
Abstract
Background:
Intrapleural tissue plasminogen activator (tPA) and DNase are used when drainage of loculated pleural effusions is inadequate, but the real-world performance of pragmatic once-daily protocols remains uncertain.
Methods:
We performed a retrospective cohort study across seven hospitals between January 1, 2019, and December 31, 2020. Adults who received intrapleural tPA 20 or 50 mg once daily with optional DNase 5 mg once daily for complicated pleural effusion, empyema, or hemothorax were included. The primary outcome was treatment success, defined as survival to hospital discharge without surgical intervention during the index admission. Secondary outcomes included chest tube drainage change, hospital length of stay, ICU length of stay, mortality, major bleeding, and peri-procedural pain requiring analgesics. A post hoc subgroup analysis compared monotherapy with combination therapy.
Results:
Among 120 included patients, treatment success occurred in 102 (85.0%; 95% CI, 77.3%-90.9%). The median paired increase in chest tube drainage was 487.5 mL (IQR, 72.5-979.0; P < .001). Major bleeding occurred in one patient (0.8%), whereas peri-procedural pain requiring additional analgesia occurred in 69 (57.5%). In the exploratory subgroup analysis, treatment success was 83.8% with tPA monotherapy and 87.0% with tPA/DNase combination therapy.
Conclusions:
In this multicenter real-world cohort, standardized intrapleural tPA with or without DNase was associated with high observed treatment success, substantial increases in drainage, and rare major bleeding. Comparative findings between combination therapy and monotherapy should be interpreted cautiously because treatment allocation was nonrandomized and exposure groups were imbalanced.
Keywords
Introduction
Parapneumonic pleural effusions complicate 20% to 40% of pneumonia hospitalizations, and pleural infection remains associated with substantial morbidity, prolonged hospitalization, and mortality.1,2 When tube drainage is limited by septations or loculations, clinicians must decide between escalation to surgery and adjunctive intrapleural fibrinolytic therapy.3,4 More recent international guidance has reinforced that pleural infection remains an increasingly important clinical problem and that timely definitive management matters.4,5
Interest in intrapleural fibrinolysis has evolved over the last two decades. MIST1 demonstrated no clinical benefit of intrapleural streptokinase for pleural infection. 6 In contrast, MIST2 showed that the combination of intrapleural tissue plasminogen activator and DNase improved radiographic clearance and reduced surgical referral and hospital length of stay compared with placebo. 7 Subsequent observational studies have supported the clinical utility of tPA/DNase, but real-world practice has remained heterogeneous with respect to dosing, frequency, timing, and administration strategy, including once-daily sequential and concurrent regimens.8-11 Contemporary expert guidance from the ERS/ESTS statement and the 2023 British Thoracic Society guideline reflects this tension: both acknowledge the growing supportive literature for intrapleural enzyme therapy, but also emphasize that the MIST2 combination regimen remains the most evidence-based standard while optimal dose selection and timing remain unsettled.4,5
This uncertainty is particularly relevant to pragmatic health-system protocols. In 2022, a large international multicenter retrospective cohort of 1833 patients found that combination intrapleural enzyme therapy was associated with a relatively low overall pleural bleeding rate of 4.1% while also identifying concurrent therapeutic anticoagulation as an important bleeding-risk modifier. 12 In parallel, dose-optimization studies have suggested that lower starting alteplase doses may remain effective, and more recent cohort data continue to support favorable outcomes with pragmatic protocols.13-16 Together, these findings suggest that the field is moving beyond a simple efficacy question toward a more nuanced question of which patients benefit most, at what dose, and with what trade-off in safety and resource use.
Across our seven-hospital health system, intrapleural alteplase is ordered through a standardized electronic order set that allows tPA 20 or 50 mg once daily with optional DNase 5 mg once daily. Because this protocol differs meaningfully from the twice-daily MIST2 regimen and because DNase use is not mandatory, questions persisted regarding the effectiveness and safety of our institutional approach in routine practice, as well as whether combination therapy offered measurable advantage over tPA monotherapy within this practice model. We therefore evaluated the effectiveness and safety of intrapleural tPA with or without DNase across a large community health system and performed an exploratory subgroup analysis comparing combination therapy with tPA monotherapy.
