
Abstract
Objective:
The extent to which individual differences in fine motor abilities affect indoor safety and efficiency of human-wheelchair systems was examined.
Background:
To reduce the currently large number of indoor wheelchair accidents, assistance systems with a high level of automation were developed. It was proposed to adapt the wheelchair’s level of automation to the user’s ability to steer the device to avoid drawbacks of highly automated wheelchairs. The state of the art, however, lacks an empirical identification of those abilities.
Method:
A study with 23 participants is described. The participants drove through various sections of a course with a powered wheelchair. Repeatedly measured criteria were safety (numbers of collisions) and efficiency (times required for reaching goals). As covariates, the participants’ fine motor abilities were assessed.
Results:
A random coefficient modeling approach was conducted to analyze the data, which were available on two levels as course sections were nested within participants. The participants’ aiming, precision, and arm–hand speed contributed significantly to both criteria: Participants with lower fine motor abilities had more collisions and required more time for reaching goals.
Conclusion:
Adapting the wheelchair’s level of automation to these fine motor abilities can improve indoor safety and efficiency. In addition, the results highlight the need to further examine the impact of individual differences on the design of automation features for powered wheelchairs as well as other applications of automation.
Application:
The results facilitate the improvement of current wheelchair technology.
Keywords
Introduction: Motivation and State of the Art
When human-automation systems fail, accident investigators often conclude that the “human factor” was responsible (Hollnagel, 1993): In the 1960s, between 20% and 30% of system failures in the general systems domain were attributed to a human (Robinson, Deutsch, & Rogers, 1970). Already in 1990, 90% of system failures were traced back to human error (Swain, 1990).
One such general system is a powered wheelchair. According to the National Center for Health Statistics (LaPlante, Hendershot, & Moss, 1992), about 1.41 million people in the United States depend on a wheelchair. About 3.3% of this population suffers from a serious indoor accident related to the use of their wheelchair per year (Calder & Kirby, 1990). Samira and Kirby (1994) examined the accidents reported to the National Electronic Injury Surveillance System between 1986 and 1990. The results indicated an average of about 37,000 wheelchair accidents and 52 fatalities per year—both numbers showing significant increases over the years. Calder and Kirby (1990) also analyzed the death certificate database of the National Information Clearinghouse of the Consumer Product Safety Commission between 1973 and 1987. According to these analyses, 11% of all fatal wheelchair accidents were collisions.
An illustrative example for an indoor collision resulting in serious injuries or even death is one in which a wheelchair user exits an elevator backward and falls down a flight of stairs. Similarly, serious injuries may result if a wheelchair falls over. This may happen if a wheel gets blocked by a rag or carpet or if a wheelchair becomes unstable because of sudden changes in the floor’s friction.
Besides these safety issues, another major drawback of today’s powered wheelchairs is efficiency (Bateni & Maki, 2005; Chase & Bailey, 1990; Fehr, Langbein, & Skaar, 2000). According to analyses of questionnaire data from physicians (Fehr et al., 2000) and of case study reports of patients (Chase & Bailey, 1990), people in need of a wheelchair required lengthy training to learn how to steer this device. In addition, experimental analyses of indoor driving behavior of wheelchair users demonstrated that it took very long to reach a goal, which was exhausting and tiring (Jipp, Bartolein, & Badreddin, 2009b).
To enhance the indoor safety and efficiency of human-wheelchair systems, a number of research efforts have emerged. First, methods developed in the field of robotics were suggested, adapted, and implemented on (semi)autonomous wheelchairs. An example is the collision avoidance algorithm, which Bell, Borenstein, Koren, and Jaros (1994) implemented on a wheelchair.
Second, researchers (Lankenau & Röfer, 2000) developed wheelchair-specific algorithms (e.g., wall following, door passage) to automate the system’s functionality especially in dangerous situations. To provide comprehensive support, intention estimation algorithms were implemented, which judge the next goal position of the wheelchair user and drive to it autonomously (Bartolein, Wagner, Jipp, & Badreddin, 2008; Demeester, Nuttin, Vanhooydonck, & Van Brussel, 2003). Demeester et al. (2003) extrapolated the route indicated by the user’s joystick input and compared it with potentially requested paths to goals in an indoor environment. Bartolein et al. (2008) interpreted the gaze behavior of a wheelchair user to judge either the desired movement direction (i.e., right, left, or straight) or the movement’s goal position (i.e., object in the environment). By applying collision avoidance and navigation algorithms, the wheelchair drove the user along the estimated direction or to the predicted goal position autonomously.
To summarize, the level of automation (cf. Endsley & Kaber, 1999) has increased from manual operation to nearly autonomous wheelchairs. However, research in other application areas has demonstrated that a high level of automation is not necessarily better in the long run (cf. Sarter, Woods, & Billings, 1997). This is the case as operating a highly autonomous system can result in a loss of situation and/or system awareness or in skill degradation (Norman et al., 1988; Wickens, 1994).
A loss of manual skills is especially critical for wheelchair users as it might generalize to other areas of personal life and, as a consequence, result in a reduction of independence (Jipp, Bartolein, & Badreddin, 2009a). To tackle this problem, Jipp et al. (2009a) proposed an indoor wheelchair system in which the level of automation is adaptive to the user’s ability to steer the device. Here, level of automation refers to the number and type of autonomous behaviors (e.g., intention estimation, navigation, collision avoidance) currently switched on or off. Such an adaptive wheelchair may enhance the indoor safety and efficiency of human-wheelchair systems by automating as many functions as necessary without risking skill degradation.
