
Abstract
Objective:
The aim of this study was to determine how selected environmental factors affect transfers and to compare our results to the Americans with Disabilities Act Accessibility Guidelines (ADAAG).
Background:
Few data are available to support standards development related to transfers in the built environment.
Method:
Participants were 120 wheeled mobility device (WMD) users who transferred to and from a modular transfer station that consisted of a height-adjustable platform with a lateral grab bar, optional obstacle to the transfer, and an optional height-adjustable front grab bar. Maximum and minimum vertical heights of the transfer surface, maximum gap distance between the WMD and transfer surface, grab bar use, and WMD space needs were recorded.
Results:
The 95th percentile lowest and highest heights attained were similar to the median WMD seat-to-floor height (56 cm). We found that 42% (47/113) could not perform a transfer with the obstacle present. Participants transferred higher when the front grab bar was added to the setup (p = .005) and higher and lower with the front grab bar than without it when the obstacle was present in the setup (p = .003 and p = .005, respectively). We found that 95% of participants performed a transfer across an 8.9-cm gap. ADAAG recommendations fall short for the height and clear-space needs of the 50th-percentile WMD users.
Conclusion:
Revisions concerning transfer heights, gaps, clear spaces, and grab bar heights are necessary to make transfers more accessible to WMD users.
Application:
The data will be used to revise the guidelines related to transfers and to enable designers and engineers to create an environment that is more accessible.
Introduction
For users of a wheeled mobility device (WMD), to work, go to school, visit with friends, go to the movies, and engage in other meaningful societal and community activities hinges on their ability to perform essential mobility skills in the community independently (e.g., without human assistance; Toro, Koontz, Kankipati, Naber, & Cooper, 2010). Many WMD users have impaired lower limb function and rely exclusively on their arms for transfers, that is, the act of maneuvering oneself into and out of the wheelchair to and from a variety of surfaces (e.g., commodes, bathtubs, motor vehicle seats, amusement park rides). As transfers are performed on the order of 15 to 25 times a day (Finley, McQuade, & Rodgers, 2005; Gagnon et al., 2009; Pentland & Twomey, 1994), it is not surprising that they have been ranked among the most strenuous wheelchair-related activities (Bayley, Cochran, & Sledge, 1987; Drongelen et al., 2005) and are believed to be a major contributor to the development of upper-limb pain and injuries (Dyson-Hudson & Kirshblum, 2004).
The ability to perform successful independent transfers hinges on several environmental factors. Some of these factors are addressed in the Americans with Disabilities Act Accessibility Guidelines (ADAAG) and include recommendations concerning vertical height for elements where transfers are expected, clear space adjacent to the element, and grab bars (in certain cases; “ADA Accessibility Guidelines,” 2002; U.S. Department of Justice, 1994, 2010).
There is general concern that the standards may be outdated, as they were developed in the 1970s and given that mobility devices have evolved because of advances in technology and to meet the expanding demographics of those using these devices. For example, powered recline-and-tilt systems on powered wheelchairs enable those who cannot perform pressure relief maneuvers using their own upper-limb strength to do so with their system (Koontz, Brindle, Kankipati, Feathers, & Cooper, 2010). These add-ons, however, increase the size and turning diameter of the mobility system. The number of people who are obese is growing at an alarming rate, as is the bariatric wheelchair industry, which produces larger mobility systems for individuals who weigh more than 1,112 N (250 lbs; Cooper, Cooper & Boninger, 2008). Also, the standards were not based on research but on expert and consumer opinions. Moreover, in the past decade, as accessibility standards have expanded, the number of elements designed for transfer has also increased. Recent additions of provisions for recreational facilities added criteria for transfer systems in play areas, transfer systems and transfer walls in swimming pools, and amusement ride seats designed for transfer. Criteria for medical diagnostic equipment are also under development at this time.
When combing the literature for data that could guide criteria for new elements, we found very little research. An expert review of the scientific literature on independent transfers revealed a small number of studies that directly relate to the influence of transfer setup, operationally defined as environmental type factors that affect transfer (Koontz, Toro, Kankipati, Naber, & Cooper, 2011). All the studies identified in this review involved small groups of participants, and all but one of them explicitly included participants with spinal cord injury, and thus a vast majority of them would not be generalizable to other populations who perform independent transfers (Koontz et al., 2011). The studies were all primarily descriptive and focused on biomechanical aspects of the transfer. Handholds, grab bars, and other environmental fixtures designed to facilitate a transfer to a target surface were identified as lacking evidence concerning their advantages to WMD users, optimal locations, and characteristics (Gagnon et al., 2009; Koontz et al., 2011).
Research to support standards development related to transfers is greatly lacking. The overarching purpose of this study was to determine how selected environmental factors affect transfers among current community-dwelling WMD users. In particular, we aimed to investigate three key criteria that are presently included in the standards (i.e., vertical heights, clear space, and grab bar heights) and to compare our results to the portions of the ADAAG that address these criteria. A second aim of our study was to evaluate two additional factors, gaps and obstacles, which are not presently included in the standards but were thought to be important for establishing new criteria. An example of where a gap, or horizontal distance separating the mobility device and transfer element, is often present is at the loading and unloading platform for an amusement park ride. The gap here refers to the “open” space between the edge of the platform where the WMD is parked and the ride itself. The second factor concerns physical obstacles in between the WMD and target surfaces. Examples include fixtures, such as bolsters (e.g., the side edges of a ride capsule) and fixed armrests on aircraft seats, which are not mandated to be removable (“Guidelines for Aircraft,” 1988). The results of this study are essential to creating an environment that is more accessible to individuals who independently transfer.
Method
Participants
Participants were eligible to participate if they (a) were at least 18 years old, (b) were able to independently perform a transfer to and from a WMD with or without a transfer assist device, (c) owned a WMD, and (d) had been using the WMD for at least 1 year. Participants were excluded from the study if they had (a) significant upper-extremity pain or injury that would inhibit the ability to perform transfers or (b) an active or recent history of pressure sores. Participants were tested at the 24th National Disabled Veterans Winter Sport Clinic in Snowmass Village, Colorado, in March 2010 (n = 26); at the 30th National Veterans Wheelchair Games in Denver, Colorado, in July 2010 (n = 33); at the Hiram G. Andrews Center in Johnstown, Pennsylvania, in November 2010 and March 2011 (n = 19); during the U.S. Access Board In-Person Meeting in Chicago, Illinois, in September 2010 (n = 9); at the Human Engineering Research Laboratories in Pittsburgh, Pennsylvania, between June 2010 and April 2011 (n = 25); and at H. John Heinz III VA Progressive Care Center in June 2011 (n = 8). Basic demographics were collected, such as gender, and self-reported variables included age, type of disability, weight, height, and years using a WMD. The study was approved by both the Department of Veterans Affairs and the University of Pittsburgh Institutional Review Board.
