
Abstract
Objectives:
The stability of metronidazole has been demonstrated for high concentration and short-term storage. Little is known about the stability of its dilutions in 0.9% sodium chloride at concentrations relevant for neonatal clinical practice. This study aimed to evaluate the stability of metronidazole solutions at concentrations of 0.1 and 0.6 mg/mL, stored at room temperature and under refrigeration for 24 and 48 hours in 0.9% sodium chloride.
Methods:
Metronidazole concentrations were measured using a high-performance liquid chromatography method with ultraviolet detection. Calibration curves were linear over the concentration range of 0.025 to 1.25 mg/mL. Stability was defined as retention of 90% to 110% of the initial concentration. Results were expressed as percent deviation from the initial (0 hour) concentration, where 0% corresponds to the initial value (100%).
Key findings:
At room temperature, mean relative accuracy ranged from 0.7 ± 1.8% to 5.5 ± 1.1%. Under refrigeration, it ranged from −5.5 ± 4.0% to 3.5 ± 1.8%. All samples remained within the pharmacopeial acceptance range (90%-110%) of the initial concentration, corresponding to deviations within ±10%.
Conclusions:
Metronidazole concentrations of 0.1 and 0.6 mg/mL remained within the predefined acceptance limits for up to 48 hours in 0.9% w/v sodium chloride at 6°C and 22°C, supporting safe short-term storage in neonatal practice.
Introduction
The nitroimidazole antibiotic, metronidazole, is administered in adults and children for the prevention and treatment of infections caused by metronidazole-susceptible anaerobic bacteria and requiring intravenous administration of the drug. 1 It is frequently prescribed to infants with serious intra-abdominal infections. 2 In premature infants, metronidazole use is typically restricted to treatment of anaerobic bacteremia, central nervous system infections and complicated intra-abdominal infections such as necrotizing enterocolitis. 3 Metronidazole dosing in neonates is complex due to developmental changes in pharmacokinetics, including an increased volume of distribution and prolonged half-life,4-6 as well as immature hepatic metabolism.6,7 In addition, drug disposition is influenced by gestational, postnatal and postmenstrual age, leading to multiple dosing recommendations. 8 The pharmacokinetic and pharmacodynamic properties of metronidazole vary across patient populations, with dosing adjusted to achieve therapeutic targets in children and adolescents based on body weight, infection severity, and clinical response. 9
Published studies have primarily evaluated metronidazole at the commercially available concentration of 5 mg/mL, mainly in the context of compatibility with other drugs, especially antibiotics (eg, cefepime, levofloxacin, ceftriaxone)1,10,11 or parenteral nutrition admixtures.12,13 Little is known about the stability of metronidazole dilutions in 0.9% w/v sodium chloride at concentrations which are of clinically relevant in neonatal wards. Therefore, the aim of this study was to evaluate the stability of metronidazole solutions at concentrations of 0.1 mg/mL and 0.6 mg/mL, stored at room temperature and under refrigeration for 24 and 48 hours, in 0.9% sodium chloride. The concentrations of 0.1 and 0.6 mg/mL are the most frequently used in clinical practice for neonates’ treatment.
Materials and Methods
Chemicals and Reagents
Metronidazole was obtained as Metronidazole 0.5% (Fresenius Kabi Polska Sp. z o.o., Warsaw, Poland), supplied in 50 mL bottles at a concentration of 5 mg/mL. This solution was used as a reference standard for calibration and validation. The 0.9% w/v sodium chloride solution was produced by B. Braun Melsungen AG (Melsungen, Germany). For mobile phase, ammonium acetate and acetonitrile, of high-performance liquid chromatography (HPLC) grade, were obtained from Merck (Darmstadt, Germany).
Chromatographic Conditions
The chromatographic method was adapted from the literature. 14 HPLC analysis was performed using a HPLC system HP1100 (Hewlett Packard, Palo Alto, CA, USA) with ultraviolet detection at 320 nm. A Zorbax Eclipse XDB C18 analytical column (4.6 × 150 mm, 5 µm) thermostated at 40°C was used. The mobile phase consisted of 50 mM ammonium acetate (pH 4.5) and acetonitrile mixed at a ratio of 90:10 (v/v). The injection volume was 10 µL, and the flow rate of the mobile phase was 1 mL/min. The retention time of metronidazole was 4.0 minutes.