Research Question and Hypotheses
As addressed above, the technology exists to enhance the indoor safety and efficiency of human-wheelchair systems by making them adaptive to user abilities. Unfortunately, more research is needed to identify the abilities that contribute to human-wheelchair performance. Therefore, the focus of this study was on investigating individual differences and their impact on human-wheelchair performance.
Fine motor abilities certainly affect the safety and efficiency of human-wheelchair systems. In general, fine motor abilities influenced motor responses that required a high level of accuracy and speed but a low level of power (Meinel & Schnabel, 1976; Teipel, 1988). These motor responses involved fingers, arms, and hands (Schoppe, 1974) and required only minor (if any) information processing demands (Ackerman, 1990). These characteristics of motor responses are also valid for wheelchair operation:
A wheelchair reacts immediately to minor changes in the joystick’s input signal. Hence, accurate joystick movements are necessary to maintain control of the wheelchair.
The joystick can be moved only within a relatively small movement space, and the power requirements are small.
The joystick is operated with the use of the hands and fingers.
Hence, fine motor abilities should affect wheelchair operation.
Fine motor abilities demonstrated their predictive validity across different tasks: For example, performance differences between the dominant and the nondominant hand were explained by fine motor abilities (Guldner, Mader, & Zeltner, 1980). Similarly, ability differences predicted performance variations between patients without and patients with disorders of the central nervous system (Hamster, 1980a). Finally, Ackerman, Ciancolo, and Bowen (1999) predicted individual performance differences when executing a dentistry task with individual differences in fine motor abilities.
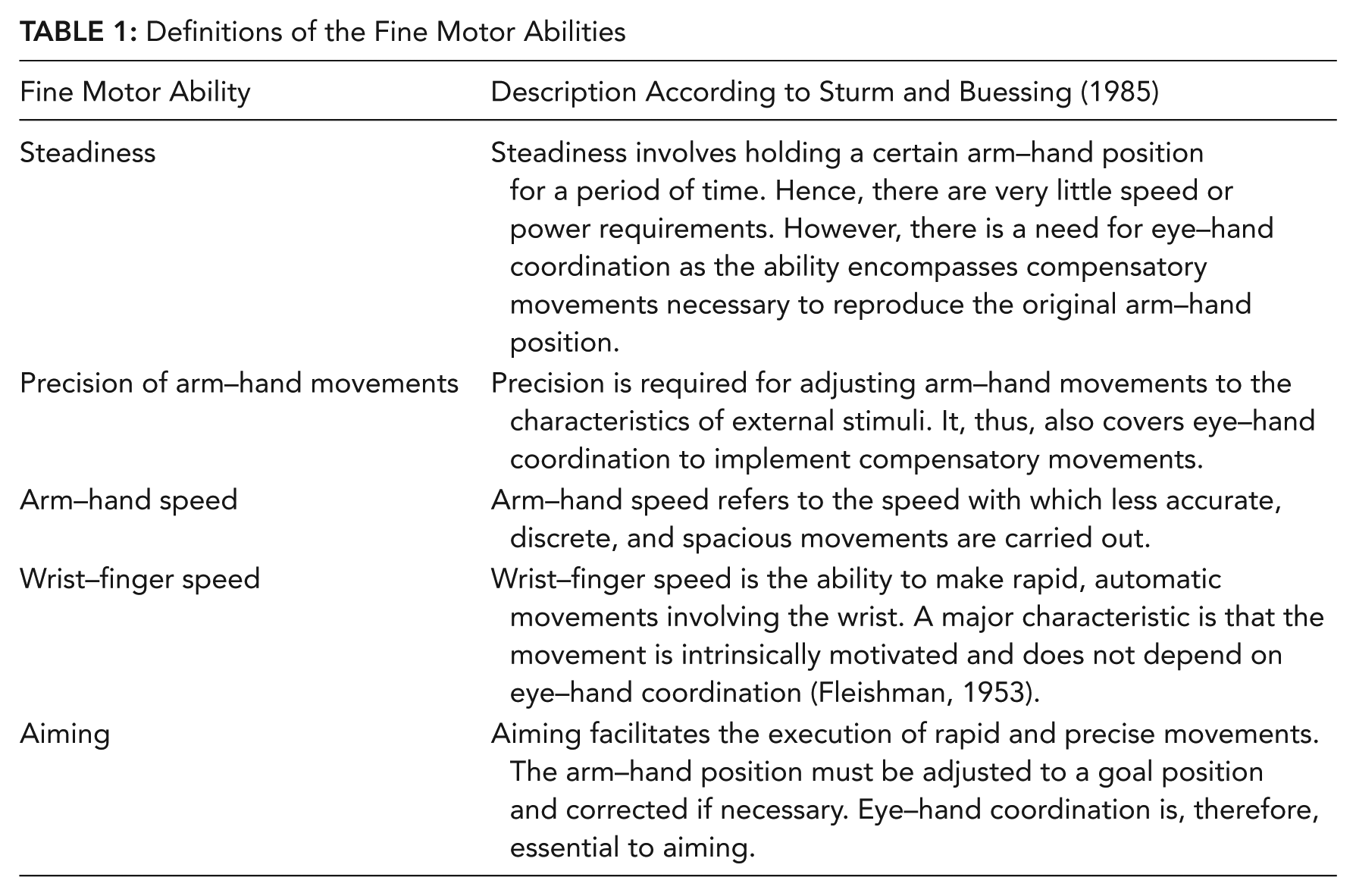
The structure of fine motor abilities was investigated by a number of researchers (Drowatzky & Zuccato, 1967; Fleishman & Parker, 1962; Keele & Hawkins, 1982). On the basis of data analyses, Sturm and Buessing (1985) identified five fine motor abilities (see Table 1). These abilities were drawn on in this study as they were expected to cover the convergent and divergent validity of human-wheelchair performance (for the need to cover both validities, see Trochim, 1999):
Steadiness (ST) should not influence wheelchair operation, as driving through a realistic indoor environment should not require a stable arm–hand position.