Methods
Setting and Study Design
This multicenter retrospective cohort study was conducted within the AdventHealth Central Florida Division South, encompassing seven hospital campuses in the Orlando, Florida region (AdventHealth Altamonte, AdventHealth Apopka, AdventHealth Celebration, AdventHealth East Orlando, AdventHealth Kissimmee, AdventHealth Orlando, and AdventHealth Winter Park). The AdventHealth Institutional Review Board determined the project to be a quality-improvement initiative exempt from full review (Approval/Exemption No. 1831458-1, date October 28, 2021). Patients were identified through the electronic medical record (Cerner) by administrations linked to the institutional intrapleural fibrinolytic order set between January 1, 2019, and December 31, 2020. This manuscript was prepared with reference to the STROBE reporting guideline, 17 and the completed STROBE checklist 18 is included as Supplemental Material A.
Institutional Protocol and Patient Selection
The standardized protocol allowed provider selection of intrapleural tPA 20 mg or 50 mg once daily, with optional DNase 5 mg once daily. The protocol defaulted to two once-daily doses, with provider discretion to discontinue after one dose or extend to four doses based on clinical response, drainage output, imaging response, adverse effects, procedural factors, or transition to alternative management. Adults aged 18 years or older were eligible if they received at least one documented dose of intrapleural tPA through the order set for complicated parapneumonic effusion, empyema, or hemothorax during the study period. Patients were excluded if tPA administration could not be confirmed or if key baseline or outcome data required for analysis were missing. A total of 172 patients were screened, of whom 52 were excluded: 40 for missing tPA administration data, 5 for missing pleural access type data, 3 for missing indication for intrapleural tPA, 2 for missing pertinent baseline demographic data, and 2 for being outside the age range for inclusion. The final analytic cohort included 120 patients (Figure 1).
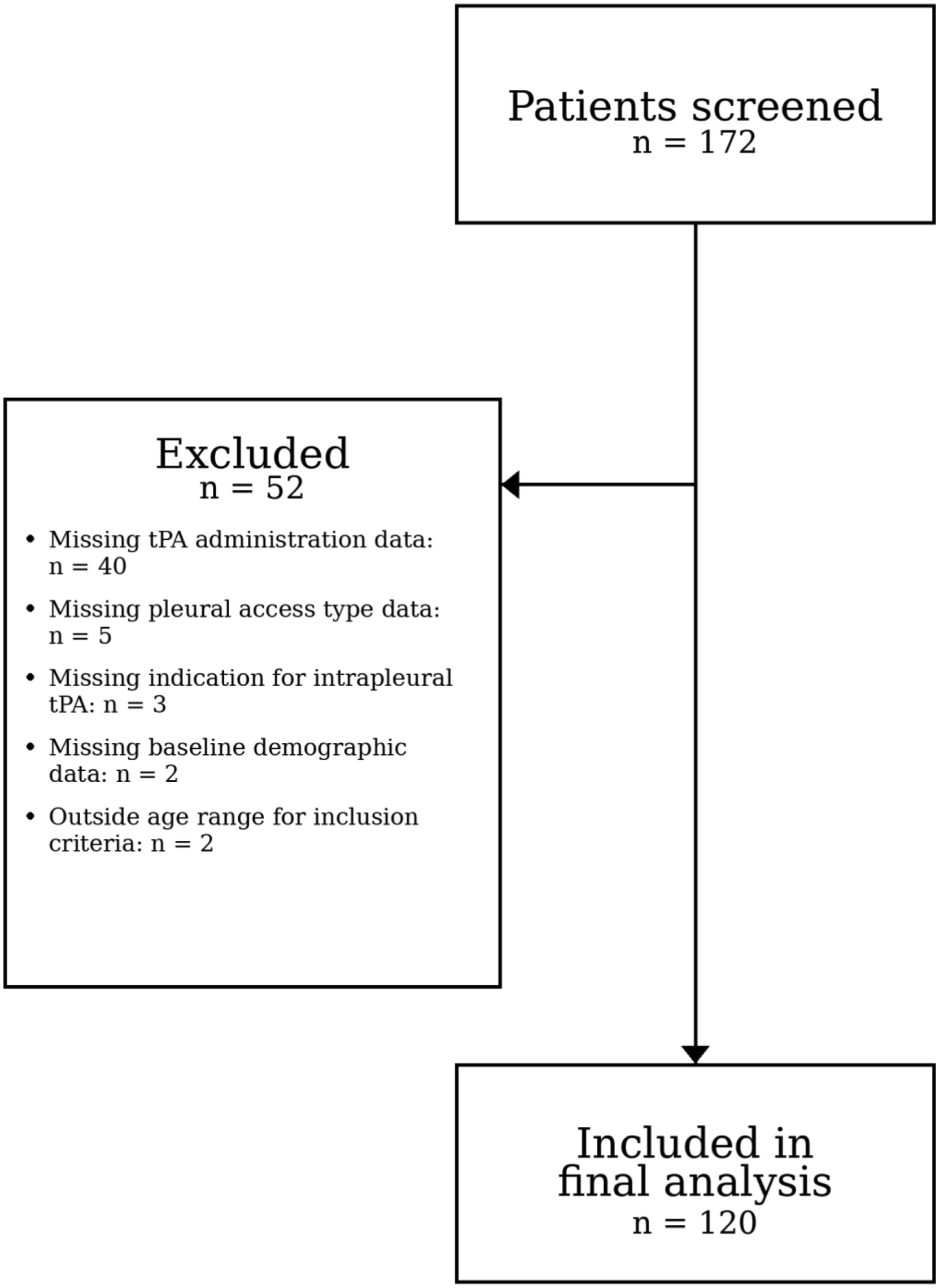
Study flow diagram showing patient screening, exclusions, and final inclusion in the analytic cohort.