Working Solutions
As a stock solution of metronidazole, the solution of 5 mg/mL was used. On each day of analysis, working solutions of metronidazole in 0.9% sodium chloride were freshly prepared at the following concentrations: 0.025, 0.05, 0.1, 0.25, 0.5, 0.75, and 1.25 mg/mL. Before injection, samples were diluted 10-fold with the mobile phase (10 μL of working solution was mixed with 90 μL of mobile phase), vortexed and injected into the HPLC system. No internal standard was used, as only intravenous fluids, not biological matrix, were analyzed, and no extraction or other sample preparation procedures were performed. Analyses were performed in quintuplicate (n = 5) for within-run accuracy and precision and in triplicate (n = 3) for between-run accuracy and precision. A t-test was applied to determine whether the intercept differed significantly from zero, with significance set at P < .05.
Stability Assessment
For stability tests, metronidazole solutions were prepared at two concentrations (0.1 and 0.6 mg/mL) in 0.9% sodium chloride and stored for 48 hours at room temperature (22°C) and under refrigerated conditions (6°C) to mimic hospital pharmacy and ward conditions, including the time frame required for the preparation, storage, and administration of drugs in clinical practice. Samples were stored in capped polypropylene tubes, protected from light, and analyzed after 24 and 48 hours. The visual inspection was conducted to exclude precipitation, turbidity or discoloration.
Calculations
For quality control (QC) concentrations, precision was calculated as the coefficient of variation (CV = SD/Cback-calculated·100%), and accuracy was estimated as (Cback-calculated/Cnominal)·100%. Stability was assessed based on the retention of metronidazole concentration over time. The test samples were divided into at least three aliquots and analyzed against a calibration curve prepared from freshly spiked standards. A preparation was considered stable if the measured concentration remained within 90% to 110% of the initial value (time 0), in line with pharmacopeial recommendations for compounded preparations (eg, USP). 15 Stability was expressed as relative accuracy (%) with respect to the initial (0 hour) concentration, where 0% corresponds to 100% of the initial concentration. In addition, the variability of analytical measurements was interpreted with reference to commonly accepted bioanalytical validation criteria (±15%), to distinguish potential analytical variability from physicochemical instability. The assay was not formally validated as stability-indicating, as no stress testing (acid, alkali, peroxide, elevated temperature) was performed to detect possible degradants.
Results
The calibration curve for metronidazole in 0.9% w/v sodium chloride was linear within the range of 0.025 to 1.25 mg/mL and equation was PSAmetronidazole = 3133·Cmetronidazole, where PSAmetronidazole denotes the peak surface area of metronidazole and Cmetronidazole stands for the metronidazole concentration. The correlation coefficient R² was 0.9999. As the intercepts were negligible, calibration was forced through zero. Calibration equation with the graph is provided in the Supplementary Material (Figure S1). The method demonstrated acceptable within-run (n = 5) and between-run (n = 3) accuracy and precision for metronidazole in 0.9% w/v sodium chloride (Supplementary Material, Table S1).
The results of the stability test for metronidazole in 0.9% w/v sodium chloride are presented in Table 1. The mean relative accuracy of 0.1 and 0.6 mg/mL concentrations remained within ±10% of the initial concentration and within the pharmacopeial acceptance range (90%-110%) under all tested conditions. For room temperature, the mean relative accuracy of metronidazole ranged from 0.7 ± 1.8% to 5.5 ± 1.1%. For storage in refrigerator, the mean relative accuracy of metronidazole was within −5.5 ± 4.0% to 3.5 ± 1.8%. For no replicate, the value of relative accuracy was higher than 10%.
The Stability of Metronidazole in 0.9% w/v Sodium Chloride, Expressed as Relative Accuracy (%) with Respect to the Initial (0 h) Concentration.