The precision of arm–hand movements (PR) should affect wheelchair operation. More specifically, PR should be required for reacting to minor deviations from an envisioned route with compensatory movements. Such deviations occur, for example, because of slippage, which biases the translation of the joystick signal into wheelchair movement.
Arm–hand speed (AH) should be needed to steer a wheelchair with a joystick, as AH should be necessary for the execution of less accurate movements with the arm and hand to drive in less cluttered environments.
Wrist–finger speed (WF) should influence wheelchair operation as the accuracy of the input command, which translates into the wheelchair’s velocity, does not need to be precise, especially in spacious environments.
Aiming (AI) should not influence wheelchair operation. Although rapid and precise movements might be required for steering a wheelchair, aiming does not involve the arm–hand position but instead the wrist.
Definitions of the Fine Motor Abilities
To summarize, it was hypothesized that PR, AH, and WF would be related to the safety and efficiency of indoor human-wheelchair performance. In contrast, ST and AI were hypothesized to not contribute to predicting safety and efficiency.
Method
Procedure and Apparatus
The study was carried out in a realistic office environment (for a floor plan, see Figure 1) as the focus was on indoor safety and efficiency. Within this environment, a course with 14 sections was defined. Each section was characterized by a start and a goal position. A section’s goal position served as the next section’s start position. The first section’s start was Position 1 (see Figure 1). The subsequent start positions were the Positions 4, 2, 5, 2, 4, 3, 1, 5, 3, 2, 1, 5, and 4. The last section’s goal was Position 1. The preferred route to reach goal positions (e.g., driving right or left around a table) was defined a priori and was communicated to the participants orally before they started driving to each goal position. This stepwise instruction was chosen to avoid the potential for memory to bias the results. The participants were asked to drive without colliding with walls or objects and as quickly as possible. To avoid a speed–accuracy trade-off, the participants were told to prioritize safety. These instructions were chosen because of the currently large number of indoor wheelchair accidents and because of the significant amount of time it takes to reach a goal. The latter was considered critical by wheelchair users (see the introduction).
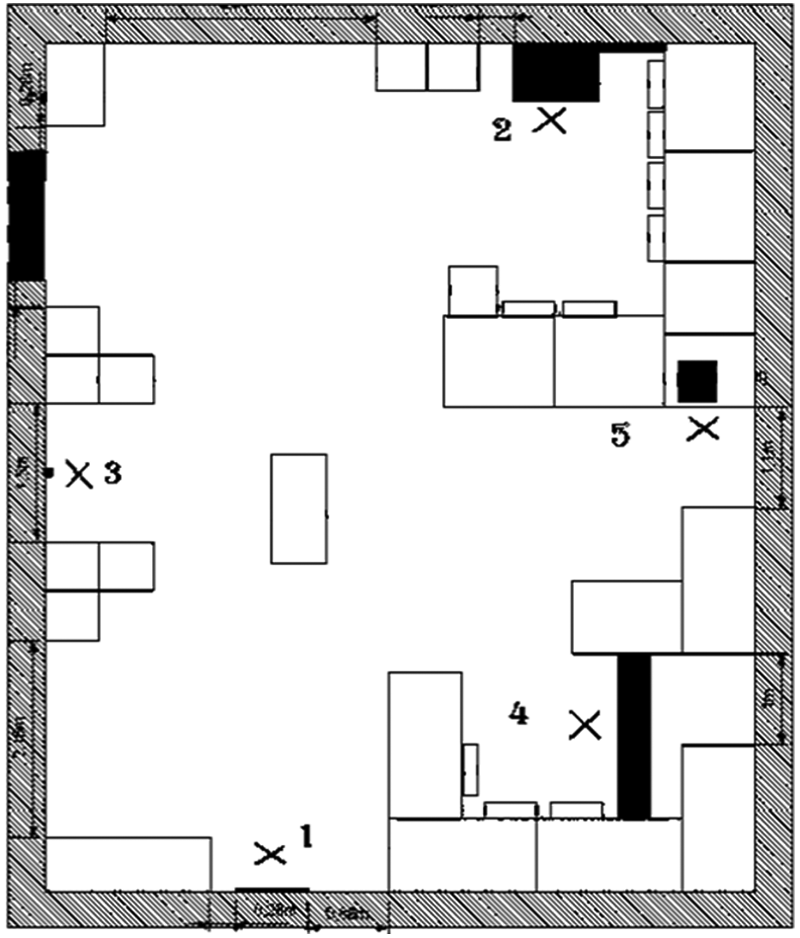
Floor plan of the office environment, in which the study took place (numbers indicate start/goal positions).