Outcomes
The primary outcome was treatment success, defined as survival to hospital discharge without surgical intervention for pleural disease during the index admission. Secondary outcomes included change in chest tube drainage volume, hospital length of stay, ICU length of stay, mortality, major bleeding, and peri-procedural pain requiring analgesic administration within 4 hours of fibrinolytic instillation. Chest tube drainage change was defined for each patient as cumulative drainage from the first dose to 24 hours after the final dose or until chest tube removal or surgical intervention (“post-medication”) minus cumulative drainage from chest tube insertion to the first fibrinolytic dose (“pre-medication”). Major bleeding was defined using International Society on Thrombosis and Haemostasis criteria, focusing on clinically significant bleeding associated with a hemoglobin decrease of at least 2 g/dL, transfusion of at least 2 units of packed red blood cells, or bleeding at a critical site. A post hoc subgroup analysis compared tPA monotherapy with tPA plus DNase combination therapy.
Statistical Analysis
Because the primary analysis was descriptive and included all eligible treated patients, no a priori power calculation was performed. The overall cohort primary endpoint was estimated as a single proportion with exact binomial 95% confidence intervals. Continuous variables central to the comparative analyses were non-normally distributed and are summarized as median [IQR]; categorical variables are summarized as number (percentage). Within-patient change in chest tube drainage was evaluated with the Wilcoxon signed-rank test. For exploratory between-group comparisons, categorical outcomes were assessed with Pearson chi-square or Fisher exact tests as appropriate, and continuous outcomes were compared with the Mann-Whitney U test. Holm adjustment was applied across six secondary between-group comparisons to limit family-wise error. Because treatment allocation was not randomized, all between-group comparisons were prespecified as exploratory and interpreted as noncausal. All statistical analyses were performed in IBM SPSS Statistics Version 30.0.0.0 (172).
Results
Study Population
A total of 172 patients were screened and 120 met inclusion criteria with analyzable data. The median age was 69.0 years [56.0, 77.2], and 61 of 120 patients (50.8%) were male. Most patients were treated for complicated pleural effusion (103/120, 85.8%), with the remaining 17 patients (14.2%) treated for empyema or hemothorax. Eight patients (6.7%) were mechanically ventilated at the time of intrapleural fibrinolytic administration. Pleural drainage catheters at the time of therapy included PleurX catheters in 61 patients (50.8%), pigtail catheters in 54 (45.0%), and large-bore chest tubes in 5 (4.2%) (Table 1).
Baseline and Treatment Characteristics by Therapy Group.
