Canada is a consultant for Fresenius Kabi. Dr Lingtak-Neander Chan is a consultant for Baxter Healthcare. Dr Sarah V. Cogle is a consultant for Fresenius Kabi and Pharmacosmos Therapeutics, Inc. Dr Diana Mulherin is a consultant for Baxter Healthcare as a non-promotional symposia speaker and advisory board member. Dr Anne M. Tucker is a consultant for UpToDate, Inc.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.