To yield valid indicators for wheelchair safety and efficiency, the path was defined to meet the following requirements:
It should evoke certain behaviors such as turning on the spot, driving around corners with different angles, and so on. These behaviors are tested in wheelchair skills tests (Kilkens, Post, Dallmeijer, Seelen, & van der Woude, 2003; Kirby, 2005). In some countries, the capability to master such behaviors determines whether persons with mobility impairments receive permission to use a powered wheelchair. These behaviors are considered representative of the behaviors essential to the safe operation of a wheelchair under expected conditions of use.
The path should evoke behaviors that may cause accidents in the real world. For instance, participants were asked to leave Position 3 backward. In this situation, a table was behind the participants, and a collision with the table was to be avoided. This situation equaled the introductory example, in which a wheelchair user exits an elevator backward and is in danger of falling downstairs. To avoid serious accidents, the stairs were replaced with a table.
The path should offset potential serial order effects by combining different start and goal positions.
To drive through the course, the participants used a commercially available powered wheelchair (Bock, n.d.), which was equipped with additional hardware and software (see Figure 2). More specifically, ultrasonic sensors were mounted to measure distances to objects in the environment. In addition, a touch screen was attached to the armrest for human-wheelchair communication. This feature was switched off during the study. The original joystick was used to steer the wheelchair. Two control PCs located underneath the wheelchair’s seat were mounted for data recording (for a description of the prototype, see Bartolein, Wagner, Jipp, & Badreddin, 2007). The following data were recorded per participant and per course section:
The numbers of collisions were registered as indicators for safety. This variable was selected because of the currently high number of indoor wheelchair collisions.
The time in seconds required for reaching a goal was measured as an indicator of efficiency. Time was chosen as it was considered critical by wheelchair users.

Wheelchair prototype used for driving.
After finishing the course, participants filled out a questionnaire and completed four items of the Motor Performance Test (MPT; Neuwirth & Benesch, 2004):
The line-tracing item requested routing a stylus along a line, which was cut into a disc, as fast as possible without touching the line’s bottom or rim.
The steadiness item required holding a stylus within a hole with a diameter of 5.8 mm without touching the hole’s rim or bottom for 30 s.
The aiming item asked participants to touch 20 metal circles successively as fast as possible.
The tapping item requested hitting a squared metal plate with a side length of 40 mm as often as possible in 32 s.
While the participants executed these items, performance indicators such as the number and duration of mistakes were measured automatically and used to calculate t values for the ST, PR, AH, WF, and AI scales.
The MPT’s scales achieved appropriate reliability (Hamster, 1980b; Ringendahl, 2002; Sturm & Buessing, 1985) and validity estimates (Kraus, Klotz, Fischer, & Przuntek, 1987; Motomura, 1994; Neuwirth & Benesch, 2004; Ringendahl, 2002) and, thus, satisfy standards of psychometric quality criteria.
The questionnaire assessed biographical variables and experiences with driving cars, motor boats, and scooters on a 5-point Likert-type scale. These experiences were assessed as positive transfer might bias the results (cf. Goska & Ackerman, 1996). Positive transfer was expected as powered wheelchairs react similar to other mobility devices. Although the impact of positive transfer was not the focus of this study, factors expected to contribute to positive transfer were assessed to help improve the model fit.
The time required for the study completion ranged from 30 to 60 min. Before data acquisition, participants gave informed consent. After finishing, participants received a monetary allowance of €5 or course credit.
Participants
The participants were recruited at the Universities of Heidelberg and Mannheim (Germany) and formed a sample of convenience. Because of health concerns related to testing people with mobility disabilities in a wheelchair prototype, which could not be adjusted to specific needs (because of the PCs underneath the wheelchair’s seat, its height could, for instance, not be adjusted), it was decided to recruit healthy individuals.
To account for skill acquisition, the participants were first given a verbal description of the wheelchair and its operation. Next, the participants were allowed to drive around the test environment until they indicated that they mastered steering the wheelchair. The wheelchair was then driven to the start position of the first section, and data recording was initiated.
After the participants’ recruitment and the exclusion of two participants because of technical problems, a sample size of N = 23 resulted for data analyses (43.5% male, 56.5% female). The average age was 23.00 years (SD = 4.26 years). Two participants did not have a car driver’s license. As none of the participants had experience with driving motor boats or scooters, these variables were not considered in the analyses.
Data Analyses and Results
Data Analytic Strategy
To answer the hypotheses, a multilevel random coefficient modeling approach (MRCM) was chosen (Hox, 2010; Tabachnick & Fidell, 2007) and implemented through SPSS MIXED (Version 16). MRCM is also known as mixed modeling (Littell, Milliken, Stroup, & Wolfinger, 1996), multilevel regression modeling (Hox, 2010), and hierarchical linear modeling (Raudenbush & Bryk, 1986). MRCM was favored in contrast to other analytic procedures such as multiple linear regression as it allows analyzing nested data with a high level of accuracy and generalizability simultaneously (cf. Nezlek, Schroeder-Abe, & Schuetz, 2006). Statistically, MRCM requires neither the assumption of homogeneity of residuals nor the assumption of independence of errors to be valid (Tabachnick & Fidell, 2007). Con-ceptually, MRCM enables avoiding pitfalls such as the ecological or the atomistic fallacy (Hox, 2010). MRCM is, thus, advocated by researchers (Bryk & Raudenbush, 1992; Kenny, Kashy, & Bolger, 1998; Kreft & de Leeuw, 1998) as the appropriate method to analyze data on multiple levels including repeated measurements (Nezlek et al., 2006).