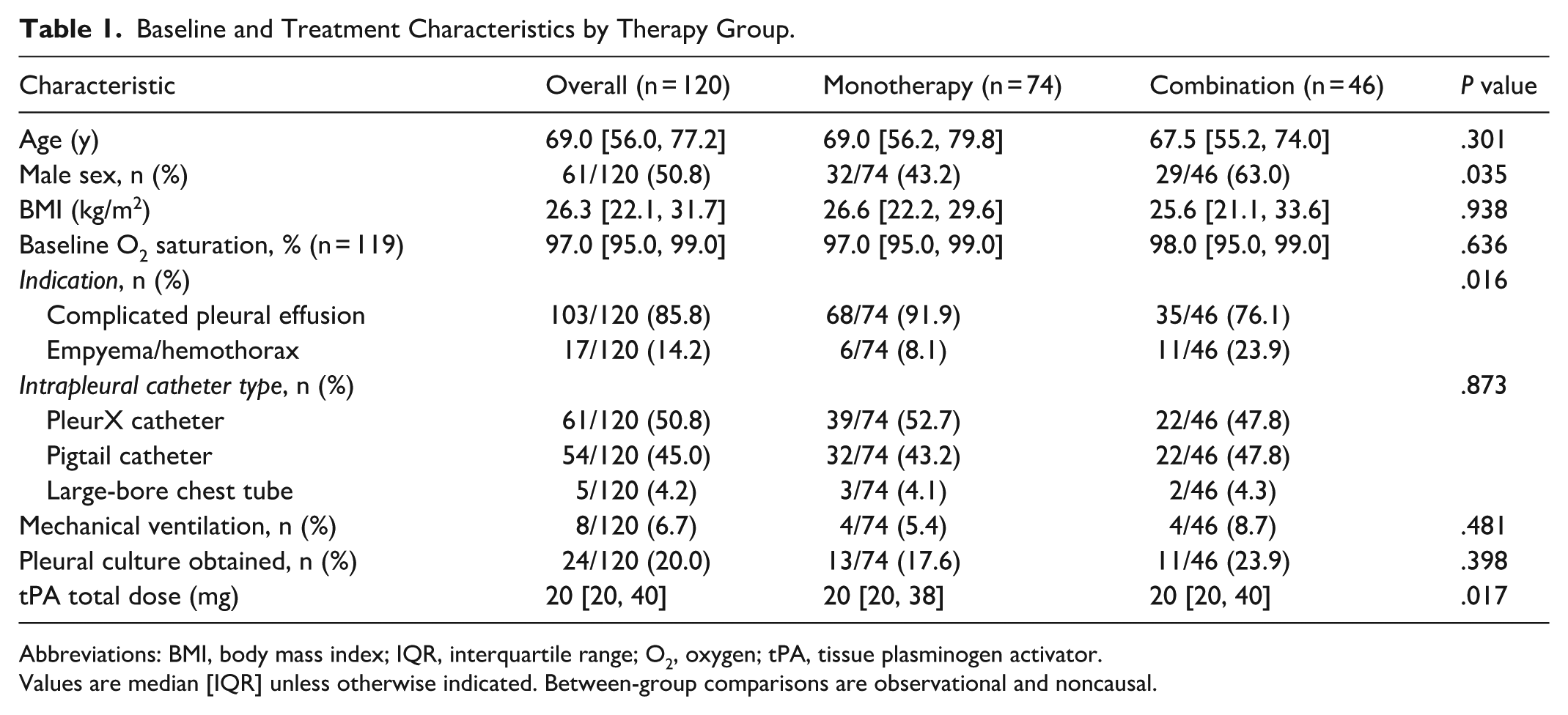
Abbreviations: BMI, body mass index; IQR, interquartile range; O2, oxygen; tPA, tissue plasminogen activator.
Values are median [IQR] unless otherwise indicated. Between-group comparisons are observational and noncausal.
Of the 120 included patients, 74 (61.7%) received tPA monotherapy and 46 (38.3%) received combination tPA/DNase. The treatment groups were not well balanced. Compared with the monotherapy group, the combination group included a higher proportion of male patients (63.0% vs 43.2%), more empyema/hemothorax cases (23.9% vs 8.1%), and a different distribution of total tPA dose (Table 1). These imbalances supported interpreting all between-group comparisons as exploratory and potentially confounded. Most patients received one documented tPA dose (86/120, 71.7%), while 34 patients (28.3%) received two or more documented tPA doses.
Overall Clinical Outcomes
Treatment success occurred in 102 of 120 patients (85.0%; 95% CI, 77.3%-90.9%). The component outcomes were similarly favorable: 111 of 120 patients (92.5%; 95% CI, 86.2%-96.5%) avoided surgery and 110 of 120 (91.7%; 95% CI, 85.2%-95.9%) survived to hospital discharge. Nine patients underwent surgical intervention, 10 patients died before discharge, and 1 patient experienced both events. No missing data remained for the primary outcome among included patients.