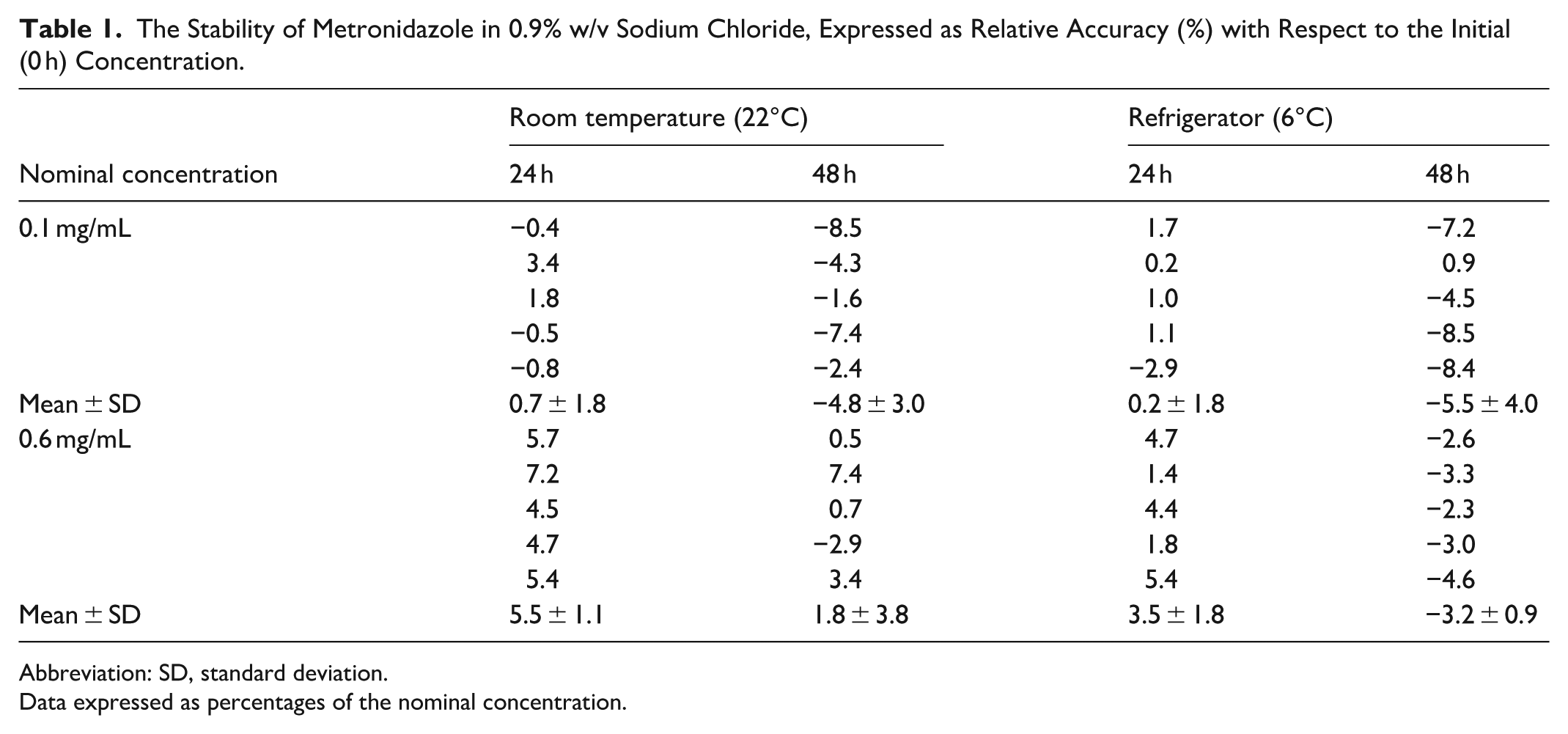
Abbreviation: SD, standard deviation.
Data expressed as percentages of the nominal concentration.
Visual inspection revealed no evidence of physical instability in any tested sample throughout the study period. No precipitation, turbidity or discoloration was observed.
Discussion
In the present study, metronidazole solutions at concentrations of 0.1 and 0.6 mg/mL remained stable for up to 48 hours at room temperature and under refrigeration, maintaining ≥90% of the initial concentration. These concentrations are the most frequently used in the Department of Neonatology at Poznan University of Medical Sciences. To our knowledge, this is the first study on the stability of diluted metronidazole. The stability of diluted intravenous metronidazole preparations should be specifically evaluated, particularly in neonatal and preterm populations where small doses often require dilution prior to administration. In neonatal practice, the use of highly diluted solutions may increase the relative impact of physicochemical processes such as adsorption to container materials or light-induced degradation. Such factors may influence drug stability and recovery, and therefore stability data obtained at higher commercial concentrations cannot always be directly extrapolated to diluted preparations. Consequently, dedicated stability studies of clinically relevant dilutions are necessary to ensure accurate dosing and safe pharmacotherapy in neonates.14,16
In previously published studies, metronidazole was tested undiluted at a concentration of 5 mg/mL and for short-term (3-4 hours) storage.1,10,12,13 Only Bailey and Orosz 11 checked the 72 h stability of ceftriaxone sodium and metronidazole hydrochloride in i.v. admixtures at room temperature, but metronidazole was tested at higher concentrations (7.5 and 15 mg/mL). For high metronidazole concentration, the authors observed slight immediate precipitation when ceftriaxone and metronidazole were mixed. Metronidazole at lower concentration when mixed with ceftriaxone (10 mg/mL) was stable for 24 hours at 24 to 26°C and for 72 hours at 4 to 6°C. In another study, metronidazole at concentration of 5 mg/mL in 0.9% w/v sodium chloride, in conjunction with cefotaxime sodium, was stable for 72 hours at 8°C in an i.v. admixture prepared from commercially available injectable formulations. The metronidazole concentration was within 93% to 102% of its initial content. 17 In the study by Nolin et al, 10 metronidazole was stable in all samples for 336 hours, retaining ≥94% of its initial concentrations at both 4°C and 23°C. No significant differences in metronidazole concentrations were observed between temperatures or between mixtures and controls, indicating that the presence of cefepime did not affect its stability.