Data on two levels were present here as course sections (Level 1) were nested within participants (Level 2). Both criteria (numbers of collisions, times required for driving) were assessed on Level 1. The Level 1 covariate was the standardized order in which the course was completed. The Level 2 covariates were the participants’ fine motor abilities and car driving experience.
Preanalyses
Descriptive statistics of the participants’ fine motor abilities (Table 2) showed, first, that ceiling effects were not present. Second, they enabled comparison of the fine motor abilities of this sample with the ones of long-term wheelchair users (cf. Jipp, 2007). Such comparisons revealed only marginal differences.
Descriptive Statistics of the Fine Motor Abilities
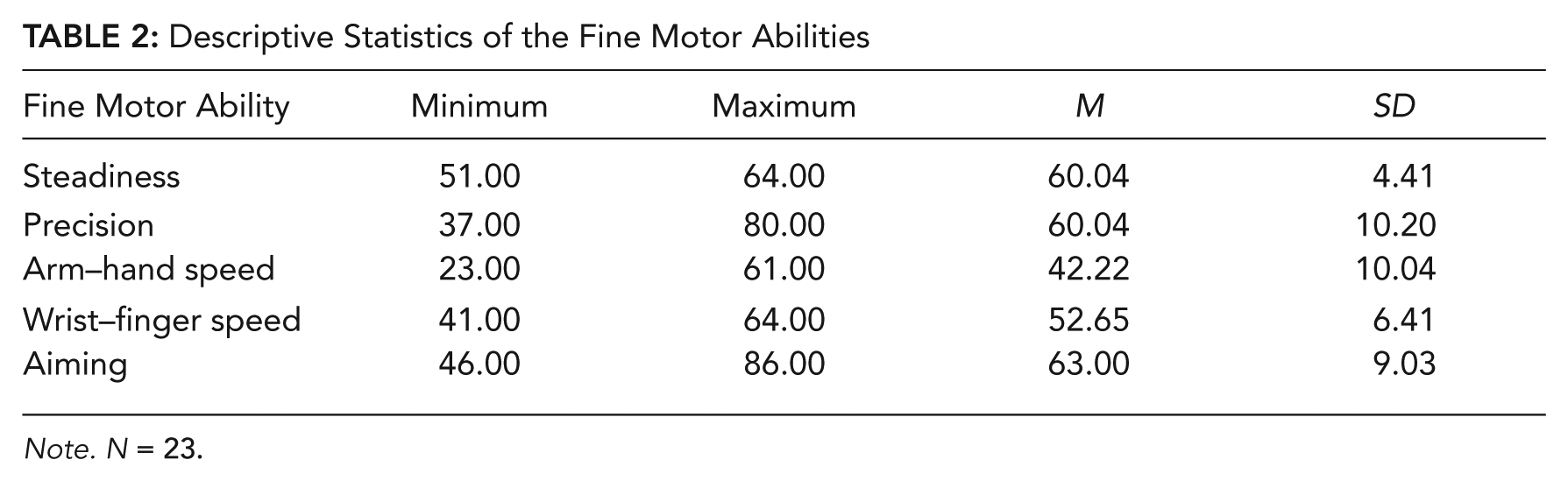
Note. N = 23.
Descriptive statistics of the criteria showed that, on average, between zero and five collisions occurred per section. Reaching a goal typically required between 20 and 50 s of driving. When aggregated over sections, the two criteria were not significantly correlated, r = −.29 (p > .05, two-tailed).
Finally, preanalyses confirmed the absence of other potential problems, including skewness in the distributions of the variables, multicollinearity, outliers, and missing data.
Multilevel Random Coefficient Modeling
In a first step, unconditional means models were executed to confirm (a) the need to conduct multilevel analyses and (b) the need to add covariates (Peugh & Enders, 2005). The full maximum likelihood method was used for modeling as it yields asymptotically unbiased, consistent, and efficient parameter estimates (Tabachnick & Fidell, 2007).