Chest tube drainage increased substantially after fibrinolytic therapy. Median pre-medication drainage was 0 mL (IQR, 0-110), median post-medication drainage was 585 mL (IQR, 161-1100), and the median paired change in drainage was 487.5 mL (IQR, 72.5-979.0; Wilcoxon signed-rank P < .001). Median hospital length of stay was 13.0 days [7.0, 21.0]. Among 22 patients with analyzable ICU stay dates, the median ICU length of stay was 10 days [5.5, 17.5]. ICU length of stay is reported only for patients with analyzable ICU admission and discharge data, and variable-specific denominators are shown where applicable. Major bleeding occurred in 1 patient (0.8%; 95% CI, 0.0%-4.6%), whereas peri-procedural pain requiring additional analgesia occurred in 69 patients (57.5%; 95% CI, 48.1%-66.5%). Mortality at discharge was 8.3% (10/120; 95% CI, 4.1%-14.8%) (Table 2).
Overall Cohort Clinical Outcomes.
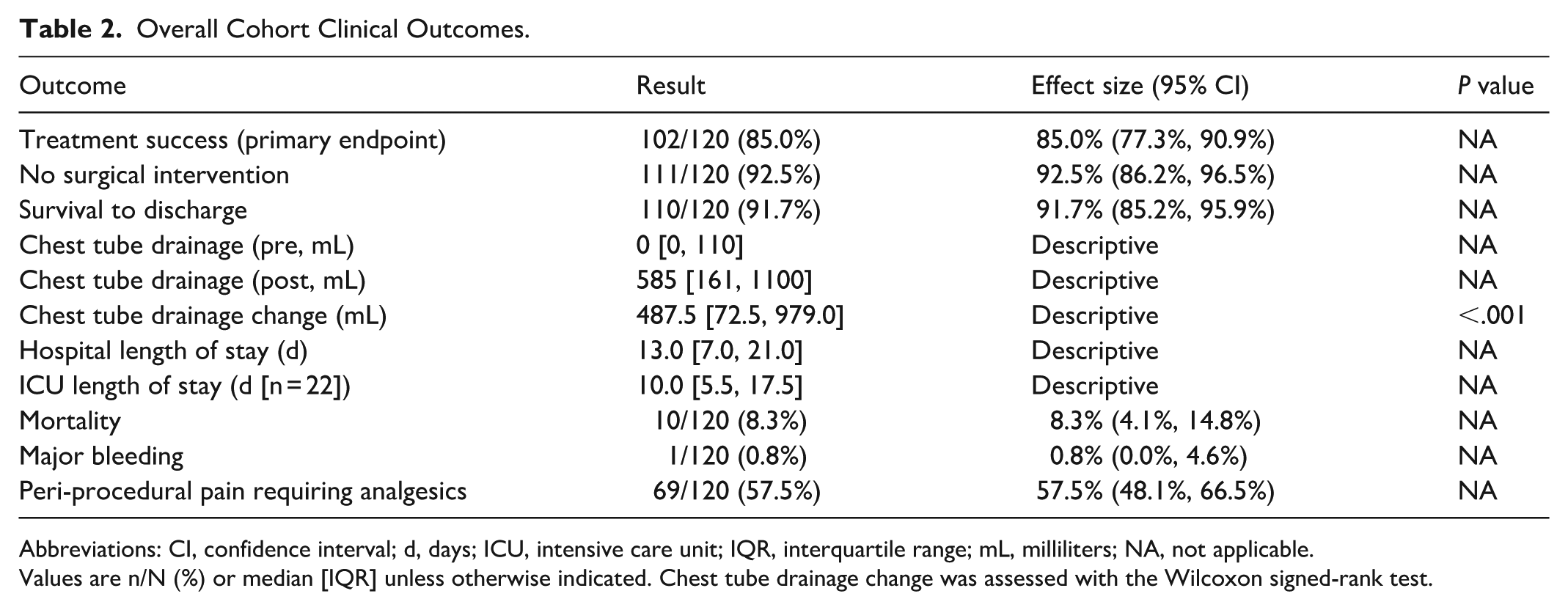
Abbreviations: CI, confidence interval; d, days; ICU, intensive care unit; IQR, interquartile range; mL, milliliters; NA, not applicable.
Values are n/N (%) or median [IQR] unless otherwise indicated. Chest tube drainage change was assessed with the Wilcoxon signed-rank test.