Description of the Transfer Station
A custom-built, modular transfer station was designed with the use of Solid Edge 2009 software and consisted of a height-adjustable platform with a range between 25.4 and 73.7 cm at increments of 2.5 cm, a fixed backrest 64 cm wide by 43 cm high and with a 95° recline, a lateral grab bar (fixed height of 81.3 cm; Figure 1) that allowed for attaching and detaching side guards (e.g., obstacle to transfer), and an optional front grab bar of varying height (Figure 2) from 48 to 96 cm at increments of 5 cm. The grab bars’ diameter was 4 cm, and the horizontal distance between the center of the grab bar and the center-front edge of the platform was fixed at 34.3 cm. The space for the legs and feet had a fixed dimension of 37 cm deep by 57 cm wide. The dimensions of this space and other features of the station were based on the experiences of the investigators, who in preparation for this study visited local amusement parks with WMD users to observe how they transfer into and out of rides and their design features. The gap was created with plywood blocks of 8.9-cm width. The blocks were added together to increase the gap every 8.9 cm up to a maximum gap of 53.3 cm.

Transfer station initial setup.

Transfer station with front grab bar and side guard.
Experimental Protocol
For the initial setup, the platform was adjusted to be level with the participant’s WMD seat, with no side guard or front grab bar in place. The participants were asked to position themselves next to the platform as they normally would to prepare for a transfer. Each participant was asked to perform a transfer from the WMD to the station and back to the WMD. Next, participants were asked to perform five protocols in random order. Table 1 lists the protocols and summarizes the main outcome variable(s) that were measured for each protocol. Participants were asked to attempt only transfers they felt comfortable and safe doing. Participants were spotted in the event that they began to slip or fall during a transfer, in which case the transfer was declared “unattainable.” Participants were informed that they could quit the study at any time if they felt fatigue or pain that affected their ability to transfer.
Protocols and Main Outcome Variables
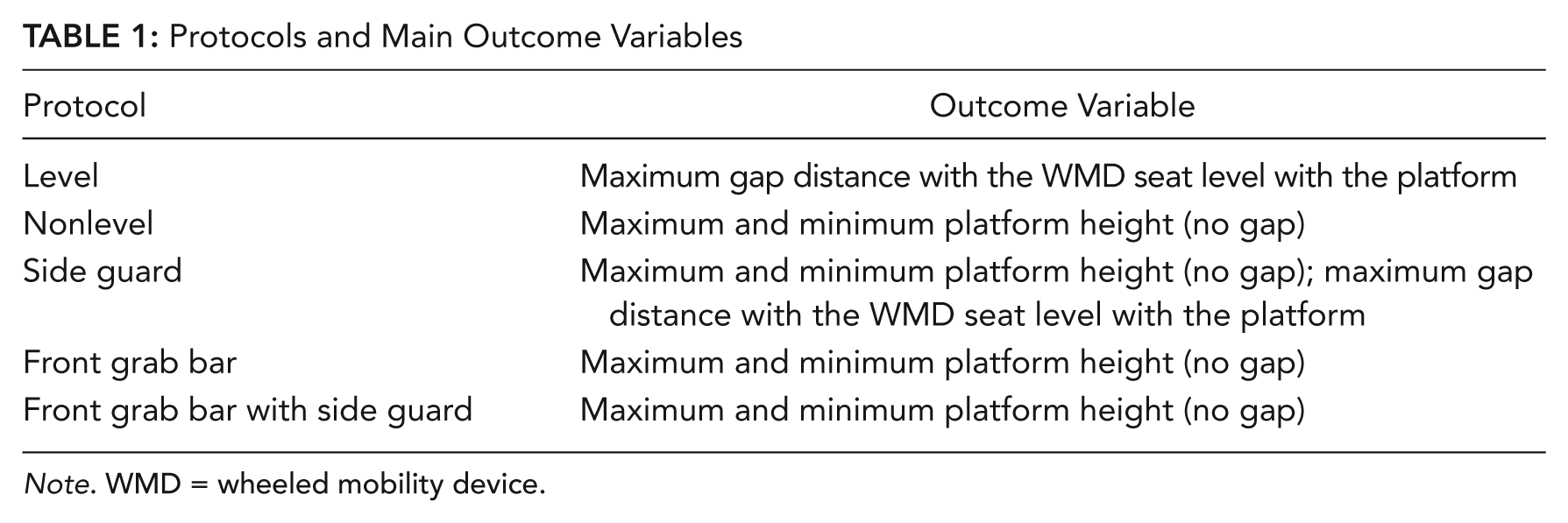
Note. WMD = wheeled mobility device.
Level
From initial setup (i.e., platform level with the WMD user’s seat height), we incrementally increased just the horizontal distance between the WMD and platform by placing plywood blocks of 8.9-cm width between the transfer station and the WMD (Figure 3). The amount of horizontal distance increased each time again depended on the participant’s perceived and observed transfer abilities. The maximum horizontal distance the participant could transfer to and from the platform was recorded.
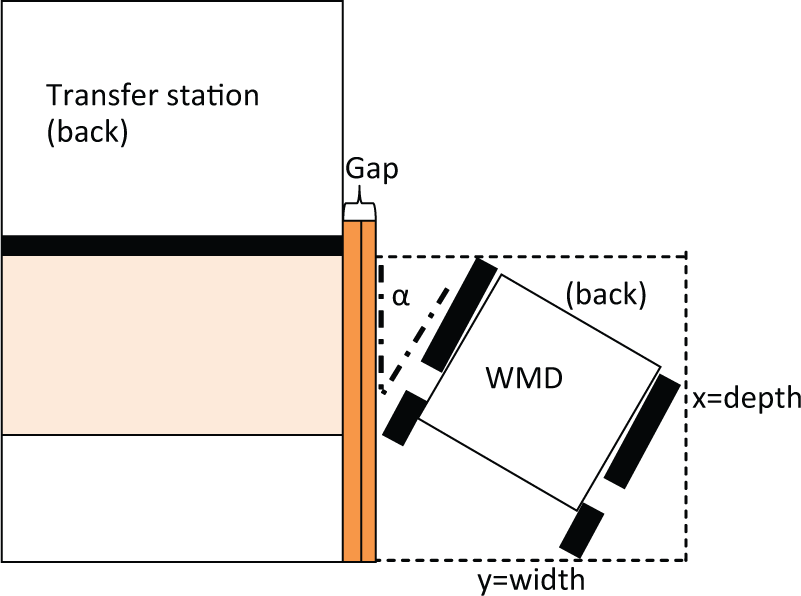
Wheeled mobility device position measures taken to calculate the overall space needed to transfer.