The estimates of the unconditional means models for the numbers of collisions and the times required for driving (see Table 3) were used to calculate the intraclass correlation coefficients (ρ) that reached ρ = .39 for the numbers of collisions and ρ = .44 for the time measures. Hence, 39% and 44% of the criteria’s variances could be traced back to variability between participants. This highlighted the need to apply MRCM as otherwise the actual Type I error rate would be increased dramatically because of the violation of the assumption of independence underlying, for instance, multiple linear regression (cf. Barcikowski, 1981). The results further showed the need to add covariates to the models: The estimates of the covariance parameters indicated heterogeneity between and within participants (i.e.,
Parameter Estimates of the Unconditional Means Models
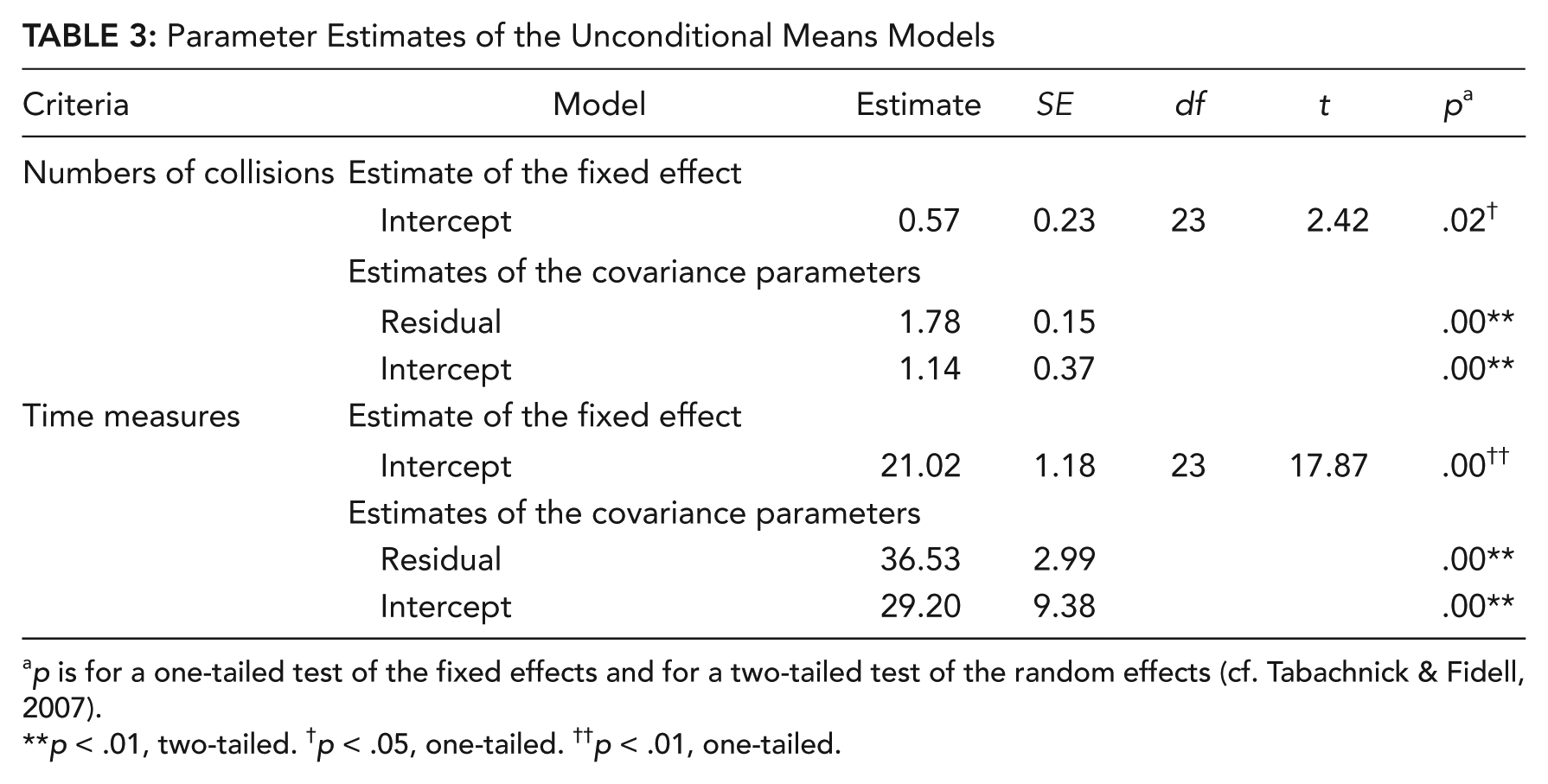
p is for a one-tailed test of the fixed effects and for a two-tailed test of the random effects (cf. Tabachnick & Fidell, 2007).
p < .01, two-tailed. †p < .05, one-tailed. ††p < .01, one-tailed.
In a second step, conditional means models were executed. To reduce intraindividual and interindividual variability, the noncentered Level 1 and Level 2 covariates were added. The intercepts of the Level 2 covariates were fixed. In contrast, the intercept of the Level 1 covariate was allowed to vary randomly between participants. Cross-level interactions were not considered.