Exploratory Subgroup Analysis
Treatment success was similar between tPA monotherapy and combination therapy (62/74 [83.8%] vs 40/46 [87.0%]). The absolute risk difference was 3.2% (95% CI, −11.5% to 16.2%), and the relative risk was 1.04 (95% CI, 0.89-1.21). Mortality, major bleeding, chest tube drainage change, and hospital length of stay also did not differ significantly between groups (Table 3). Additional analgesic use was more frequent in the combination group (69.6% vs 50.0%), corresponding to a raw risk difference of 19.6% (95% CI, 1.5%-36.0%), but this signal did not persist after Holm adjustment (adjusted P = .210).
Exploratory Secondary Outcomes Comparing Monotherapy with Combination Therapy.
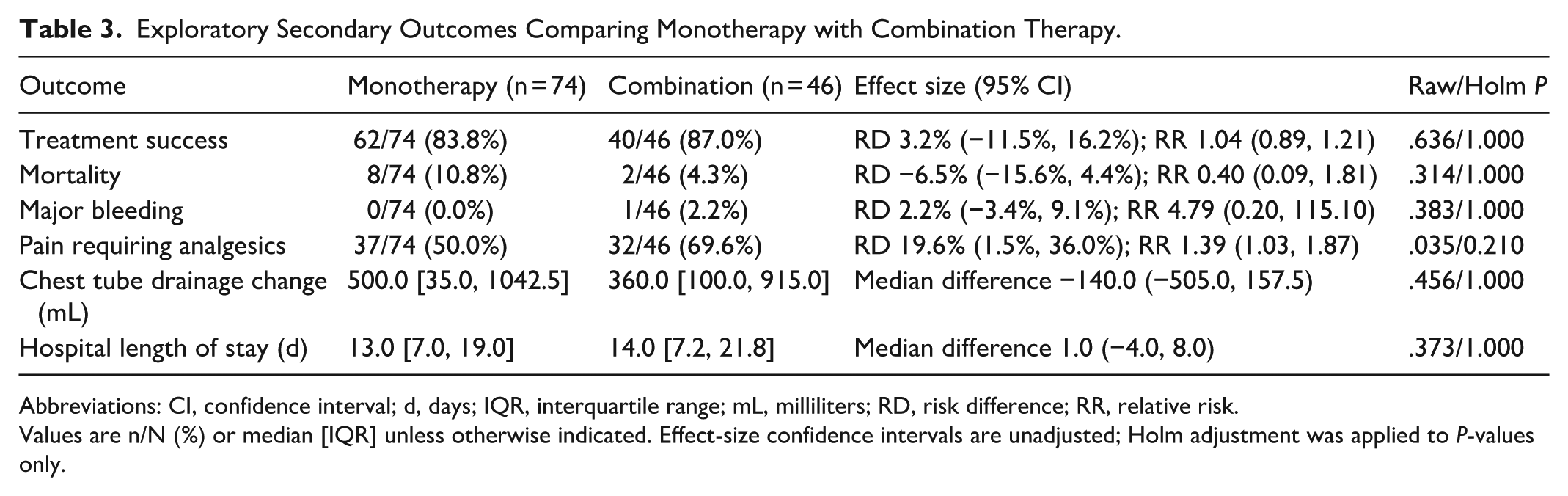
Abbreviations: CI, confidence interval; d, days; IQR, interquartile range; mL, milliliters; RD, risk difference; RR, relative risk.
Values are n/N (%) or median [IQR] unless otherwise indicated. Effect-size confidence intervals are unadjusted; Holm adjustment was applied to P-values only.
Discussion
In this multicenter retrospective cohort of patients treated through a standardized once-daily intrapleural fibrinolytic order set, intrapleural tPA with or without DNase was associated with high observed treatment success, substantial increases in chest tube drainage, and rare major bleeding. These findings remain broadly consistent with the contemporary literature that has emerged since 2021. Recent post-MIST2 studies have continued to support the effectiveness of intrapleural fibrinolytic therapy in routine practice while shifting the discussion toward dose optimization, timing of escalation, and complication stratification rather than re-establishing whether the therapy has biologic activity.12-16 Our observed treatment success rate of 85.0% is especially notable because it was achieved with a pragmatic once-daily protocol that permitted tPA monotherapy, optional DNase use, and higher alteplase doses than those used in MIST2.