Nonlevel
From initial setup, the height of the platform was adjusted incrementally: higher and lower than the participant’s seat. The amount of vertical distance that the seat was raised or lowered each time depended on the participant’s perceived and observed transfer abilities. The maximum and minimum heights the participant could transfer to and from the platform were recorded.
Side guard
From initial setup, two side guards adjusted 15 cm higher than the participant’s WMD seat were attached to the station. Then the height of the platform was adjusted incrementally in height (higher and lower than the participant’s WMD seat), and the maximum transfer heights (high and low) that were attainable were recorded. Then from initial setup, the horizontal distance between the wheelchair and platform was incrementally increased, and the maximum attainable gap distance was recorded. The side guard height was adjusted to always remain at 15 cm from the WMD seat when the station was lowered and was not adjusted when the station’s height was above the height of the WMD seat.
Front grab bar
From initial setup, a grab bar in front of the platform was added. The platform was adjusted incrementally in height (higher and lower than the participant’s WMD seat), and the maximum transfer heights (high and low) that were attainable were recorded. Participants were asked to select their preferred grab bar height for (a) transferring to lower heights and (b) transferring to higher heights than their WMD seat height. The preferred grab bar height was measured between the floor and the top of the grab bar surface. They had the option to use or not use the grab bar. Front grab bar use (yes or no) and grab bar heights (if used) for the lower-height and higher-height transfers were recorded.
Front grab bar with side guard
This protocol was exactly the same as that for the front grab bar except the side guards and front bar were part of the setup.
Device positioning (x, y, α in Figure 3) was recorded one time in each protocol at the maximum and minimum transfer configurations (e.g., maximum and minimum height or maximum gap). The angle between the WMD and the transfer station (α) was defined from 0° to 180° (Figure 3). When the WMD was aligned parallel to the transfer station and the participant was facing toward the front of the station, the angle was defined as 0°; when the WMD was perpendicular to the station, the angle was defined as 90°; and when the WMD was parallel to the station but the participant was facing forward, the angle was defined as 180°.
Data Analysis
Two approaches were taken to describe the results, one descriptive and one statistical in nature. For the descriptive approach, the number of participants who attempted to perform each protocol and the number of participants who were not able to attain the transfer(s) were reported for each protocol. For those who were able to attain each protocol, percentiles (5th, 50th, and 95th) for the gap variable (level and side guard), height variable (nonlevel, side guard, front grab bar, front grab bar with side guard option), and the clear-space variable (e.g., device positioning for all protocols) were computed.