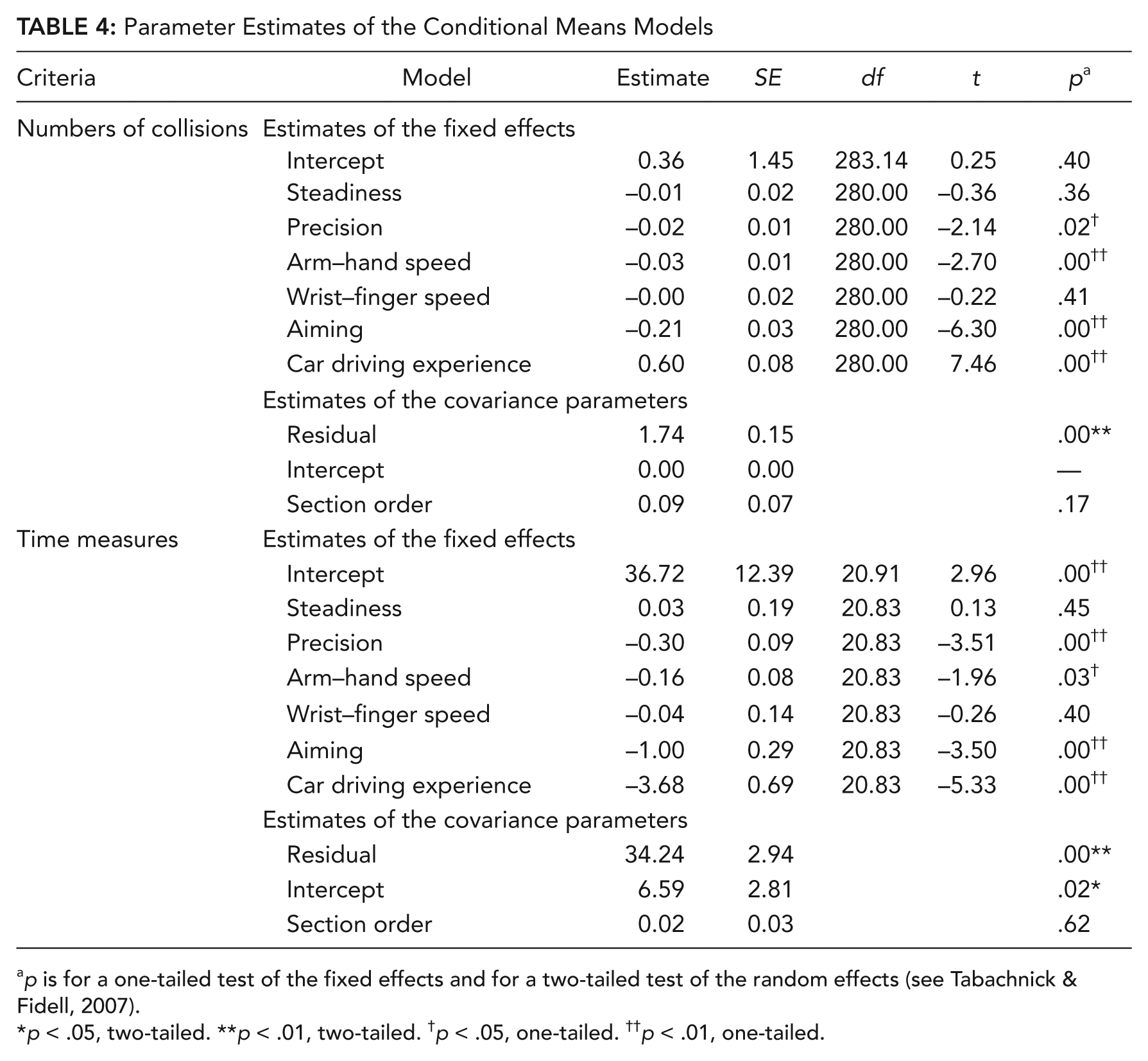
The results of the modeling, for which the full maximum likelihood method was chosen as well, are summarized in Table 4.
Parameter Estimates of the Conditional Means Models
p is for a one-tailed test of the fixed effects and for a two-tailed test of the random effects (see Tabachnick & Fidell, 2007).
p < .05, two-tailed. **p < .01, two-tailed. †p < .05, one-tailed. ††p < .01, one-tailed.
Findings regarding the numbers of collisions
The following fine motor abilities contributed significantly (p < .05) to the prediction of the numbers of collisions (see Table 4):
PR was related to the numbers of collisions with γ0PR = −0.02, t(280) = −2.14, p < .05.
AH was related to the numbers of collisions with γ0AH = −0.03, t(280) = −2.70, p < .01.
AI was related to the numbers of collisions with γ0AI = −0.21, t(280) = −6.30, p < .01). This estimate was larger than the ones of PR and AH.
The estimates’ negative signs showed that the numbers of collisions decreased with better PR, AH, and AI.
Post hoc power analyses were conducted for ST and WF to investigate whether the estimates were not significant because of low power or because of the absence of an effect. The analyses were conducted as described by Hox (2010) and revealed a power of 1 – β = .98 (ST) and of 1 – β = .84 (WF) assuming a real effect size of η2 = .10 and a Type I error rate of α = .05.
Findings regarding the time measures
The following fine motor abilities added significantly to the prediction of the criterion (see Table 4):
PR was related to the time measures with γ0PR = −0.30, t(20.83) = −3.51, p < .01.
AH was related to the time measures with γ0AH = −0.16, t(20.83) = −1.96, p < .05.
AI was related to the time measures with γ0AI = −1.00, t(20.83) = −3.50, p < .01. The estimate was larger than the ones of PR and AH.
The estimates’ negative signs showed that the time measures decreased with better PR, AH, and AI.
Again, neither ST nor WF contributed to predicting the time measures. Post hoc power analyses revealed powers of 1 – β = .84 (ST) and of 1 – β = .85 (WF). Hence, the insignificance of the two estimates could hardly be traced back to low power. The calculations assumed a real effect size of η2 = .10 and a Type I error rate of α = .05 and followed the propositions of Hox (2010).
Postanalyses
Comparing the residual estimates of the covariance parameters of the unconditional and of the conditional means models (Table 3 and Table 4) revealed that adding the covariates reduced the variances between and within persons for the numbers of collisions (
The Akaike information criteria (Akaike, 1987) allowed comparison of the unconditional and conditional means models descriptively (Hox, 2010):
Regarding the numbers of collisions, the Akaike information criterion of the unconditional means model was AIC = 1157.88, and the one of the conditional means model was AIC = 1031.60. This reduction showed that the conditional means model was better.
Regarding the time measures, the Akaike information criterion reached AIC = 2136.00 for the unconditional means model and AIC = 1922.31 for the conditional one. Again, the conditional means model was better.
Comparing the unconditional and conditional means models with inferential statistics showed that the differences were significant, with χ2(7, N = 322) = 140.29, p < .001 for the numbers of collisions and with χ2(7, N = 322) = 227.64, p < .001 for the time measures.