Several recent studies help place our efficacy findings in context. In a 2022 retrospective cohort, Baumgartner et al 15 found high success with both tPA monotherapy and tPA with DNase, with no clear dose-response relationship across cumulative tPA exposure. In ADAPT Study-2, a starting regimen of 2.5 mg tPA plus 5 mg DNase achieved 88.4% treatment success at 90 days, suggesting that lower-dose strategies may remain effective when paired with dose escalation for inadequate response. 13 Likewise, a 2024 Singapore cohort of pleural infection cases treated with intrapleural fibrinolytic therapy reported 85.5% treatment success with a median starting tPA dose of 5 mg and found that earlier administration after chest tube placement was associated with better outcomes. 16 Taken together, these studies suggest that favorable outcomes may be achievable across a range of tPA doses, but they also reinforce that cross-study comparisons are limited by differing treatment protocols, patient selection, radiographic definitions, and escalation thresholds.
Our subgroup analysis did not demonstrate a clear comparative advantage for adding DNase to tPA within this institutional protocol. That finding should be interpreted cautiously and should not be read as contradicting the broader direction of current guideline recommendations. The 2023 British Thoracic Society guideline recommends combination tPA and DNase when initial drainage has ceased and residual pleural collection remains, and specifically advises against relying on single-agent tPA or DNase alone for pleural infection. 4 The 2023 ERS/ESTS statement similarly concluded that, although newer data support the safety and efficacy of intrapleural enzyme therapy, the MIST2 combination regimen remains the most evidence-based approach pending further prospective optimization studies. 5 Our observational comparison is more appropriately understood as hypothesis-generating, particularly because treatment assignment was not randomized and the exposure groups were imbalanced in sex, indication, and total tPA dose. Although treatment success appeared numerically similar between the cohorts, the combination therapy group achieved these outcomes despite a substantially higher baseline burden of frank empyema and hemothorax. Patients receiving DNase or additional tPA doses may have represented a clinically more complex subgroup, further limiting direct comparability between treatment strategies. A contemporary retrospective cohort by Baumgartner et al 15 also reported high success in both monotherapy and combination groups without a statistically significant difference, underscoring how real-world nonrandomized data can produce clinically reassuring but methodologically non-definitive comparisons.
The dosing and combination-therapy patterns observed in this cohort should be interpreted as features of real-world protocol implementation rather than randomized treatment assignment. Selection of tPA 20 mg versus 50 mg and the decision to add DNase were left to provider discretion within the order set and were not governed by prespecified study criteria. Most patients (71.7%) received a single documented tPA dose, whereas a minority (28.3%) received two or more documented tPA doses. The rationale for patients receiving only one dose was not systematically captured. Discontinuation after a single dose may have reflected clinical improvement, inadequate response prompting alternative management, adverse effects, procedural factors, or documentation limitations. This uncertainty introduces potential selection and information bias and limits causal interpretation of dose-response or monotherapy-versus-combination comparisons.
The safety findings in our cohort also align with more contemporary evidence. The international multicenter 2022 cohort by Akulian et al 12 reported an overall pleural bleeding rate of 4.1% with combination intrapleural enzyme therapy and identified concurrent systemic anticoagulation as a major predictor of bleeding risk. Our major bleeding rate of 0.8% is lower than that estimate, but such comparisons must remain cautious because our cohort differed in regimen, treatment intensity, and outcome ascertainment. Importantly, newer data suggest that lower-dose tPA strategies do not necessarily sacrifice safety or effectiveness. The ADAPT Study-2 found no clear efficacy signal loss with a 2.5 mg starting dose plus DNase, 13 and a 2022 prospective study using a modified 16 mg tPA plus 5 mg DNase regimen administered over 24 hours reported 90% treatment success with no surgical referrals. 14 The impact of intrapleural fibrinolytic regimens on pain also deserves emphasis. In the large 2022 international cohort, nonbleeding complications were uncommon apart from pain, 12 and in the modified-regimen prospective study, pain requiring escalation of analgesia affected 20% of patients. 14 In our cohort, additional analgesic requirement occurred in 57.5% of patients, suggesting that peri-procedural pain may be more frequent in pragmatic real-world use than is often appreciated, especially when captured through medication administration rather than spontaneous adverse-event reporting or validated pain scales. Given that over half of the patients required supplemental analgesics following instillation, health systems utilizing similar pragmatic protocols may consider the utilization of preemptive analgesia prior to intrapleural administration. Transitioning from reactive to proactive pain management may improve patient tolerance and minimize procedural morbidity.