For the statistical approach, a Shapiro-Wilk normality test was performed on the gap, height, and space variables. As the results indicated that the data were non-normal, Wilcoxon signed rank tests were used to compare (a) the maximum (and minimum) attainable height with and without grab bar, (b) maximum (and minimum) attainable height with and without side guard, (c) maximum (minimum) attainable height between side guard with and side guard without grab bar, and (d) differences across gap length with and without side guard. A Friedman’s test with multiple post hoc Wilcoxon tests (applying a Bonferroni correction of p = .05/10, p = .005) was used to assess differences in the clear-space needs between the five protocols. Descriptive statistics were used to present results for front grab bar use and the optimal heights of the grab bars.
Results
Participants
The sample consisted of 96 men and 24 women with an average age of 47.7 ± 15.3 years, body mass of 77.8 ± 21.8 kg, and height of 1.70 ± 0.14 m. Participants had a broad variety of disabilities, including spinal cord injury (SCI), multiple sclerosis (MS), cerebral palsy (CP), and amputation, among others (Table 2). Of the group with SCI, 59% reported a motor incomplete injury.
Number of Participants by Self-Reported Type of Disability, WMD Type, and Gender (N = 120)
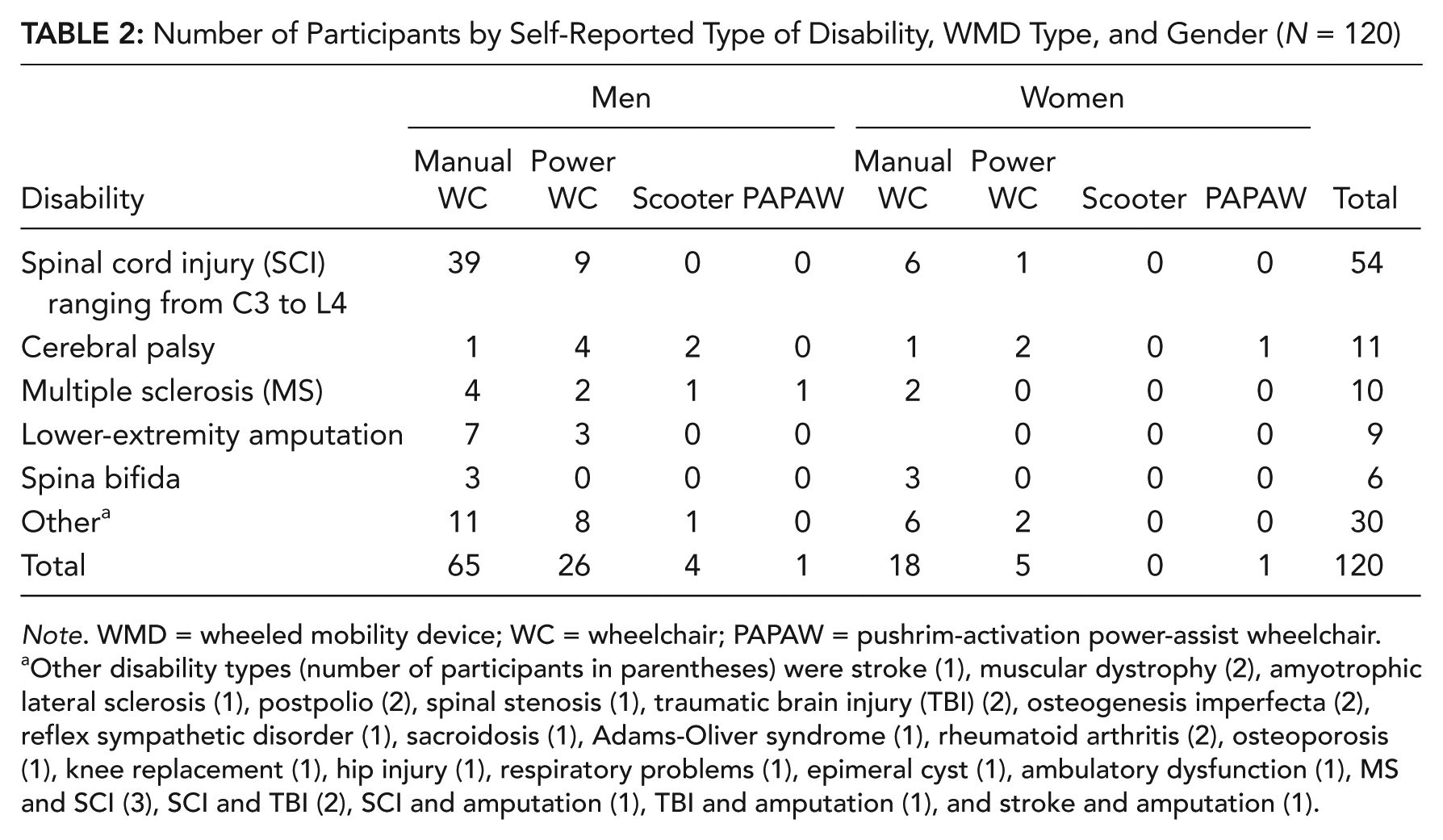
Note. WMD = wheeled mobility device; WC = wheelchair; PAPAW = pushrim-activation power-assist wheelchair.
Other disability types (number of participants in parentheses) were stroke (1), muscular dystrophy (2), amyotrophic lateral sclerosis (1), postpolio (2), spinal stenosis (1), traumatic brain injury (TBI) (2), osteogenesis imperfecta (2), reflex sympathetic disorder (1), sacroidosis (1), Adams-Oliver syndrome (1), rheumatoid arthritis (2), osteoporosis (1), knee replacement (1), hip injury (1), respiratory problems (1), epimeral cyst (1), ambulatory dysfunction (1), MS and SCI (3), SCI and TBI (2), SCI and amputation (1), TBI and amputation (1), and stroke and amputation (1).
There were 83 manual wheelchair, 31 power wheelchair, 4 scooter, and 2 power-assist users. The sample had been using a WMD for 14.9 ± 12.1 years, with a range from 1 to 59 years. Wheelchair seat plus the cushion height measured at the edge was 55 ± 3 cm, median was 56 cm, and range was 43 to 64 cm. The overall width and length of the WMDs were 67.3 ± 6.1 cm and 94.0 ± 15.2 cm, respectively. Of the total, 18% (22/120) reported using assistive technology for transfers: 14 used a transfer board; 3, lifts; 3, canes; and 2, walkers.
Of the 120 participants, 4 enrolled in the study met inclusion criteria for independent transfer but were unable to transfer to and from the station because of space constraints and their method of approach. All these participants were power wheelchair users except for Participant S4, who used a manual wheelchair (Table 3). Participant S3 used a transfer board in his transfers. The remaining 116 participants completed all or portions of the study (Figure 4). The reason for not completing all portions of the study was mainly time constraints. A few participants ended the study early because they experienced fatigue or pain affecting their ability to transfer. Randomization of protocols and breaks between transfers controlled for any minor fatigue-related effects for those who remained in the study.
Characteristics of the Four Participants Who Were Not Able to Attain Any Transfers
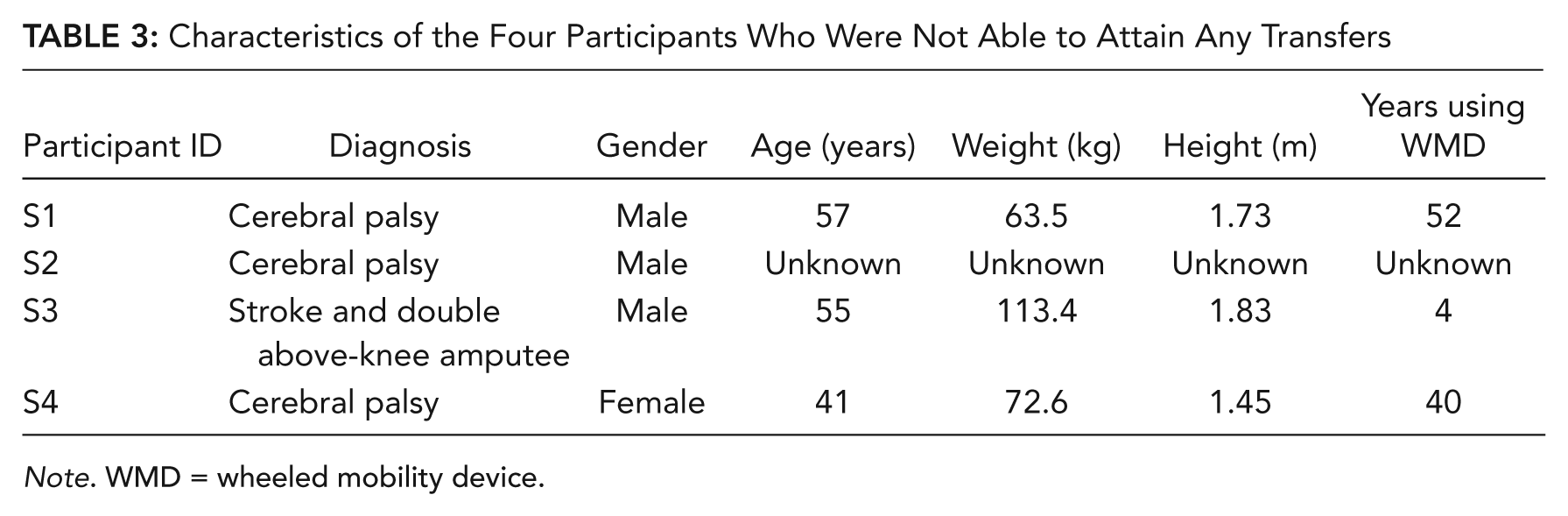
Note. WMD = wheeled mobility device.