Metronidazole has been used in diluted aqueous solutions for intraperitoneal lavage in surgical settings, including studies by Saha 18 and by Pooja et al, 19 where the antibiotic was added to saline irrigation fluid without precise reporting of the final concentration. Based on similar study designs, the resulting concentrations are typically in the sub-milligram per milliliter range (approximately 0.5 mg/mL), although physicochemical stability was not assessed in these studies. The concentrations investigated in the present study (0.1 and 0.6 mg/mL) are therefore within or close to this clinically relevant range, providing novel data on the stability of diluted metronidazole preparations.
Although the protection from light was not necessary to maintain stability in the Nolin et al 10 study during the recommended timeframe (72 hours) they tested, in our study the dilutions were protected from light. As reported by Chen et al, 20 metronidazole in aqueous solution is photosensitive, which can result in the formation of N-(2-hydroxyethyl)-5-methyl-l,2,4-oxadiazole-3-carboxamide.
This study has several limitations. First, only two concentrations and two storage temperatures were evaluated. Higher temperatures, such as those encountered in neonatal incubators, may also be clinically relevant. Second, the analytical method used in this study was not demonstrated to be stability-indicating; therefore, the presence of potential degradation products cannot be excluded. As metronidazole concentrations remained within the predefined acceptance limits throughout the study period, the findings should be interpreted as evidence of concentration stability under the tested conditions, supported by visual assessment of physical compatibility, rather than as a comprehensive stability-indicating assessment. Third, microbiological stability was not assessed, as the solutions were assumed to be prepared under aseptic hospital pharmacy conditions. Finally, additional physicochemical parameters, such as pH and osmolality, were not evaluated. These aspects should be addressed in future studies. Although a 10% degradation threshold is widely used in the literature, it is not universally applicable and should be interpreted in the context of the drug, formulation, and potential degradation products. Methodological guidance for hospital pharmaceutical preparations also indicates that concentration changes alone may not fully reflect stability, and additional physicochemical factors should be considered.21,22
Conclusions
In conclusion, our results indicate that metronidazole solutions at concentrations of 0.1 and 0.6 mg/mL remained within the predefined acceptance limits for up to 48 hours at room temperature and under refrigeration, maintaining ≥90% of the initial concentration. These results support safe short-term storage and preparation of diluted metronidazole in neonatal hospital practice.
Supplemental Material
sj-docx-1-hpx-10.1177_00185787261462798 – Supplemental material for Stability of Diluted Intravenous Metronidazole in 0.9% Sodium Chloride
Supplemental material, sj-docx-1-hpx-10.1177_00185787261462798 for Stability of Diluted Intravenous Metronidazole in 0.9% Sodium Chloride by Grzegorz Szynkaruk, Marta Puchalska, Kacper Osuch, Maria Miotk, Wiktoria Ziaja, Daria Sygnecka, Marta Karaźniewicz-Łada and Joanna Sobiak in Hospital Pharmacy
Supplemental Material
sj-xlsx-2-hpx-10.1177_00185787261462798 – Supplemental material for Stability of Diluted Intravenous Metronidazole in 0.9% Sodium Chloride
Supplemental material, sj-xlsx-2-hpx-10.1177_00185787261462798 for Stability of Diluted Intravenous Metronidazole in 0.9% Sodium Chloride by Grzegorz Szynkaruk, Marta Puchalska, Kacper Osuch, Maria Miotk, Wiktoria Ziaja, Daria Sygnecka, Marta Karaźniewicz-Łada and Joanna Sobiak in Hospital Pharmacy
Footnotes
Author Contributions
Grzegorz Szykaruk (investigation), Marta Puchalska (conceptualization, writing—review and editing), Kacper Osuch (investigation), Maria Miotk (investigation), Wiktoria Ziaja (investigation), Daria Sygnecka (investigation), Marta Karaźniewicz-Łada (conceptualization, writing—review and editing, supervision), Joanna Sobiak (conceptualization, methodology, data curation, project administration, writing—original draft preparation).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and analyzed during the current study are available from the corresponding author on request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.