Recent surgical literature also sharpens the context for interpreting our study. A 2023 pilot randomized trial comparing intrapleural fibrinolytic therapy with surgical decortication showed that a head-to-head algorithm was feasible and safe, with similar short-term complication profiles but a nonsignificant trend toward shorter hospital stay in the surgery group. 19 The MIST-3 feasibility randomized trial likewise demonstrated that early escalation trials are feasible, with signals that early surgery may shorten length of stay while early intrapleural enzyme therapy may favor recovery-related outcomes. 20 Consistent with this, a 2024 systematic review and meta-analysis found that surgery was associated with higher treatment success and shorter hospital length of stay and chest-drain duration than intrapleural fibrinolysis, although in-hospital mortality did not differ. 21 These contemporary data do not diminish the relevance of our findings, but instead serve to frame them appropriately. Our results support intrapleural fibrinolytic therapy as a viable nonsurgical strategy within a large health system, especially when surgery is undesirable or deferred, but they do not establish medical therapy as superior to earlier operative intervention in patients who are good surgical candidates.
This study has several strengths. It reflects real-world practice across seven hospitals within a large community health system, evaluates outcomes associated with a standardized electronic order set rather than isolated clinician preference, and reports clinically relevant safety outcomes in addition to effectiveness. At the same time, the retrospective design introduces risk of selection bias, information bias, and residual confounding. Fifty-two screened patients were excluded, most commonly because tPA administration or key outcome data could not be confirmed. The subgroup comparison was particularly vulnerable to bias because treatment assignment was nonrandom and the groups were imbalanced at baseline. Contemporary statements now emphasize dose optimization, earlier treatment consideration, multidisciplinary escalation pathways, and prospective evaluation of patient-centered outcomes such as pain and dyspnea.5,20,21 Our data fit well within that agenda and support further prospective comparisons of once-daily pragmatic regimens with more conventional combination-therapy strategies. These findings may be most generalizable to similar large community health systems using pragmatic once-daily intrapleural fibrinolytic protocols. For hospital pharmacy practice, these findings support the value of standardized order sets, prospective monitoring for pain and bleeding, and continued evaluation of dose selection and medication-use efficiency in patients receiving intrapleural fibrinolytic therapy.
Conclusion
Intrapleural tPA administered through this standardized once-daily protocol, with or without DNase, was associated with high observed treatment success and low major bleeding rates in this multicenter retrospective cohort. Pain requiring additional analgesia was common. Within this retrospective dataset, exploratory subgroup analysis did not show clear comparative benefit for combination therapy, but those findings are constrained by confounding and limited event counts. Prospective studies are needed to define the optimal dosing, timing, and role of DNase within pragmatic intrapleural fibrinolytic strategies.
Supplemental Material
sj-docx-1-hpx-10.1177_00185787261462057 – Supplemental material for Intrapleural Tissue Plasminogen Activator With or Without Dornase Alfa: A Multicenter Retrospective Cohort Study
Supplemental material, sj-docx-1-hpx-10.1177_00185787261462057 for Intrapleural Tissue Plasminogen Activator With or Without Dornase Alfa: A Multicenter Retrospective Cohort Study by Michelle P. Dillon, Eric C. Pyles and Emily H. To in Hospital Pharmacy
Footnotes
Ethical Considerations
This study was reviewed by the AdventHealth Institutional Review Board and determined to be a quality-improvement initiative exempt from full review (Approval/Exemption No. 1831458-1, date October 28, 2021).
Consent to Participate
The AdventHealth Institutional Review Board determined that informed consent to participate was not required for this exempt quality-improvement project.
Author Contributions
All authors contributed substantially to study conception and design, data acquisition and interpretation, drafting or critical revision of the manuscript, and approval of the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are not publicly available because of institutional and patient privacy restrictions.
Use of Generative AI and AI-Assisted Technologies in the Writing Process
During preparation of this manuscript, the authors used ChatGPT (OpenAI) to assist with refinement of author-drafted text for readability and clarity, and to help identify and summarize potentially relevant recent literature for the Introduction and Discussion. The authors independently reviewed all suggested literature against the original source publications and independently verified all statistical analyses reported in the manuscript in IBM SPSS before inclusion. No AI tool was used to create, alter, or fabricate primary study data. The authors take full responsibility for the content of this manuscript.
Disclaimer
The views expressed in this article do not communicate an official position of AdventHealth.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.