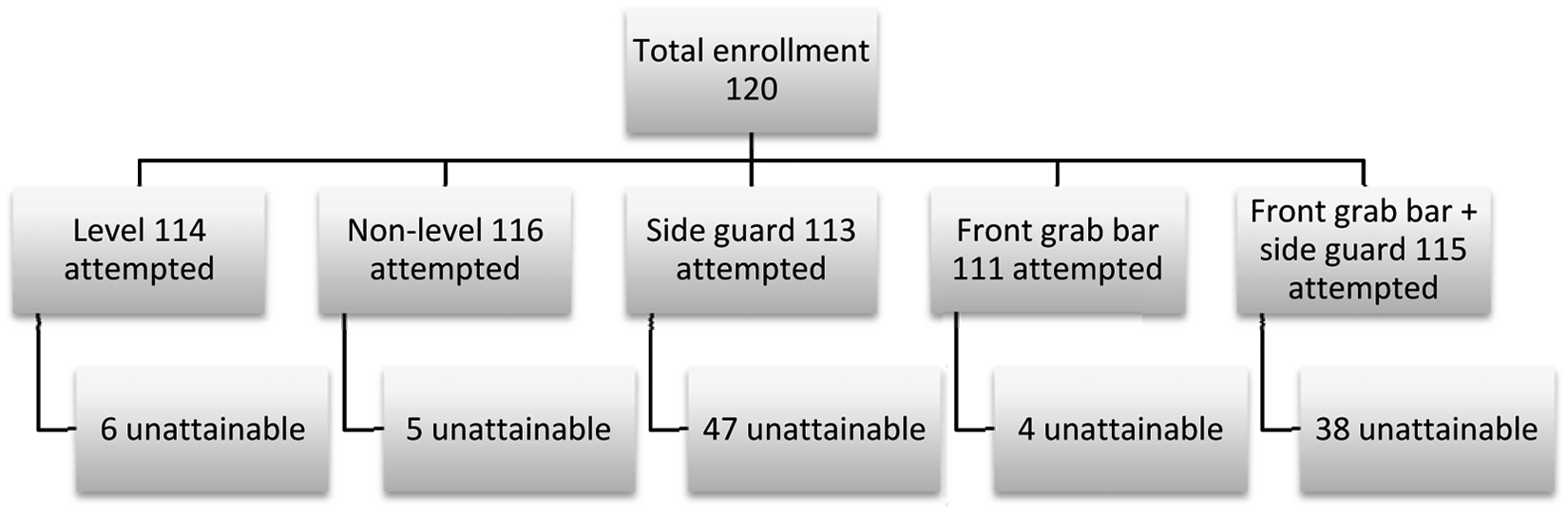
Total number of participants who attempted each protocol and number of participants who were unable to attain any transfers within each protocol.
At the beginning of each protocol, participants were also allowed to judge where they thought their maximum (or minimum) height or gap would be, and this estimate was set as the starting point. As such, they did not have to perform all transfers at every possible height increment in the station, which helped to minimize fatigue and the number of transfers they had to complete. If they could easily do the transfer at their starting point, then we continued to incrementally increase or decrease the height (or gap) accordingly from their starting point until the maximum (or minimum) height or gap was achieved. The number of trials (transfers) varied for each participant and for each protocol on the basis of how many transfer attempts were needed before finding the maximum or minimum height or gap. The average number of transfers performed during the course of the study per participant was 27 ± 9 (range 2 to 48). Moving from the WMD to the transfer station and back from the transfer station to the WMD counted as two transfers. Most of the participants who remained in the study could perform at least one transfer in each protocol with the exception of the two protocols that included the side guard obstacle. Although 42% (47/113) could not perform a transfer with the side guards present (Figure 4), 23% (11/47) of those participants were able to transfer when the front grab bar was added to the setup.
Height
The 95th-percentile lowest and highest heights attained were similar to the median WMD seat height (56 cm) across all four protocols that measured height as an outcome variable (Table 4). Table 4 also shows that the 5th-percentile attainable heights were the same as the maximums recorded for the group in each protocol. This result is attributable to ceiling effects (e.g., the transfer station platform could be lowered only to 25.4 cm and raised only to 73.7 cm), whereby there were several participants who could cover the full range of height that was allowed by the transfer station in all the protocols. The majority (95th percentile) hovered more closely around the minimum heights for the group, which are similar again to the median WMD seat height. Participants transferred higher when the front grab bar was added to the setup (p = .005) and higher and lower with the front grab bar than without it when the side guard was present in the setup (p = .003 and p = .005, respectively).