Discussion, Conclusions, and Implications
The results suggest that major fine motor abilities influence indoor safety (number of collisions) and efficiency (time) of a human-wheelchair system and provide some support for the hypotheses.
As hypothesized, the participants’ AH and PR were significantly associated with the numbers of collisions and the times measures. By considering the definitions of these abilities, the effects can be interpreted as follows: Driving a wheelchair indoors requires executing less accurate, discrete, and spacious arm–hand movements and reacting to deviations from a predefined route with compensatory movements. This raises the assumption that AH is needed to steer and PR to control a wheelchair when using the terminology of control theory. The need for control may derive from unexpected wheelchair movements such as slippage. In contrast, the need for steerage may result from intentional, user-initiated movements.
In accordance with the hypotheses, ST did not add to the prediction of human-wheelchair performance. Post hoc power analyses showed that this is the result of a small or a nonexisting effect. Hence, indoor wheelchair operation does hardly involve maintaining a certain arm–hand position for a longer time. This result might, however, be an effect of the situation chosen for this study. Driving a wheelchair in less cluttered, outdoor environments might require stable arm–hand positioning. There, longer distances may need to be traveled with the same rotational and translational speed so that the joystick may need to be kept in the same position for a longer time period.
The importance of the arm–hand position for human-wheelchair performance is highlighted by the results regarding AI and WF: AI added to the prediction of the numbers of collisions and the time measures. Although unexpected, these effects were the largest ones. They show that the arm–hand position is involved to a larger extent than the wrist. This conclusion is supported by the nonsignificant results regarding WF.
The data analyses further revealed that adding the Level 2 covariates to the model reduced interindividual criteria variation. Further reduction may be achieved by considering additional Level 2 covariates such as age, skill acquisition, and experience with other mobility devices such as scooters or bicycles. In addition, the effect of car driving experience on human-wheelchair performance needs further theoretical and empirical analyses, as car driving experience was only marginally covered within this study.
The intraindividual criteria variation was hardly reduced with inserting the Level 1 covariate section order. Hence, future research needs to focus on identifying additional Level 1 covariates affecting human-wheelchair performance. One such covariate may be navigation difficulty, as it certainly varied throughout the course. Other Level 1 covariates, which were kept constant in this study, may be the method with which the wheelchair is steered (e.g., joystick vs. switches) and its characteristics (e.g., joystick sensitivity, number of switches).
In addition, cross-level interactions need to be considered. It can, for instance, be assumed that the degree to which fine motor abilities influence the criteria depends on the difficulty of the course navigation. Then, cross-level interactions will explain additional criteria variance.
Future studies also need to focus on analyzing further human-wheelchair performance variables and their interrelationships. Although PR, AH, and AI were related successfully to the numbers of collisions, the criterion’s range was limited. In the future, types of collisions (classified, e.g., according to their impact) could also be considered, in addition to further indicators such as the exact distances to objects. In addition, a potential speed–accuracy trade-off of collisions and time measures needs to be investigated. In this study, I attempted to reduce the role of a speed–accuracy trade-off by explicitly instructing participants to focus on accuracy, not speed. Still, a negative but nonsignificant correlation between the two criteria was found. This indicates that the participants who caused more collisions drove faster, which points to a potential speed–accuracy trade-off.
Still, the modeling revealed that some fine motor abilities affect human-wheelchair performance—at least in the current sample for this study’s course. As in any controlled environment, the extent to which the results can be generalized to other settings and/or persons including long-term wheelchair users needs to be discussed. To yield a high level of external validity, the course was designed to evoke behaviors that are covered in wheelchair skills tests and that may cause serious indoor accidents. In addition, this sample’s fine motor abilities hardly differed from the ones of long-term wheelchair users. These are indicators of the results’ external validity. Still, future research needs to focus on replicating the results in different situations (e.g., realistic home environment, outdoors) and with persons with varying levels and degrees of disabilities.
The original motivation for this study was to identify the fine motor abilities to which an indoor wheelchair system should be adaptive. These fine motor abilities are AI, AH, and PR, as better abilities resulted in better human-wheelchair safety and efficiency. The effects were largest for AI, such that it might bring the greatest benefit to adapt a wheelchair system’s assistive functionality to the user’s AI. To make wheelchair systems safer at least indoors, future research also needs to focus on implementing and evaluating such a device.
Key Points
This study provides empirical evidence that individual differences in fine motor abilities affect the indoor safety (numbers of collisions) and efficiency (times required for reaching goal positions) of human-wheelchair systems.
These results provide evidence that adapting the level of automation of a wheelchair system to its user’s fine motor abilities reduces the number of wheelchair-related accidents and increases human–wheelchair efficiency without risking skill degradation.
Future research in this area should carefully consider the important role of individual differences when designing and implementing automated wheelchair systems.
Footnotes
Acknowledgements
This research was partially conducted while Meike Jipp was with Heidelberg University (Germany). At that time, the study was supported by a grant from the Baden-Württemberg state within the scope of the BW-FIT initiative. The author thanks Christian Bartolein and Simone Schmid for their assistance with the data collection as well as Uwe Teegen and the reviewers for many helpful ideas that shaped this article.
Meike Jipp is a researcher at the Human Factors Department of the Institute of Flight Guidance of the German Aerospace Centre. She received her PhD in psychology from the University of Mannheim (Germany) in 2008.