Percentiles for the Height Variable, Four Protocols (in centimeters)
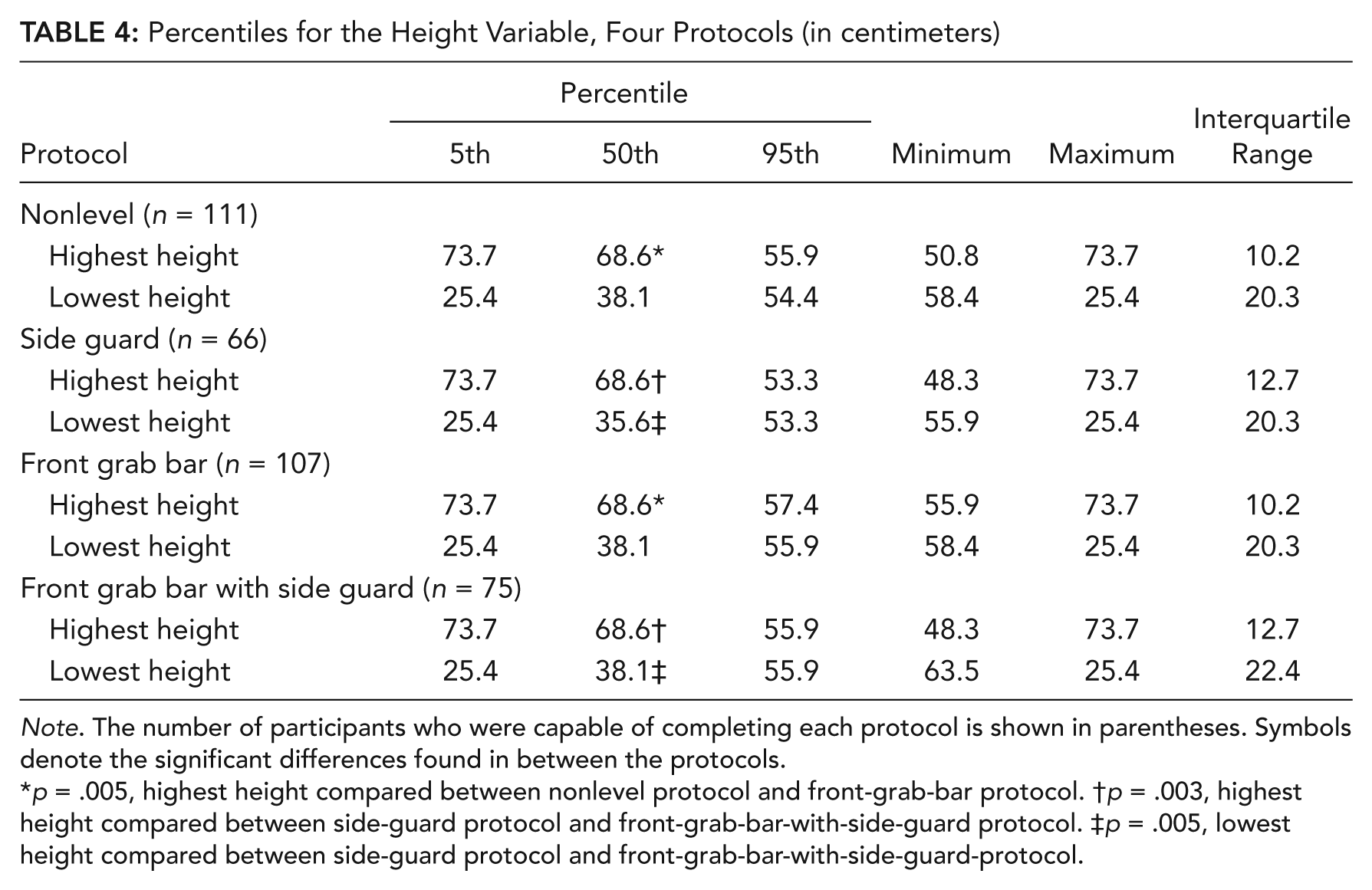
Note. The number of participants who were capable of completing each protocol is shown in parentheses. Symbols denote the significant differences found in between the protocols.
p = .005, highest height compared between nonlevel protocol and front-grab-bar protocol. †p = .003, highest height compared between side-guard protocol and front-grab-bar-with-side-guard protocol. ‡p = .005, lowest height compared between side-guard protocol and front-grab-bar-with-side-guard-protocol.
Gap
All participants who attempted this protocol, which was 95% of the total sample (108/114 total participants; see Figure 4), were able to perform a transfer across the first gap interval (8.9 cm). Participants transferred with a significantly smaller gap interval with the side guard present in the setup than without the side guard (Table 5).
Percentiles for the Gap Variable, Two Protocols (in centimeters)
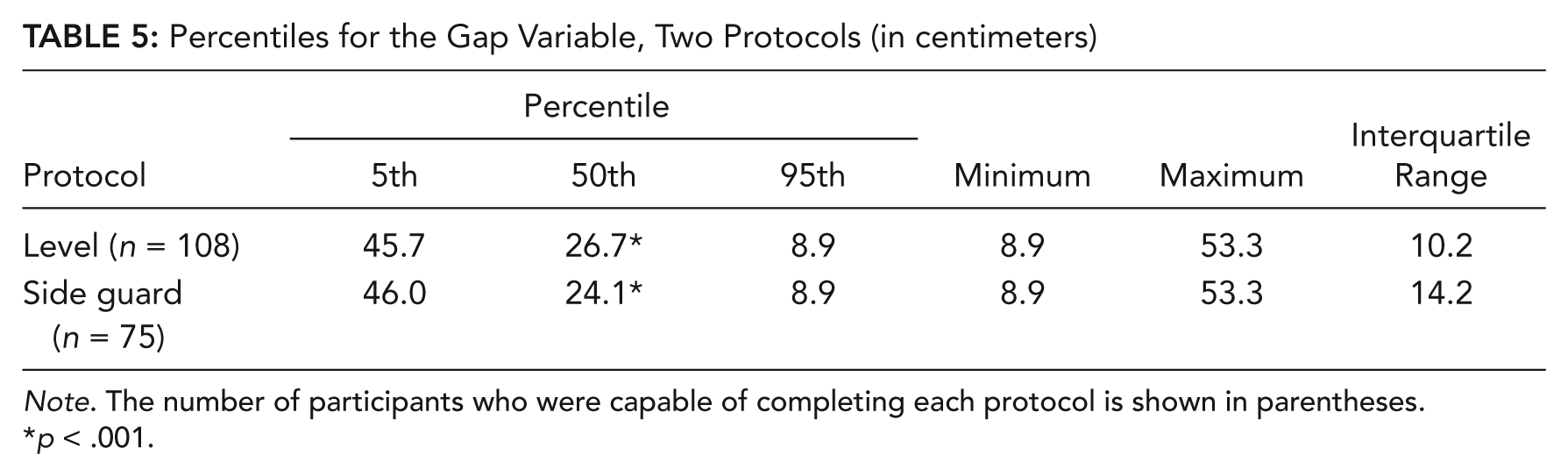
Note. The number of participants who were capable of completing each protocol is shown in parentheses.
p < .001.
Space Requirements for WMD
The 50th-percentile participants approached the transfer platform at a 30° angle (Figure 3 and Table 6). The width dimension was smaller when the gap was introduced compared with the other protocols that tested maximum and minimum height differences without the gap. Adding a front grab bar and/or side guard had no significant impact on changing the amount of clear space needed to perform the transfers at various heights.
Percentiles for the Space Parameter for All the Protocols (in centimeters)

Note. The number of participants who were capable of completing each protocol is shown in parentheses. Symbols denote the significant differences found in between the protocols.
p < .002 between the width needed to transfer at level and the width needed to transfer with the side guard in place. †p < .002 between the width needed to transfer at level and the width needed to transfer when the front grab bar was provided. ‡p < .002 between the width needed to transfer at level and the width needed when the front grab bar and the side guard were in place.
Front Grab Bar Use
When transferring to a lower height, with the front grab bar available and without side guard, 51% (59/115) used the front bar; 20% (23/115) could transfer to a lower height when using the bar; and the bar height preference was 76.2 ± 9.9 cm (median = 76.2 cm). When transferring to a higher height, with the front grab bar and without side guard, 59% (68/115) used the front bar; 17% (20/115) could transfer to a higher height when using the bar; and the bar height preference was 84.8 ± 7.88 cm (median = 81.3 cm).
When transferring to a lower height, with the front grab bar available and side guard in place, 56% (64/115) used the front bar and 19% (22/115) could transfer to a lower height when using the front grab bar. When transferring to a higher height, with the front grab bar available and the side guard, 45% (59/115) used the front bar and 17% (20/115) could transfer to a higher height when using the bar. Although presented with the option to change the front grab bar height with the side guard added, participants chose the same height for all the lower height and higher height transfers as they used for the front grab bar protocol when the side guard was not present.
Results Comparison With Accessibility Guidelines
Accessibility standards recommend transfer surfaces to be between 43.1 and 48.3 cm and for amusement ride seats to be between 35.6 and 61.0 cm (U.S. Access Board, 2004). Our data suggest that element height should ideally fall within a range of 54.4 and 55.9 cm to meet the 95th-percentile WMD user and between 38.1 and 68.6 cm to meet the 50th-percentile WMD user when there are no gaps or obstacles present. No recommendation could be found in the current standards related to an allowable gap distance. The ADAAG suggests a minimum of 76.2 cm width by 121.9 cm depth for spaces where a transfer is expected (see Figure 3); however, our 50th-percentile WMD users required more width than this minimum for all the protocols (Table 6). The ADAAG concerning handholds and grab bars where transfers are expected suggests the height of a horizontal grab bar (parallel to the floor) to be between 83.8 and 91.4 cm for water stalls, water closets, bathtubs, and bathrooms. Our participants preferred the front grab bar height to be lower, between 76.2 and 81.3 cm.
Discussion
In our study, we found that transfer surface heights above and below the WMD seat height, gaps, and obstacles pose serious transfer-related accessibility problems for WMD users. On the basis of data pertaining to transfer heights alone, we can conclude that current standards do not come close to meeting the 95th-percentile needs of the WMD users. WMD users at the 95th-percentile attained their highest height at 55.9 cm with no gap or obstacle in place. This height is very close to their own WMD seat height (median = 56.0 cm). Thus it follows that transfers are the easiest to achieve when the height of the transfer surface is at the same height as the WMD (seat height + cushion). This finding is consistent with research showing that level transfers require less exertion of the upper limb compared with uphill and downhill transfers (Gagnon et al., 2005; Gagnon, Nadeau, Noreau, Eng, & Gravel, 2008; Nyland et al., 2000).
In general, our data suggest that element height should fall within a range of 55.9 cm (highest end) and 54.4 cm (lowest end) to meet the 95th-percentile needs and, similarly, between 68.6 cm and 38.1 cm to meet the 50th-percentile needs when there are no gaps or obstacles present. Current standards accommodate the 50th-percentile needs for height of elements on the higher end of the recommended amusement ride seat height. However, the standards do not accommodate the 50th-percentile needs on the lower end of recommended amusement ride seat height (35.6 cm) because the relative difference in the vertical height drop between the median WMD seat height (56 cm) and this seat level (35.6 cm) is large (20.4 cm), and none of the WMD users had seat heights lower than 43.2 cm off the ground.
Gaps up to 8.9 cm at a height level with the WMD were achievable by 95% of the WMD users. However, our results showed that managing larger gaps beyond this becomes increasingly more difficult, especially in the presence of an obstacle. This finding is consistent with previous research that showed that transferring across a 10-cm gap requires more muscle effort than when the WMD is closest to the surface a user is transferring to and from (Koontz, Gagnon, Brindle & Cooper, 2009). These results underscore the importance of incorporating gap distances into the guidelines. There is also a need to consider the combined effects of gaps and heights when designing new transfer elements.
The recommended minimum clear space for transfers, particularly in the y dimension (width dimension in Figure 3) is insufficient (Table 6). The reason is not that the devices were too large but that most users oriented their devices at an angle instead of using a parallel approach, which affected primarily the amount of width required. Device sizes in this study were comparable in size to those reported in other recent studies (Koontz et al., 2010; Paquet & Feathers, 2004). Many studies have evaluated current accessibility guidelines in terms of space needed for maneuverability and found them insufficient for current device sizes (Dutta, King, Holliday, Gorski, & Fernie, 2011; King, Dutta, Gorski, Holliday, & Fernie, 2011; Koontz et al., 2011). The ADAAG for pools and spas suggests a more plausible clear area of 1.5 m by 1.5 m for transfer walls (“Accessible Pools and Spas,” 2003). This area around all elements where transfers are expected would accommodate the 75th-percentile space needs of current WMD users for transfers on the basis of interpolation of the 50th- and 95th-percentile data shown in Table 6. The data also show that when gaps were introduced, not surprisingly, participants positioned themselves as close as they could to the station, resulting in significantly less clear space in y (width dimension) when compared with the other protocols that evaluated heights and no gaps.
The addition of the side guard obstacle to the station made transferring to the platform impossible for 42% of the WMD users. Although guidelines for aircraft transportation recommend that the armrest be able to pivot for an airplane seat to be accessible, it is not mandated (Zaworski & Hunter-Zaworski, 2010). Similarly, the ADAAG for pools and spas suggests that if the lift seat has armrests, they need to be able to pivot so people can transfer from and to their WMD and the lift more easily (“Accessible Pools and Spas,” 2003). Our data show that although obstacles are challenging, adding a grab bar in front of the transfer seat helped 11 people who could not otherwise do the side guard protocol to do it with the grab bar present. Moreover, the front grab bar helped several participants who performed the side guard transfer to attain higher and lower heights. Both grab bars (front and lateral) and the side guard were used often for repositioning the trunk and buttocks onto the platform after landing; however, their use for this purpose was not documented. It is possible that grab bars and handhelds placed in other locations around the station could have enabled more successful transfers. Our study underscores the need for further research on alternative hand placement options for both initial hand placement and repositioning after landing on the target surface.
A large number of our participants were veterans who participated in organized sports–related events; however, we have shown in previous research that their daily activity levels apart from the time of the event do not differ from community-dwelling adult WMD users (Tolerico et al., 2007). The demographics of our sample closely resemble those of other studies. For instance, in a study of minimum space requirements for WMD maneuverability, the majority of participants had SCI, followed by those with central nervous system disorders (e.g., MS, CP, and spina bifida; Koontz et al., 2010). Similarly, in a pilot study of environmental barriers and facilitators for wheelchair users, the majority of participants had SCI, followed by those with MS (Meyers, Anderson, Miller, Shipp, & Hoenig, 2002). In another study, focusing of the effect of cross-slopes on the mobility of manual wheelchair users, the majority of participants had SCI, followed by those with MS, CP, spina bifida, and amputations (Souza, Teodorski, Sporner, & Cooper, 2010). Given demographic similarities between these studies and ours, and the efforts taken to recruit and test at multiple test facilities and locations, we believe that the results of this study are generalizable to the population of active, community-dwelling WMD users.
Limitations and Future Work
Horizontal gap was not evaluated in all protocols in Table 2 to limit the total number of transfers required and to avoid excessive overloading on the upper limbs and fatigue in a single test session. Moreover, for the same reason, we evaluated changes in one variable while keeping the other variable constant (e.g., either heights were varied with a constant [0-cm] gap or gap was varied at a constant-level WMD seat height), which limits the generalizability of the findings to these specific experimental conditions. A study with multiple test sessions (e.g., because of the large number of transfers necessary) would be needed to systematically evaluate the interactions between varying both gap and height for each environmental setup.
Successful transfers in this study were defined by the participant’s making it to the platform without losing his or her balance or falling. It is possible that the maximum heights and gaps achieved by the WMD users were attained in a “safe” way but by using techniques that may predispose them to other injuries, such as rotator cuff tears or compression of the median nerve, that may occur from placing their hands, wrists, and shoulders in awkward positions during weight bearing. Future studies should include a measure of transfer quality, such as recording joint biomechanics during the transfers or using the Transfer Assessment Instrument (McClure, Boninger, Ozawa, & Koontz, 2011), a simple checklist that can be used to evaluate whether the transfer is being performed in accordance with evidence-based “best” transfer practices. Measures such as these would provide great insight into the relationship between transfer skill and performance. Similarly, the WMD users presented with a wide variety of physical limitations and function. Future studies incorporating measures such as upper-extremity range-of-motion, strength, and balance tests are needed to better understand the relationship between the specific capabilities of the WMD users and their transfer performance. However, although measures of skill and function increase the understanding of the factors influencing performance, from an accessibility viewpoint, the findings in this study provide ample insight into critical design needs for improving accessibility for a broad and diverse group of WMD users who independently transfer.
In this study, we followed the “accessibility” approach and not a “universal design” approach as defined in a previous study (Gossett, Mirza, Barnds, & Feidt, 2009), by which we studied the barriers to transfers and the addition of features to enhance the transfer process specifically of a subset of the population. As universal design is about providing environments that are fully experienced by all people, we do not know whether implementation of the results would lend to an environment that would do so, and it may in fact come in conflict with it. For example, lowering the current ADA-compliant grab bar height to better accommodate current WMD users may not work well for older frail standing adults who use a grab bar to assist with stability and balance during the transfer. Along these same lines, the study findings are specific to individuals who independently transfer. Individuals requiring assistance with transfer by a caregiver may have different design needs (e.g., more clear space). The results of this study may help universal designers find the right balance between meeting the accessibility needs of WMD users and maintaining the features of universal design.
Conclusion
Transfer surfaces that are above or below the WMD seat height, gaps, and obstacles pose serious transfer-related accessibility problems for WMD users. Transferring to a height similar to the median WMD seat-to-floor height (56 cm) when there are no gaps or obstacles present meets the 95th-percentile of WMD users who can independently transfer. Current ADAAG recommendations fall short in terms of height recommendations and space available for 50th-percentile WMD users. More investigation is needed on handhelds and different ways to adapt transfer elements to eliminate obstacles and enable for more level transfers. The results of this study could help airline, motor vehicle, amusement park ride, and adaptive equipment manufacturers to improve and create designs that facilitate the transfer process.
Key Points
The purpose of this study was to investigate the impact of setup on the transfer process, including height, gap, use and placement of handhelds or grab bars, effect of an obstacle, and space for positioning the mobility device.
We used a custom-built transfer station and had participants transfer to and from it with different setup parameters.
Our results showed that height above and below wheeled mobility device (WMD) seat-to-floor height, gaps, and obstacles pose serious transfer-related accessibility problems for WMD users. Current accessibility guidelines would exclude the majority of our sample.
The results from this study have implications for refining current accessibility guidelines and design of the built environment.
Footnotes
Acknowledgements
The authors are also affiliated with the University of Pittsburgh, Pittsburgh, Pennsylvania. Funding for this study was provided by the Department of Education (NIDRR), United States Access Board Grant H133E070024 and Project No. 84.133E. This material is the result of work supported with resources and the use of facilities at the Human Engineering Research Laboratories, VA Pittsburgh Healthcare System. The contents do not represent the views of the Department of Veterans Affairs or the U.S. government.
Maria Luisa Toro is a PhD student in rehabilitation science at the University of Pittsburgh. She obtained her master of science at the University of Pittsburgh in 2011.
Alicia M. Koontz is a research biomedical engineer at the Human Engineering Research Laboratories. She is also an associate professor in the School of Health and Rehabilitation Sciences at the University of Pittsburgh. She received a PhD in rehabilitation science from the University of Pittsburgh in 2001.
Rory A. Cooper is the FISA and PVA Chair and Distinguished Professor of the Department of Rehabilitation Science and Technology and a professor of bioengineering and mechanical engineering at the University of Pittsburgh. He is also a professor in the Department of Physical Medicine and Rehabilitation within the Department of Orthopedic Surgery at the University of Pittsburgh Medical Center Health System. He is a founding director and VA senior research career scientist of the VA Rehabilitation Research and Development Center of Excellence in Pittsburgh. He received a PhD degree in electrical and computer engineering with a concentration in bioengineering from the University of California at Santa Barbara in 1989.